


Evaluating Thrombolysis Rates and Emergency Department Time Targets in Acute Ischemic Stroke: Need for Personalized Medicine

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Material and Methods
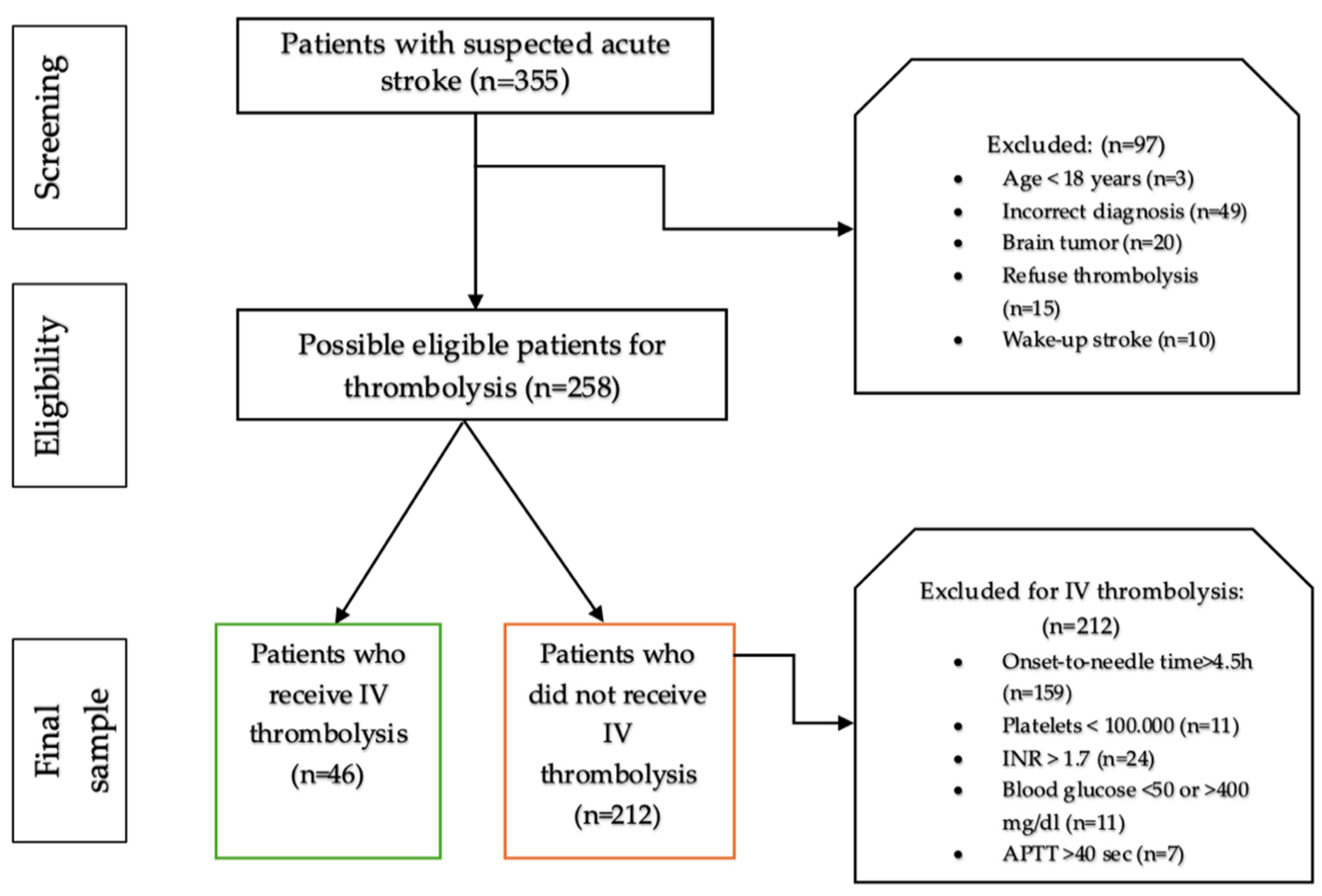
2.1. Study Design and Patient Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients at Admission to ED
3.2. Analysis of Correlations between Stroke Severity Scores and Performing IV Thrombolysis
3.3. Analysis of Correlations between ED Time Targets and Performing IV Thrombolysis
3.4. The Logistic Regression Analysis of ED Times Targets and Comorbidities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saini, V.; Guada, L.; Yavagal, D.R. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology 2021, 97 (Suppl. S2), S6–S16. [Google Scholar] [CrossRef] [PubMed]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.; Fonseca, A.C.; Padiglioni, C.; Pérez de la Ossa, N.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I-LXII. [Google Scholar] [CrossRef]
- Gajurel, B.P.; Nepal, G.; Jaiswal, V.; Ang, S.P.; Nain, P.; Shama, N.; Ruchika, F.N.U.; Bohara, S.; Kharel, S.; Yadav, J.K.; et al. Utilization rates of intravenous thrombolysis for acute ischemic stroke in Asian countries: A systematic review and meta-analysis. Medicine 2023, 102, e35560. [Google Scholar] [CrossRef] [PubMed]
- Aguiar de Sousa, D.; von Martial, R.; Abilleira, S.; Gattringer, T.; Kobayashi, A.; Gallofré, M.; Fazekas, F.; Szikora, I.; Feigin, V.; Caso, V.; et al. Access to and delivery of acute ischaemic stroke treatments: A survey of national scientific societies and stroke experts in 44 European countries. Eur. Stroke J. 2019, 4, 13–28. [Google Scholar] [CrossRef]
- Stroke Alliance for Europe. The Burden of Stroke in Europe—Challenges for Policy Makers. Available online: https://www.stroke.org.uk/sites/default/files/the_burden_of_stroke_in_europe_-_challenges_for_policy_makers.pdf (accessed on 14 January 2022).
- Strilciuc, S.; Grad, D.A.; Mixich, V.; Stan, A.; Buzoianu, A.D.; Vladescu, C.; Vintan, M.A. Societal Cost of Ischemic Stroke in Romania: Results from a Retrospective County-Level Study. Brain Sci. 2021, 11, 689. [Google Scholar] [CrossRef]
- Tiu, C.; Terecoasă, E.O.; Tuță, S.; Bălașa, R.; Simu, M.; Sabău, M.; Stan, A.; Radu, R.A.; Tiu, V.; Cășaru, B.; et al. Quality of acute stroke care in Romania: Achievements and gaps between 2017 and 2022. Eur. Stroke J. 2023, 8 (Suppl. S1), 44–51. [Google Scholar] [CrossRef] [PubMed]
- Priority Action for Interventional Treatment of Patients with Acute Stroke. Standard Operating Procedure Regarding the Patient Track and Therapeutic Protocol in Romania. Available online: https://legislatie.just.ro/Public/DetaliiDocument/209994 (accessed on 12 October 2023).
- Popa, D.; Iancu, A.; Petrica, A.; Buleu, F.; Williams, C.G.; Sutoi, D.; Trebuian, C.; Tudor, A.; Mederle, O.A. Emergency Department Time Targets for Interhospital Transfer of Patients with Acute Ischemic Stroke. J. Pers. Med. 2023, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Mowla, A.; Doyle, J.; Lail, N.S.; Rajabzadeh-Oghaz, H.; Deline, C.; Shirani, P.; Ching, M.; Crumlish, A.; Steck, D.A.; Janicke, D.; et al. Delays in door-to-needle time for acute ischemic stroke in the emergency department: A comprehensive stroke center experience. J Neurol Sci. 2017, 376, 102–105. [Google Scholar] [CrossRef]
- Craig, L.E.; McInnes, E.; Taylor, N.; Grimley, R.; Cadilhac, D.A.; Considine, J.; Middleton, S. Identifying the barriers and enablers for a triage, treatment, and transfer clinical intervention to manage acute stroke patients in the emergency department: A systematic review using the theoretical domains framework (TDF). Implement. Sci. 2016, 11, 1–18. [Google Scholar] [CrossRef]
- Middleton, S.; Dale, S.; Cheung, N.W.; Cadilhac, D.A.; Grimshaw, J.M.; Levi, C.; McInnes, E.; Considine, J.; McElduff, P.; Gerraty, R.; et al. Nurse-Initiated Acute Stroke Care in Emergency Departments: The Triage, Treatment, and Transfer Implementation Cluster Randomized Controlled Trial. Stroke 2019, 50, 1346–1355. [Google Scholar] [CrossRef]
- Price, C.I.; White, P.; Balami, J.; Bhattarai, N.; Coughlan, D.; Exley, C.; Flynn, D.; Halvorsrud, K.; Lally, J.; McMeekin, P.; et al. Improving emergency treatment for patients with acute stroke: The PEARS research programme, including the PASTA cluster RCT, in Programme Grants for Applied Research. Programme Grants Appl. Res. 2022, 10, 1–96. [Google Scholar] [CrossRef] [PubMed]
- Buleu, F.; Popa, D.; Williams, C.; Tudor, A.; Sutoi, D.; Trebuian, C.; Ioan, C.C.; Iancu, A.; Cozma, G.; Marin, A.M.; et al. Code Stroke Alert: Focus on Emergency Department Time Targets and Impact on Door-to-Needle Time across Day and Night Shifts. J. Pers. Med. 2024, 14, 596. [Google Scholar] [CrossRef]
- Bathla, G.; Ajmera, P.; Mehta, P.M.; Benson, J.C.; Derdeyn, C.P.; Lanzino, G.; Agarwal, A.; Brinjikji, W. Advances in Acute Ischemic Stroke Treatment: Current Status and Future Directions. Am. J. Neuroradiol. 2023, 44, 750–758. [Google Scholar] [CrossRef]
- Wireklint Sundström, B.; Herlitz, J.; Hansson, P.O.; Brink, P. Comparison of the university hospital and county hospitals in western Sweden to identify potential weak links in the early chain of care for acute stroke: Results of an observational study. BMJ Open 2015, 5, e008228. [Google Scholar] [CrossRef] [PubMed]
- Aho, K.; Harmsen, P.; Hatano, S.; Marquardsen, J.; Smirnov, V.E.; Strasser, T. Cerebrovascular disease in the community: Results of a WHO collaborative study. Bull. World Health Organ. 1980, 58, 113. [Google Scholar] [PubMed]
- Goldstein, L.B.; Bertels, C.; Davis, J.N. Interrater reliability of the NIH stroke scale. Arch. Neurol. 1989, 46, 660–662. [Google Scholar] [CrossRef]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef]
- Dorado, L.; Millán, M.; Dávalos, A. Reperfusion therapies for acute ischemic stroke: An update. Curr. Cardiol. Rev. 2014, 10, 327–335. [Google Scholar] [CrossRef]
- Myrou, A.; Tsolaki, A.; Tegos, T.; Savopoulo, C. Thrombolytic Therapy in Strokes: A Retrospective Clinical Data Analysis of 40 Patients in a 7-Year Period: The Experience of a Greek Internal Medicine Department. Saudi J. Med. 2023, 8, 580–584. [Google Scholar] [CrossRef]
- Hassankhani, H.; Soheili, A.; Vahdati, S.S.; Mozaffari, F.A.; Fraser, J.F.; Gilani, N. Treatment Delays for Patients with Acute Ischemic Stroke in an Iranian Emergency Department: A Retrospective Chart Review. Ann. Emerg. Med. 2019, 73, 118–129. [Google Scholar] [CrossRef]
- Muhsin, A.; Blackburn, B. Treatment Delays for Patients with Acute Ischemic Stroke in a Rural Arkansas Emergency Department: A Retrospective Chart Review. Cureus 2024, 16, e61103. [Google Scholar] [CrossRef]
- Ganti, L.; Mirajkar, A.; Banerjee, P.; Stead, T.; Hanna, A.; Tsau, J.; Khan, M.; Garg, A. Impact of emergency department arrival time on door-to-needle time in patients with acute stroke. Front. Neurol. 2023, 14, 1126472. [Google Scholar] [CrossRef]
- Baskar, P.S.; Chowdhury, S.Z.; Bhaskar, S.M.M. In-hospital systems interventions in acute stroke reperfusion therapy: A meta-analysis. Acta Neurol. Scand. 2021, 144, 418–432. [Google Scholar] [CrossRef] [PubMed]
- Bhat, A.; Mahajan, V.; Wolfe, N. Implicit bias in stroke care: A recurring old problem in the rising incidence of young stroke. J. Clin. Neurosci. 2021, 85, 27–35. [Google Scholar] [CrossRef]
- Johnson, C.O.; Nguyen, M.; Roth, G.A.; Nichols, E.; Alam, T.; Abate, D.; Abd-Allah, F.; Abdelalim, A.; Abraha, H.N.; Abu-Rmeileh, N.M.; et al. Global, regional, and national burden of stroke, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Alkhotani, A.; Alharbi, Y.; Alghamdi, H.; Alshareef, H.; Abdulmuttalib, J.A.; Alsulami, A.; Alharbi, A. Time Window for Acute Stroke Treatment: Current Practice in King Abdullah Medical City Specialist Hospital in Makkah, Saudi Arabia. Cureus 2022, 14, e28878. [Google Scholar] [CrossRef]
- Lachkhem, Y.; Rican, S.; Minvielle, É. Understanding delays in acute stroke care: A systematic review of reviews. Eur. J. Public Health 2018, 28, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Chai, E.; Li, C.; Jiang, L. Factors affecting in-hospital delay of intravenous thrombolysis for acute ischemic stroke: A retrospective cohort study. Medicine 2019, 98, e15422. [Google Scholar] [CrossRef]
- Fladt, J.; Meier, N.; Thilemann, S.; Polymeris, A.; Traenka, C.; Seiffge, D.J.; Sutter, R.; Peters, N.; Gensicke, H.; Flückiger, B.; et al. Reasons for Prehospital Delay in Acute Ischemic Stroke. J. Am. Heart Assoc. 2019, 8, e013101. [Google Scholar] [CrossRef]
- Iancu, A.; Buleu, F.; Chita, D.S.; Tutelca, A.; Tudor, R.; Brad, S. Early Hemorrhagic Transformation after Reperfusion Therapy in Patients with Acute Ischemic Stroke: Analysis of Risk Factors and Predictors. Brain Sci. 2023, 13, 840. [Google Scholar] [CrossRef]
- Carrera, J.F.; Sorace, B.J.; Worrall, B.B.; Southerland, A.M.; Chiota-McCollum, N.A. Delay to Tissue Plasminogen Activator in Hypertensive Stroke Patients: An Analysis of Delay Duration Across Agents. J. Stroke Cerebrovasc. Dis. 2020, 29, 104525. [Google Scholar] [CrossRef] [PubMed]
- Navalkele, D.D.; Cai, C.; Vahidy, F.; Rahbar, M.H.; Pandurengan, R.; Wu, T.C.; Sarraj, A.; Barreto, A.; Grotta, J.C.; Gonzales, N. Higher prehospital blood pressure prolongs door to needle thrombolysis times: A target for quality improvement? Am. J. Emerg. Med. 2016, 34, 1268–1272. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, X.; You, S.; Cao, X.; Wang, X.; Gong, W.; Qin, Y.; Huang, X.; Cao, Y.; Shi, R. Factors Associated with Pre-Hospital Delay and Intravenous Thrombolysis in China. J. Stroke Cerebrovasc. Dis. 2020, 29, 104897. [Google Scholar] [CrossRef]
- Kummarg, U.; Sindhu, S.; Muengtaweepongsa, S. The early outcomes of nurse case management in patients with acute ischemic stroke treated with intravenous recombinant tissue plasminogen activator: A prospective randomized controlled trial. Neurol. Res. Int. 2018, 2018, 1717843. [Google Scholar] [CrossRef]
- Kamal, N.; Holodinsky, J.K.; Stephenson, C.; Kashayp, D.; Demchuk, A.M.; Hill, M.D.; Vilneff, R.L.; Bugbee, E.; Zerna, C.; Newcommon, N.; et al. Improving Door-to-Needle Times for Acute Ischemic Stroke: Effect of Rapid Patient Registration, Moving Directly to Computed Tomography, and Giving Alteplase at the Computed Tomography Scanner. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003242. [Google Scholar] [CrossRef] [PubMed]
- Leite, K.F.S.; Dos Santos, S.R.; Andrade, R.L.P.; de Faria, M.; Saita, N.M.; Arcêncio, R.A.; Isaac, I.; de Rezende, C.E.M.; Villa, T.C.S.; Pontes Neto, O.M.; et al. Reducing care time after implementing protocols for acute ischemic stroke: A systematic review. Arq. Neuropsiquiatr. 2022, 80, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Xia, H.; Xu, J.; Long, C.; Liu, L.; Huang, F.; Zeng, J.; Yuan, L. Reducing intravenous thrombolysis delay in acute ischemic stroke through a quality improvement program in the emergency department. Front. Neurol. 2022, 13, 931193. [Google Scholar] [CrossRef]
- Khidir, H.; Salhi, R.; Sabbatini, A.K.; Franks, N.M.; Green, A.; Richardson, L.D.; Terry, A.; Vasquez, N.; Goyal, P.; Kocher, K.; et al. A Quality Framework to Address Racial and Ethnic Disparities in Emergency Department Care. Ann. Emerg. Med. 2023, 81, 47–56. [Google Scholar] [CrossRef]
- Kocher, K.E.; Arora, R.; Bassin, B.S.; Benjamin, L.S.; Bolton, M.; Dennis, B.J.; Ham, J.J.; Krupp, S.S.; Levasseur, K.A.; Macy, M.L. Baseline performance of real-world clinical practice within a statewide emergency medicine quality network: The Michigan Emergency Department Improvement Collaborative (MEDIC). Ann. Emerg. Med. 2020, 75, 192–205. [Google Scholar] [CrossRef]
- Schuur, J.D.; Hsia, R.Y.; Burstin, H.; Schull, M.J.; Pines, J.M. Quality measurement in the emergency department: Past and future. Health Aff. 2013, 32, 2129–2138. [Google Scholar] [CrossRef]
- Huang, Q.; Zhang, J.-z.; Xu, W.-d.; Wu, J. Generalization of the right acute stroke promotive strategies in reducing delays of intravenous thrombolysis for acute ischemic stroke: A meta-analysis. Medicine 2018, 97, e11205. [Google Scholar] [CrossRef]
- Tunkl, C.; Paudel, R.; Bajaj, S.; Thapa, L.; Tunkl, P.; Chandra, A.; Shah, B.; Karmacharya, B.; Subedi, A.; Jalan, P.; et al. Implementing stroke care in a lower-middle-income country: Results and recommendations based on an implementation study within the Nepal Stroke Project. Front. Neurol. 2023, 14, 1272076. [Google Scholar] [CrossRef] [PubMed]
- Santana Baskar, P.; Cordato, D.; Wardman, D.; Bhaskar, S. In-hospital acute stroke workflow in acute stroke—Systems-based approaches. Acta Neurol. Scand. 2021, 143, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, K.; Balucani, C.; Walter, S.; Levine, S.R.; Haass, A.; Grotta, J. Streamlining of prehospital stroke management: The golden hour. Lancet Neurol. 2013, 12, 585–596. [Google Scholar] [CrossRef]
- Feda, S.; Nikoubashman, O.; Schürmann, K.; Matz, O.; Tauber, S.; Wiesmann, M.; Schulz, J.; Reich, A. Endovascular stroke treatment does not preclude high thrombolysis rates. Eur. J. Neurol. 2019, 26, 428-e33. [Google Scholar] [CrossRef]
- Ma, H.; Campbell, B.C.; Parsons, M.W.; Churilov, L.; Levi, C.R.; Hsu, C.; Kleinig, T.J.; Wijeratne, T.; Curtze, S.; Dewey, H.M. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N. Engl. J. Med. 2019, 380, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Psychogios, K.; Magoufis, G.; Safouris, A.; Kargiotis, O.; Katsanos, A.H.; Spiliopoulos, S.; Papageorgiou, E.; Palaiodimou, L.; Brountzos, E.; Stamboulis, E. Eligibility for intravenous thrombolysis in acute ischemic stroke patients presenting in the 4.5–9 h window. Neuroradiology 2020, 62, 733–739. [Google Scholar] [CrossRef]
- Iancu, A.; Tudor, R.; Chita, D.S.; Juratu, C.; Tudor, A.; Buleu, F.; Popa, D.; Brad, S. Mechanical Thrombectomy via Transbrachial Approach in the Emergency Management of Acute Ischemic Stroke Patients with Aortic Pathologies: Our Experience and Literature Review. J. Pers. Med. 2024, 14, 216. [Google Scholar] [CrossRef]
- Bhaskar, S.; Stanwell, P.; Cordato, D.; Attia, J.; Levi, C. Reperfusion therapy in acute ischemic stroke: Dawn of a new era? BMC Neurol. 2018, 18, 8. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Thrombolysis | Valid | Mean ± SD | Median (Q1–Q2) | p |
|---|---|---|---|---|---|
| Age, years | No | 212 | 66.71 ± 11.94 | 67 (60.75–75) | <0.001 * |
| Yes | 46 | 74.39 ± 10.94 | 76.5 (70–81) | ||
| Male, n | No | 119 (56.1%) | - | - | 0.449 |
| Yes | 23 (50%) | - | - | ||
| Height, cm | No | 212 | 172.11 ± 7.9 | 172 (167–178) | <0.001 * |
| Yes | 46 | 163.28 ± 4.49 | 165 (160–165) | ||
| Weight, kg | No | 212 | 78.03 ± 12.32 | 80 (70–85) | <0.001 * |
| Yes | 46 | 70.96 ± 10.42 | 70 (65.75–77.25) | ||
| SBP, mmHg | No | 212 | 154.54 ± 20.57 | 154.5 (140–170) | 0.392 |
| Yes | 46 | 155.98 ± 21.31 | 160 (141.25–175) | ||
| DBP, mmHg | No | 212 | 81.46 ± 12.26 | 80 (75–90) | 0.817 |
| Yes | 46 | 81.2 ± 15.92 | 80 (70–93.75) | ||
| GCS | No | 212 | 13.85 ± 2.41 | 15 (14–15) | <0.001 * |
| Yes | 46 | 9 ± 4.94 | 10 (3.25–15) |
| Variable | Thrombolysis | Valid | Mean ± SD | Median (IQR) | p |
|---|---|---|---|---|---|
| Platelets count, ×109 uL | No | 212 | 220.63 ± 63.45 | 219 (171.75–255) | 0.944 |
| Yes | 46 | 228.35 ± 90.57 | 221 (176–248.5) | ||
| Hemoglobin, mg/dL | No | 212 | 13.56 ± 1.85 | 14 (12–15) | 0.007 * |
| Yes | 46 | 12.85 ± 1.55 | 13 (12–14) | ||
| Blood Glucose, mg/dL | No | 212 | 140.32 ± 48.49 | 125.5 (104–171.25) | 0.359 |
| Yes | 46 | 130.83 ± 37.69 | 121 (104.25–150.75) | ||
| INR | No | 212 | 1.68 ± 1.72 | 1.18 (1.038–1.41) | 0.672 |
| Yes | 46 | 1.27 ± 0.36 | 1.225 (1.08–1.39) | ||
| Partial thromboplastin time, sec | No | 212 | 29.3 ± 15.32 | 25.85 (23.075–29.225) | 0.020 * |
| Yes | 46 | 28.37 ± 4.91 | 28.1 (24.8–31.3) | ||
| Prothrombin time, sec | No | 212 | 17.65 ± 19.63 | 12.95 (12–14.9) | 0.006 * |
| Yes | 46 | 14.69 ± 2.83 | 14.3 (13.025–15.25) |
| Variable | Thrombolysis | Valid | Mean ± SD | Median (IQR) | p |
|---|---|---|---|---|---|
| NIHSS at presentation | No | 212 | 14.49 ± 5.33 | 15 (10–19) | 0.654 |
| Yes | 46 | 13.94 ± 6.15 | 15 (8.5–19) | ||
| NIHSS at 1 h | No | 212 | 12.3 ± 6.21 | 13 (7–17) | 0.861 |
| Yes | 46 | 12 ± 6.86 | 11.5 (6–18) | ||
| NIHSS at 2 h | No | 212 | 11.37 ± 6.48 | 12 (6–16) | 0.889 |
| Yes | 46 | 11.48 ± 7.01 | 10 (4.5–17.75) | ||
| NIHSS at 24 h | No | 210 | 10.65 ± 7.01 | 10 (5–16) | 0.649 |
| Yes | 45 | 11.33 ± 8.32 | 9 (3.25–18.75) | ||
| ASPECTS | No | 212 | 9.43 ± 0.86 | 10 (9–10) | 0.901 |
| Yes | 46 | 9.5 ± 0.69 | 10 (9–10) | ||
| ASPECTS at 24 h | No | 210 | 7.68 ± 1.59 | 8 (7–9) | 0.002 * |
| Yes | 45 | 8.48 ± 1.23 | 9 (7–9) |
| Variable | Thrombolysis | Valid | Mean ± SD | Median (IQR) | p |
|---|---|---|---|---|---|
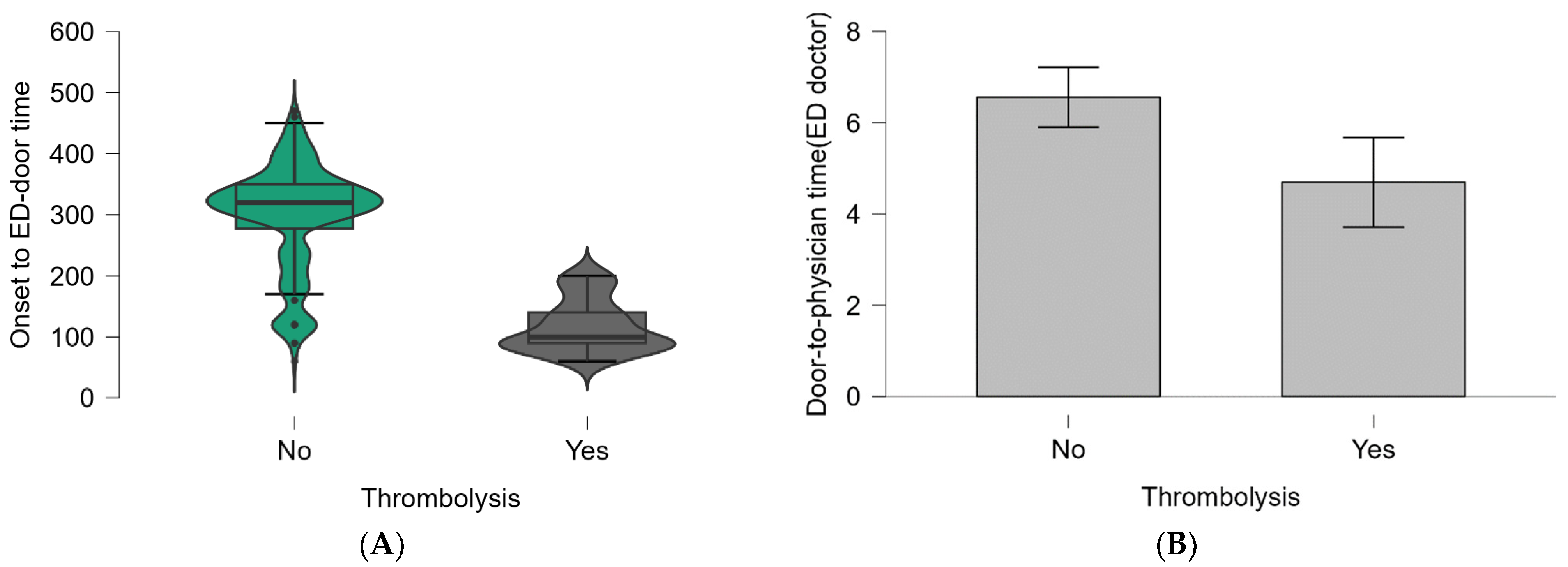
| Onset-to-ED door | No | 212 | 298.63 ± 86.26 | 320 (277.5−350) | <0.001 * |
| Yes | 46 | 116.74 ± 42.69 | 100 (90−140) | ||
| Door-to-physician (ED doctor) | No | 212 | 6.56 ± 4.85 | 5 (3−9) | 0.009 * |
| Yes | 46 | 4.7 ± 3.31 | 4 (2.25−6) | ||
| Door-to-physician (Neurologist) | No | 212 | 7.93 ± 4.88 | 7 (5−10) | 0.786 |
| Yes | 46 | 7.52 ± 3.31 | 8 (5−9) | ||
| Door-to-blood samples | No | 212 | 8.14 ± 2.42 | 10 (5−10) | 0.026 * |
| Yes | 46 | 7.28 ± 2.73 | 5 (5−10) | ||
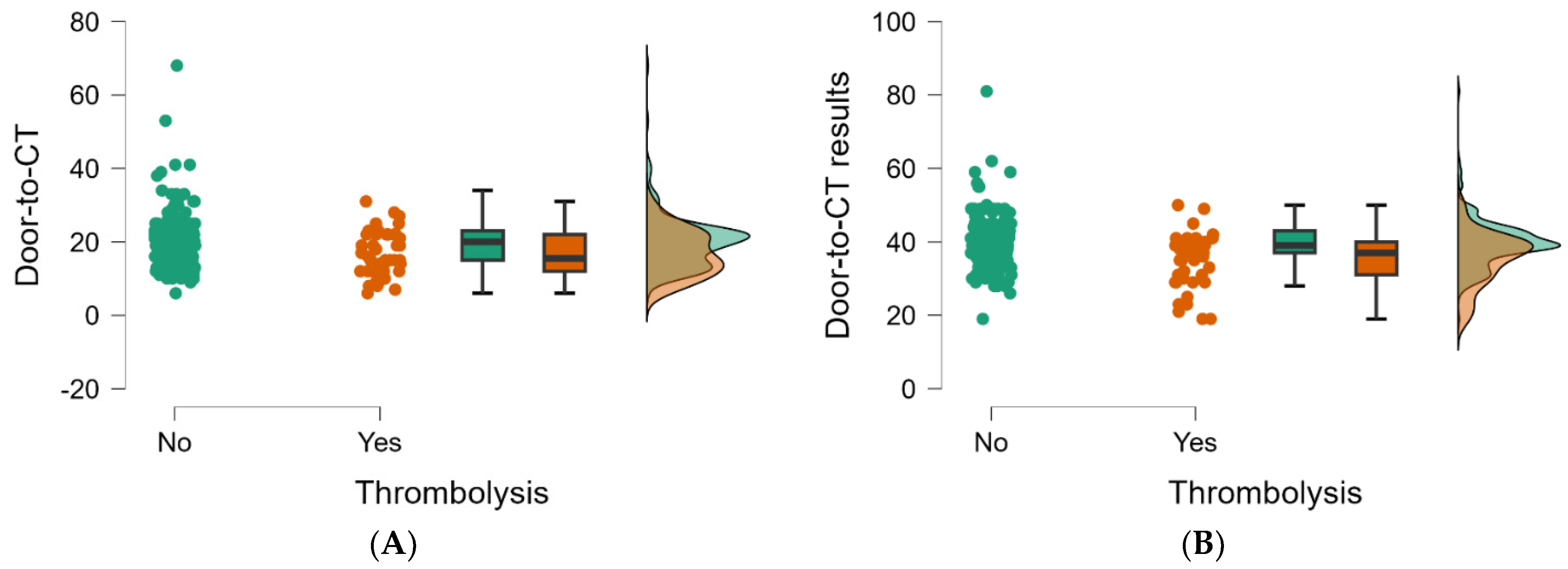
| Door-to-CT | No | 212 | 19.92 ± 7.33 | 20 (15−23) | 0.009 * |
| Yes | 46 | 16.72 ± 6.13 | 15.5 (12−22) | ||
| Door-to-CT results | No | 212 | 39.72 ± 6.68 | 39 (37−43) | <0.001 * |
| Yes | 46 | 35.26 ± 7.15 | 37 (31−40) |
| Variables in the Equation | B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Onset-to-door | −0.232 | 0.017 | 31.105 | 1 | <0.001 * | 0.937 | 0.927 | 0.970 |
| Door-to-physician (ED doctor) | −0.508 | 0.209 | 5.823 | 1 | 0.014 * | 0.506 | 0.450 | 0.941 |
| Door-to-physician (neurologist) | 0.119 | 0.125 | 2.047 | 1 | 0.194 | 1.215 | 0.945 | 1.998 |
| Door-to-blood samples | −0.026 | 0.124 | 0.044 | 1 | 0.782 | 0.955 | 0.431 | 1.570 |
| Door-to-CT | −0.194 | 0.025 | 2.441 | 1 | 0.103 | 0.898 | 0.652 | 1.143 |
| Door-to-CT-results | −0.141 | 0.022 | 1.941 | 1 | 0.107 | 0.902 | 0.815 | 1.227 |
| Constant | 9.408 | 2.355 | 16.104 | 1 | <0.001 * | 11,405.603 | ||
| Variables in the Equation | B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Obesity (Yes) | 0.122 | 0.716 | 0.029 | 1 | 0.865 | 1.129 | 0.277 | 4.600 |
| Smoking (Yes) | 1.195 | 0.660 | 3.283 | 1 | 0.070 | 3.304 | 0.907 | 12.037 |
| Dyslipidemia (Yes) | 2.664 | 1.070 | 6.203 | 1 | 0.013 * | 14.359 | 1.764 | 116.887 |
| Hypertension (Yes) | −2.393 | 0.667 | 12.894 | 1 | <0.001 * | 0.091 | 0.025 | 0.337 |
| Diabetes (Yes) | 1.706 | 0.480 | 12.632 | 1 | <0.001 * | 5.506 | 2.149 | 14.105 |
| CHD (Yes) | 0.028 | 0.461 | 0.004 | 1 | 0.951 | 1.029 | 0.416 | 2.540 |
| COPD (Yes) | 19.563 | 4748.850 | 0.000 | 1 | 0.997 | 313,274,701.511 | 0.000 | |
| CKD (Yes) | 0.808 | 0.534 | 2.292 | 1 | 0.130 | 2.243 | 0.788 | 6.384 |
| Constant | −25.502 | 4748.850 | 0.000 | 1 | 0.996 | 0.000 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popa, D.I.; Buleu, F.; Williams, C.; Tudor, A.; Sutoi, D.; Trebuian, C.I.; Ioan, C.C.; Forțofoiu, D.; Badalica-Petrescu, M.; Petre, I.; et al. Evaluating Thrombolysis Rates and Emergency Department Time Targets in Acute Ischemic Stroke: Need for Personalized Medicine. J. Pers. Med. 2024, 14, 955. https://doi.org/10.3390/jpm14090955
Popa DI, Buleu F, Williams C, Tudor A, Sutoi D, Trebuian CI, Ioan CC, Forțofoiu D, Badalica-Petrescu M, Petre I, et al. Evaluating Thrombolysis Rates and Emergency Department Time Targets in Acute Ischemic Stroke: Need for Personalized Medicine. Journal of Personalized Medicine. 2024; 14(9):955. https://doi.org/10.3390/jpm14090955
Chicago/Turabian StylePopa, Daian Ionel, Florina Buleu, Carmen Williams, Anca Tudor, Dumitru Sutoi, Cosmin Iosif Trebuian, Covasala Constantin Ioan, Dragoș Forțofoiu, Marius Badalica-Petrescu, Ion Petre, and et al. 2024. "Evaluating Thrombolysis Rates and Emergency Department Time Targets in Acute Ischemic Stroke: Need for Personalized Medicine" Journal of Personalized Medicine 14, no. 9: 955. https://doi.org/10.3390/jpm14090955
APA StylePopa, D. I., Buleu, F., Williams, C., Tudor, A., Sutoi, D., Trebuian, C. I., Ioan, C. C., Forțofoiu, D., Badalica-Petrescu, M., Petre, I., Iancu, A., & Mederle, O. A. (2024). Evaluating Thrombolysis Rates and Emergency Department Time Targets in Acute Ischemic Stroke: Need for Personalized Medicine. Journal of Personalized Medicine, 14(9), 955. https://doi.org/10.3390/jpm14090955