
Clinical and Pathological Profile of Children and Adolescents with Osteosarcoma

 , , , ,
, , , , 
Abstract
1. Introduction
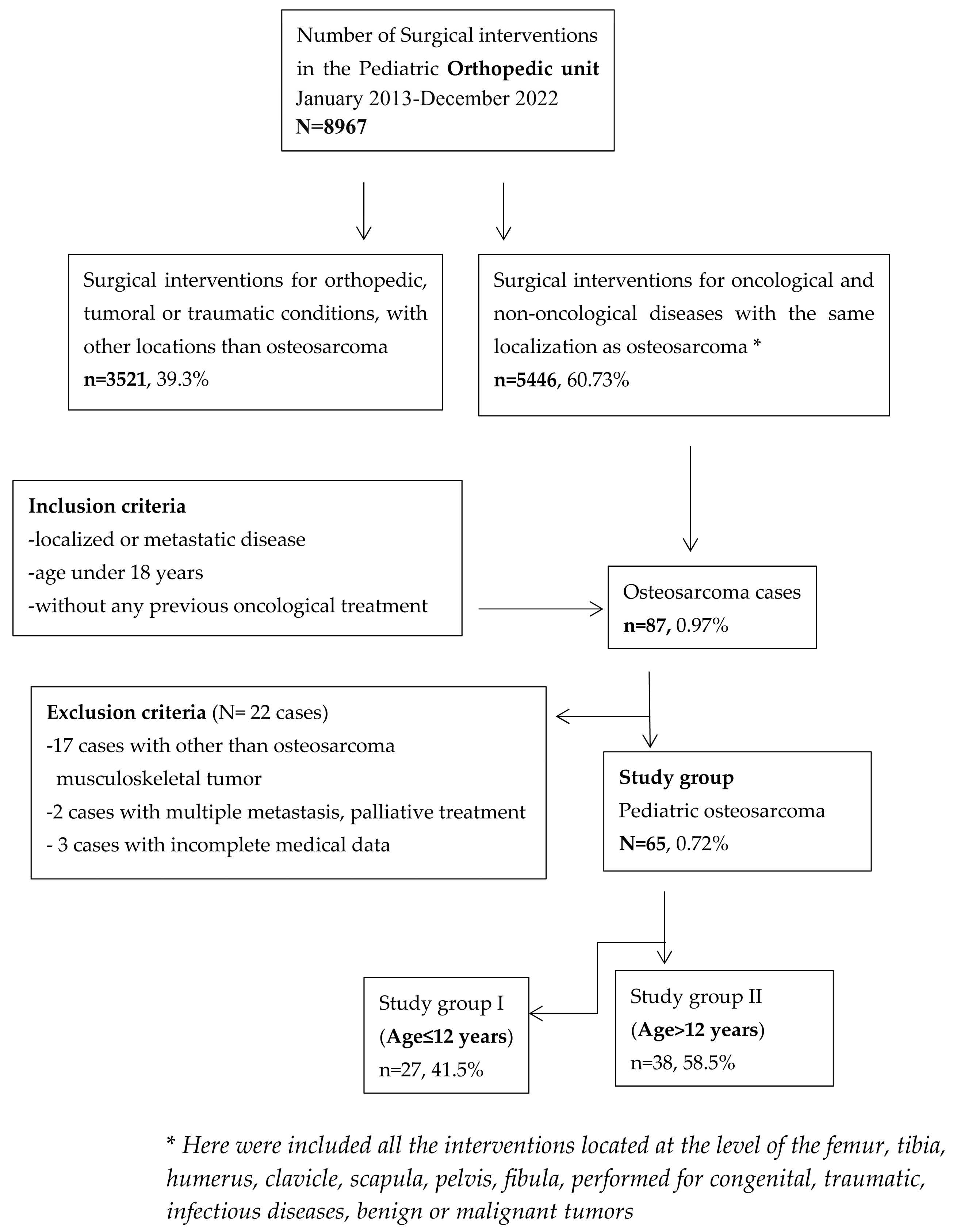
2. Materials and Methods
Statistics
3. Results
3.1. Demographic and Clinical–Pathological Characteristics of Osteosarcomas in Children and Adolescents
3.2. Biological Markers
3.3. Survival
3.4. Prognostic Factors Based on Clinical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taran, S.J.; Taran, R.; Malipatil, N.B. Pediatric Osteosarcoma: An Updated Review. Indian J. Med. Paediatr. Oncol. 2017, 38, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E.; Stiller, C.; Kaatsch, P.; Berrino, F.; Coebergh, J.W.; Lacour, B.; Parkin, M. Geographical patterns and time trends of cancer incidence and survival among children and adolescents in Europe since the 1970s (the ACCISproject): An epidemiological study. Lancet 2004, 364, 2097–2105. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.A.; Mirabello, L. Using epidemiology and genomics to understand osteosarcoma etiology. Sarcoma 2011, 2011, 548151. [Google Scholar] [CrossRef] [PubMed]
- Picci, P. Osteosarcoma (osteogenic sarcoma). Orphanet J. Rare Dis. 2007, 2, 6. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Sun, H.; Li, J.; Guo, Y.; Zhang, K.; Lang, C.; Zou, C.; Ma, H. Increased survival of patients aged 0–29 years with osteosarcoma: A period analysis, 1984–2013. Cancer Med. 2018, 7, 3652–3661. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cole, S.; Gianferante, D.M.; Zhu, B.; Mirabello, L. Osteosarcoma: A Surveillance, Epidemiology, and End Results program-based analysis from 1975 to 2017. Cancer 2022, 128, 2107–2118. [Google Scholar] [CrossRef]
- Foucar, K.; Chabot-Richards, D.; Czuchlewski, D.R.; Karner, K.H.; Reichard, K.K.; Vasef, M.A.; Wilson, C.S.; Zhang, Q.-Y.; Culbreath, K. (Eds.) Neutropenia. In Diagnostic Pathology, Diagnostic Pathology: Blood and Bone Marrow, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 180–187. ISBN 9780323392549. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Choi, J.H.; Ro, J.Y. The 2020 WHO Classification of Tumors of Bone: An Updated Review. Adv. Anat. Pathol. 2021, 28, 119–138. [Google Scholar] [CrossRef] [PubMed]
- Choderlos de Laclos, X.; Risbourg, S.; Brennan, B.; Bertucci, F.; Gaspar, N.; Gelderblom, H.; Hawkins, D.S.; Janeway, K.; Juergens, H.; Kasper, B.; et al. Impact of age on safety of Busulfan-Melphalan followed by autologous hematopoietic stem-cell transplantation versus standard chemotherapy in the patients of the EURO-E.W.I.N.G. 99 and Ewing 2008 clinical trials. Eur. J. Cancer 2024, 208, 114229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Botta, L.; Gatta, G.; Capocaccia, R.; Stiller, C.; Cañete, A.; Dal Maso, L.; Innos, K.; Mihor, A.; Erdmann, F.; Spix, C.; et al. Long-term survival and cure fraction estimates for childhood cancer in Europe (EUROCARE-6): Results from a population-based study. Lancet Oncol. 2022, 23, 1525–1536. [Google Scholar] [CrossRef] [PubMed]
- Kansara, M.; Teng, M.W.; Smyth, M.J.; Thomas, D.M. Translational biology of osteosarcoma. Nat. Rev. Cancer 2014, 14, 722–735. [Google Scholar] [CrossRef]
- Rothzerg, E.; Xu, J.; Wood, D. Different Subtypes of Osteosarcoma: Histopathological Patterns and Clinical Behaviour. J. Mol. Pathol. 2023, 4, 99–108. [Google Scholar] [CrossRef]
- van Ewijk, R.; Herold, N.; Baecklund, F.; Baumhoer, D.; Boye, K.; Gaspar, N.; Harrabi, S.B.; Haveman, L.M.; Hecker-Nolting, S.; Hiemcke-Jiwa, L.; et al. European standard clinical practice recommendations for children and adolescents with primary and recurrent osteosarcoma. EJC Paediatr. Oncol. 2023, 2, 100029. [Google Scholar] [CrossRef]
- Zarghooni, K.; Bratke, G.; Landgraf, P.; Simon, T.; Maintz, D.; Eysel, P. The Diagnosis and Treatment of Osteosarcoma and Ewing’s Sarcoma in Children and Adolescents. Dtsch. Arztebl. Int. 2023, 120, 405–412. [Google Scholar] [CrossRef] [PubMed]
- (GPOH) GfPOuH: S1-Leitlinie Ewing-Sarkom des Kinder-und Jugendalters. Available online: https://register.awmf.org/de/leitlinien/detail/025-006 (accessed on 15 January 2024).
- Prater, S.; McKeon, B. Osteosarcoma; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK549868/ (accessed on 3 December 2024).
- Mirabello, L.; Troisi, R.J.; Savage, S.A. International osteosarcoma incidence patterns in children and adolescents, middle ages and elderly persons. Int. J. Cancer 2009, 125, 229–234. [Google Scholar] [CrossRef]
- Damron, T.A.; Ward, W.G.; Stewart, A. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma: National cancer data base report. Clin. Orthop. Relat. Res. 2007, 459, 40–47. [Google Scholar] [CrossRef]
- Eleutério, S.J.; Senerchia, A.A.; Almeida, M.T.; Da Costa, C.M.; Lustosa, D.; Calheiros, L.M.; Barreto, J.H.; Brunetto, A.L.; Macedo, C.R.; Petrilli, A.S. Osteosarcoma in patients younger than 12 years old without metastases have similar prognosis as adolescent and young adults. Pediatr. Blood Cancer 2015, 62, 1209–1213. [Google Scholar] [CrossRef] [PubMed]
- Mai, P.L.; Best, A.F.; Peters, J.A.; DeCastro, R.M.; Khincha, P.P.; Loud, J.T.; Bremer, R.C.; Rosenberg, P.S.; Savage, S.A. Risks of first and subsequent cancers among TP53 mutation carriers in the National Cancer Institute Li-Fraumeni syndrome cohort. Cancer 2016, 122, 3673–3681. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wong, F.L.; Boice, J.D., Jr.; Abramson, D.H.; Tarone, R.E.; Kleinerman, R.A.; Stovall, M.; Goldman, M.B.; Seddon, J.M.; Tarbell, N.; Fraumeni, J.F., Jr.; et al. Cancer incidence after retinoblastoma. Radiation dose and sarcoma risk. JAMA 1997, 278, 1262–1267. [Google Scholar] [CrossRef] [PubMed]
- Czarnecka, A.M.; Synoradzki, K.; Firlej, W.; Bartnik, E.; Sobczuk, P.; Fiedorowicz, M.; Grieb, P.; Rutkowski, P. Molecular Biology of Osteosarcoma. Cancers 2020, 12, 2130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Eyre, R.; Feltbower, R.G.; James, P.W.; Blakey, K.; Mubwandarikwa, E.; Forman, D.; McKinney, P.A.; Pearce, M.S.; McNally, R.J. The epidemiology of bone cancer in 0–39 year olds in northern England, 1981–2002. BMC Cancer 2010, 10, 357. [Google Scholar] [CrossRef]
- Stiller, C.A.; Passmore, S.J.; Kroll, M.E.; Brownbill, P.A.; Wallis, J.C.; Craft, A.W. Patterns of care and survival for patients aged under 40 years with bone sarcoma in Britain, 1980–1994. Br. J. Cancer 2006, 94, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef] [PubMed]
- Ilcisin, L.A.S.; Han, R.; Krailo, M.D.; Gorlick, R.G.; Nadel, H.R.; Binitie, O.; Janeway, K.A.; Bona, K. Poverty, race, ethnicity, and survival among U.S. children with non-metastatic osteosarcoma treated on EURAMOS-1: A report from the Children’s Oncology Group. J. Clin. Oncol. 2022, 40, 16. [Google Scholar] [CrossRef]
- WHOCoTEB. WHO Classification of Tumours. Soft Tissue and Bone Tumors, 5th ed.; International Agency for Research on Cancer; WHO: Lyon, France, 2020; Volume 3. [Google Scholar]
- Țarcă, V.; Țarcă, E.; Moscalu, M. Social and Economic Determinants of Life Expectancy at Birth in Eastern Europe. Healthcare 2024, 12, 1148. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Filipeanu, D.; Luca, F.A.; Maha, L.G.; Țarcă, V.; Țigănaș, C. The nexus between digital skills’ dynamics and employment in the pandemic context. East. J. Eur. Stud. 2024, 14, 245–264. [Google Scholar] [CrossRef]
- Eyre, R.; Feltbower, R.G.; Mubwandarikwa, E.; Eden, T.O.B.; McNally, R.J.Q. Epidemiology of bone tumours in children and young adults. Pediatr. Blood Cancer 2009, 53, 941–952. [Google Scholar] [CrossRef]
- Andreou, D.; Ranft, A.; Gosheger, G.; Timmermann, B.; Ladenstein, R.; Hartmann, W.; Bauer, S.; Baumhoer, D.; van den Berg, H.; Dijkstra, P.D.S.; et al. Which Factors Are Associated with Local Control and Survival of Patients with Localized Pelvic Ewing’s Sarcoma? A Retrospective Analysis of Data from the Euro-EWING99 Trial. Clin. Orthop. Relat. Res. 2020, 478, 290–302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Simpson, E.; Brown, H.L. Understanding osteosarcomas. J. Am. Acad. Physician Assist. 2018, 31, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, H.; Wang, Z. Predictive value of the systemic immune-inflammation index for cancer-specific survival of osteosarcoma in children. Front. Public. Health 2022, 10, 879523. [Google Scholar] [CrossRef] [PubMed]
- Dakal, T.C.; George, N.; Xu, C.; Suravajhala, P.; Kumar, A. Predictive and Prognostic Relevance of Tumor-Infiltrating Immune Cells: Tailoring Personalized Treatments against Different Cancer Types. Cancers 2024, 16, 1626. [Google Scholar] [CrossRef] [PubMed]
- Zuo, S.; Wei, M.; Wang, S.; Dong, J.; Wei, J. Pan-Cancer Analysis of Immune Cell Infiltration Identifies a Prognostic Immune-Cell Characteristic Score (ICCS) in Lung Adenocarcinoma. Front. Immunol. 2020, 11, 1218. [Google Scholar] [CrossRef] [PubMed]
- Basoli, S.; Cosentino, M.; Traversari, M.; Manfrini, M.; Tsukamoto, S.; Mavrogenis, A.F.; Bordini, B.; Donati, D.M.; Errani, C. The Prognostic Value of Serum Biomarkers for Survival of Children with Osteosarcoma of the Extremities. Curr. Oncol. 2023, 30, 7043–7054. [Google Scholar] [CrossRef] [PubMed]
- Jettoo, P.; Tan, G.; Gerrand, C.H.; Rankin, K.S. Role of routine blood tests for predicting clinical outcomes in osteosarcoma patients. J. Orthop. Surg. 2019, 27, 2309499019838293. [Google Scholar] [CrossRef]
- Song, X.; Zhang, H.; Yin, F.; Guo, P.; Yang, X.; Liu, J.; Han, Y.; Ren, Z. Systemic Inflammatory Markers for Predicting Overall Survival in Patients with Osteosarcoma: A Systematic Review and Meta-Analysis. Mediat. Inflamm. 2021, 2021, 3456629. [Google Scholar] [CrossRef]
- Aggerholm-Pedersen, N.; Maretty-Kongstad, K.; Keller, J.; Baerentzen, S.; Safwat, A. The Prognostic Value of Serum Biomarkers in Localized Bone Sarcoma. Transl. Oncol. 2016, 9, 322–328. [Google Scholar] [CrossRef]
- Fu, Y.; Lan, T.; Cai, H.; Lu, A.; Yu, W. Meta-analysis of serum lactate dehydrogenase and prognosis for osteosarcoma. Medicine 2018, 97, e0741. [Google Scholar] [CrossRef]
- Ren, H.Y.; Sun, L.L.; Li, H.Y.; Ye, Z.M. Prognostic Significance of Serum Alkaline Phosphatase Level in Osteosarcoma: A Meta-Analysis of Published Data. Biomed. Res. Int. 2015, 2015, 160835. [Google Scholar] [CrossRef]
- Foster, L.; Dall, G.F.; Reid, R.; Wallace, W.H.; Porter, D.E. Twentieth-century survival from osteosarcoma in childhood: Trends from 1933 to 2004. J. Bone Jt. Surg. Ser. B 2007, 89, 1234–1238. [Google Scholar] [CrossRef]
- Luca, F.-A.; Ciobanu, C.-I.; Andrei, A.G.; Horodnic, A.V. Raising Awareness on Health Impact of the Chemicals Used in Consumer Products: Empirical Evidence from East-Central Europe. Sustainability 2018, 10, 209. [Google Scholar] [CrossRef]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef]
- Gorlick, R.; Janeway, K.; Lessnick, S.; Randall, R.L.; Marina, N. COG Bone Tumor Committee Children’s Oncology Group’s 2013 blueprint for research: Bone tumors. Pediatr. Blood Cancer 2013, 60, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Hu, H.; Zhang, W.; Shao, Z. Prognostic value of prognostic nutritional index and systemic immune-inflammation index in patients with osteosarcoma. J. Cell. Physiol. 2019, 234, 18408–18414. [Google Scholar] [CrossRef]
- Huang, R.; Xian, S.; Shi, T.; Yan, P.; Hu, P.; Yin, H.; Meng, T.; Huang, Z. Evaluating and Predicting the Probability of Death in Patients with Non-Metastatic Osteosarcoma: A Population-Based Study. Med. Sci. Monit. 2019, 25, 4675–4690. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meyer, W.H.; Pratt, C.B.; Poquette, C.A.; Rao, B.N.; Parham, D.M.; Marina, N.M.; Pappo, A.S.; Mahmoud, H.H.; Jenkins, J.J.; Harper, J.; et al. Carboplatin/ifosfamide window therapy for osteosarcoma: Results of the St Jude Children’s Research Hospital os-91 Trial. J. Clin. Oncol. 2001, 19, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, A.; Ryan, A.L.; Gibson, P.; Hendershot, E.; Hopyan, S.; Ranson, M.; Stimec, J.; Gupta, A.A. Radiological assessment and outcome of local disease progression after neoadjuvant chemotherapy in children and adolescents with localized osteosarcoma. J. Clin. Med. 2020, 9, 4070. [Google Scholar] [CrossRef]
- Corre, I.; Verrecchia, F.; Crenn, V.; Redini, F.; Trichet, V. The Osteosarcoma Microenvironment: A Complex But Targetable Ecosystem. Cells 2020, 9, 976. [Google Scholar] [CrossRef] [PubMed]
- Luca, A.C.; Miron, I.C.; Trandafir, L.M.; Cojocaru, E.; Pădureţ, I.A.; Trandafirescu, M.F.; Iordache, A.C.; Ţarcă, E. Morphological, genetic and clinical correlations in infantile hemangiomas and their mimics. Rom. J. Morphol. Embryol. 2020, 61, 687–695. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gill, J.; Gorlick, R. Advancing therapy for osteosarcoma. Nat. Rev. Clin. Oncol. 2021, 18, 609–624. [Google Scholar] [CrossRef] [PubMed]
- Stătescu, L.; Trandafir, L.M.; Țarcă, E.; Moscalu, M.; Leon Constantin, M.M.; Butnariu, L.I.; Trandafirescu, M.F.; Tîrnovanu, M.C.; Heredea, R.; Pătrașcu, A.V.; et al. Advancing Cancer Research: Current Knowledge on Cutaneous Neoplasia. Int. J. Mol. Sci. 2023, 24, 11176. [Google Scholar] [CrossRef] [PubMed]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current Treatment and a Collaborative Pathway to Success. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No. of Cases | Min | Max | Median Age (Years) | Q25 | Q75 | |
|---|---|---|---|---|---|---|---|
| Total | 65 | 4.0 | 18.0 | 13.0 | 10.0 | 16.0 | |
| Gender (p = 0.436) | Male (63.1%) | 41 | 4.0 | 18.0 | 13.0 | 11.0 | 16.0 |
| Female (36.9%) | 24 | 5.0 | 18.0 | 12.5 | 9.5 | 16.0 | |
| Social environment (p = 0.395) | Rural (69.2%) | 45 | 5.0 | 18.0 | 13.0 | 11.0 | 16.0 |
| Urban (30.8%) | 20 | 5.0 | 18.0 | 12.0 | 10.0 | 16.0 | |
| No. of Cases | Mean Diameter (cm) | Std. Dev. | p-Value | |
|---|---|---|---|---|
| Total | 65 | 12.3 | 4.3 | - |
| Gender | ||||
| Male (M) | 41 | 12.6 | 4.3 | 0.473 |
| Female (F) | 24 | 11.8 | 4.4 | |
| Age group (child/teenager) | ||||
| <12 years | 27 | 12.7 | 4.5 | 0.529 |
| ≥12 years | 38 | 12.1 | 4.2 | |
| Location of the primary tumour | ||||
| Femur | 35 (12 F + 23 M) | 13.6 | 3.3 | <0.01 |
| Tibia | 17 (8 F + 9 M) | 14.1 | 3.7 | |
| Humerus | 5 (0 F + 5 M) | 6.8 | 1.5 | |
| Clavicle | 3 (2 F + 1 M) | 4.7 | 0.6 | |
| Scapula | 3 (2 F + 1 M) | 7.0 | 2.0 | |
| Pelvis | 1 (0 F + 1 M) | 5.0 | 1.8 | |
| Fibula | 1 (0 F + 1 M) | 12.0 | 2.6 | |
| Total | <12 Years | ≥12 Years | Pearson Chi-Square | ||
|---|---|---|---|---|---|
| No. of Patients | 65 | 27 | 38 | ||
| Location of the primary tumour | Femur | 35 | 14 (51.85%) | 21 (55.26%) | χ2 = 4.183 p = 0.652 |
| Tibia | 17 | 9 (33.33%) | 8 (21.05%) | ||
| Humerus | 5 | 1 (3.70%) | 4 (10.53%) | ||
| Clavicle | 3 | 1 (3.70%) | 2 (5.26%) | ||
| Scapula | 3 | 2 (7.41%) | 1 (2.63%) | ||
| Pelvis | 1 | 0 (0.00%) | 1 (2.63%) | ||
| Fibula | 1 | 0 (0.00%) | 1 (2.63%) | ||
| Histopathological subtype of osteosarcoma | Osteoblastic | 44 | 19 (70.37%) | 25 (65.79%) | χ2 = 0.843 p = 0.839 |
| Chondroblastic | 17 | 7 (25.93%) | 10 (26.32%) | ||
| Pleomorph | 3 | 1 (3.70%) | 2 (5.26%) | ||
| With clear cells | 1 | 0 (0.00%) | 1 (2.63%) | ||
| Tumour grading | High grade | 47 | 17 (70.83%) | 30 (73.17%) | χ2 = 0.731 p = 0.693 |
| Intermediate grade | 17 | 7 (29.17%) | 10 (24.39%) | ||
| Periostal–low grade | 1 | 0 (0.00%) | 1 (2.44%) | ||
| Degree of osteosarcoma differentiation | Well | 8 | 2 (7.41%) | 6 (15.79%) | χ2 = 15.407 p = 0.0015 |
| Moderate | 11 | 6 (22.22%) | 5 (13.16%) | ||
| Poorly | 38 | 11 (40.74%) | 27 (71.05%) | ||
| Undifferentiated | 8 | 8 (29.63%) | 0 (0.00%) | ||
| TNM staging of osteosarcoma | Stage 1 | 7 | 2 (7.41%) | 5 (13.16%) | χ2 = 9.574 p = 0.0367 |
| Stage 2 | 12 | 6 (22.22%) | 6 (15.79%) | ||
| Stage 3 | 19 | 4 (14.81%) | 15 (39.47%) | ||
| Stage 4 | 27 | 15 (55.56%) | 12 (31.58%) | ||
| Variable | Age Group | Mean | SD | p-Value | Normal Values |
|---|---|---|---|---|---|
| Alkaline Phosphatase (U/L) | <12 years | 982.6 | 407.0 | 0.875 | <500 |
| ≥12 years | 998.1 | 377.6 | <420 (Female) <750 (Male) | ||
| Lactate Dehydrogenase (U/L) | <12 years | 612.4 | 246.4 | 0.775 | 157–272 |
| ≥12 years | 629.1 | 221.2 | |||
| ESR (mm/h) | <12 years | 67.0 | 25.1 | 0.727 | 18–48 |
| ≥12 years | 69.3 | 25.8 | |||
| Neutrophils (No/µL) | <12 years | 795.9 | 294.8 | 0.035 (*) | 13.000–38.000 |
| ≥12 years | 929.3 | 318.5 | |||
| Lymphocytes (No/µL) | <12 years | 718.3 | 370.3 | 0.437 | 3000–9500 |
| ≥12 years | 789.2 | 353.5 | |||
| Platelets (No/µL) | <12 years | 67.8 | 15.8 | 0.759 | 150.000–450.000 |
| ≥12 years | 69.1 | 17.5 |
| Multiple Regression | B | SE | Wald | Sig. p | Odd Ratio Exp(β) | 95% CI for Exp(B) | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Age | 2.654 | 0.002 | 1.231 | 0.1241 | 0.538 | 0.587 | 5.819 |
| Gender | 5.537 | 0.271 | 0.847 | 0.7982 | 0.087 | 0.682 | 9.008 |
| Location | 7.004 | 0.679 | 2.833 | 0.0931 | 1.007 | 0.271 | 3.965 |
| Tumoural Grading | 3.541 | 0.167 | 18.65 | 0.0268 * | 2.879 | 1.869 | 6.379 |
| Histological Subtype | 8.576 | 0.105 | 19.74 | 0.0187 * | 3.544 | 1.886 | 5.871 |
| TNM Stage | 6.241 | 0.217 | 21.61 | 0.0042 * | 5.973 | 2.671 | 9.822 |
| Constant | 2.844 | 0.194 | 1.69 | 0.0256 | 1.520 | 1.279 | 6.774 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivan, A.; Cojocaru, E.; Sirbu, P.D.; Al Namat, D.R.; Tîrnovanu, Ș.D.; Butnariu, L.I.; Bernic, J.; Bernic, V.; Țarcă, E. Clinical and Pathological Profile of Children and Adolescents with Osteosarcoma. Diagnostics 2025, 15, 266. https://doi.org/10.3390/diagnostics15030266
Ivan A, Cojocaru E, Sirbu PD, Al Namat DR, Tîrnovanu ȘD, Butnariu LI, Bernic J, Bernic V, Țarcă E. Clinical and Pathological Profile of Children and Adolescents with Osteosarcoma. Diagnostics. 2025; 15(3):266. https://doi.org/10.3390/diagnostics15030266
Chicago/Turabian StyleIvan, Andrei, Elena Cojocaru, Paul Dan Sirbu, Dina Roșca Al Namat, Ștefan Dragoș Tîrnovanu, Lăcrămioara Ionela Butnariu, Jana Bernic, Valentin Bernic, and Elena Țarcă. 2025. "Clinical and Pathological Profile of Children and Adolescents with Osteosarcoma" Diagnostics 15, no. 3: 266. https://doi.org/10.3390/diagnostics15030266
APA StyleIvan, A., Cojocaru, E., Sirbu, P. D., Al Namat, D. R., Tîrnovanu, Ș. D., Butnariu, L. I., Bernic, J., Bernic, V., & Țarcă, E. (2025). Clinical and Pathological Profile of Children and Adolescents with Osteosarcoma. Diagnostics, 15(3), 266. https://doi.org/10.3390/diagnostics15030266