
Utility of a Card-Type Respiratory Rate Measuring Device for Spontaneously Breathing Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Card-Type Device
2.2. Study Protocol
3. Results
3.1. Respiratory Rate
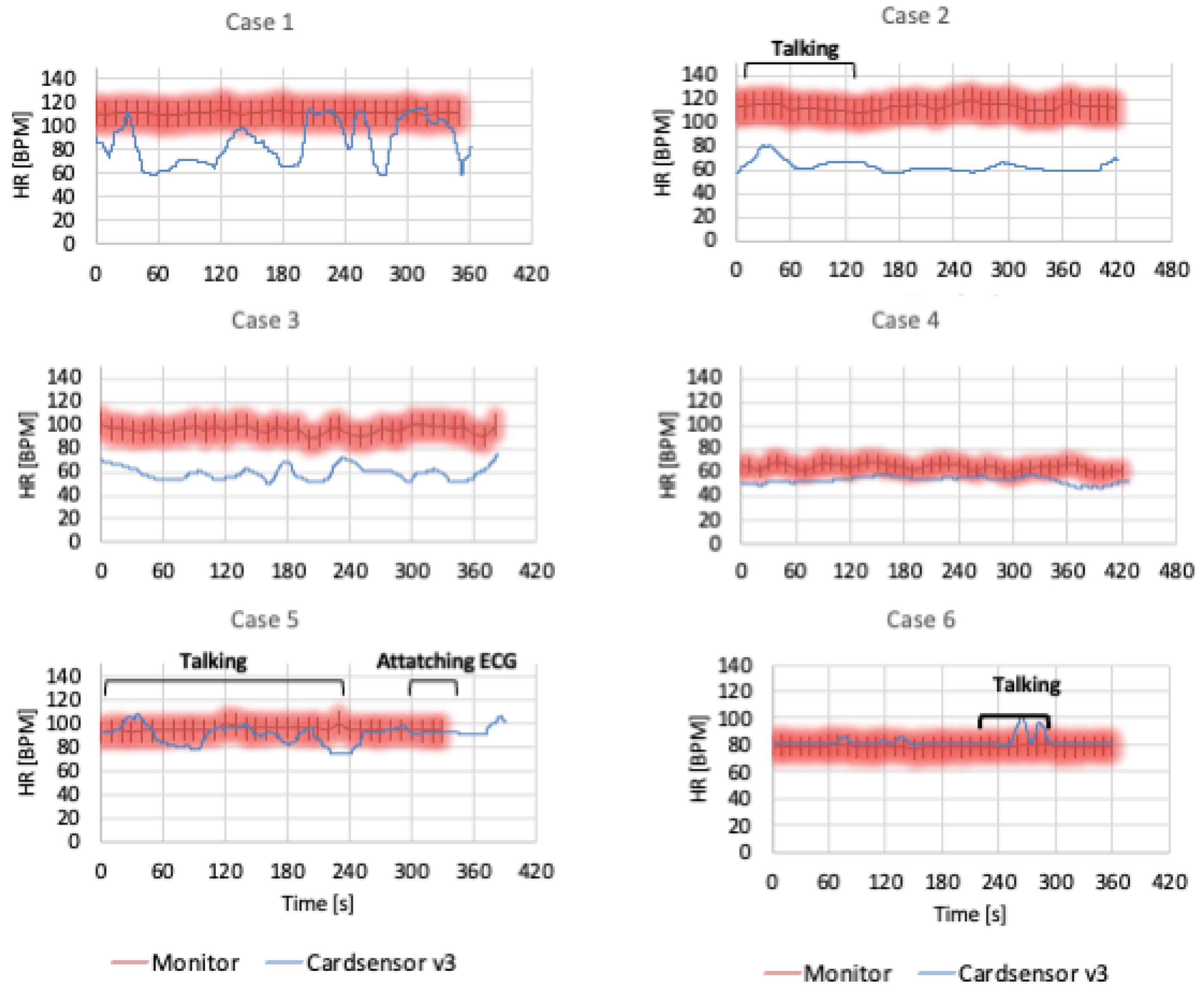
3.2. Heart Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| RRS | rapid response system |
| RR | respiratory rate |
| HR | heart rate |
| BMI | body mass index |
| NPPV | non-invasive positive pressure ventilation |
References
- Shappell, C.; Snyder, A.; Edelson, D.P.; Churpek, M.M. American Heart Association’s Get With The Guidelines-Resuscitation Investigators: Predictors of in-hospital mortality after rapid response team calls in a 274 hospital nationwide sample. Crit. Care Med. 2018, 46, 1041–1048. [Google Scholar] [CrossRef]
- Okawa, R.; Yokono, T.; Koyama, Y.; Uchiyama, M.; Oono, N. Clinical sign-based rapid response team call criteria for identifying patients requiring intensive care management in Japan. Medicina 2021, 57, 1194. [Google Scholar] [CrossRef] [PubMed]
- Fieselmann, J.F.; Hendryx, M.S.; Helms, C.M.; Wakefield, D.S. Respiratory rate predicts cardiopulmonary arrest for internal medicine inpatients. J. Gen. Intern. Med. 1993, 8, 354–360. [Google Scholar] [CrossRef]
- Elliott, M.; Baird, J. Pulse oximetry and the enduring neglect of respiratory rate assessment: A commentary on patient surveillance. Br. J. Nurs. 2019, 28, 1256–1259. [Google Scholar] [CrossRef] [PubMed]
- Flenady, T.; Dwyer, T.; Applegarth, J. Accurate respiratory rates count: So should you! Australas. Emerg. Nurs. J. 2017, 20, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory rate: The neglected vital sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar]
- Harry, M.L.; Heger, A.M.C.; Woehrle, T.A.; Kitch, L.A. Understanding respiratory rate assessment by emergency nurses: A health care improvement project. J. Emerg. Nurs. 2020, 46, 488–496. [Google Scholar] [CrossRef]
- Dresser, S.; Teel, C.; Peltzer, J. Frontline Nurses’ clinical judgment in recognizing, understanding, and responding to patient deterioration: A qualitative study. Int. J. Nurs. Stud. 2023, 139, 104436. [Google Scholar]
- Iwashita, Y.; Nebuya, S. Evaluation of a novel contactless electrical impedance device for measuring respiratory and heart rates: A pilot study. Cureus 2021, 13, e18622. [Google Scholar] [CrossRef]
- Vincent, C.; Neale, G.; Woloshynowych, M. Adverse events in British hospitals: Preliminary retrospective record review. BMJ 2001, 322, 517–519. [Google Scholar]
- Halfon, P.; Staines, A.; Burnand, B. Adverse events related to hospital care: A retrospective medical records review in a Swiss hospital. Int. J. Qual. Health Care 2017, 29, 527–533. [Google Scholar] [PubMed]
- Baker, G.R.; Norton, P.G.; Flintoft, V.; Blais, R.; Brown, A.; Cox, J.; Tamblyn, R. The Canadian Adverse Events Study: The incidence of adverse events among hospital patients in Canada. CMAJ 2004, 170, 1678–1686. [Google Scholar] [PubMed]
- Subbe, C.; Davies, R.G.; Williams, E.; Rutherford, P.; Gemmell, L. Effect of introducing the Modified Early Warning score on clinical outcomes, cardio-pulmonary arrests and intensive care utilisation in acute medical admissions. Anaesthesia 2003, 58, 797–802. [Google Scholar] [CrossRef]
- Kim, L.; Yun, K.S.; Park, J.D.; Lee, B. Effect of Diurnal Variation of Heart Rate and Respiratory Rate on Activation of Rapid Response System and Clinical Outcome in Hospitalized Children. Children 2023, 10, 167. [Google Scholar] [CrossRef]
- Naito, T.; Hayashi, K.; Hsu, H.C.; Aoki, K.; Nagata, K.; Arai, M.; Nakada, T.A.; Suzaki, S.; Hayashi, Y.; Fujitani, S.; et al. Validation of National Early Warning Score for predicting 30-day mortality after rapid response system activation in Japan. Acute Med. Surg. 2021, 8, e666. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Pack, E.; Cambiano, V.; Rollmann, H.; Weil, S.; O’Beirne, J. The accuracy of respiratory rate assessment by doctors in a London teaching hospital: A cross-sectional study. J. Clin. Monit. Comput. 2015, 29, 455–460. [Google Scholar] [CrossRef]
- Brabrand, M.; Hallas, P.; Folkestad, L.; Lautrup-Larsen, C.H.; Brodersen, J.B. Measurement of respiratory rate by multiple raters in a clinical setting is unreliable: A cross-sectional simulation study. J. Crit. Care. 2018, 44, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, L.G.; Folkestad, L.; Brodersen, J.B.; Brabrand, M. Inter-observer agreement in measuring respiratory rate. PLoS ONE 2015, 10, e0129493. [Google Scholar] [CrossRef]
- Takaki, S.; Hara, K.; Motoyama, A.; Kawana, Y.; Kuroki, M.; Sasaki, S. A multi-nudge-based behavioural insight into ward nurses’ respiratory rate measurement: An observational study. J. Clin. Nurs. 2025, 34, 805–815. [Google Scholar] [CrossRef]
- Van Loon, K.; van Zaane, B.; Bosch, E.J.; Kalkman, C.J.; Peelen, L.M. Non-invasive continuous respiratory monitoring on general hospital wards: A systematic review. PLoS ONE 2015, 10, e0144626. [Google Scholar] [CrossRef]
- Wei, J.C.; van den Broek, T.J.; van Baardewijk, J.U.; van Stokkum, R.; Kamstra, R.J.; Rikken, L.; van den Brink, W.J. Validation and user experience of a dry electrode based Health Patch for heart rate and respiration rate monitoring. Sci. Rep. 2024, 14, 23098. [Google Scholar] [CrossRef]
- Takahashi, Y.; Okura, K.; Minakata, S.; Watanabe, M.; Hatakeyama, K.; Chida, S.; Shimada, Y. Accuracy of heart rate and respiratory rate measurements using two types of wearable devices. Prog. Rehabil. Med. 2022, 7, 20220016. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.; Zhou, M.; Bian, D.; Mehta, P.; Shah, M.; Rajput, K.S.; Selvaraj, N. Novel Continuous Respiratory Rate Monitoring Using an Armband Wearable Sensor. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2021, 2021, 7470–7475. [Google Scholar] [CrossRef]
- Bujan, B.; Fischer, T.; Dietz-Terjung, S.; Bauerfeind, A.; Jedrysiak, P.; Große Sundrup, M.; Schöbel, C. Clinical validation of a contactless respiration rate monitor. Sci. Rep. 2023, 13, 3480. [Google Scholar] [CrossRef]
- Lauteslager, T.; Maslik, M.; Siddiqui, F.; Marfani, S.; Leschziner, G.D.; Williams, A.J. Validation of a New Contactless and Continuous Respiratory Rate Monitoring Device Based on Ultra-Wideband Radar Technology. Sensors 2021, 21, 4027. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, K.K.G.; Della Monica, C.; Atzori, G.; Lambert, D.; Hassanin, H.; Revell, V.; Dijk, D.J. Reliable Contactless Monitoring of Heart Rate, Breathing Rate, and Breathing Disturbance During Sleep in Aging: Digital Health Technology Evaluation Study. JMIR Mhealth Uhealth 2024, 12, e53643. [Google Scholar] [CrossRef]
- Do, W.; Russell, R.; Wheeler, C.; Lockwood, M.; De Vos, M.; Pavord, I.; Bafadhel, M. Performance of Contactless Respiratory Rate Monitoring by Albus HomeTM, an Automated System for Nocturnal Monitoring at Home: A Validation Study. Sensors 2022, 22, 7142. [Google Scholar] [CrossRef]
- Collyer, S.; Davis, P.J. Effect of facemask use on respiratory patterns of women in speech and singing. J. Speech Lang. Hear. Res. 2006, 49, 412–423. [Google Scholar] [CrossRef]
- Loudon, R.G.; Lee, L.; Holcomb, B.J. Volumes and breathing patterns during speech in healthy and asthmatic subjects. J. Speech Hear. Res. 1988, 31, 219–227. [Google Scholar] [CrossRef]
- Lee, L.; Loudon, R.G.; Jacobson, B.H.; Stuebing, R. Speech breathing in patients with lung disease. Am. Rev. Respir. Dis. 1993, 147, 1199–1206. [Google Scholar] [CrossRef]
- Lind, F.G. Respiratory drive and breathing pattern during exercise in man. Acta Physiol. Scand. Suppl. 1984, 533, 1–47. [Google Scholar] [PubMed]
- Van Meerhaeghe, A.; Scano, G.; Sergysels, R.; Bran, M.; De Coster, A. Respiratory drive and ventilatory pattern during exercise in interstitial lung disease. Bull. Eur. Physiopathol. Respir. 1981, 17, 15–26. [Google Scholar] [PubMed]
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Van Heerden, D.; Luan, H.; Cullen, K.; et al. Reliability and Validity of Commercially Available Wearable Devices for Measuring Steps, Energy Expenditure, and Heart Rate: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e18694. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Age | Sex | Height (cm) | Weight (kg) | BMI | Diagnosis | |
|---|---|---|---|---|---|---|
| 1 | 61 | F | 155 | 40.8 | 17 | Pneumonia, on NPPV |
| 2 | 38 | F | 166 | 70 | 25 | Left tubal pyosalpinx |
| 3 | 97 | F | 145 | 42 | 20 | Right femur fracture |
| 4 | 83 | M | 157 | 66.4 | 27 | Renal failure, pulmonary edema, on NPPV |
| 5 | 78 | M | 154 | 54.3 | 23 | Esophageal stricture |
| 6 | 70 | M | 167 | 70 | 25 | Lung cancer |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwashita, Y.; Takeda, S.; Kawashima, S.; Sato, S.; Nebuya, S. Utility of a Card-Type Respiratory Rate Measuring Device for Spontaneously Breathing Patients. Diagnostics 2025, 15, 864. https://doi.org/10.3390/diagnostics15070864
Iwashita Y, Takeda S, Kawashima S, Sato S, Nebuya S. Utility of a Card-Type Respiratory Rate Measuring Device for Spontaneously Breathing Patients. Diagnostics. 2025; 15(7):864. https://doi.org/10.3390/diagnostics15070864
Chicago/Turabian StyleIwashita, Yoshiaki, Shun Takeda, Satoshi Kawashima, Shinya Sato, and Satoru Nebuya. 2025. "Utility of a Card-Type Respiratory Rate Measuring Device for Spontaneously Breathing Patients" Diagnostics 15, no. 7: 864. https://doi.org/10.3390/diagnostics15070864
APA StyleIwashita, Y., Takeda, S., Kawashima, S., Sato, S., & Nebuya, S. (2025). Utility of a Card-Type Respiratory Rate Measuring Device for Spontaneously Breathing Patients. Diagnostics, 15(7), 864. https://doi.org/10.3390/diagnostics15070864