
Physiotherapy versus Consecutive Physiotherapy and Cognitive Treatment in People with Parkinson’s Disease: A Pilot Randomized Cross-Over Study

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
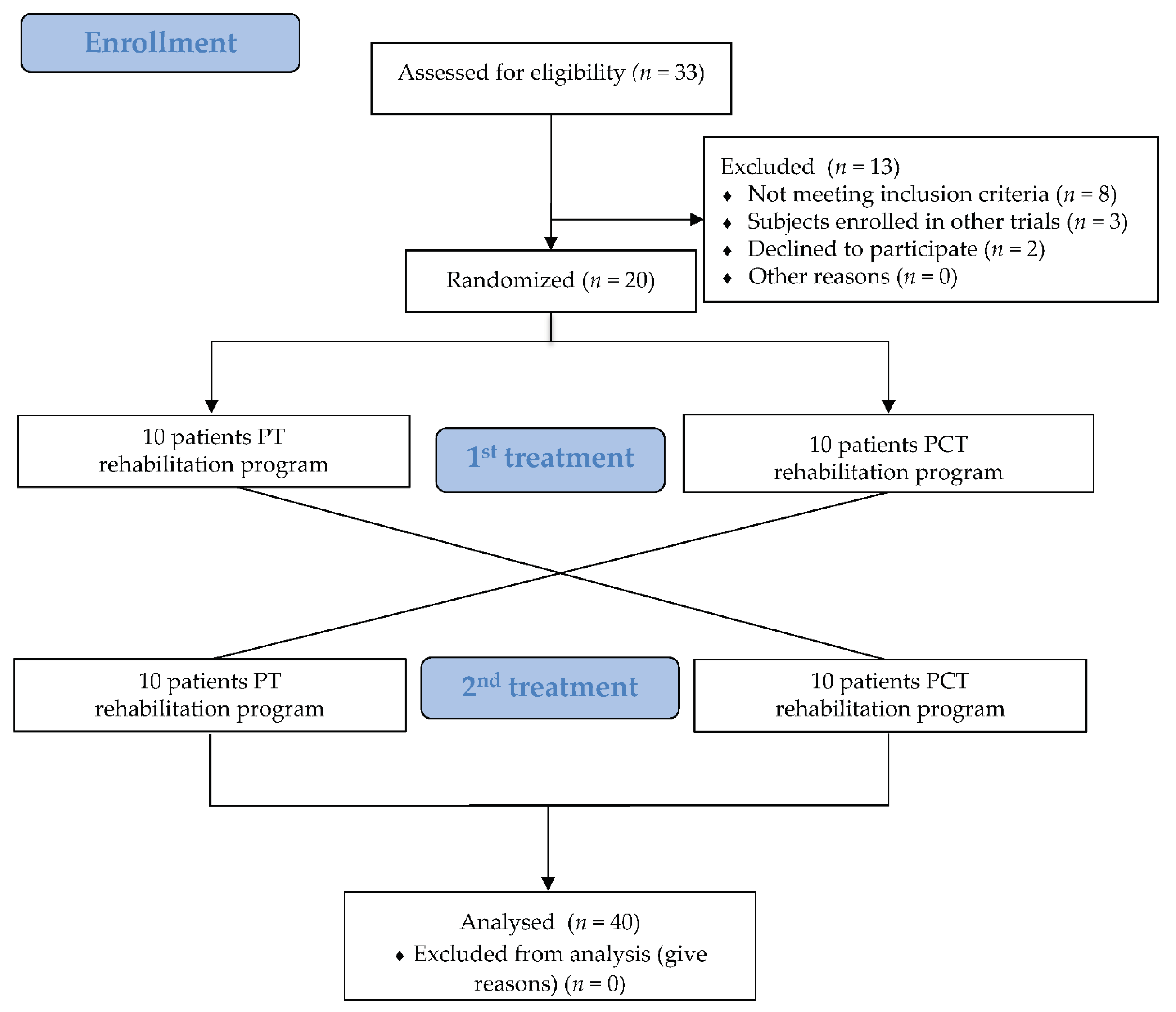
2.1. Study Design
2.2. Ethical Aspects
2.3. Subjects
2.4. Intervention and Procedures
2.5. Data Collection and Assessment Procedures
2.6. Outcome Measures
2.6.1. Primary Outcome Measures
2.6.2. Secondary Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Baseline
3.2. Primary Outcomes
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, Y.X.; Zhao, J.; Li, D.K.; Peng, F.; Wang, Y.; Yang, K.; Liu, Z.Y.; Liu, F.T.; Wu, J.J.; Wang, J. Associations between cognitive impairment and motor dysfunction in Parkinson’s disease. Brain Behav. 2017, 7, e00719. [Google Scholar] [CrossRef]
- Pothakos, K.; Kurz, M.J.; Lau, Y.S. Restorative effect of endurance exercise on behavioral deficits in the chronic mouse model of Parkinson’s disease with severe neurodegeneration. BMC Neurosci. 2009, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Picelli, A.; Camin, M.; Tinazzi, M.; Vangelista, A.; Cosentino, A.; Fiaschi, A.; Smania, N. Three-dimensional motion analysis of the effects of auditory cueing on gait pattern in patients with Parkinson’s disease: A preliminary investigation. Neurol. Sci. 2010, 31, 423–430. [Google Scholar] [CrossRef]
- Muslimović, D.; Post, B.; Speelman, J.D.; Schmand, B. Cognitive profile of patients with newly diagnosed Parkinson disease. Neurology 2005, 65, 1239–1245. [Google Scholar] [CrossRef]
- Uekermann, J.; Daum, I.; Peters, S.; Wiebel, B.; Przuntek, H.; Müller, T. Depressed mood and executive dysfunction in early Parkinson’s disease. Acta Neurol. Scand. 2003, 107, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Lawson, R.A.; Yarnall, A.J.; Duncan, G.W.; Khoo, T.K.; Breen, D.P.; Barker, R.A.; Collerton, D.; Taylor, J.P.; Burn, D.J. Severity of mild cognitive impairment in early Parkinson’s disease contributes to poorer quality of life. Parkinsonism Relat. Disord. 2014, 20, 1071–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varalta, V.; Picelli, A.; Fonte, C.; Amato, S.; Melotti, C.; Zatezalo, V.; Saltuari, L.; Smania, N. Relationship between cognitive performance and motor dysfunction in patients with Parkinson’s disease: A pilot cross-sectional study. Biomed. Res. Int. 2015, 365959. [Google Scholar] [CrossRef]
- Varalta, V.; Fonte, C.; Munari, D. The influence of cognitive factors on balance and gait. In Advanced Technologies for the Rehabilitation of Gait and Balance Disorders; Sandrini, G., Homberg, V., Saltuari, L., Smania, N., Pedrocchi, A., Eds.; Springer: Cham, Switzerland, 2018; Volume 19. [Google Scholar]
- Nagano-Saito, A.; Martinu, K.; Monchi, O. Function of basal ganglia in bridging cognitive and motor modules to perform an action. Front. Neurosci. 2014, 8, 187. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, I.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.; Deane, K.H.O.; Wheatley, K.; et al. Physiotherapy intervention in Parkinson’s disease: Systematic review and meta-analysis. BMJ 2012, 345, e5004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbruzzese, G.; Marchese, R.; Avanzino, L.; Pelosin, E. Rehabilitation for Parkinson’s disease: Current outlook and future challenges. Parkinsonism Relat. Disord. 2016, 22 (Suppl. 1), S60–S64. [Google Scholar] [CrossRef]
- Lauzé, M.; Daneault, J.F.; Duval, C. The Effects of Physical Activity in Parkinson’s Disease: A Review. J. Parkinsons Dis. 2016, 6, 685–698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intzandt, B.; Beck, E.N.; Silveira, C.R.A. The effects of exercise on cognition and gait in Parkinson’s disease: A scoping review. Neurosci. Biobehav. Rev. 2018, 95, 136–169. [Google Scholar] [CrossRef] [PubMed]
- Strouwen, C.; Molenaar, E.; Münks, L.; Keus, S.; Zijlmans, J.; Vandenberghe, W.; Bloem, B.R.; Nieuwboer, A. Training dual tasks together or apart in Parkinson’s disease: Results from the DUALITY trial. Mov. Disord. 2017, 32, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Barboza, N.M.; Terra, M.B.; Brandão Bueno, M.E.; Christofoletti, G.; Smaili, S.M. Physiotherapy versus physiotherapy plus cognitive training on cognition and quality of life in Parkinson disease randomized clinical trial. Am. J. Phys. Med. Rehabil. 2019, 98, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Walton, C.C.; Mowszowski, L.; Gilat, M.; Hall, J.M.; O’Callaghan, C.; Muller, A.J.; Georgiades, M.; Szeto, J.; Ehgoetz Martens, K.A.; Shine, J.M.; et al. Cognitive training for freezing of gait in Parkinson’s disease: A randomized controlled trial. NPJ Parkinsons Dis. 2018, 4, 15. [Google Scholar] [CrossRef]
- Leung, I.H.; Walton, C.C.; Hallock, H.; Lewis, S.J.; Valenzuela, M.; Lampit, A. Cognitive training in Parkinson disease: A systematic review and meta-analysis. Neurology 2015, 85, 1843–1851. [Google Scholar] [CrossRef] [Green Version]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- European Physiotherapy Guideline for Parkinson’s Disease. 2014. Available online: https://www.parkinsonnet.nl/app/uploads/sites/3/2019/11/eu_guideline_parkinson_guideline_for_pt_s1.pdf (accessed on 12 July 2021).
- Smania, N.; Corato, E.; Tinazzi, M.; Stanzani, C.; Fiaschi, A.; Girardi, P.; Gandolfi, M. Effect of balance training on postural instability in patients with idiopathic Parkinson’s disease. Neurorehabil. Neural Repair 2010, 24, 826–834. [Google Scholar] [CrossRef] [PubMed]
- Santangelo, G.; Siciliano, M.; Pedone, R.; Vitale, C.; Falco, F.; Bisogno, R.; Siano, P.; Barone, P.; Grossi, D.; Santangelo, F.; et al. Normative data for the Montreal Cognitive Assessment in an Italian population sample. Neurol. Sci. 2015, 36, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Song, J.; Fisher, B.E.; Petzinger, G.; Wu, A.; Gordon, J.; Salem, G.J. The relationships between the unified Parkinson’s disease rating scale and lower extremity functional performance in persons with early-stage Parkinson’s disease. Neurorehabil. Neural Repair 2009, 23, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Chertkow, H.; Nasreddine, Z.; Johns, E.; Phillips, N.; McHenry, C. P1-143: The Montreal cognitive assessment (MoCA): Validation of alternate forms and new recommendations for education corrections. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2011, 7, S157. [Google Scholar] [CrossRef]
- Appollonio, I.; Leone, M.; Isella, V.; Piamarta, F.; Consoli, T.; Villa, M.L.; Forapani, E.; Russo, A.; Nichelli, P. The frontal assessment battery (FAB): Normative values in an Italian population sample. Neurol. Sci. 2005, 26, 108–116. [Google Scholar] [CrossRef]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail Making Test: Normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.; Bagoj, E.; Monaco, M.; Zabberoni, S.; De Rosa, S.; Papantonio, A.M.; Mundi, C.; Caltagirone, C.; Carlesimo, G.A. Standardization and normative data obtained in the Italian population for a new verbal fluency instrument, the phonemic/semantic alternate fluency test. Neurol. Sci. 2014, 35, 365–372. [Google Scholar] [CrossRef]
- Monaco, M.; Costa, A.; Caltagirone, C.; Carlesimo, G.A. Forward and backward span for verbal and visuo-spatial data: Standardization and normative data from an Italian adult population. Neurol. Sci. 2013, 34, 749–754. [Google Scholar] [CrossRef]
- Carlesimo, G.A.; Caltagirone, C.; Gainotti, G. The Mental Deterioration Battery: Normative data, diagnostic reliability and qualitative analyses of cognitive impairment. The Group for the Standardization of the Mental Deterioration Battery. Eur. Neurol. 1996, 36, 378–384. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. General Psych. 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I. The balance scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehab. Med. 1995, 27, 27–36. [Google Scholar]
- Light, K.E.; Bebrman, A.L.; Thigpen, M.; Triggs, W.J. The 2-min walk test: A tool for evaluating walking endurance in clients with Parkinson’s disease. J. Neurol. Phys. Ther. 1997, 21, 136. [Google Scholar]
- Morris, S.; Morris, M.E.; Iansek, R. Reliability of measurements obtained with the Timed ‘Up & Go’ test in people with Parkinson disease. Phys. Ther. 2001, 81, 810–818. [Google Scholar]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the timed up & go test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Statist. Soc. B 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Gautschi, O.P.; Stienen, M.N.; Corniola, M.V.; Joswig, H.; Schaller, K.; Hildebrandt, G.; Smoll, N.R. Assessment of the Minimum Clinically Important Difference in the Timed Up and Go Test After Surgery for Lumbar Degenerative Disc Disease. Neurosurgery 2017, 80, 380–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domenech-Cebrían, P.; Martinez-Martinez, M.; Cauli, O. Relationship between mobility and cognitive impairment in patients with Alzheimer’s disease. Clin. Neurol. Neurosurg 2019, 179, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Varalta, V.; Melotti, C.; Zatezalo, V.; Fonte, C.; Amato, S.; Saltuari, L.; Santamato, A.; Fiore, P.; Smania, N. Effects of treadmill training on cognitive and motor features of patients with mild to moderate Parkinson’s disease: A pilot, single-blind, randomized controlled trial. Funct. Neurol. 2016, 31, 25–31. [Google Scholar] [PubMed]
- Altmann, L.J.P.; Stegemöller, E.; Hazamy, A.A.; Wilson, J.P.; Bowers, D.; Okun, M.S.; Hass, C.J. Aerobic exercise improves mood, cognition, and language function in parkinson’s disease: Results of a controlled study. J. Inter. Neuropsy. Soc. 2016, 22, 878–889. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Prakash, R.S.; Erickson, K.I.; Basak, C.; Chaddock, L.; Kim, J.S.; Alves, H.; Heo, S.; Szabo, A.N.; White, S.M.; et al. Plasticity of brain networks in a randomized intervention trial of exercise training in older adults. Front. Aging Neurosci. 2010, 2, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, G.; Wentzel-Larsen, T.; Aarsland, D.; Larsen, J.P. Progression of motor impairment and disability in Parkinson disease: A population-based study. Neurology 2005, 65, 1436–1441. [Google Scholar] [CrossRef]
- Sánchez-Ferro, Á.; Matarazzo, M.; Martínez-Martín, P.; Martínez-Ávila, J.C.; Gómez de la Cámara, A.; Giancardo, L.; Arroyo Gallego, T.; Montero, P.; Puertas-Martín, V.; Obeso, I.; et al. Minimal Clinically Important Difference for UPDRS-III in Daily Practice. Mov. Disord. Clin. Pract. 2018, 5, 448–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Outcome | Rehabilitation Program | Pre Treatment | Post Treatment | Within Group Comparison |
|---|---|---|---|---|
| Post vs. Pre-Treatment p Value (95% CI) | ||||
| MoCA (0–30) median (IQR) | PCT | 26.5 (24.75; 28) | 26 (24; 27.25) | 0.099 (−1.41; 0.21) |
| PT | 26.5 (23; 27) | 26 (24.5; 27.25) | 0.536 (−1.01; 0.51) | |
| UPDRS-III (0–56) median (IQR) | PCT | 9.5 (5; 16.25) | 13 (11; 21.5) | 0.002 (1.64; 7.76) * |
| PT | 11 (7.5; 13) | 13 (11; 17) | 0.004 (1.19; 7.11) * | |
| FABit (0–18) median (IQR) | PCT | 16 (15; 18) | 16 (13.5; 17) | 0.243 (1.99; 0.59) |
| PT | 17 (14.75; 18) | 17.5 (13.5; 18) | 0.893 (−1.61; 1.01) | |
| TMTa (seconds) mean (SD) | PCT | 57.55 (24.37) | 59.65 (37.21) | 0.808 (−11.86; 16.06) |
| PT | 55.6 (25.37) | 56.2 (27.77) | 0.872 (−6.90; 8.10) | |
| TMTb (seconds) mean (SD) | PCT | 197.4 (93.54) | 200.6 (92.96) | 0.73 (−15.88; 22.28) |
| PT | 195.1 (94.27) | 197.4 (94.07) | 0.977 (−20.72; 25.32) | |
| DSF (0–9) median (IQR) | PCT | 6 (5; 6) | 6 (5; 6) | 0.564 (−0.47; 0.27) |
| PT | 5 (5; 6) | 6 (5;6) | 0.109 (−0.08; 0.68) | |
| DSB (0–8) median (IQR) | PCT | 4 (3; 4.25) | 4 (4; 4) | 0.571 (−0.40; 0.70) |
| PT | 4 (3; 4) | 4 (3.75; 5) | 0.35 (−0.35; 0.95) | |
| BBS (0–56) median (IQR) | PCT | 53.5 (50; 55) | 54 (48; 55) | 0.954 (2.37; 1.37) |
| PT | 52 (50.5; 55) | 54 (50.75; 55) | 0.652 (−3.62; 1.02) | |
| 2MWT (meters) mean (SD) | PCT | 107.28 (30.54) | 130.53 (38.32) | 0.006 (7.63; 38.88) * |
| PT | 112.9 (48.48) | 130.6 (39.07) | 0.011 (5.13; 30.23) * | |
| TUG (seconds) mean (SD) | PCT | 11.96 (6.65) | 10.89 (6.85) | 0.033 (−2.37; 1.37) * |
| PT | 10.49 (4.46) | 11.12 (6.73) | 0.823 (−0.73; 1.98) | |
| TUG-COG (seconds) mean (SD) | PCT | 14.30 (6.99) | 12.85 (6.96) | 0.067 (−2.93; 0.05) |
| PT | 12.58 (5.19) | 12.66 (7.37) | 0.601 (−1.38; 1.54) | |
| TUG-MOT (seconds) mean (SD) | PCT | 13.37 (6.53) | 9.36 (2.23) | 0.007 (−9.05; -0.86) * |
| PT | 10.99 (4.98) | 11.6 (6.94) | 0.149 (−2.84; 5.11) | |
| STAI-Y2 (0–80) median (IQR) | PCT | 43 (38.75; 50) | 43 (36; 48.25) | 0.432 (−5.18; 3.18) |
| PT | 41 (36; 49) | 40 (35; 50.25) | 0.904 (−4.79; 6.79) |
| Outcome | Rehabilitation Program | Pre Treatment | Post Treatment | Repeated Measures ANOVA | Post Hoc Analysis | |
|---|---|---|---|---|---|---|
| Group Between-Subjects | Time Whitin-Subjects | Whitin-Group | ||||
| p | p | Post vs. Pre-Treatment p Value (95% CI) p | ||||
| FAS (no. words) mean (SD) | PCT | 11.65 (3.99) | 13.02 (3.98) | 0.838 | 0.075 | / |
| PT | 12.39 (3.91) | 12.82 (5.57) | / | |||
| RAVL-I (0-75) mean (SD) | PCT | 34.1 (6.81) | 39.4 (10.58) | 0.785 | 0.004 * | 0.002 (2.04; 8.56) * |
| PT | 35.2 (9.96) | 36.9 (7.4) | 0.297 (−1,56; 4.96) | |||
| RAVL-D (0-15) mean (SD) | PCT | 5.6 (2.86) | 7.65 (3.3) | 0.909 | 0.001 * | 0.002 (0.77; 3.33) * |
| PT | 6.1 (3.14) | 7.35 (3.05) | 0.055 (−0.03; 2.53) | |||
| BDI (0-63) mean (SD) | PCT | 12.37 (7.03) | 12 (7.61) | 0.906 | 0.577 | / |
| PT | 11.3 (8.23) | 12.9 (7.52) | / | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Varalta, V.; Poiese, P.; Recchia, S.; Montagnana, B.; Fonte, C.; Filippetti, M.; Tinazzi, M.; Smania, N.; Picelli, A. Physiotherapy versus Consecutive Physiotherapy and Cognitive Treatment in People with Parkinson’s Disease: A Pilot Randomized Cross-Over Study. J. Pers. Med. 2021, 11, 687. https://doi.org/10.3390/jpm11080687
Varalta V, Poiese P, Recchia S, Montagnana B, Fonte C, Filippetti M, Tinazzi M, Smania N, Picelli A. Physiotherapy versus Consecutive Physiotherapy and Cognitive Treatment in People with Parkinson’s Disease: A Pilot Randomized Cross-Over Study. Journal of Personalized Medicine. 2021; 11(8):687. https://doi.org/10.3390/jpm11080687
Chicago/Turabian StyleVaralta, Valentina, Paola Poiese, Serena Recchia, Barbara Montagnana, Cristina Fonte, Mirko Filippetti, Michele Tinazzi, Nicola Smania, and Alessandro Picelli. 2021. "Physiotherapy versus Consecutive Physiotherapy and Cognitive Treatment in People with Parkinson’s Disease: A Pilot Randomized Cross-Over Study" Journal of Personalized Medicine 11, no. 8: 687. https://doi.org/10.3390/jpm11080687