
Applicability of the Cumberland Ankle Instability Tool in Elite Volleyball Athletes: A Cross-Sectional Observational Study

 ,
,  ,
,  ,
, 
 ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants and Procedure
2.3. The Cumberland Ankle Instability Tool (CAIT)
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yeung, M.S.; Chan, K.M.; So, C.H.; Yuan, W.Y. An epidemiological survey on ankle sprain. Br. J. Sports Med. 1994, 28, 112–116. [Google Scholar] [CrossRef]
- Nozu, S.; Takemura, M.; Sole, G. Assessments of Sensorimotor Deficits Used in Randomized Clinical Trials with Individuals with Ankle Sprains and Chronic Ankle Instability: A Scoping Review. PM&R 2021, 13, 901–914. [Google Scholar] [CrossRef]
- Hertel, J. Sensorimotor deficits with ankle sprains and chronic ankle instability. Clin. Sports Med. 2008, 27, 353–370. [Google Scholar] [CrossRef]
- Bonnel, F.; Toullec, E.; Mabit, C.; Tourne, Y.; Sofcot. Chronic ankle instability: Biomechanics and pathomechanics of ligaments injury and associated lesions. Orthop. Traumatol. Surg. Res. 2010, 96, 424–432. [Google Scholar] [CrossRef]
- Skazalski, C.; Kruczynski, J.; Bahr, M.A.; Bere, T.; Whiteley, R.; Bahr, R. Landing-related ankle injuries do not occur in plantarflexion as once thought: A systematic video analysis of ankle injuries in world-class volleyball. Br. J. Sports Med. 2018, 52, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Agel, J.; Palmieri-Smith, R.M.; Dick, R.; Wojtys, E.M.; Marshall, S.W. Descriptive Epidemiology of Collegiate Women’s Volleyball Injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J. Athl. Train. 2007, 42, 295–302. [Google Scholar] [PubMed]
- van der Does, H.T.D.; Brink, M.S.; Benjaminse, A.; Visscher, C.; Lemmink, K. Jump Landing Characteristics Predict Lower Extremity Injuries in Indoor Team Sports. Int. J. Sports Med. 2016, 37, e10. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.A. Instability of the foot after injuries to the lateral ligament of the ankle. J. Bone Jt. Surg. Br. 1965, 47, 669–677. [Google Scholar] [CrossRef]
- Lian, J.; Sewani, F.; Dayan, I.; Voleti, P.B.; Gonzalez, D.; Levy, I.M.; Musahl, V.; Allen, A. Systematic Review of Injuries in the Men’s and Women’s National Basketball Association. Am. J. Sports Med. 2022, 50, 1416–1429. [Google Scholar] [CrossRef] [PubMed]
- Giustino, V.; Messina, G.; Patti, A.; Padua, E.; Zangla, D.; Drid, P.; Battaglia, G.; Palma, A.; Bianco, A. Effects of a Postural Exercise Program on Vertical Jump Height in Young Female Volleyball Players with Knee Valgus. Int. J. Environ. Res. Public Health 2022, 19, 3953. [Google Scholar] [CrossRef]
- Schwesig, R.; Hermassi, S.; Wagner, H.; Fischer, D.; Fieseler, G.; Molitor, T.; Delank, K.S. Relationship Between the Range of Motion and Isometric Strength of Elbow and Shoulder Joints and Ball Velocity in Women Team Handball Players. J. Strength Cond. Res. 2016, 30, 3428–3435. [Google Scholar] [CrossRef]
- McKean, M.R.; Burkett, B. The relationship between joint range of motion, muscular strength, and race time for sub-elite flat water kayakers. J. Sci. Med. Sport 2010, 13, 537–542. [Google Scholar] [CrossRef]
- Bere, T.; Kruczynski, J.; Veintimilla, N.; Hamu, Y.; Bahr, R. Injury risk is low among world-class volleyball players: 4-year data from the FIVB Injury Surveillance System. Br. J. Sports Med. 2015, 49, 1132–1137. [Google Scholar] [CrossRef]
- Panoutsakopoulos, V.; Kotzamanidou, M.C.; Papaiakovou, G.; Kollias, I.A. The Ankle Joint Range of Motion and Its Effect on Squat Jump Performance with and without Arm Swing in Adolescent Female Volleyball Players. J. Funct. Morphol. Kinesiol. 2021, 6, 14. [Google Scholar] [CrossRef]
- Flores, D.F.; Gentil, P.; Brown, L.E.; Pinto, R.S.; Carregaro, R.L.; Bottaro, M. Dissociated time course of recovery between genders after resistance exercise. J. Strength Cond. Res. 2011, 25, 3039–3044. [Google Scholar] [CrossRef] [PubMed]
- Monteleone, G.; Tramontana, A.; Sorge, R.; Tiloca, A.; Roselli, M. Ankle sprain and podoscopic footprint pattern in female volleyball players. Acta Orthop. Belg. 2023, 89, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland ankle instability tool: A report of validity and reliability testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef]
- Sanchez-Alcaraz, B.J.; Jimenez, V.; Munoz, D.; Ramon-Llin, J. External Training Load Differences between Male and Female Professional Padel. J. Sport. Health Res. 2021, 13, 445–454. [Google Scholar]
- Martin, R.L.; Irrgang, J.J.; Lalonde, K.A.; Conti, S. Current concepts review: Foot and ankle outcome instruments. Foot Ankle Int. 2006, 27, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.; Fourchet, F.; Fong, D.T.; Hertel, J.; Hiller, C.; Kaminski, T.; et al. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. Br. J. Sports Med. 2014, 48, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Yingyongsaksri, S.; Hiller, C.E.; Tharawadeepimuk, K.; Nanbancha, A. Reliability and validation of the Thai version of the Cumberland Ankle Instability Tool (CAIT-THA). Disabil. Rehabil. 2023, 45, 3762–3767. [Google Scholar] [CrossRef] [PubMed]
- Olszewski, M.; Zajac, B.; Golec, J. Cross cultural adaptation, reliability and validity of the Polish version of the Cumberland Ankle Instability Tool. Disabil. Rehabil. 2023, 68, 102873. [Google Scholar] [CrossRef] [PubMed]
- Jayalath, L.; Senanayake, K.; Deeghanu, M.; Pathirana, C. Cross-cultural adaptation, reliability, and validity of the Sinhala version of the Cumberland Ankle Instability Tool: An instrument for measuring chronic ankle instability in Sri Lanka. Disabil. Rehabil. 2023, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hui, J.Y.; Tong, A.H.; Chui, V.W.; Fong, D.T.P.; Chau, W.W.; Yung, P.S.; Ling, S.K. Cross-cultural adaptation, reliability and validity of the Cantonese-Chinese Cumberland Ankle Instability Tool (CAIT-HK). Foot 2023, 56, 102015. [Google Scholar] [CrossRef] [PubMed]
- Contri, A.; Ballardin, F.; De Marco, G.; Gaucci, M.; Scariato, A.; Zanoni, V.; Vanti, C.; Pillastrini, P. Italian version of the Cumberland Ankle Instability Tool (CAIT-I). Foot 2023, 56, 102043. [Google Scholar] [CrossRef] [PubMed]
- Candeniz, S.; Kocaman, H.; Erol Celik, S.; Bek, N. Cross-Cultural Adaptation, Reliability, and Validity of the Turkish Version of the Cumberland Ankle Instability Tool. Musculoskelet. Sci. Pract. 2023, 68, 102873. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.I.; Mayer, F.; Wippert, P.M. Cross-Cultural Adaptation, Reliability, and Validation of the Taiwan-Chinese Version of Cumberland Ankle Instability Tool. Disabil. Rehabil. 2022, 44, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Liao, D.; Kang, X.; Zheng, W.; Xu, W.; Chen, S.; Xie, Q. Development of a valid Chinese version of the Cumberland Ankle Instability Tool in Chinese-speaking patients with chronic ankle instability disorders. Sci. Rep. 2021, 11, 9747. [Google Scholar] [CrossRef]
- Kadli, S.; Lekskulchai, R.; Jalayondeja, C.; Hiller, C.E. Cross-cultural adaptation of the Cumberland Ankle Instability Tool—Youth Thai version. Pediatr. Int. 2020, 62, 1374–1380. [Google Scholar] [CrossRef]
- Mirshahi, M.; Halabchi, F.; Golbakhsh, M.; Saadat, S. Reliability and Recalibration of the Persian Version of Cumberland Ankle Instability Tool Cut-off Score in Athletes with Functional Ankle Instability. Adv. J. Emerg. Med. 2019, 3, e26. [Google Scholar] [CrossRef]
- Wang, L.; Ye, J.; Zhang, X. Ankle biomechanics of the three-step layup in a basketball player with chronic ankle instability. Sci. Rep. 2023, 13, 18667. [Google Scholar] [CrossRef]
- Navarro-Santana, M.J.; Albert-Lucena, D.; Gomez-Chiguano, G.F.; Plaza-Manzano, G.; Fernandez-de-Las-Penas, C.; Cleland, J.; Perez-Silvestre, A.; Asin-Izquierdo, I. Pressure pain sensitivity over nerve trunk areas and physical performance in amateur male soccer players with and without chronic ankle instability. Phys. Ther. Sport 2019, 40, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Kunugi, S.; Masunari, A.; Yoshida, N.; Miyakawa, S. Association between Cumberland Ankle Instability Tool score and postural stability in collegiate soccer players with and without functional ankle instability. Phys. Ther. Sport 2018, 32, 29–33. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Michels, F.; Wastyn, H.; Pottel, H.; Stockmans, F.; Vereecke, E.; Matricali, G. The presence of persistent symptoms 12 months following a first lateral ankle sprain: A systematic review and meta-analysis. Foot Ankle Surg. 2022, 28, 817–826. [Google Scholar] [CrossRef]
- Wright, C.J.; Arnold, B.L.; Ross, S.E.; Linens, S.W. Recalibration and validation of the Cumberland Ankle Instability Tool cutoff score for individuals with chronic ankle instability. Arch. Phys. Med. Rehabil. 2014, 95, 1853–1859. [Google Scholar] [CrossRef]
- Bonavolonta, V.; Cataldi, S.; Latino, F.; Carvutto, R.; De Candia, M.; Mastrorilli, G.; Messina, G.; Patti, A.; Fischetti, F. The Role of Parental Involvement in Youth Sport Experience: Perceived and Desired Behavior by Male Soccer Players. Int. J. Environ. Res. Public Health 2021, 18, 8698. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.; Manion, L.; Morrison, K. Research Methods in Education. In Research Methods in Education, 5th ed.; Routledge Falmer: London, UK, 2000. [Google Scholar] [CrossRef]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Bowring, A.; Telschow, F.J.E.; Schwartzman, A.; Nichols, T.E. Confidence Sets for Cohen’s d effect size images. Neuroimage 2021, 226, 117477. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Chicco, D.; Warrens, M.J.; Jurman, G. The coefficient of determination R-squared is more informative than SMAPE, MAE, MAPE, MSE and RMSE in regression analysis evaluation. PeerJ Comput. Sci. 2021, 7, e623. [Google Scholar] [CrossRef] [PubMed]
- Hadzic, V.; Sattler, T.; Pori, P.; Veselko, M.; Dervisevic, E.; Sarabon, N.; Markovic, G. Quadriceps strength asymmetry as predictor of ankle sprain in male volleyball players. J. Sports Med. Phys. Fit. 2022, 62, 822–829. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| A | Participants (n) | No Injury Group Total Score CAIT | Participants (n) | Injury Group Total Score CAIT | p | Effect Size |
| Right Ankle | 66 | 22.3 ± 6.59 | 14 | 17.2 ± 9.99 | 0.084 | 0.295 |
| Left Ankle | 67 | 22.2 ± 5.82 | 13 | 20.2 ± 8.74 | 0.724 | 0.0631 |
| B | Participants (n) | Pain Group Total Score CAIT | Participants (n) | No Pain Group Total Score CAIT | p | Effect Size |
| Right Ankle | 35 | 15.3 ± 7.05 | 45 | 26.2 ± 2.88 | <0.001 | 0.911 |
| Left Ankle | 39 | 17.2 ± 5.68 | 41 | 26.4 ± 2.61 | <0.001 | 0.906 |
| Predictor | Estimate | SE | t | p |
|---|---|---|---|---|
| Intercept | 269.164 | 1.10 | 244.421 | <0.001 |
| Any previous ankle injuries? | ||||
| Yes–No | −33.289 | 1.52 | −21.969 | 0.031 |
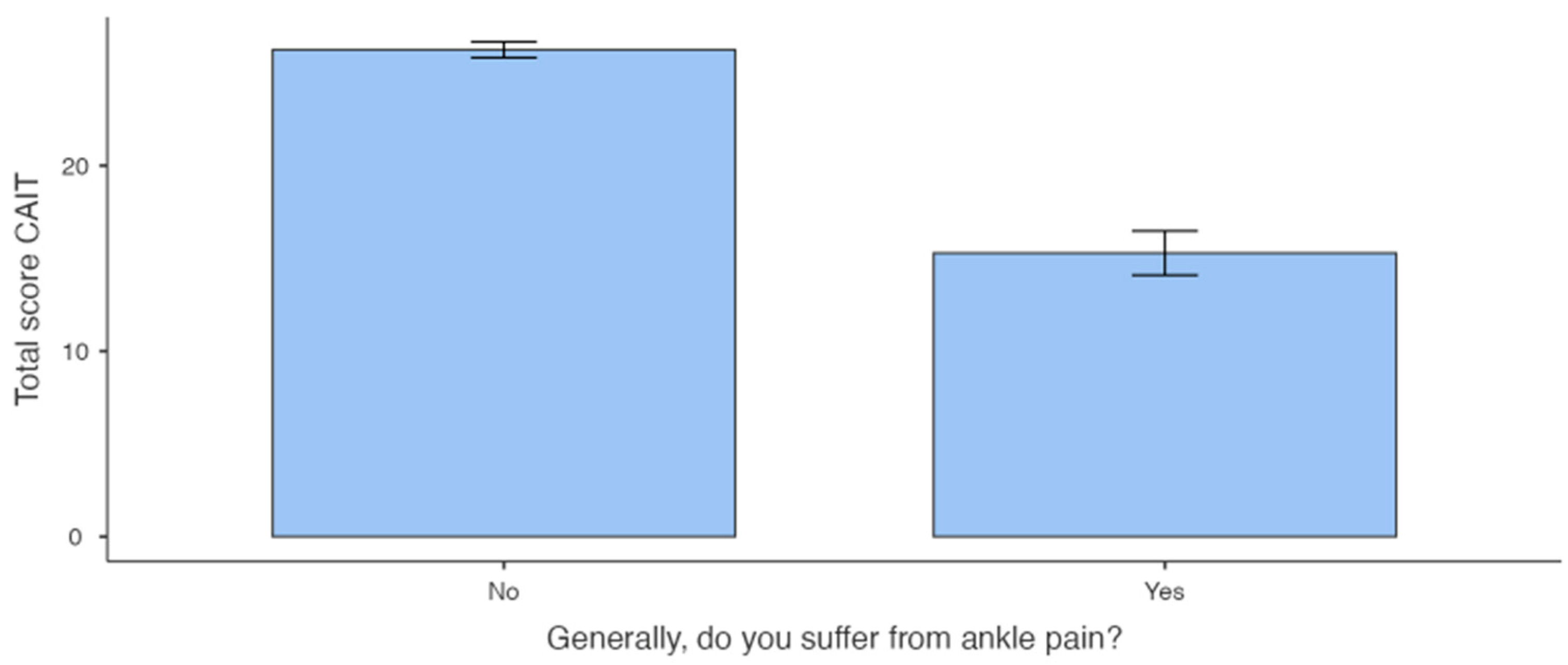
| Generally, do you suffer from ankle pain? | ||||
| Yes–No | −106.563 | 1.15 | −93.000 | <0.001 |
| Series: | ||||
| B–C | 0.0681 | 1.31 | 0.0521 | 0.959 |
| A–C | −10.445 | 1.48 | −0.7060 | 0.482 |
| Predictor | Estimate | SE | t | p |
|---|---|---|---|---|
| Intercept | 26.397 | 1.167 | 22.624 | <0.001 |
| Any previous ankle injuries? | ||||
| Yes–No | −2.299 | 1.332 | −1.726 | 0.089 |
| Generally, do you suffer from ankle pain? | ||||
| Yes–No | −9.235 | 0.981 | −9.416 | <0.001 |
| Series: | ||||
| B–C | 0.497 | 1.281 | 0.388 | 0.699 |
| A–C | 0.429 | 1.286 | −0.334 | 0.740 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Figlioli, F.; Belmonte, G.; Giustino, V.; Canzone, A.; Ferrantello, E.; Gervasi, M.; Fernández-Peña, E.; Battaglia, G.; Bianco, A.; Patti, A. Applicability of the Cumberland Ankle Instability Tool in Elite Volleyball Athletes: A Cross-Sectional Observational Study. Sports 2024, 12, 71. https://doi.org/10.3390/sports12030071
Figlioli F, Belmonte G, Giustino V, Canzone A, Ferrantello E, Gervasi M, Fernández-Peña E, Battaglia G, Bianco A, Patti A. Applicability of the Cumberland Ankle Instability Tool in Elite Volleyball Athletes: A Cross-Sectional Observational Study. Sports. 2024; 12(3):71. https://doi.org/10.3390/sports12030071
Chicago/Turabian StyleFiglioli, Flavia, Giacomo Belmonte, Valerio Giustino, Alberto Canzone, Elena Ferrantello, Marco Gervasi, Eneko Fernández-Peña, Giuseppe Battaglia, Antonino Bianco, and Antonino Patti. 2024. "Applicability of the Cumberland Ankle Instability Tool in Elite Volleyball Athletes: A Cross-Sectional Observational Study" Sports 12, no. 3: 71. https://doi.org/10.3390/sports12030071
APA StyleFiglioli, F., Belmonte, G., Giustino, V., Canzone, A., Ferrantello, E., Gervasi, M., Fernández-Peña, E., Battaglia, G., Bianco, A., & Patti, A. (2024). Applicability of the Cumberland Ankle Instability Tool in Elite Volleyball Athletes: A Cross-Sectional Observational Study. Sports, 12(3), 71. https://doi.org/10.3390/sports12030071