

The Relationship between Surrogate Markers of Insulin Resistance and Occurrence of Colorectal Adenoma in Individuals under 50 Years Old: A Single-Center Retrospective Cross-Sectional Study


Abstract
1. Introduction
2. Materials and Methods
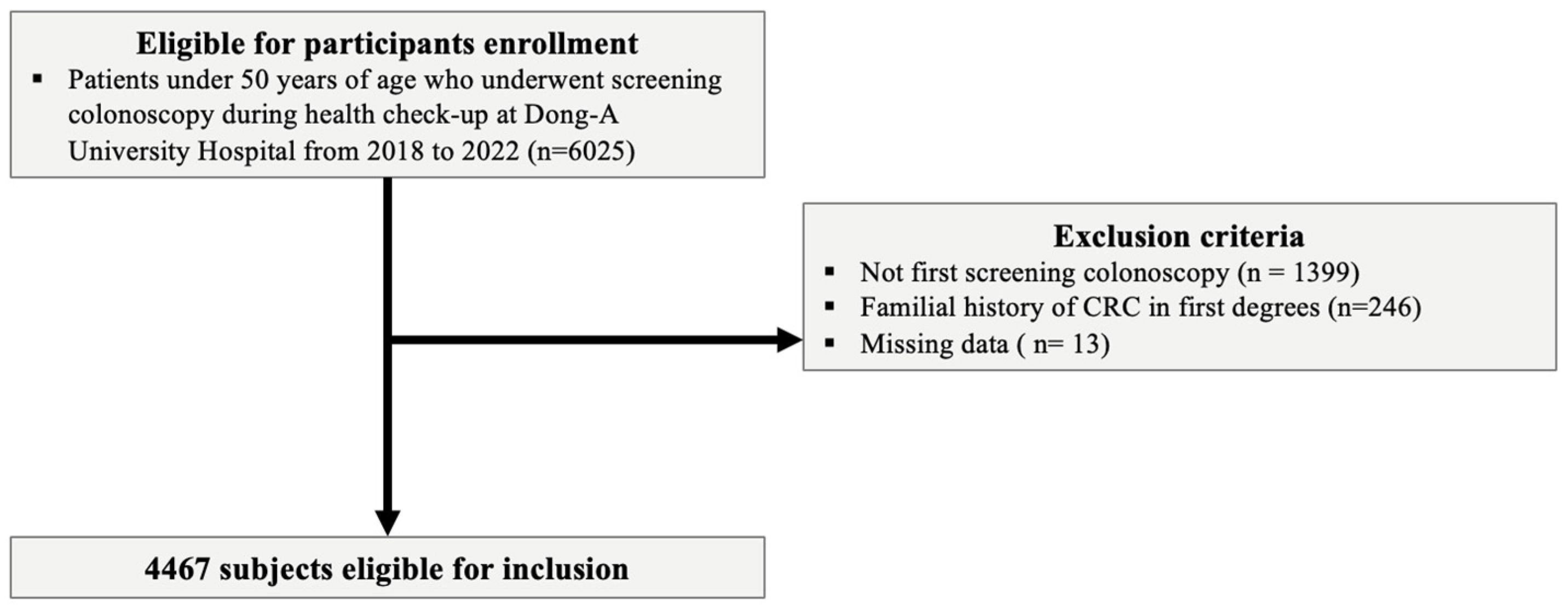
2.1. Study Design and Population
2.2. Definitions of Variables
2.3. Primary Endpoint
2.4. Statistics and Data Analysis
3. Results
3.1. Baseline Characteristics and Clinical Features
3.2. Univariate and Multivariate Analyses of YOAs
3.3. Univariate and Multivariate Analyses of Advanced YOAs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Jasperson, K.W.; Tuohy, T.M.; Neklason, D.W.; Burt, R.W. Hereditary and familial colon cancer. Gastroenterology 2010, 138, 2044–2058. [Google Scholar] [CrossRef] [PubMed]
- Rothwell, J.A.; Jenab, M.; Karimi, M.; Truong, T.; Mahamat-Saleh, Y.; Ferrari, P.; Dashti, S.G.; Kühn, T.; Cross, A.J.; Severi, G.; et al. Metabolic Syndrome and Risk of Gastrointestinal Cancers: An Investigation Using Large-scale Molecular Data. Clin. Gastroenterol. Hepatol. 2022, 20, e1338–e1352. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.T.; Gunathilake, M.; Lee, J.; Kim, J. Association between metabolic syndrome and its components and incident colorectal cancer in a prospective cohort study. Cancer 2022, 128, 1230–1241. [Google Scholar] [CrossRef]
- Singh, B.; Saxena, A. Surrogate markers of insulin resistance: A review. World J. Diabetes 2010, 1, 36–47. [Google Scholar] [CrossRef]
- Low, S.; Khoo, K.C.J.; Irwan, B.; Sum, C.F.; Subramaniam, T.; Lim, S.C.; Wong, T.K.M. The role of triglyceride glucose index in development of Type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2018, 143, 43–49. [Google Scholar] [CrossRef]
- Sánchez-Íñigo, L.; Navarro-González, D.; Fernández-Montero, A.; Pastrana-Delgado, J.; Martínez, J.A. The TyG index may predict the development of cardiovascular events. Eur. J. Clin. Investig. 2016, 46, 189–197. [Google Scholar] [CrossRef]
- Okamura, T.; Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. Triglyceride–glucose index (TyG index) is a predictor of incident colorectal cancer: A population-based longitudinal study. BMC Endocr. Disord. 2020, 20, 113. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; Bjørge, T.; Nagel, G.; Manjer, J.; Engeland, A.; Häggström, C.; Concin, H.; Teleka, S.; Tretli, S.; Gylling, B.; et al. The triglyceride-glucose index as a measure of insulin resistance and risk of obesity-related cancers. Int. J. Epidemiol. 2020, 49, 193–204. [Google Scholar] [CrossRef]
- Son, M.; Moon, S.Y.; Koh, M.; Kang, Y.; Lee, J.Y. Association between Surrogate Markers of Insulin Resistance and the Incidence of Colorectal Cancer in Korea: A Nationwide Population-Based Study. J. Clin. Med. 2024, 13, 1628. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, Q.; Wang, Y.; Ma, X.; Zhang, Q.; Song, M.; Cao, L.; Shi, H. Association between the TyG index and TG/HDL-C ratio as insulin resistance markers and the risk of colorectal cancer. BMC Cancer 2022, 22, 1007. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.G.; Karlitz, J.J.; Yen, T.; Lieu, C.H.; Boland, C.R. The rising tide of early-onset colorectal cancer: A comprehensive review of epidemiology, clinical features, biology, risk factors, prevention, and early detection. Lancet Gastroenterol. Hepatol. 2022, 7, 262–274. [Google Scholar] [CrossRef]
- Daca Alvarez, M.; Quintana, I.; Terradas, M.; Mur, P.; Balaguer, F.; Valle, L. The Inherited and Familial Component of Early-Onset Colorectal Cancer. Cells 2021, 10, 710. [Google Scholar] [CrossRef]
- Chen, H.; Zheng, X.; Zong, X.; Li, Z.; Li, N.; Hur, J.; Fritz, C.D.; Chapman, W., Jr.; Nickel, K.B.; Tipping, A.; et al. Metabolic syndrome, metabolic comorbid conditions and risk of early-onset colorectal cancer. Gut 2021, 70, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Puzzono, M.; Mannucci, A.; Grannò, S.; Zuppardo, R.A.; Galli, A.; Danese, S.; Cavestro, G.M. The Role of Diet and Lifestyle in Early-Onset Colorectal Cancer: A Systematic Review. Cancers 2021, 13, 5933. [Google Scholar] [CrossRef]
- Liu, P.H.; Wu, K.; Ng, K.; Zauber, A.G.; Nguyen, L.H.; Song, M.; He, X.; Fuchs, C.S.; Ogino, S.; Willett, W.C.; et al. Association of Obesity With Risk of Early-Onset Colorectal Cancer Among Women. JAMA Oncol. 2019, 5, 37–44. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, D.E.; Sutherland, R.L.; Town, S.; Chow, K.; Fan, J.; Forbes, N.; Heitman, S.J.; Hilsden, R.J.; Brenner, D.R. Risk Factors for Early-Onset Colorectal Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2022, 20, 1229–1240.e1225. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J.; LeRoith, D. Epidemiology and molecular mechanisms tying obesity, diabetes, and the metabolic syndrome with cancer. Diabetes Care 2013, 36 (Suppl. 2), S233–S239. [Google Scholar] [CrossRef]
- Renehan, A.G.; Zwahlen, M.; Egger, M. Adiposity and cancer risk: New mechanistic insights from epidemiology. Nat. Rev. Cancer 2015, 15, 484–498. [Google Scholar] [CrossRef]
- Harbs, J.; Rinaldi, S.; Gicquiau, A.; Keski-Rahkonen, P.; Mori, N.; Liu, X.; Kaaks, R.; Katzke, V.; Schulze, M.B.; Agnoli, C.; et al. Circulating Sex Hormone Levels and Colon Cancer Risk in Men: A Nested Case-Control Study and Meta-Analysis. Cancer Epidemiol. Biomark. Prev. 2022, 31, 793–803. [Google Scholar] [CrossRef]
- Singh, S.; Sharma, P.; Sarma, D.K.; Kumawat, M.; Tiwari, R.; Verma, V.; Nagpal, R.; Kumar, M. Implication of Obesity and Gut Microbiome Dysbiosis in the Etiology of Colorectal Cancer. Cancers 2023, 15, 1913. [Google Scholar] [CrossRef] [PubMed]
- Bogazzi, F.; Ultimieri, F.; Raggi, F.; Russo, D.; Vanacore, R.; Guida, C.; Viacava, P.; Cecchetti, D.; Acerbi, G.; Brogioni, S. PPARgamma inhibits GH synthesis and secretion and increases apoptosis of pituitary GH-secreting adenomas. Eur. J. Endocrinol. 2004, 150, 863–875. [Google Scholar] [CrossRef] [PubMed]
- Saldeen, J.; Welsh, N. p38 MAPK inhibits JNK2 and mediates cytokine-activated iNOS induction and apoptosis independently of NF-κB translocation in insulin-producing cells. Eur. Cytokine Netw. 2004, 15, 47–52. [Google Scholar] [PubMed]
- Friedrich, N.; Thuesen, B.; Jørgensen, T.; Juul, A.; Spielhagen, C.; Wallaschofksi, H.; Linneberg, A. The association between IGF-I and insulin resistance: A general population study in Danish adults. Diabetes Care 2012, 35, 768–773. [Google Scholar] [CrossRef]
- Li, J.; Chen, J.; Liu, H.; Yan, S.; Wang, Y.; Xing, M.; Ding, S. Association of the triglyceride-glucose index with the occurrence and recurrence of colorectal adenomas: A retrospective study from China. BMC Public Health 2024, 24, 579. [Google Scholar] [CrossRef] [PubMed]
- Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; Kubik, M.; et al. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1965–1977. [Google Scholar] [CrossRef]
- Casey, Y.; Demb, J.; Enwerem, N.; Liu, L.; Jackson, C.; Earles, A.; Bustamante, R.; Mahata, S.; Shah, S.; Gupta, S. Risk of Incident and Fatal Colorectal Cancer After Young-Onset Adenoma Diagnosis: A National Cohort Study. Am. J. Gastroenterol. 2023, 118, 1656–1663. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | All Patients (n = 4467) | Control (n = 3547) | Patients with YOA (n = 920) | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 39.02 ± 6.32 | 38.41 ± 6.36 | 41.36 ± 5.58 | <0.001 |
| Gender male, n (%) | 2448 (54.8) | 1841 (51.9) | 607 (66.0) | <0.001 |
| BMI (mean ± SD) | 23.85 ± 4.84 | 23.67 ± 5.05 | 24.54 ± 3.88 | <0.001 |
| Fasting glucose (mean ± SD) | 90.39 ± 17.13 | 89.54 ± 16.61 | 93.65 ± 18.63 | <0.001 |
| HDL-C (mean ± SD) | 57.34 ± 13.86 | 57.90 ± 13.85 | 55.18 ± 13.68 | <0.001 |
| LDL-C (mean ± SD) | 126.79 ± 30.84 | 125.27 ± 30.53 | 132.67 ± 31.34 | <0.001 |
| TG (mean ± SD) | 114.13 ± 87.70 | 109.18 ± 75.80 | 133.23 ± 121.44 | <0.001 |
| Alcohol consumption, n (%) | 2140 (47.9) | 1665 (46.9) | 475 (51.6) | 0.011 |
| Current smoker, n (%) | 878 (19.7) | 640 (18.0) | 238 (25.9) | <0.001 |
| Medical History | ||||
| Hypertension, n (%) | 238 (5.3) | 152 (4.3) | 86 (9.3) | <0.001 |
| Diabetes, n (%) | 94 (2.1) | 67 (1.9) | 27 (2.9) | 0.053 |
| Dyslipidemia, n (%) | 130 (2.9) | 90 (2.5) | 40 (4.3) | 0.004 |
| TyG index (mean ± SD) | 8.36 ± 0.64 | 8.32 ± 0.61 | 8.51 ± 0.71 | <0.001 |
| TG/HDL-C (mean ± SD) | 2.25 ± 2.17 | 2.12 ± 1.85 | 2.78 ± 3.05 | <0.001 |
| METS-IR (mean ± SD) | 33.91 ± 9.01 | 33.44 ± 9.11 | 35.72 ± 8.37 | <0.001 |
| Characteristics | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR | p Value | OR | p Value | |
| Age | 1.084 (1.070–1.098) | 0.000 | 1.080 (1.066–1.095) | 0.000 |
| Gender Male | 1.797 (1.545–2.097) | 0.000 | 1.520 (1.230–1.877) | 0.000 |
| BMI | 1.044 (1.025–1.064) | 0.000 | 1.003 (0.987–1.019) | 0.740 |
| Fasting Glucose | 1.012 (1.008–1.016) | 0.000 | 1.002 (0.998–1.007) | 0.263 |
| HDL-C | 0.985 (0.980–0.991) | 0.000 | 0.996 (0.990–1.003) | 0.253 |
| LDL-C | 1.008 (1.005–1.010) | 0.000 | 1.004 (1.002–1.006) | 0.002 |
| TG | 1.003 (1.002–1.004) | 0.000 | 1.001 (1.000–1.002) | 0.041 |
| Alcohol consumption | 1.207 (1.044–1.395) | 0.011 | 0.959 (0.813–1.132) | 0.625 |
| Smoker | 0.000 | 0.152 | ||
| Ex-smoker | 1.510 (1.249–1.825) | 0.000 | 1.017 (0.815–1.268) | 0.883 |
| Current smoker | 1.752 (1.466–2.093) | 0.000 | 1.218 (0.982–1.511) | 0.072 |
| Hypertension | 2.303 (1.749–3.033) | 0.000 | 1.458 (1.086–1.957) | 0.012 |
| Diabetes | 1.570 (0.999–2.470) | 0.051 | ||
| Dyslipidemia | 1.746 (1.194–2.552) | 0.004 | 1.098 (0.739–1.633) | 0.643 |
| Characteristics | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR | p Value | OR | p Value | |
| TyG index | 1.552 (1.389–1.733) | 0.000 | 1.064 (1.023–1.325) | 0.021 |
| TG/HDL-C | 1.131 (1.096–1.168) | 0.000 | 1.067 (1.031–1.105) | 0.000 |
| METS-IR | 1.031 (1.022–1.041) | 0.000 | 1.011 (1.002–1.021) | 0.023 |
| Characteristics | All Patients (n = 4467) | Control (n = 4422) | Patients with Advanced YOA (n = 45) | p Value |
|---|---|---|---|---|
| Age (mean ± SD) | 39.02 ± 6.32 | 38.99 ± 6.32 | 41.49 ± 5.27 | 0.004 |
| Gender male, n (%) | 2448 (54.8) | 2415 (54.6) | 33 (73.3) | 0.012 |
| BMI (mean ± SD) | 23.85 ± 4.84 | 23.84 ± 4.85 | 25.29 ± 3.61 | 0.046 |
| Fasting glucose (mean ± SD) | 90.39 ± 17.13 | 90.33 ± 17.09 | 96.16 ± 20.01 | 0.023 |
| HDL-C (mean ± SD) | 57.34 ± 13.86 | 57.39 ± 13.84 | 52.80 ± 15.22 | 0.027 |
| LDL-C (mean ± SD) | 126.79 ± 30.84 | 126.73 ± 30.85 | 133.64 ± 29.85 | 0.134 |
| TG (mean ± SD) | 114.13 ± 87.70 | 113.62 ± 85.73 | 164.53 ± 199.17 | 0.094 |
| Alcohol consumption, n (%) | 2140 (47.9) | 2119 (47.9) | 21 (46.7) | 0.882 |
| Current smoker, n (%) | 878 (19.7) | 864 (19.3) | 14 (31.1) | 0.052 |
| Medical History | ||||
| Hypertension, n (%) | 238 (5.3) | 231 (5.2) | 7 (15.6) | 0.002 |
| Diabetes, n (%) | 94 (2.1) | 93 (2.1) | 1 (2.2) | 0.618 |
| Dyslipidemia, n (%) | 130 (2.9) | 126 (2.8) | 4 (8.9) | 0.041 |
| TyG index (mean ± SD) | 8.36 ± 0.64 | 8.36 ± 0.63 | 8.62 ± 0.85 | 0.045 |
| TG/HDL-C (mean ± SD) | 2.25 ± 2.17 | 2.24 ± 2.11 | 3.69 ± 5.22 | 0.069 |
| METS-IR (mean ± SD) | 33.91 ± 9.01 | 33.87 ± 9.01 | 37.70 ± 8.49 | 0.005 |
| Characteristics | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR | p Value | OR | p Value | |
| TyG | 1.769 (1.177–2.659) | 0.006 | 1.288 (0.804–2.064) | 0.292 |
| TG/HDL-C | 1.120 (1.053–1.191) | 0.000 | 1.078 (1.006–1.155) | 0.032 |
| METS-IR | 1.014 (1.002–1.027) | 0.022 | 1.009 (0.994–1.025) | 0.245 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, C.H.; Moon, S.Y.; Lee, J.Y. The Relationship between Surrogate Markers of Insulin Resistance and Occurrence of Colorectal Adenoma in Individuals under 50 Years Old: A Single-Center Retrospective Cross-Sectional Study. J. Pers. Med. 2024, 14, 971. https://doi.org/10.3390/jpm14090971
Choi CH, Moon SY, Lee JY. The Relationship between Surrogate Markers of Insulin Resistance and Occurrence of Colorectal Adenoma in Individuals under 50 Years Old: A Single-Center Retrospective Cross-Sectional Study. Journal of Personalized Medicine. 2024; 14(9):971. https://doi.org/10.3390/jpm14090971
Chicago/Turabian StyleChoi, Chi Hyeon, Sang Yi Moon, and Jong Yoon Lee. 2024. "The Relationship between Surrogate Markers of Insulin Resistance and Occurrence of Colorectal Adenoma in Individuals under 50 Years Old: A Single-Center Retrospective Cross-Sectional Study" Journal of Personalized Medicine 14, no. 9: 971. https://doi.org/10.3390/jpm14090971
APA StyleChoi, C. H., Moon, S. Y., & Lee, J. Y. (2024). The Relationship between Surrogate Markers of Insulin Resistance and Occurrence of Colorectal Adenoma in Individuals under 50 Years Old: A Single-Center Retrospective Cross-Sectional Study. Journal of Personalized Medicine, 14(9), 971. https://doi.org/10.3390/jpm14090971