Radiogenomics and Radiomics in Liver Cancers

 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Discussion
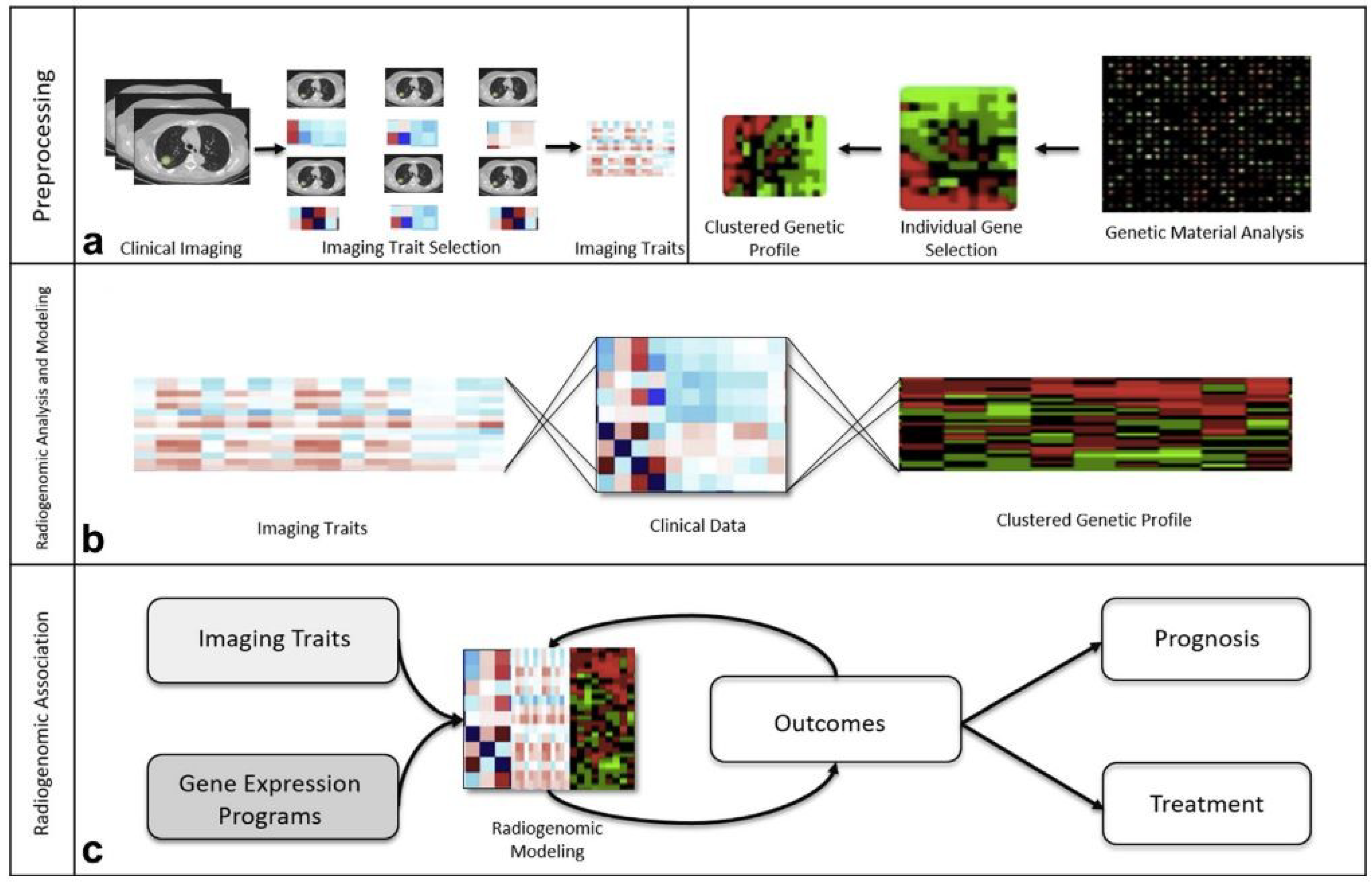
2.1. Radiogenomics in Liver Cancers
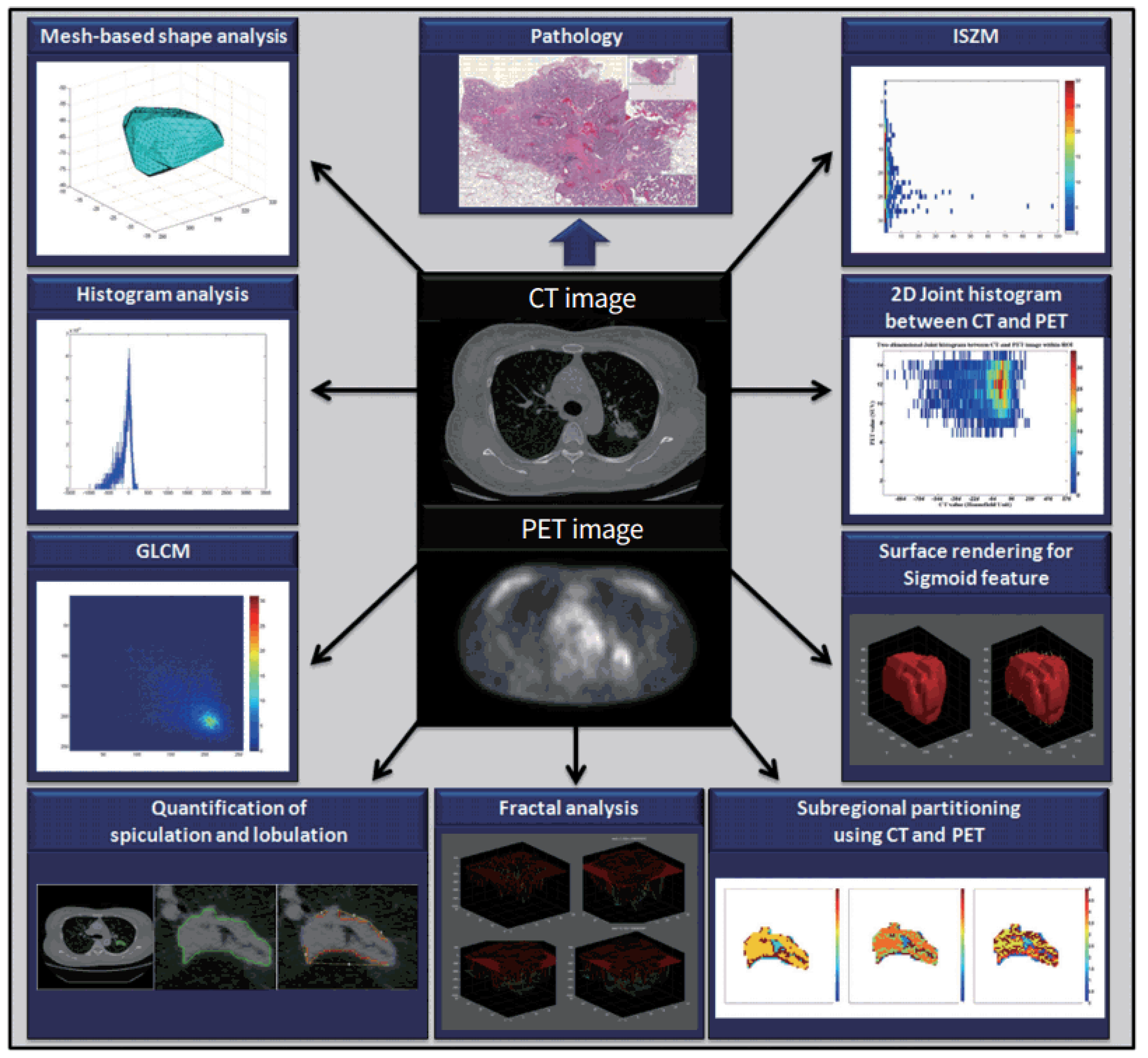
2.2. Radiomics in Liver Cancers
2.2.1. Radiomics in HCC
2.2.2. Radiomics in ICC
2.2.3. Radiomics in Liver Metastases
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, R.L.; Zhu, A.X.; Oklu, R. Hepatocellular Carcinoma: Can Circulating Tumor Cells and Radiogenomics Deliver Personalized Care? Am. J. Clin. Oncol. 2015, 38, 431–436. [Google Scholar] [CrossRef]
- Pinker, K.; Shitano, F.; Sala, E.; Do, R.K.; Young, R.J.; Wibmer, A.G.; Hricak, H.; Sutton, E.J.; Morris, E.A. Background, Current Role, and Potential Applications of Radiogenomics. J. Magn. Reson. Imaging 2018, 47, 604–620. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.; Bui, K.; Hernandez Rangel, E.; Nguyentat, M.; Fernando, D.; Nelson, K.; Abi-Jaoudeh, N. Radiogenomics and IR. J. Vasc. Interv. Radiol. 2018, 29, 706–713. [Google Scholar] [CrossRef] [PubMed]
- Segal, E.; Sirlin, C.B.; Ooi, C.; Adler, A.S.; Gollub, J.; Chen, X.; Chan, B.K.; Matcuk, G.R.; Barry, C.T.; Chang, H.Y.; et al. Decoding Global Gene Expression Programs in Liver Cancer by Noninvasive Imaging. Nat. Biotechnol. 2007, 25, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.D.; Gollub, J.; Sirlin, C.B.; Ooi, C.; Chen, X. Radiogenomic Analysis to Identify Imaging Phenotypes Associated with Drug Response Gene Expression Programs in Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2007, 18, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Wang, D.S.; Kim, H.J.; Sirlin, C.B.; Chan, M.G.; Korn, R.L.; Rutman, A.M.; Siripongsakun, S.; Lu, D.; Imanbayev, G.; et al. A Computed Tomography Radiogenomic Biomarker Predicts Microvascular Invasion and Clinical Outcomes in Hepatocellular Carcinoma. Hepatology 2015, 62, 792–800. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Brocchi, S.; Cucchetti, A.; Mazzotti, F.; Mosconi, C.; Sportoletti, C.; Brandi, G.; Pinna, A.D.; Golfieri, R. Can Current Preoperative Imaging Be Used to Detect Microvascular Invasion of Hepatocellular Carcinoma? Radiology 2016, 279, 432–442. [Google Scholar] [CrossRef]
- Taouli, B.; Hoshida, Y.; Kakite, S.; Chen, X.; Tan, P.S.; Sun, X.; Kihira, S.; Kojima, K.; Toffanin, S.; Fiel, M.I.; et al. Imaging-Based Surrogate Markers of Transcriptome Subclasses and Signatures in Hepatocellular Carcinoma: Preliminary Results. Eur. Radiol. 2017, 27, 4472–4481. [Google Scholar] [CrossRef]
- Miura, T.; Ban, D.; Tanaka, S.; Mogushi, K.; Kudo, A.; Matsumura, S.; Mitsunori, Y.; Ochiai, T.; Tanaka, H.; Tanabe, M. Distinct Clinicopathological Phenotype of Hepatocellular Carcinoma with Ethoxybenzyl-Magnetic Resonance Imaging Hyperintensity: Association with Gene Expression Signature. Am. J. Surg. 2015, 210, 561–569. [Google Scholar] [CrossRef]
- Kitao, A.; Matsui, O.; Yoneda, N.; Kozaka, K.; Kobayashi, S.; Sanada, J.; Koda, W.; Minami, T.; Inoue, D.; Yoshida, K.; et al. Hepatocellular Carcinoma with β-Catenin Mutation: Imaging and Pathologic Characteristics. Radiology 2015, 275, 141315. [Google Scholar] [CrossRef] [PubMed]
- Hectors, S.J.; Wagner, M.; Bane, O.; Besa, C.; Lewis, S.; Remark, R.; Chen, N.; Fiel, M.I.; Zhu, H.; Gnjatic, S.; et al. Quantification of Hepatocellular Carcinoma Heterogeneity with Multiparametric Magnetic Resonance Imaging. Sci. Rep. 2017, 7, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Sadot, E.; Simpson, A.L.; Do, R.K.G.; Gonen, M.; Shia, J.; Allen, P.J.; D’Angelica, M.I.; DeMatteo, R.P.; Kingham, T.P.; Jarnagin, W.R. Cholangiocarcinoma: Correlation between Molecular Profiling and Imaging Phenotypes. PLoS ONE 2015, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kiryu, S.; Akai, H.; Nojima, M.; Hasegawa, K.; Shinkawa, H. Impact of Hepatocellular Carcinoma Heterogeneity on Computed Tomography as a Prognostic Indicator. Sci. Rep. 2017, 7, 12689. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Chen, Y.; Zhang, R.; Yan, Z.; Zhou, X.; Zhang, B.; Gao, X. Radiogenomics of Hepatocellular Carcinoma: Multiregion Analysis-Based Identification of Prognostic Imaging Biomarkers by Integrating Gene Data—A Preliminary Study. Phys. Med. Biol. 2018, 63. [Google Scholar] [CrossRef] [PubMed]
- Akai, H.; Yasaka, K.; Kunimatsu, A.; Nojima, M.; Kokudo, T.; Kokudo, N.; Hasegawa, K.; Abe, O.; Ohtomo, K.; Kiryu, S. Predicting Prognosis of Resected Hepatocellular Carcinoma by Radiomics Analysis with Random Survival Forest. Diagn. Interv. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Echegaray, S.; Gevaert, O.; Shah, R.; Kamaya, A.; Louie, J.; Kothary, N.; Napel, S. Core Samples for Radiomics Features That Are Insensitive to Tumor Segmentation: Method and Pilot Study Using CT Images of Hepatocellular Carcinoma. J. Med. Imaging 2015, 2, 041011. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; He, L.; Huang, Y.; Chen, S.; Wu, P.; Ye, W.; Liu, Z.; Liang, C. CT-Based Radiomics Signature: A Potential Biomarker for Preoperative Prediction of Early Recurrence in Hepatocellular Carcinoma. Abdom. Radiol. 2017, 42, 1695–1704. [Google Scholar] [CrossRef]
- Lee, G.; Lee, H.Y.; Ko, E.S.; Jeong, W.K. Radiomics and Imaging Genomics in Precision Medicine. Precis. Future Med. 2017, 1, 10–31. [Google Scholar] [CrossRef]
- Wolfort, R.M.; Papillion, P.W.; Turnage, R.H.; Lillien, D.L.; Ramaswamy, M.R.; Zibari, G.B. Role of FDG-PET in the Evaluation and Staging of Hepatocellular Carcinoma with Comparison of Tumor Size, AFP Level, and Histologic Grade. Int. Surg. 2010, 95, 67–75. [Google Scholar]
- Dong, A.; Yu, H.; Wang, Y.; Dong, H.; Zuo, C. FDG PET/CT and Enhanced CT Imaging of Tumor Heterogeneity in Hepatocellular Carcinoma. Clin. Nucl. Med. 2014, 39, 808–810. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Durand, P.; Van Der Gucht, A.; Jreige, M.; Nicod-Lalonde, M.; Silva-Monteiro, M.; Prior, J.O.; Denys, A.; Depeursinge, A.; Schaefer, N. Signature of Survival: A 18 F-FDG PET Based Whole-Liver Radiomic Analysis Predicts Survival after 90 Y-TARE for Hepatocellular Carcinoma. Oncotarget 2018, 9, 4549–4558. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.A.; Lee, J.M.; Lee, K.B.; Kim, S.H.; Yoon, S.H.; Han, J.K.; Choi, B.I. Intrahepatic Mass-Forming Cholangiocarcinomas: Enhancement Patterns at Multiphasic CT, with Special Emphasis on Arterial Enhancement Pattern-Correlation with Clinicopathologic Findings. Radiology 2011, 260, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Fujita, N.; Asayama, Y.; Nishie, A.; Ishigami, K.; Ushijima, Y.; Takayama, Y.; Okamoto, D.; Moirta, K.; Shirabe, K.; Aishima, S.; et al. Mass-Forming Intrahepatic Cholangiocarcinoma: Enhancement Patterns in the Arterial Phase of Dynamic Hepatic CT—Correlation with Clinicopathological Findings. Eur. Radiol. 2017, 27, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Aherne, E.A.; Pak, L.M.; Goldman, D.A.; Gonen, M.; Jarnagin, W.R.; Simpson, A.L.; Do, R.K. Intrahepatic Cholangiocarcinoma: Can Imaging Phenotypes Predict Survival and Tumor Genetics? Abdom. Radiol. 2018, 43, 2665–2672. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, S.; Kang, T. Mass-Forming Intrahepatic Cholangiocarcinoma: Diffusion-Weighted Imaging as a Preoperative Prognostic Marker. Radiology 2016, 281, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Lubner, M.G.; Stabo, N.; Lubner, S.J.; del Rio, A.M.; Song, C.; Halberg, R.B.; Pickhardt, P.J. CT Textural Analysis of Hepatic Metastatic Colorectal Cancer: Pre-Treatment Tumor Heterogeneity Correlates with Pathology and Clinical Outcomes. Abdom. Imaging 2015, 40, 2331–2337. [Google Scholar] [CrossRef] [PubMed]
- Simpson, A.L.; Doussot, A.; Creasy, J.M.; Adams, L.B.; Allen, P.J.; DeMatteo, R.P.; Gönen, M.; Kemeny, N.E.; Kingham, T.P.; Shia, J.; et al. Computed Tomography Image Texture: A Noninvasive Prognostic Marker of Hepatic Recurrence After Hepatectomy for Metastatic Colorectal Cancer. Ann. Surg. Oncol. 2017, 24, 2482–2490. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.S.; Schneider, M.A.; Wurnig, M.C.; Wagner, M.; Clavien, P.A.; Boss, A. Radiomics of Liver MRI Predict Metastases in Mice. Eur. Radiol. Exp. 2018, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.X.; Lambregts, D.M.J.; Schnerr, R.S.; Beckers, R.C.J.; Maas, M.; Albarello, F.; Riedl, R.G.; Dejong, C.H.C.; Martens, M.H.; Heijnen, L.A.; et al. CT Texture Analysis in Colorectal Liver Metastases: A Better Way than Size and Volume Measurements to Assess Response to Chemotherapy? United Eur. Gastroenterol. J. 2016, 4, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Reimer, R.P.; Reimer, P.; Mahnken, A.H. Assessment of Therapy Response to Transarterial Radioembolization for Liver Metastases by Means of Post-Treatment MRI-Based Texture Analysis. Cardiovasc. Intervent. Radiol. 2018, 41, 1545–1556. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saini, A.; Breen, I.; Pershad, Y.; Naidu, S.; Knuttinen, M.G.; Alzubaidi, S.; Sheth, R.; Albadawi, H.; Kuo, M.; Oklu, R. Radiogenomics and Radiomics in Liver Cancers. Diagnostics 2019, 9, 4. https://doi.org/10.3390/diagnostics9010004
Saini A, Breen I, Pershad Y, Naidu S, Knuttinen MG, Alzubaidi S, Sheth R, Albadawi H, Kuo M, Oklu R. Radiogenomics and Radiomics in Liver Cancers. Diagnostics. 2019; 9(1):4. https://doi.org/10.3390/diagnostics9010004
Chicago/Turabian StyleSaini, Aman, Ilana Breen, Yash Pershad, Sailendra Naidu, M. Grace Knuttinen, Sadeer Alzubaidi, Rahul Sheth, Hassan Albadawi, Malia Kuo, and Rahmi Oklu. 2019. "Radiogenomics and Radiomics in Liver Cancers" Diagnostics 9, no. 1: 4. https://doi.org/10.3390/diagnostics9010004
APA StyleSaini, A., Breen, I., Pershad, Y., Naidu, S., Knuttinen, M. G., Alzubaidi, S., Sheth, R., Albadawi, H., Kuo, M., & Oklu, R. (2019). Radiogenomics and Radiomics in Liver Cancers. Diagnostics, 9(1), 4. https://doi.org/10.3390/diagnostics9010004