
Efficacy of Laser Doppler Flowmetry, as a Diagnostic Tool in Assessing Pulp Vitality of Traumatised Teeth: A Split Mouth Clinical Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Subject Selection
2.1.2. Eligibility Criteria
Inclusion Criteria
- Fit and healthy patients aged <18-year-old;
- Patients with maxillary permanent incisor subjected to any type of traumatic injury (concussion, subluxation, extrusion, lateral luxation, intrusion, crown fracture) without any dentoalveolar trauma involvement (confirmed by a clinical examination and imaging evaluation) and have a contralateral homologous tooth with no signs/symptoms of injury. Treatment of all traumatized teeth was performed, and the established dental trauma guidelines were followed [19];
- Patients attended their first dental visit within 3 days of the dental trauma;
- Sensitivity value of the electric pulp test over 200 μA [20] (an electric pulp tester (Scorpion, 405-7A, Optica Laser, Bulgaria) was used to test the vitality of the traumatised and non-traumatised teeth)
- Patients with at least one vital and non-traumatised maxillary incisor acting as a control tooth;
- Ability to obtain a verbal acceptance from all the subjects to comply with all the treatments and follow-up timepoints attendance;
- Ability to obtain written informed consent by the patients’ parents/guardians for treatment, participation in the study and publication.
Exclusion Criteria
- Patients who were undergoing therapy for neurological conditions or with mental or cognitive problems;
- Patients who were taking sedative, analgesic, and/or anti-inflammatory medication 7 days prior to the treatment commencement;
- Patients who have never had any first dental visit or treatment;
- Patients with systemic diseases or physiological development delay;
- Patients with active infectious diseases such as; influenza, scarlet fever, etc.
- Patients with restorations covered more than half the labial surface of the investigated teeth.
2.2. Interventions
2.2.1. An Electric Pulp Testing
- The patient held the passive electrode in the right hand;
- Instructions were given to the patient-when the slightest irritation in the tooth was felt, he/she must press the passive electrode button;
- An isolation of the investigated tooth followed;
- The tooth surfaces were dried with air spray for 15 s;
- The tip of the active electrode was placed perpendicular to the most sensitive point of the tooth which was at the middle of the incisal edge;
- The measurement started by pressing the button on the active electrode;
- The result was read after the button was pressed by the patient.
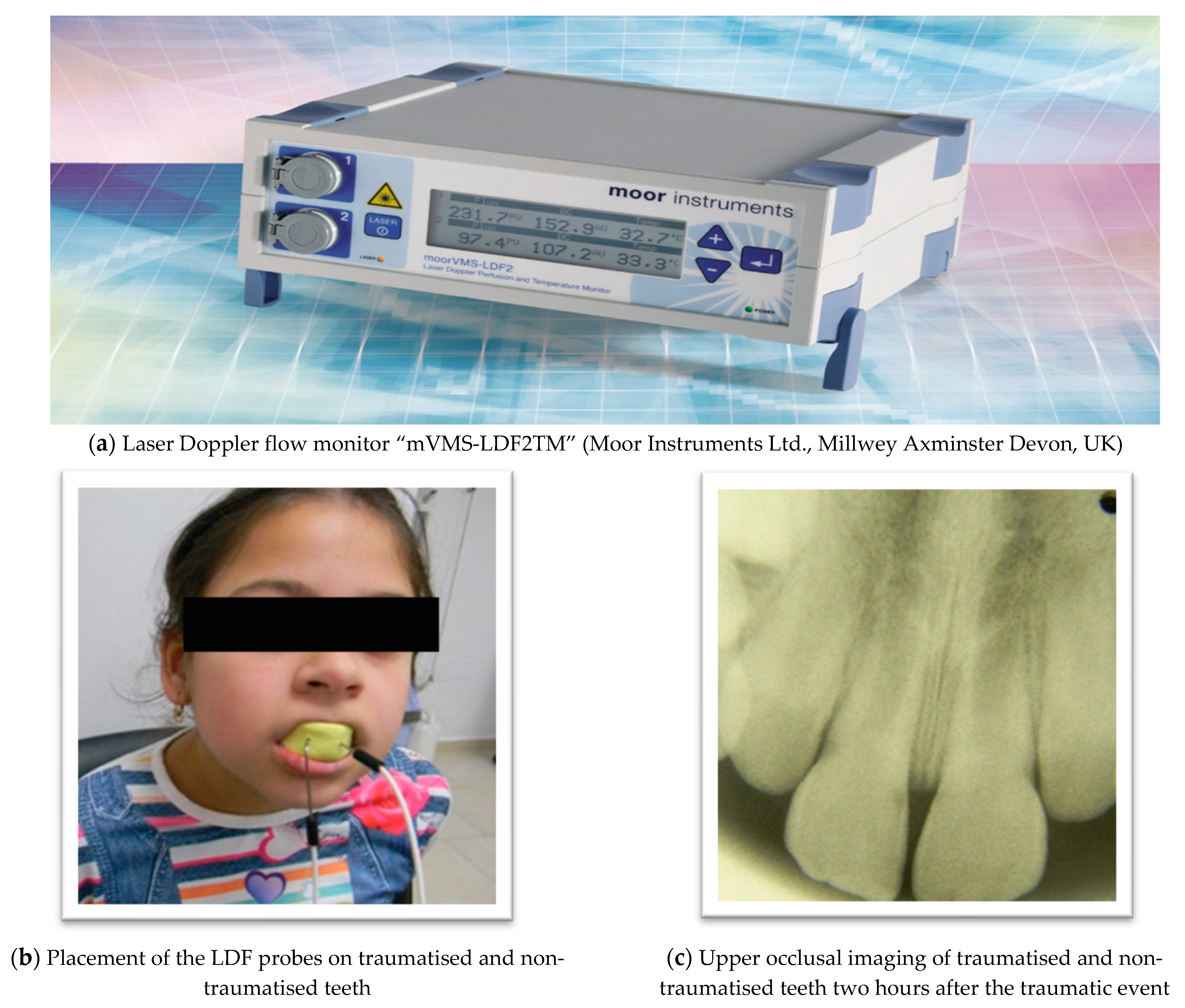
2.2.2. Laser Doppler Flowmeter (LDF) Description and Utilised Parameters
- Average power—1.0 mV;
- Diameter of the probe—1.5 mm;
- Frequency—40 Hz;
- Monitoring time—180 s (sec).
2.2.3. The Treatment Description
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abdel Malak, C.; Chakar, C.; Romanos, A.; Rachidi, S. Prevalence and Etiological Factors of Dental Trauma among 12- and 15-Year-Old Schoolchildren of Lebanon: A National Study. Sci. World J. 2021, 2021, 5587431. [Google Scholar] [CrossRef]
- Kishen, A.; Muralidharan, N.P. Recent Advancements in Pulp Testing Devices. Indian J. Forensic Med. Toxicol. 2020, 14, 6049–6059. [Google Scholar]
- Noblett, W.C.; Wilcox, L.R.; Scamman, F.; Johnson, W.T.; Diaz-Arnold, A. Detection of pulpal circulation in vitro by pulse oximetry. J. Endod. 1996, 22, 1–5. [Google Scholar] [CrossRef]
- Tomer, A.K.; Raina, A.A.; Ayub, F.; Bhatt, M. Recent advances in pulp vitality testing: A review. Int. J. Appl. Dent. Sci. 2019, 5, 8–12. [Google Scholar]
- Estrela, C.; Oliveira, K.S.; Alencar, A.H.G.; Barletta, F.B.; Estrela, C.R.; Felippe, W.T. Oxygen Saturation in the Dental Pulp of Maxillary and Mandibular Molars—Part 2. Braz. Dent. J. 2017, 28, 704–709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gopikrishna, V.; Tinagupta, K.; Kandaswamy, D. Evaluation of efficacy of a new custom-made pulse oximeter dental probe in comparison with the electrical and thermal tests for assessing pulp vitality. J. Endod. 2007, 33, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Janani, K.; Ajitha, P.; Sandhya, R.; Subbaiyan, H.; Jose, J. Efficiency of new custom-made pulse oximeter sensor holder in assessment of actual pulp status. J. Fam. Med. Prim. Care 2020, 9, 3333–3337. [Google Scholar]
- Jacob, Y.; Nivedhitha, M.S. Clinical practice guidelines in the testing of pulp sensibility and vitality. Drug Invent. Today 2019, 11, 2719–2724. [Google Scholar]
- Limjeerajarus, C. Laser Doppler flowmetry: Basic principle, current clinical and research applications in dentistry. CU Dent. J. 2014, 37, 123–136. [Google Scholar]
- Roeykens, H.J.J.; De Coster, P.; Jacquet, W.; De Moor, R.J.G. How standard deviation contributes to the validity of a LDF signal: A cohort study of 8 years of dental trauma. Lasers Med. Sci. 2019, 34, 1905–1916. [Google Scholar] [CrossRef]
- Emshoff, R.; Moschen, I.; Strobl, H. Use of laser Doppler flowmetry to predict vitality of luxated or avulsed permanent teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004, 98, 750–755. [Google Scholar] [CrossRef]
- Emshoff, R.; Emshoff, I.; Moschen, I.; Strobl, H. Laser Doppler flowmetry of luxated permanent incisors: A receiver operator characteristic analysis. J. Oral Rehabil. 2004, 31, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Roeykens, H.; De Moor, R. The use of laser Doppler flowmetry in paediatric dentistry. Eur. Arch. Paediatr. Dent. 2011, 12, 85–89. [Google Scholar] [CrossRef]
- Strobl, H.; Moschen, I.; Emshoff, I.; Emshoff, R. Effect of luxation type on pulpal blood flow measurements: A long-term follow-up of luxated permanent maxillary incisors. J. Oral Rehabil. 2005, 32, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Yanpiset, K.; Sigurdsson, A.; Vann, W.F., Jr. Laser Doppler flowmetry for monitoring traumatized teeth. Dent. Traumatol. 2001, 17, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Strobl, H.; Haas, M.; Norer, B.; Gerhard, S.; Emshoff, R. Evaluation of pulpal blood flow after tooth splinting of luxated permanent maxillary incisors. Dent. Traumatol. 2004, 20, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Emshoff, R.; Moschen, I.; Oberrauch, A.; Gerhard, S.; Strobl, H. Outcomes of dental fracture injury as related to laser Doppler flow measurements of pulpal blood-flow level. Dent. Traumatol. 2008, 24, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; For the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [Green Version]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef]
- Kosturkov, D.N. Pulse Oximetry in Dental Medicine. Ph.D. Thesis, Medical University-Sofia, Sofia, Bulgaria, 2019. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Kakino, S.; Kushibiki, S.; Yamada, A.; Miwa, Z.; Takagi, Y.; Matsuura, Y. Optical measurement of blood saturation of dental pulp. Int. Sch. Res. Notices 2013, 2013, 502869. [Google Scholar] [CrossRef]
- Setzer, F.C.; Challagulla, P.; Kataoka, S.H.H.; Trope, M. Effect of tooth isolation on laser Doppler readings. Int. Endod. J. 2012, 46, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Todea, C.; Canjau, S.; Miron, M.; Vitez, B.; Noditi, G. Laser Doppler Flowmetry Evaluation of the Microcirculation in Dentistry. Microcirculation Revisited—From Molecules to Clinical Practice; IntechOpen: London, UK, 2016. [Google Scholar] [CrossRef] [Green Version]
- Gazelius, B.; Olgart, L.; Edwall, B.; Edwall, L. Non-invasive recording of blood flow in human dental pulp. Endod. Dent. Traumatol. 1986, 2, 219–221. [Google Scholar] [CrossRef] [PubMed]
- Ingolfsson, A.R.; Tronstad, L.; Hersh, E.V.; Riva, C.E. Efficacy of laser Doppler flowmetry in determining pulp vitality of human teeth. Endod. Dent. Traumatol. 1994, 10, 83–87. [Google Scholar] [CrossRef]
- Akpinar, K.E.; Er, K.; Polat, S.; Polat, N.T. Effect of gingiva on laser doppler pulpal blood flow measurements. J. Endod. 2004, 30, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Gopikrishna, V.; Pradeep, G.; Venkateshbabu, N. Assessment of pulp vitality: A review. Int. J. Paediatr. Dent. 2009, 19, 3–15. [Google Scholar] [CrossRef]
- Polat, S.; Er, K.; Polat, N.T. Penetration depth of laser Doppler flowmetry beam in teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 125–129. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Session | Group | p Value | |
|---|---|---|---|
| Session I | Traumatised teeth | Non-traumatised teeth | |
| 26.32 ± 17.14 AU | 21.53 ± 13.87 AU | 0.02 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belcheva, A.; Shindova, M.; Hanna, R. Efficacy of Laser Doppler Flowmetry, as a Diagnostic Tool in Assessing Pulp Vitality of Traumatised Teeth: A Split Mouth Clinical Study. J. Pers. Med. 2021, 11, 801. https://doi.org/10.3390/jpm11080801
Belcheva A, Shindova M, Hanna R. Efficacy of Laser Doppler Flowmetry, as a Diagnostic Tool in Assessing Pulp Vitality of Traumatised Teeth: A Split Mouth Clinical Study. Journal of Personalized Medicine. 2021; 11(8):801. https://doi.org/10.3390/jpm11080801
Chicago/Turabian StyleBelcheva, Ani, Maria Shindova, and Reem Hanna. 2021. "Efficacy of Laser Doppler Flowmetry, as a Diagnostic Tool in Assessing Pulp Vitality of Traumatised Teeth: A Split Mouth Clinical Study" Journal of Personalized Medicine 11, no. 8: 801. https://doi.org/10.3390/jpm11080801