
Cephalometric and Photographic Evaluation of the Nasolabial Angle in Orthodontically Treated Patients: An Observational Cohort Study

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
Study Design, Patient Selection, and Measurements
- White female and male healthy patients;
- No history of orthodontic treatment or facial surgery;
- Upper premolar extraction;
- Radiographs showing good hard and soft tissue resolution;
- Good quality and contrast imaging.
- Previous orthodontic treatment:
- History of trauma;
- Surgical interventions at the level of head or neck;
- The presence of congenital facial deformities;
- Low X-ray image quality;
- Movement or metal artifacts on the lateral radiographs.
- SNA angle—indicates the position of the maxilla in the sagittal plane. We considered it essential to examine because the maxilla provides bony support for the upper lips;
- SN-P angle—shows the position between the skull base and the bispinal line (palatal plane—PP), i.e., the vertical position of the maxilla;
- ANS-Gn—shows the distance between the spina nasalis anterior and the bony gnathion, i.e., the skeletal height of the lower third of the face;
- GoGn-SN—provides information about the position of the base of the mandible [5].
- Is-SN—the angle formed by the axis of the upper incisors and the base of the skull shows the sagittal position of the incisors in relation to the base of the skull and independently of the maxilla;
- Is-PP—the angle between the axis of the upper incisors and the bispinal line (palatal plane—PP), showing the position of the incisors in relation to the vertical position of the maxilla;
- Is-NA—the angle enclosed by the line between the axis of the upper incisors and the nasion, A-point, showing the position of the incisors in relation to the sagittal position of the maxilla;
- Is-NA—the distance between the most incisally located point of the upper incisors and the NA-line, expressed in millimeters [5].
- ULT (upper lip thickness)—upper lip thickness, which is the distance between the outer and inner points of the upper lip (Ls-Ls_int);
- UL-E—the distance of the upper lip from the E-line (Rickkets’ aesthetic line drawn between the pronasale and soft tissue pogonion points).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauro Fradeani–Esthetic Rehabilitation. In Fixed Prosthodontics Volume 1, 1st ed.; Quintessence Publishing Co.: Carol Stream, IL, USA, 2004; pp. 50–52.
- Bergman, R.T.; Waschak, J.; Borzabadi-Farahani, A.; Murphy, N.C. Longitudinal Study of Cephalometric Soft Tissue Profile Traits between the Ages of 6 and 18 Years. Angle Orthod. 2014, 84, 48–55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fernández-Riveiro, P.; Smyth-Chamosa, E.; Suárez-Quintanilla, D.; Suárez-Cunqueiro, M. Angular Photogrammetric Analysis of the Soft Tissue Facial Profile. Eur. J. Orthod. 2003, 25, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.T. Cephalometric Soft Tissue Facial Analysis. Am. J. Orthod. Dentofacial Orthop. 1999, 116, 373–389. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, J.P.; Nanda, R.S.; Currier, G.F. An Evaluation of the Nasolabial Angle and the Relative Inclinations of the Nose and Upper Lip. Am. J. Orthod. Dentofacial Orthop. 1992, 102, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.L.; Sakima, M.T.; Pinto, A.d.S.; Bowman, S.J. Upper Lip Changes Correlated to Maxillary Incisor Retraction—A Metallic Implant Study. Angle Orthod. 2005, 75, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Paskay, L.C.; D’Andrea, N.; Albani, A.; Monaco, A.; Saccomanno, S. Evaluation of the Nasolabial Angle in Orthodontic Diagnosis: A Systematic Review. Appl. Sci. 2021, 11, 2531. [Google Scholar] [CrossRef]
- Gołębiowski, M.; Świątkowska, A.; Pastuszak, P.; Rahnama, M. Relationship between Selected Cephalometric Parameters, Nasolabial Angle and Its Components in Adolescent Females. Diagnostics 2023, 13, 1199. [Google Scholar] [CrossRef]
- Talass, M.F.; Talass, L.; Baker, R.C. Soft-Tissue Profile Changes Resulting from Retraction of Maxillary Incisors. Am. J. Orthod. Dentofacial Orthop. 1987, 91, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Rathod, A.B.; Araujo, E.; Vaden, J.L.; Behrents, R.G.; Oliver, D.R. Extraction vs No Treatment: Long-Term Facial Profile Changes. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M.; Markic, G.; Doulis, I.; Göllner, P.; Patcas, R.; Hänggi, M.P. Effect of Different Incisor Movements on the Soft Tissue Profile Measured in Reference to a Rough-Surfaced Palatal Implant. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Hodges, A.; Rossouw, P.E.; Campbell, P.M.; Boley, J.C.; Alexander, R.A.; Buschang, P.H. Prediction of Lip Response to Four First Premolar Extractions in White Female Adolescents and Adults. Angle Orthod. 2009, 79, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Mattos, C.T.; de Almeida, N.V.; Silveira, G.S.; Motta, A.T.; Mota-Júnior, S.L.; Mucha, J.N. Reconsidering the Role of Nasolabial Angle in Premolar Extraction Decision-Making: A Case-Series Study. Orthod. Craniofac. Res. 2024, 27, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Saelens, N.A.; De Smit, A.A. Therapeutic Changes in Extraction versus Non-Extraction Orthodontic Treatment. Eur. J. Orthod. 1998, 20, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, A.; Janiszewska-Olszowska, J.; Jedliński, M.; Grocholewicz, K. Methods of Analysis of the Nasal Profile: A Systematic Review with Meta-analysis. BioMed Res. Int. 2021, 2021, 6680175. [Google Scholar] [CrossRef] [PubMed]
- Sangalli, L.; Savoldi, F.; Dalessandri, D.; Visconti, L. Historical Development of the Planning of Incisal Position in Orthodontic Treatments: A Narrative Review of the Literature. Curr. Trends Dent. 2021, 1, 01. [Google Scholar]
- Rosa, M. Essay I: Orthodontic Edentulous Space Closure in All Malocclusions. Int. J. Esthet. Dent. 2020, 15 (Suppl. S1), S14–S31. [Google Scholar] [PubMed]
- Perović, T.M.; Blažej, Z.; Jovanović, I. The Influence of Antero-Posterior Dentoskeletal Pattern on the Value of Nasal Soft Tissue Angles: A Cephalometric Study. Folia Morphol. 2021, 80, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Ballin, A.C.; Carvalho, B.; Dolci, J.E.L.; Becker, R.; Berger, C.; Mocellin, M. Anthropometric Study of the Caucasian Nose in the City of Curitiba: Relevance of Population Evaluation. Braz. J. Otorhinolaryngol. 2018, 84, 486–493. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Uysal, T.; Baysal, A.; Yagci, A.; Sigler, L.M.; McNamara, J.A., Jr. Ethnic Differences in the Soft Tissue Profiles of Turkish and European-American Young Adults with Normal Occlusions and Well-Balanced Faces. Eur. J. Orthod. 2012, 34, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Raffaini, M.; Magri, A.; Conti, M.; Arcuri, F. Advanced Facial Rejuvenation After Bimaxillary Surgery in Three Different Facial Types. Aesthetic Plast. Surg. 2022, 46, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Kocadereli, I. Changes in Soft Tissue Profile After Orthodontic Treatment with and without Extractions. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Konstantonis, D.; Vasileiou, D.; Papageorgiou, S.N.; Eliades, T. Soft Tissue Changes Following Extraction vs. Nonextraction Orthodontic Fixed Appliance Treatment: A Systematic Review and Meta-Analysis. Eur. J. Oral Sci. 2018, 126, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Kokodynski, R.A.; Marshall, S.D.; Ayer, W.; Weintraub, N.H.; Hoffman, D.L. Profile Changes Associated with Maxillary Incisor Retraction in the Postadolescent Orthodontic Patient. Int. J. Adult Orthodon. Orthognath. Surg. 1997, 12, 129–134. [Google Scholar] [PubMed]
- Brock, R.A., 2nd; Taylor, R.W.; Buschang, P.H.; Behrents, R.G. Ethnic Differences in Upper Lip Response to Incisor Retraction. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 683–691; quiz 755. [Google Scholar] [CrossRef] [PubMed]
- Alkadhi, R.M.; Finkelman, M.D.; Trotman, C.A.; Kanavakis, G. The Role of Lip Thickness in Upper Lip Response to Sagittal Change of Incisor Position. Orthod. Craniofac. Res. 2019, 22, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Pearlman, S.J. Surgical Treatment of the Nasolabial Angle in Balanced Rhinoplasty. Facial Plast. Surg. 2006, 22, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Burstone, C.J. Lip Posture and Its Significance in Treatment Planning. Am. J. Orthod. 1967, 53, 262–284. [Google Scholar] [CrossRef] [PubMed]
- Hodgkinson, D.; Firth, F.A.; Farella, M. Effect of Incisor Retraction on Facial Aesthetics. J. Orthod. 2019, 46 (Suppl. S1), 49–53. [Google Scholar] [CrossRef] [PubMed]
- Bravo, L.A.; Canut, J.A.; Pascual, A.; Bravo, B. Comparison of the Changes in Facial Profile after Orthodontic Treatment, with and without Extractions. Br. J. Orthod. 1997, 24, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Ismail, S.F.; Moss, J.P.; Hennessy, R. Three-Dimensional Assessment of the Effects of Extraction and Nonextraction Orthodontic Treatment on the Face. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 244–256. [Google Scholar] [CrossRef] [PubMed]
- Stephens, C.K.; Boley, J.C.; Behrents, R.G.; Alexander, R.G.; Buschang, P.H. Long-Term Profile Changes in Extraction and Nonextraction Patients. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Garg, H.; Khundrakpam, D.; Saini, V.; Rukshana, R.; Kaldhari, K.; Kaur, J. Relationship of Nasolabial Angle with Maxillary Incisor Proclination and Upper Lip Thickness in North Indian Population. Int. J. Clin. Pediatr. Dent. 2022, 15, 489–492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Holdaway, R.A. A Soft-Tissue Cephalometric Analysis and Its Use in Orthodontic Treatment Planning. Part I. Am. J. Orthod. 1983, 84, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Mendes, L.M.; Junqueira, C.H.Z.; Garib, D.G. Soft-tissue changes in Class II malocclusion patients treated with extractions: A systematic review. Eur. J. Orthod. 2016, 38, 631–637. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Landmarks | Definitions |
|---|---|
| Sella—S | Center of the pituitary fossa of the sphenoid bone. |
| Nasion—N | Most anterior point on the frontonasal suture in the midsagittal plane. |
| Point A, subspinale—A | Deepest point of the curve of the anterior border of the maxilla. |
| Point B, submentale—B | Most posterior point in the concavity along the anterior border of the symphysis. |
| Subnasale—Sn | A sagittal point where the nasal septum and the upper lip meet in the midsagittal plane. |
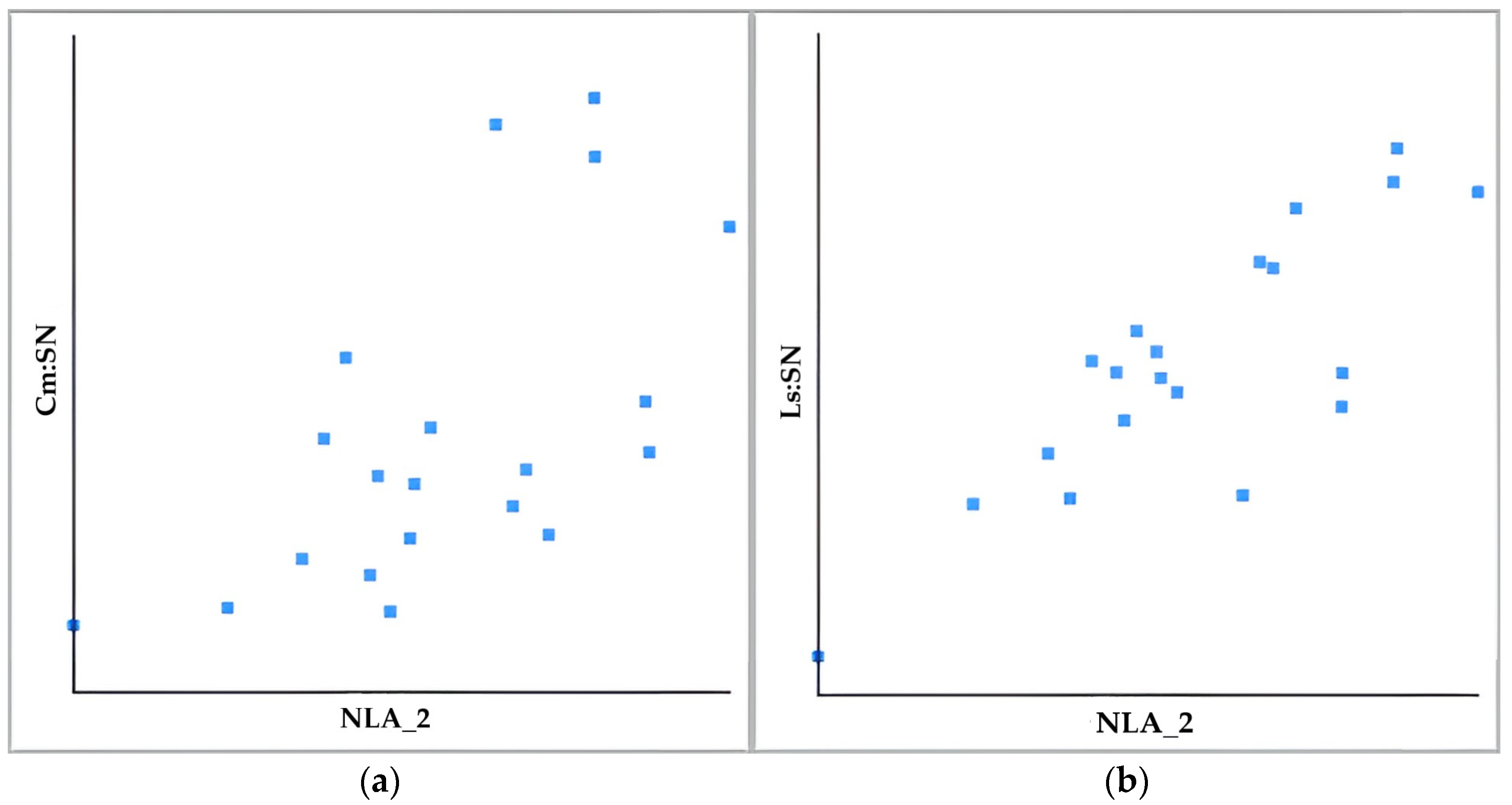
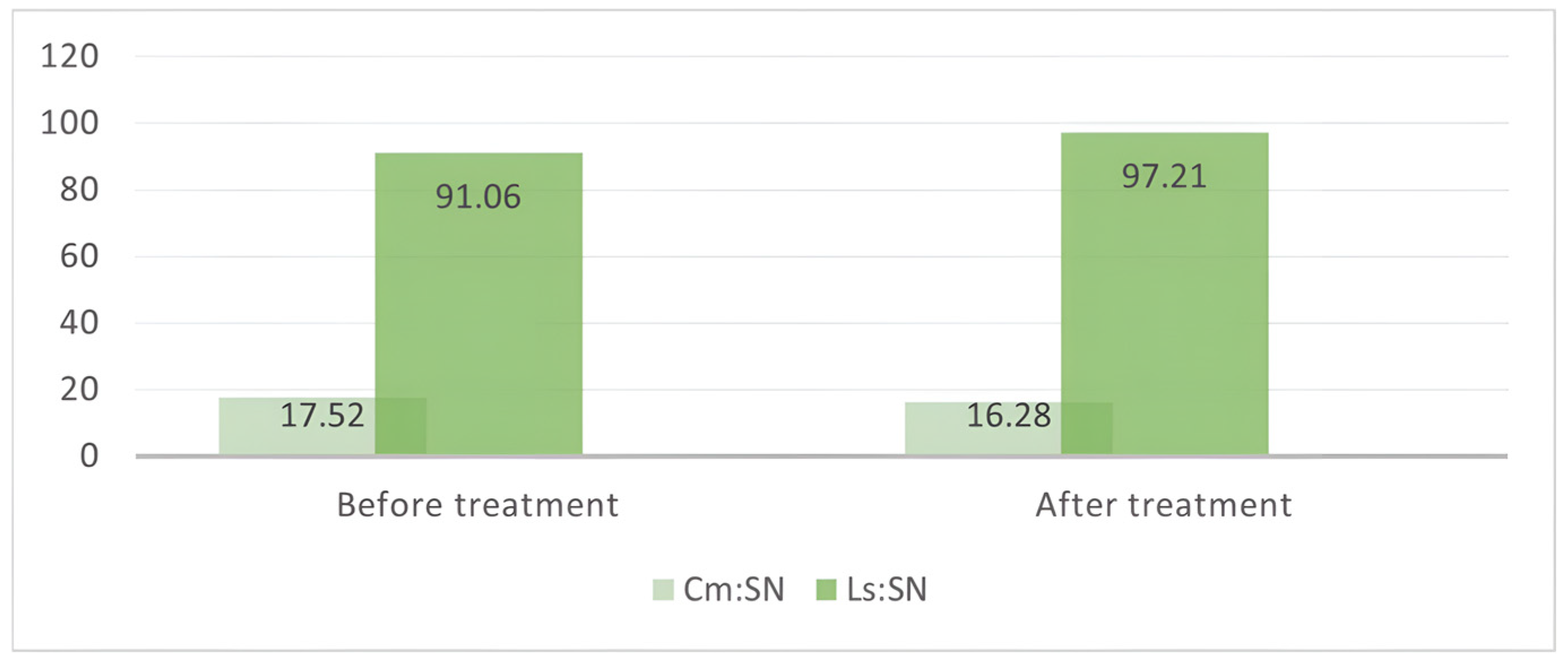
| Columella nasi—Cm | The external end of the nasal septum. |
| Labral superior—Ls | The uppermost point of the upper lip. |
| Labral inferior—Ls_inf | The boundary of the lower lip and the skin intersected in the median sagittal plane. |
| Spina nasalis anterior—SNA | Most anterior midpoint of the anterior nasal spine of the maxilla. |
| Spina nasalis posterior—SNP | The sharp and well-defined posterior extremity of the nasal crest of the hard palate. |
| Incisor superior incisal—Is_i | The most anterior point on the labial surface of the most prominent maxillary central incisor. |
| Incisor superior apex—Is_a | The most apical point of the upper incisor root. |
| Pronasale—Mon | The most prominent point of the tip of the nose. |
| Soft Tissue Pogonion—Pog’ | The most anterior point on the mandibular symphysis. |
| Gnathion—Gn | The most antero-inferior point on the mandibular symphysis. |
| Soft Tissue Gnathion—Gn’ | |
| Gonion—Go | The most posterior and inferior point on the mandible corpus. |
| NLA_1 (° ± SD) | NLA_2 (° ± SD) | |
|---|---|---|
| Before treatment | 106.86° ± 12.88° | 111.61° ± 11.97° |
| After treatment | 107.97° ± 9.43° | 113.42° ± 9.58° |
| Parameters | Before Treatment | After Treatment | p Value |
|---|---|---|---|
| SNA | 80.75° ± 2.91° | 79.98° ± 2.88° | 0.06 |
| SN-PP | 8° ± 3.32° | 8,15° ± 3.63° | 0.22 |
| ANS-Gn | 115.59 mm ± 12.17 mm | 116.86 mm ± 12.59 mm | 0.08 |
| GoGn-SN | 148.67° ± 6.2° | 149.61° ± 5.49° | 0.62 |
| Is-SN | 103.75° ± 9.26° | 102.18° ± 7.51° | 0.41 |
| Is-PP | 111.74° ± 8.11° | 110.33° ± 7.49° | 0.44 |
| Is-NA | 23° ± 8.71° | 22.2° ± 7.34° | 0.99 |
| Is-NA | 7.84 mm ± 4.97 mm | 6.43 mm ± 3.84 mm | 0.18 |
| ULT | 21.4 mm ± 4.07 mm | 22.9 mm ± 4.06 mm | 0.03 * |
| UL-E | 8.42 mm ± 4.84 mm | 10.35 mm ± 423 mm | 0.00 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, S.I.; Bud, E.; Mártha, K.; Mureșan, I.É.; Jánosi, K.M.; Dósa, B.; Kerekes-Máthé, B. Cephalometric and Photographic Evaluation of the Nasolabial Angle in Orthodontically Treated Patients: An Observational Cohort Study. Diagnostics 2025, 15, 132. https://doi.org/10.3390/diagnostics15020132
Pop SI, Bud E, Mártha K, Mureșan IÉ, Jánosi KM, Dósa B, Kerekes-Máthé B. Cephalometric and Photographic Evaluation of the Nasolabial Angle in Orthodontically Treated Patients: An Observational Cohort Study. Diagnostics. 2025; 15(2):132. https://doi.org/10.3390/diagnostics15020132
Chicago/Turabian StylePop, Silvia Izabella, Eugen Bud, Krisztina Mártha, Izabella Éva Mureșan, Kinga Mária Jánosi, Boglárka Dósa, and Bernadette Kerekes-Máthé. 2025. "Cephalometric and Photographic Evaluation of the Nasolabial Angle in Orthodontically Treated Patients: An Observational Cohort Study" Diagnostics 15, no. 2: 132. https://doi.org/10.3390/diagnostics15020132
APA StylePop, S. I., Bud, E., Mártha, K., Mureșan, I. É., Jánosi, K. M., Dósa, B., & Kerekes-Máthé, B. (2025). Cephalometric and Photographic Evaluation of the Nasolabial Angle in Orthodontically Treated Patients: An Observational Cohort Study. Diagnostics, 15(2), 132. https://doi.org/10.3390/diagnostics15020132