
Quality of Life Assessment After Uterine Artery Embolization in Patients with Fibroids Treated in an Ambulatory Setting



 ,
,
Abstract
1. Introduction
2. Materials and Methods
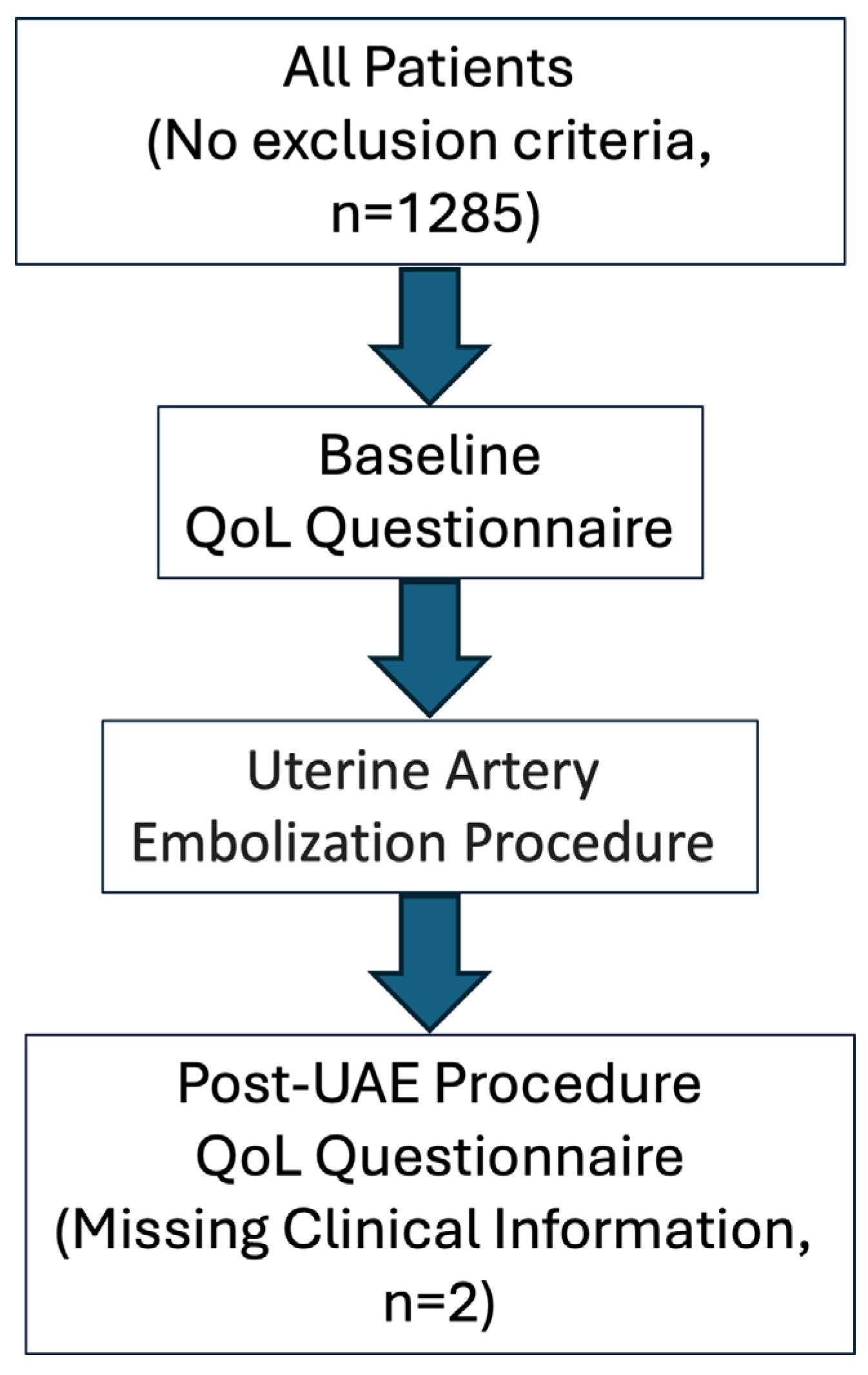
2.1. Study Design and Patient Population
2.2. Assessment of Quality of Life
2.3. Clinical and Imaging Evaluation and Uterine Artery Embolization Protocol
2.4. Statistical Analysis
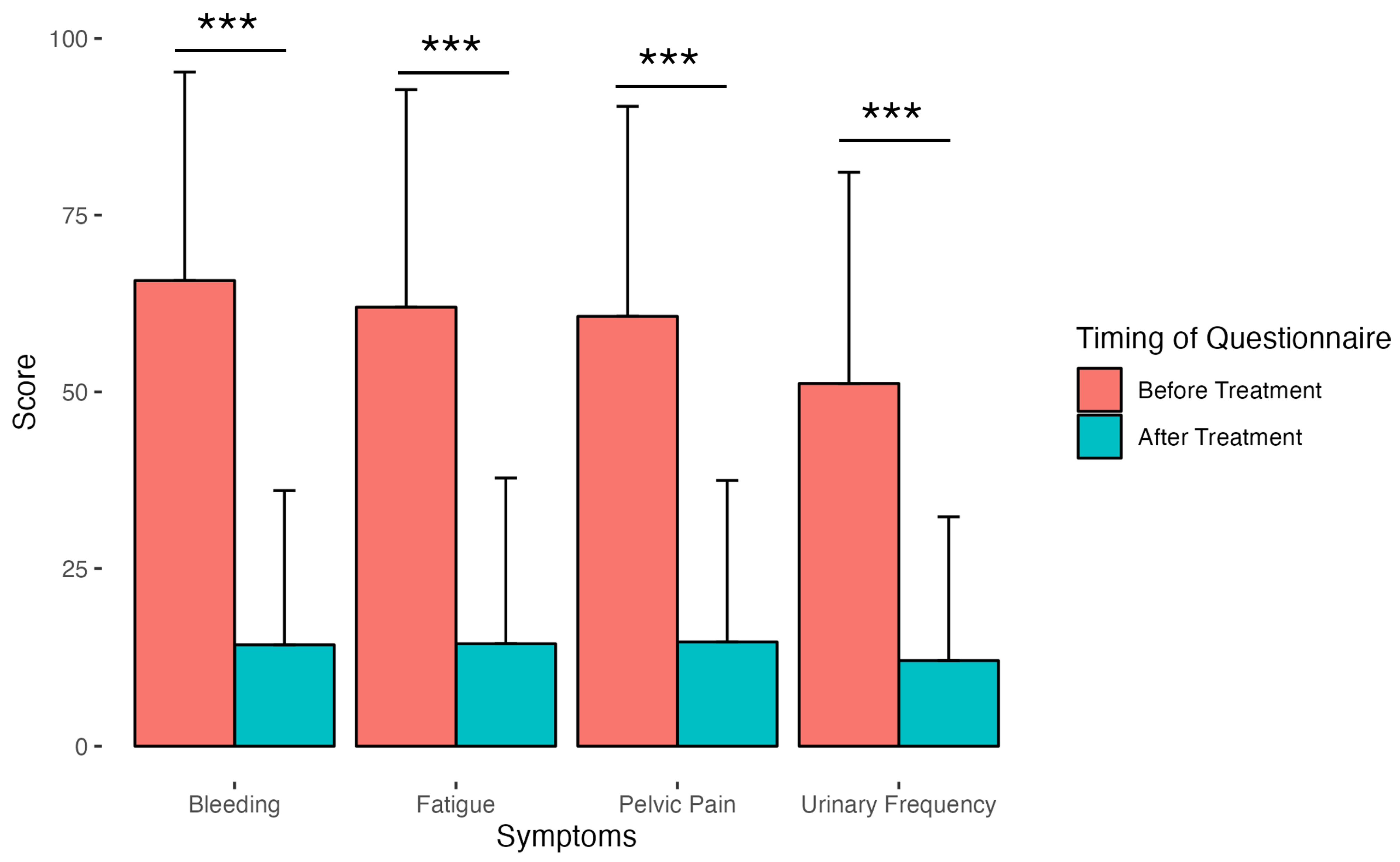
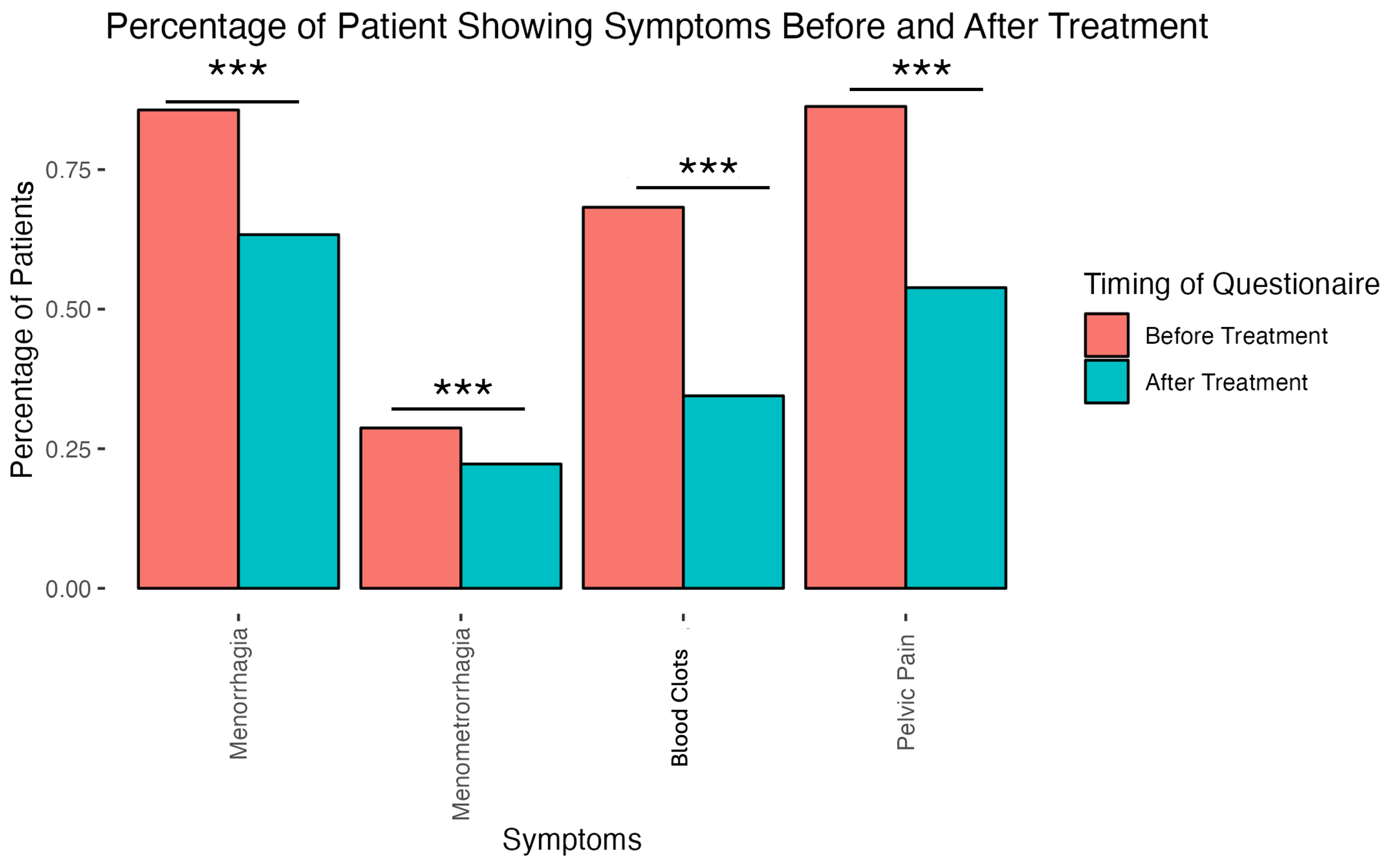
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drayer, S.M.; Catherino, W.H. Prevalence, morbidity, and current medical management of uterine leiomyomas. Int. J. Gynaecol. Obstet. 2015, 131, 117–122. [Google Scholar] [CrossRef]
- Stewart, E.A.; Cookson, C.; Gandolfo, R.A.; Schulze-Rath, R. Epidemiology of uterine fibroids: A systematic review. BJOG 2017, 124, 1501–1512. [Google Scholar] [CrossRef] [PubMed]
- Stewart, E.A.; Laughlin-Tommaso, S.K.; Catherino, W.H.; Lalitkumar, S.; Gupta, D.; Vollenhoven, B. Uterine fibroids. Nat. Rev. Dis. Primers 2016, 2, 16043. [Google Scholar] [CrossRef] [PubMed]
- Baird, D.D.; Dunson, D.B.; Hill, M.C.; Cousins, D.; Schectman, J.M. High cumulative incidence of uterine leiomyoma in black and white women: Ultrasound evidence. Am. J. Obstet. Gynecol. 2003, 188, 100–107. [Google Scholar] [CrossRef]
- Bartels, C.B.; Cayton, K.C.; Chuong, F.S.; Holthouser, K.; Mehr, S.A.; Abraham, T.; Segars, J.H. An evidence-based approach to the medical management of fibroids: A systematic review. Clin. Obstet. Gynecol. 2016, 59, 30–52. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.T.; Shehmar, M.; Gupta, J.K. Uterine fibroids: Current perspectives. Int. J. Womens Health 2014, 6, 95–114. [Google Scholar] [CrossRef]
- Ghant, M.S.; Sengoba, K.S.; Vogelzang, R.; Lawson, A.K.; Marsh, E.E. An altered perception of normal: Understanding causes for treatment delay in women with symptomatic uterine fibroids. J. Womens Health 2016, 25, 846–852. [Google Scholar] [CrossRef]
- Marsh, E.E.; Brocks, M.E.; Ghant, M.S.; Recht, H.S.; Simon, M. Prevalence and knowledge of heavy menstrual bleeding among African American women. Int. J. Gynaecol. Obstet. 2014, 125, 56–59. [Google Scholar] [CrossRef]
- Ekpo, G.E.; Ghant, M.S.; Woodley, L.M.; Recht, H.S.; McKnight, T.; Marsh, E.E. Knowledge of uterine fibroid symptoms and presentation among African-American women: A pilot study. J. Reprod. Med. 2014, 59, 448–454. [Google Scholar] [PubMed]
- Borah, B.J.; Nicholson, W.K.; Bradley, L.; Stewart, E.A. The impact of uterine leiomyomas: A national survey of affected women. Am. J. Obstet. Gynecol. 2013, 209, 319.e311–319.e320. [Google Scholar] [CrossRef]
- Spies, J.B. Current evidence on uterine embolization for fibroids. Semin. Intervent. Radiol. 2013, 4, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Spies, J.B. Current role of uterine artery embolization in the management of uterine fibroids. Clin. Obstet. Gynecol. 2016, 1, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Spies, J.B.; Cornell, C.; Worthington-Kirsch, R.; Lipman, J.C.; Benenati, J.F. Long-term outcome from uterine fibroid embolization with tris-acryl gelatin microspheres: Results of a multicenter study. J. Vasc. Interv. Radiol. 2007, 18, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.K.; Sinha, A.; Lumsden, M.A.; Hickey, M. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst. Rev. 2014, CD005073. [Google Scholar] [CrossRef]
- Spies, J.B.; Coyne, K.; Guaou Guaou, N.; Boyle, D.; Skyrnarz-Murphy, K.; Gonzalves, S.M. The UFS-QOL, a new disease specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet. Gynecol. 2002, 99, 290–300. [Google Scholar]
- Coyne, K.S.; Soliman, A.M.; Margolis, M.K.; Thompson, C.L.; Chwalisz, K. Validation of the 4 week recall version of the Uterine Fibroid Symptom and Health-related Quality of Life (UFS-QOL) Questionnaire. Curr. Med. Res. Opin. 2017, 33, 193–200. [Google Scholar] [CrossRef]
- Spies, J.B.; Bradley, L.D.; Guido, R.; Maxwell, G.L.; Levine, B.A.; Coyne, K. Outcomes from leiomyoma therapies: Comparison with normal controls. Obstet. Gynecol. 2010, 116, 641–652. [Google Scholar] [CrossRef]
- Kohi, M.P.; Spies, J.B. Updates on Uterine Artery Embolization. Semin. Intervent. Radiol. 2018, 35, 48–55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Melton, J.; Ferguson, M. OBL, ASC, or Hybrid: Which model Is right for you? Endovasc. Today 2021, 20, 6. [Google Scholar]
- Nicholson, W.K.; Wegienka, G.; Zhang, S.; Wallace, K.; Stewart, E.; Laughlin-Tommaso, S.; Thomas, L.; Jacoby, V.L.; Marsh, E.E.; Wise, L.; et al. Short-term health-related quality of life after hysterectomy compared with myomectomy for symptomatic leiomyomas. Obstet. Gynecol. 2019, 134, 261–269. [Google Scholar] [CrossRef]
- Anchan, R.M.; Wojdyla, D.; Bortoletto, P.; Terry, K.; Disler, E.; Milne, A.; Gargiulo, A.; Petrozza, J.; Brook, O.; Srouji, S.; et al. A Comparative Analysis of Health-Related Quality of Life 1 Year Following Myomectomy or Uterine Artery Embolization: Findings from the COMPARE-UF Registry. J. Womens Health 2023, 32, 423–433. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Anchan, R.M.; Spies, J.B.; Zhang, S.; Wojdyla, D.; Bortoletto, P.; Terry, K.; Disler, E.; Milne, A.; Gargiulo, A.; Petrozza, J.; et al. Long-term health-related quality of life and symptom severity following hysterectomy, myomectomy, or uterine artery embolization for the treatment of symptomatic uterine fibroids. Am. J. Obstet. Gynecol. 2023, 229, 275.e1–275.e17. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: London, UK, 2013. [Google Scholar]
- Madueke-Laveaux, O.S.; Elsharoud, A.; Al-Hendy, A. What we know about the long-term risks of hysterectomy for benign indication—A systematic review. J. Clin. Med. 2021, 10, 5335. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | ||||
| All Ages | <45 | 45–55 | >55 | |
| Sample No | 1284 | 721 | 513 | 50 |
| Mean Age | 44.48 | 39.81 | 49.22 | 58.54 |
| Laterality of Fibroids | ||||
| Bilateral | 207 | 114 | 87 | 6 |
| Unilateral | 1004 | 564 | 399 | 40 |
| Type of Fibroids | ||||
| Intramural | 596 | 331 | 242 | 23 |
| Submucosal | 217 | 138 | 77 | 2 |
| Subserosal | 392 | 205 | 166 | 20 |
| Location of Fibroids | ||||
| Body | 818 | 471 | 318 | 28 |
| Cervix | 24 | 14 | 7 | 3 |
| Fundus | 368 | 192 | 161 | 15 |
| Patient Group | ||||
| Mean Volume | 184.84 | 181.27 | 189.52 | 186.12 |
| Sd Volume | 84.73 | 88.37 | 79.80 | 81.47 |
| Arterial Access Site (Approach) | ||||
| Femoral | 628 | 366 | 244 | 17 |
| Radial | 348 | 187 | 148 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geschwind, J.-F.; Afsari, B.; Nezami, N.; White, J.; Shor, M.; Katsnelson, Y. Quality of Life Assessment After Uterine Artery Embolization in Patients with Fibroids Treated in an Ambulatory Setting. Diagnostics 2025, 15, 739. https://doi.org/10.3390/diagnostics15060739
Geschwind J-F, Afsari B, Nezami N, White J, Shor M, Katsnelson Y. Quality of Life Assessment After Uterine Artery Embolization in Patients with Fibroids Treated in an Ambulatory Setting. Diagnostics. 2025; 15(6):739. https://doi.org/10.3390/diagnostics15060739
Chicago/Turabian StyleGeschwind, Jean-Francois, Bahman Afsari, Nariman Nezami, Jacob White, Michael Shor, and Yan Katsnelson. 2025. "Quality of Life Assessment After Uterine Artery Embolization in Patients with Fibroids Treated in an Ambulatory Setting" Diagnostics 15, no. 6: 739. https://doi.org/10.3390/diagnostics15060739
APA StyleGeschwind, J.-F., Afsari, B., Nezami, N., White, J., Shor, M., & Katsnelson, Y. (2025). Quality of Life Assessment After Uterine Artery Embolization in Patients with Fibroids Treated in an Ambulatory Setting. Diagnostics, 15(6), 739. https://doi.org/10.3390/diagnostics15060739