Abstract
Positive effects from sports are achieved primarily through physical activity, but secondary effects bring health benefits such as psychosocial and personal development and less alcohol consumption. Negative effects, such as the risk of failure, injuries, eating disorders, and burnout, are also apparent. Because physical activity is increasingly conducted in an organized manner, sport’s role in society has become increasingly important over the years, not only for the individual but also for public health. In this paper, we intend to describe sport’s physiological and psychosocial health benefits, stemming both from physical activity and from sport participation per se. This narrative review summarizes research and presents health-related data from Swedish authorities. It is discussed that our daily lives are becoming less physically active, while organized exercise and training increases. Average energy intake is increasing, creating an energy surplus, and thus, we are seeing an increasing number of people who are overweight, which is a strong contributor to health problems. Physical activity and exercise have significant positive effects in preventing or alleviating mental illness, including depressive symptoms and anxiety- or stress-related disease. In conclusion, sports can be evolving, if personal capacities, social situation, and biological and psychological maturation are taken into account. Evidence suggests a dose–response relationship such that being active, even to a modest level, is superior to being inactive or sedentary. Recommendations for healthy sports are summarized.
1. Introduction
Sport is a double-edged sword regarding effects on health. Positive effects are achieved primarily through physical activity, which is the main part of most sports. Many secondary effects of sport also bring health benefits, such as psychosocial development of both young [1] and old [2], personal development [3], later onset, and less consumption of alcohol [4,5]. Finally, those who play sports have a higher level of physical activity later in life [6], and through sport, knowledge of nutrition, exercise, and health can be developed [7]. Negative effects include the risk of failure leading to poor mental health [8,9], risk of injury [10,11], eating disorders [12], burnout [13], and exercise-induced gastrointestinal tract discomfort [14]. In sport, there are unfortunately also reports of physical and psychological abuse [15]. Negative aspects are more common in elite-level sports, where there is a fine balance between maximum performance and negative health. A somewhat unexpected effect of sport participation is that people submitting to planned training in some cases perform less physical activity compared to those who are exercising without a set schedule. One explanation can be a reduced spontaneous physical activity in the latter group [16]. Because physical activity is increasingly executed in an organized manner [17,18,19], sport’s role in society has become increasingly important over the years, not only for the individual but also for public health.
In this paper, we describe the health effects of sport from a physiological and psychological perspective, related both to physical activity and added values of sport per se. Initially, brief definitions of various concepts related to physical activity and health are given. This is then followed by: (1) A brief description of how physical activity and training affect our body from a physiological perspective; (2) a report on the health effects of physical activity and training; and (3) sport’s specific influences on the various dimensions of health. We chose to discuss the subject from an age-related perspective, separating children/adolescents, adults, and the elderly, as well as separating for sex in each age group.
2. Definitions of Physical Activity, Exercise, Training, Sport, and Health
Definitions and terms are based on “Physical activity in the prevention and treatment of disease” (FYSS, www.fyss.se [Swedish] [20]), World Health Organization (WHO) [21] and the US Department of Human Services [22]. The definition of physical activity in FYSS is: “Physical activity is defined purely physiologically, as all body movement that increases energy use beyond resting levels”. Health is defined according to the World Health Organization (WHO) as: “[…] a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity” [21].
Physical activity can occur spontaneously (leisure/work/transport) or organized and be divided according to purpose: Physical exercise is aimed primarily at improving health and physical capacity. Physical training is aimed primarily at increasing the individual’s maximum physical capacity and performance [23]. Physical inactivity is described as the absence of body movement, when energy consumption approximates resting levels. People who do not meet recommendations for physical activity are considered physically inactive and are sometimes called “sedentary”. Sport can be organized by age, sex, level of ambition, weight or other groupings [24]. Sport can also be spontaneous [7,17] and defined as a subset of exercises undertaken individually or as a part of a team, where participants have a defined goal [7]. General recommendations for physical activity are found in Table 1, not considering everyday activities. One can meet the daily recommendations for physical activity by brief, high-intensity exercise, and remaining physically inactive for the rest of the day, thereby creating a “polarization” of physical activity: Having a high dose of conscious physical training, despite having a low energy expenditure in normal life due to high volumes of sedentary time. Polarization of physical activity may lead to increased risk of poor health despite meeting the recommendations for physical activity [25,26,27]. During most of our lives, energy expenditure is greater in normal daily life than in sport, physical training, and exercise, with the exceptions of children and the elderly, where planned physical activity is more important [28].

Table 1.
Recommendations regarding physical activity for different target groups. Note that additional health effects can be achieved if, in addition to these recommendations, the amount of physical activity increases, either by increasing the intensity or duration or a combination of both.
3. Aerobic and Muscle-Strengthening Physical Activity
Physical activity is categorized according to FYSS as: (1) Aerobic physical activity and (2) muscle-strengthening physical activity. Physical activity in everyday life and exercise training is mainly an aerobic activity, where a majority of energy production occurs via oxygen-dependent pathways. Aerobic physical activity is the type of activity typically associated with stamina, fitness, and the biggest health benefits [29,30,31]. Muscle-strengthening physical activity is referred to in everyday language as “strength training” or “resistance training” and is a form of physical exercise/training that is primarily intended to maintain or improve various forms of muscle strength and increase or maintain muscle mass [32]. Sometimes, another category is defined: Muscle-enhancing physical activity, important for maintenance or improvement of coordination and balance, especially in the elderly [33]. According to these definitions, muscle-strengthening activities primarily involve the body’s anaerobic (without oxygen) energy systems, proportionally more as intensity increases.
Exercise intensity can be expressed in absolute or relative terms. Absolute intensity means the physical work (for example; Watts [W], kg, or metabolic equivalent [MET]), while relative intensity is measured against the person’s maximum capacity or physiology (for example; percentage of maximum heart rate (%HR), rate of perceived exhaustion (RPE), W·kg−1 or relative oxygen uptake in L·min−1·kg−1 (VO2)). In terms of recommendations to the public, as in Table 1, the intensity is often described in subjective terms (“makes you breathe harder” for moderate intensity, and “makes you puff and pant” for vigorous intensity) [27]. While objective criteria such as heart rate and accelerometry will capture the intensity of activity, they may not distinguish between different types of physical activity behaviors [34]. FYSS defines low intensity as 20%–39% of VO2max, <40 %HR, 1.5–2.9 METs; moderate intensity as 40%–59% of VO2max, 60–74 %HR, 3.0–5.9 METs, and vigorous intensity as 60%–89% of VO2max, 75–94 %HR, 6.0–8.9 METs. Absolute intensity, however, can vary greatly between individuals where a patient with heart disease may have a maximal capacity of <3 MET, and an elite athlete >20 MET [35].
4. How does the Body Adapt to Physical Activity and Training?
Adaption to physical activity and training is a complex physiological process, but may, in the context of this paper, be simplified by a fundamental basic principle:” The general adaptation syndrome (GAS)” [36,37,38]. This principle assumes that physical activity disturbs the body’s physiological balance, which the body then seeks to restore, all in a dose-related response relationship. The overload principle states that if exercise intensity is too low, overload is not reached to induce desired physiological adaptations, whereas an intensity too high will result in fatigue and possibly overtraining. Thus, for adaptation to occur, greater than normal stress must be induced, interspersed with sufficient recovery periods for restoration of physiological balance [39]. During and immediately after physical exercise/training, functions of affected tissues and systems are impaired, manifested as temporarily decreased performance. You feel tired. In order to gradually improve performance capacity, repeated cycles of adequate overload and recovery are required [40]. In practice, positive effects can be seen after a relatively short period of a few weeks, but more substantial improvements if the training is maintained for a longer period.
As a rule of thumb, it is assumed that all people can adapt to physical activity and exercise, but the degree of adaptation depends on many factors, including age, heredity, the environment, and diet [41,42,43,44]. The hereditary factor (genetics) may be the most critical for adaptation [45]. The degree of adaptation also depends on how the person in question trained previously; a well-trained athlete usually does not have the same relative improvement as an untrained one. Even if training is thought to be specific to mode, intensity, and duration, there are some overlaps. For example, it has been found that strength training in some individuals contributes to a relatively large positive impact on health and endurance, effects previously associated primarily with aerobic exercise [46,47]. The overload principle may, if applied too vigorously in relation to a person’s individual adaptation ability, have detrimental effects, including reduced performance, injury, overtraining, and disease [10]. Training is a commodity that must be renewed; otherwise, you gradually lose achieved performance improvements [48], although some capacities, such as muscle memory, seem to persist for life [49].
General recommendations for health may be stated, but individual predispositions make general training schedules for specific performance effects unpredictable. All exercise training should be adjusted to individual purposes, goals, and circumstances.
5. Health Effects of Physical Activity and Training
Human biology requires a certain amount of physical activity to maintain good health and wellbeing. Biological adaption to life with less physical activity would take many generations. People living today have, more or less, the same requirements for physical activity as 40,000 years ago [50,51]. For an average man with a body weight of 70 kg, this corresponds to about 19 km daily walking in addition to everyday physical activity [52]. For most people, daily physical activity decreases, while planned, conscious exercise and training increases [19,53]. Unfortunately, average daily energy intake is increasing more than daily energy output, creating an energy surplus. This is one reason for the increasing number of overweight people, and a strong contributor to many health problems [54]. More sedentary living (not reaching recommended level of physical activity), combined with increased energy intake, impairs both physical and mental capabilities and increases the risk of disease. Despite this, Swedes (as an example) seemed to be as physically active and stressed but had better general health in 2015, compared to 2004 (Figure 1). Compared to 2004–2007, the Swedish population in 2012–2015 reported better overall health (more county-dots are blue) and less fatigue (smaller county-dots) with similar level of physical activity (~65% indicated at least 30 min daily physical activity) and stress (~13% were stressed).
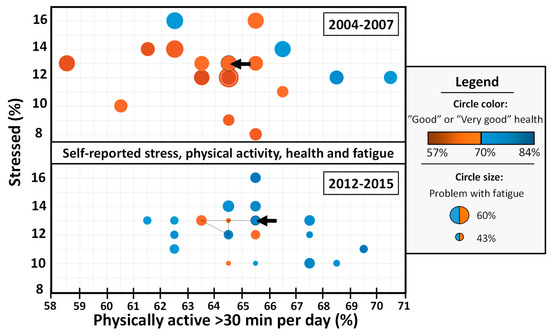
Figure 1.
Selected physical and mental health indicators of a Sweden cohort, in relation to the degree of physical activity for the period of years 2004–2007 (N = 29,254) and years 2012–2015 (N = 38,553). Surveyed subjects are age 16 to 84 years old, with data representing median scores of four years, not normalized for age. Y-axis: Percentage of subjects reporting “stressed”; X-axis: Percentage of subjects indicating physical active at least 30 minutes each day. Each dot represents one County (Län), dot-size indicates self-reported fatigue, and color self-reported healthiness of the County. If 70% of the population states they are having “Good/Very good” health, the dot is blue. If less than 70% states they are having good/very good health, the dot is red. The circle indicated with a black arrow corresponds to nation median. The black line connected to the nation circle represents the movement in the X–Y plane from the year 2004 to 2007, and from 2012 to 2015, respectively. Data retrieved from the Public Health Agency of Sweden 2019-04-22 (www.folkhalsomyndigheten.se).
Results in Figure 1 may in part be explained by a polarization of who is physically active: Some individuals are extremely active, others very inactive, giving a similar central tendency (mean/median). As physical activity and mental stress are not changed, but health is, the figure indicates that other factors must be more important to our overall health and fatigue. Recently, a national study of Swedish 11- to 15-year-olds concluded that this age group is inactive for most of their time awake, that is, sitting, standing or moving very little [55]. Time as inactive increased with age, from 67 percent for 11-year-olds to 75 percent for 15-year-olds. The study states that in all age groups, the inactive time is evenly distributed over the week, with school time, leisure time, and weekend. Further, those who feel school-related stress have more inactive time, both overall and during school hours, than those who have less school-related stress.
People active in sports have, in general, better health than those who do not participate in sports, because they are physically and mentally prepared for the challenges of sports, abilities that in many cases can be transferred to other parts of life [56].
However, there is a certain bias in this statement. Sport practitioners are already positively selected, because sickness and injury may prevent participation. As many health benefits of sport are related to the level of physical activity, separation of sport and physical exercise may be problematic. Regardless, societal benefits of these health effects can be seen in lower morbidity, healthier elderly, and lower medical costs [7,57,58].
Health effects of physical activity in many cases follow a dose–response relationship; dose of physical activity is in proportion to the effect on health [59,60]. Figure 2 depicts the relationship between risk of death and level of physical activity, in a Finnish twin cohort, adjusted for smoking, occupational group, and alcohol consumption [59]. Odds ratio (OR) for the risk of all-cause mortality in a larger sample in the same study was 0.80 for occasional exercisers (p = 0.002, 95% CI = 0.69–0.91). This dose–response relationship between risk of all-cause mortality and physical activity is evident in several extensive studies [60,61,62]. The total dose is determined by the intensity (how strenuous), duration (duration), and frequency (how often). While Figure 2 shows sex differences in death rates, it is likely that sedentary behavior is equally hazardous for men and women, but inconsistent results sometime occur due to inadequate assessment measures, or low statistical power [59,63]. To obtain the best possible development due to physical exercise/training, both for prevention and treatment purposes, a basic understanding of how these variables affect the dose of activity is required, as well as understanding how they can be modified to suit individual requirements. A physically active population is important for the health of both the individual and society, with sport participation being one, increasingly important, motivator for exercise.
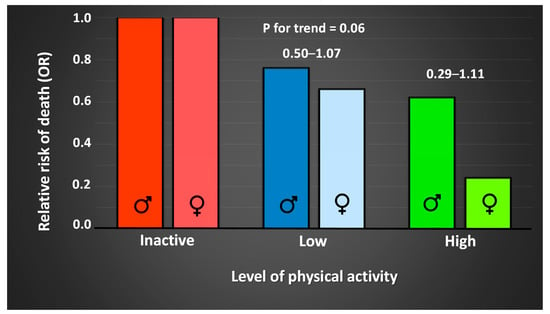
Figure 2.
Relative risk (odds ratio; OR) of premature death in relationship to level of physical activity, in 286 male and 148 female twin pairs, adjusted for smoking, occupational group, and use of alcohol [59].
There is strong scientific evidence supporting an association between physical exercise/training and good physical and mental health. For example: A reduction in musculoskeletal disorders and reduced disability due to chronic disease [27,64], better mental health with reduced anxiety [65,66], insomnia [67], depression [31], stress [68], and other psychological disorders [69]. Physical and mental health problems are related to an increased risk of developing a number of our major public health diseases and may contribute to premature death (Table 2).
Table 2.
Health-related physiological effects of aerobic and muscle strengthening physical activity. Green circle indicates that the activity contributes with an effect, whereas a red circle indicates that the activity has no proven effect. Orange circle indicates that the activity may in some cases be effective.
5.1. Effects on Physical Health
The effects of physical activity and exercise are both acute (during and immediately after) and long-lasting. Effects remaining after a long period of regular physical activity have far-reaching consequences for health and are described below. For example, some muscle enzymes’ activity can be quickly increased by physical exercise/training but just as quickly be lost when idle [118]. Other changes remain for months or years even if training ends—for instance, increased number and size of muscle fibers and blood vessels [49,119,120]. Good health, therefore, requires physical activity to be performed with both progression and continuity. Most of the conducted physical exercise/training is a combination of both aerobic and muscle strengthening exercise, and it can be difficult to distinguish between their health effects (Table 2).
To describe ill-health, indicators of life expectancy, disease incidence (number), and prevalence (how often) are used [121]. In describing the relationship between physical activity and falling ill with certain diseases, the dose–response relationship, the effect size (the risk reduction that is shown in studies), and the recommended type and dose of physical activity are considered [122]. Table 3 shows the relative effects of regular physical activity ton the risk of various diseases (US Department of Human Services, 2009). The greatest health gains are for people who move from completely sedentary to moderately active lifestyles, with health effects seen before measurable improvements in physical performance. Previously, most scientific studies collected data only on aerobic physical activity. However, resistance exercise also shows promising health (mental and physical) and disease-prevention effects [123,124,125,126,127].
Table 3.
Disease prevention effects of regular physical activity.
Aerobic physical activity has been shown to benefit weight maintenance after prior weight loss, reduce the risk of metabolic syndrome, normalize blood lipids, and help with cancer/cancer-related side effects (Table 2 and Table 3), while effects on chronic pain are not as clear [29].
Muscle-strengthening physical activity has, in contrast to aerobic exercise, been shown to reduce muscle atrophy [128], risk of falling [75], and osteoporosis [74] in the elderly. Among the elderly, both men and women adapt positively to strength training [129]. Strength training also prevents obesity [130], enhances cognitive performance if done alongside aerobic exercise [131], counteracts the development of neurodegenerative diseases [132,133,134], reduces the risk of metabolic syndrome [135], counteracts cancer/cancer-related side effects [135,136], reduces pain and disability in joint diseases [137], and enhances bone density [137,138]. The risk of falling increases markedly with age and is partly a result of reduced muscle mass, and reduced coordination and balance [76,139,140]. A strong correlation between physical performance, reduced risk of falls, and enhanced quality of life is therefore, not surprisingly, found in older people [141]. Deterioration in muscle strength, but not muscle mass, increases the risk of premature death [142] but can be counteracted by exercise as a dose–response relationship describes the strength improvement in the elderly [122,143]. Recommendations state high-intensity strength training (6–8 repetitions at 80% of 1-repetition maximum) as most effective [144]. Muscle strengthening physical activity for better health is recommended as a complement to aerobic physical activity [29]. Amongst the elderly, vibration training can be an alternative to increase strength [145].
5.2. Effects on Mental Health
Mental illness is a global problem affecting millions of people worldwide [147]. Headache, stress, insomnia, fatigue, and anxiety are all measures of mental ill health. The term “ill health” constitutes a collection of several mental health problems and symptoms with various levels of seriousness. Studies have compared expected health benefits from regular physical activity for improvement of mental health with other treatments, for example, medication. Most recent studies show that physical activity and exercise used as a primary, or secondary, processing method have significant positive effects in preventing or alleviating depressive symptoms [31,148,149,150,151] and have an antidepressant effect in people with neurological diseases [152]. Training and exercise improve the quality of life and coping with stress and strengthen self-esteem and social skills [69,153]. Training and exercise also lessen anxiety in people who are diagnosed with an anxiety- or stress-related disease [68], improve vocabulary learning [154], memory [155,156], and creative thinking [157].
The same Swedish data as used in Figure 1 show that between the years 2004–2007 and 2012–2015 anxiety, worry, and insomnia decreased but were not obviously correlated to the slightly increased level of physical activity in the population during the same period. Thus, in a multifactorial context, the importance of physical exercise alone cannot be demonstrated in this dataset.
Some of the suggested physiological explanations for improved mental health with physical activity and exercise are greater perfusion and increased brain volume [107,158], increased volume of the hippocampus [106], and the anti-inflammatory effects of physical activity, reducing brain inflammation in neurological diseases [159]. Physical exercise may also mediate resilience to stress-induced depression via skeletal muscle peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α), enhancing kynurenine conversion to kynurenine acid, which in turn protects the brain and reduces the risk for stress-induced depression [153]. Further, increased release of growth factors, endorphins, and signaling molecules are other exercise-induced enhancers of mental health [69].
6. How Sport Affects Health
Sport’s main purposes are to promote physical activity and improve motor skills for health and performance and psychosocial development [56]. Participants also gain a chance to be part of a community, develop new social circles, and create social norms and attitudes. In healthy individuals, and patients with mental illness, sport participation has been shown to provide individuals with a sense of meaning, identity, and belonging [160,161]. Whether the sport movement exists or not, training and competition including physical activity will happen. Sport’s added values, in addition to the health benefits of physical activity, are therefore of interest. Some argue that it is doubtful, or at least not confirmed, that health development can come from sport, while others believe that healthy sport is something other than health, reviewed in depth by Coakley [162]. In a sporting context, health is defined as subjective (e.g., one feels good), biological (e.g., not being sick), functional (e.g., to perform), and social (e.g., to collaborate) [163]. Holt [56] argued that the environment for positive development in young people is distinctly different from an environment for performance, as the latter is based on being measured and assessed. That said, certain skills (goal setting, leadership, etc.) can be transferred from a sporting environment to other areas of life. The best way to transfer these abilities is, at the moment, unclear.
Having the goal to win at all costs can be detrimental to health. This is especially true for children and adolescents, as early engagement in elite sports increases the risk of injury, promotes one-dimensional functional development, leads to overtraining, creates distorted social norms, risks psychosocial disorders, and has the risk of physical and psychological abuse [15,164]. Of great importance, therefore, is sport’s goal of healthy performance development, starting at an early age. For older people, a strong motivating factor to conduct physical activity is sports club membership [165]. One can summarize these findings by stating sport’s utility at the transition between different stages of the life; from youth to adulthood and from adulthood to old age. There, sports can be a resource for good physical and mental health [166].
Today, a higher proportion of the population, compared to 50 years ago, is engaged in organized sports, and to a lesser extent performs spontaneous sports (Figure 3), something that Engström showed in 2004 [17] and is confirmed by data from The Swedish Sports Confederation (www.rf.se). Of the surveyed individuals in 2001, 50%–60% of children and young people said they were active in a sports club. The trend has continued showing similar progression to 2011, with up to 70% of school students playing sports in a club. Furthermore, the study shows that those active in sport clubs also spontaneously do more sports [167]. Similar data from the years 2007–2018, compiled from open sources at The Swedish Sports Confederation, confirm the trend with an even higher share of youths participating in organized sports, compared to 1968 and 2001 (Figure 4).
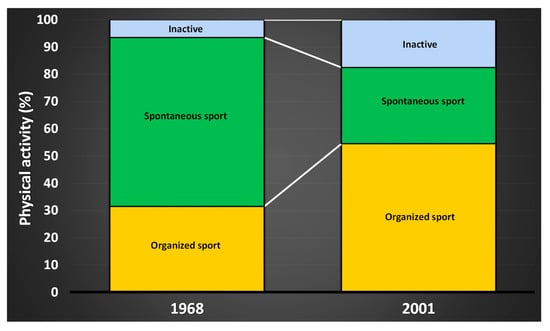
Figure 3.
Spontaneous sport has decreased over the last decades, to the advantage of organized sport. Data compiled from Engström, 2004, The Swedish Research Council for Sport Science.
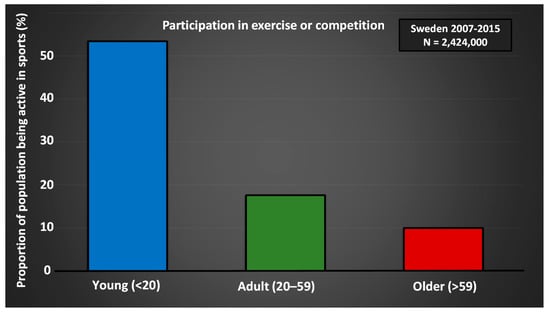
Figure 4.
Data compiled from open sources report Sport Statistics (Idrotten i siffror) at The Swedish Sports Confederation for the year 2011 (www.rf.se).
Taking part in sports can be an important motivator for physical activity for older people [165,166]. With aging, both participation in sports (Figure 4) and physical activity in everyday life [168] decreases. At the same time, the number of people who are physically active both in leisure and in organized sports increases (The Public Health Agency of Sweden 2017; www.folkhalsomyndigheten.se). Consequently, among elderly people, a greater proportion of the physical activity occurs within the context of sport [8,28]. Together, research shows that organized sports, in clubs or companies, are more important for people’s overall physical activity than ever before. Groups that are usually less physically active can be motivated through sport—for example, elderly men in sport supporters’ clubs [169], people in rural areas [170], migrants [171], and people with alternative physical and mental functions [172]. No matter how you get your sporting interest, it is important to establish a physical foundation at an early age to live in good health when you get older (Figure 5). As seen in Figure 5, a greater sport habitus at age 15 results in higher physical activity at 53 years of age. Early training and exposure to various forms of sports are therefore of great importance. Participation creates an identity, setting the stage for a high degree of physical activity later in life [173].
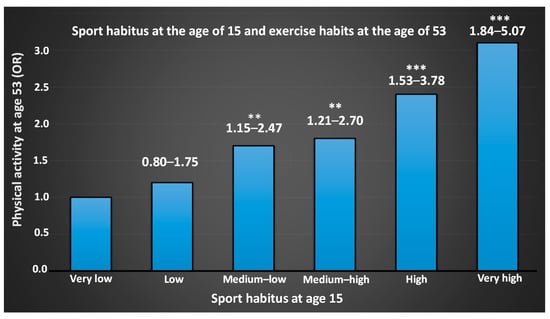
Figure 5.
Odds ratio (OR) of physical activity at age 53 in relation to Sport habitus at age 15. Sport habitus (“the total physical capital"), including cultural capital, athletic diversity, and grades in physical education and health are, according to Engström [173], the factors most important for being physically active in later life. For a further discussion on sport habitus, the readers are referred to Engström, 2008 [173]. Numbers above bar show the 95% confidence interval. ** = significant difference from “Very low”, p < 0.01. *** = p < 0.001.
7. Sport’s Effects on the Health of Children and Young People
The effects of participation in organized sports for children and young people are directly linked to physical activity, with long term secondary effects; an active lifestyle at a young age fosters a more active lifestyle as an adult. As many diseases that are positively affected by physical activity/exercise appear later in life, continued participation in sport as an adult will reduce morbidity and mortality.
It must be emphasized that good physical and mental health of children and young people participating in sport requires knowledge and organization based on everyone’s participation. Early specialization counteracts, in all regards, both health and performance development [174,175].
7.1. Positive Aspects
According to several reviews, there is a correlation between high daily physical activity in children and a low risk for obesity, improved development of motor and cognitive skills, as well as a stronger skeleton [176,177]. Positive effects on lipidemia, blood pressure, oxygen consumption, body composition, metabolic syndrome, bone density and depression, increased muscle strength, and reduced damage to the skeleton and muscles are also described [178,179]. If many aspects are merged in a multidimensional analysis [8,173], the factors important for future good health are shown to be training in sports, broad exposure to different sports, high school grades, cultural capital, and that one takes part in sport throughout childhood (Table 4).
Table 4.
Compiled health profiles for men and women at the age of 20 years, depending on participation in organized sports at the age of 5, 7, 8, 10, 14, and 17 years.
Psychological benefits of sports participation of young people were compiled by Eime et al. [1], where the conclusion was that sporting children have better self-esteem, less depression, and better overall psychosocial health. One problem with most of these studies, though, is that they are cross-sectional studies, which means that no cause–effect relationship can be determined. As there is a bias for participating children towards coming from socially secure environments, the results may be somewhat skewed.
7.2. Negative Aspects
As Table 4 and Table 5 show, there are both positive and negative aspects of sports. Within children’s and youth sports, early specialization to a specific sport is a common phenomenon [175]. There is no scientific evidence that early specialization would have positive impact, neither for health nor for performance later in life [175]. No model or method including performance at a young age can predict elite performance as an adult. By contrast, specialization and competitiveness can lead to injury, overtraining, increased psychological stress, and reduced training motivation, just to mention a few amongst many negative aspects [174,175]. Another important aspect is that those who are excluded from sports feel mentally worse [8]. As there is a relationship between depressive episodes in adolescence, and depression as adults [116], early exclusion has far-reaching consequences. Therefore, sports for children and young people have future health benefits by reducing the risk of developing depression and depressive symptoms, as well as improved wellbeing throughout life.
Table 5.
Positive and negative aspects with sport (at young age).
While some degree of sport specialization is necessary to develop elite-level athletes, research shows clear adverse health effects of early specialization and talent selection [180]. More children born during the fall and winter (September–December) are excluded [181], and as a group, they are less physically active than spring (January–April) children, both in sports and leisure (Figure 6). In most sports and in most countries, there is a skewed distribution of participants when sorted by birth-date, and there are more spring children than fall children among those who are involved in sport [182,183,184,185,186]. Because a large part of the physical activity takes place in an organized form, this leads to lower levels of physical activity for late-born persons (Malm, Jakobsson, and Julin, unpublished data). Early orientation and training in physical activity and exercise will determine how active you are later in life. Greater attention must be given to stimulating as many children and young people as possible to participate in sport as long as possible, both in school and on their leisure time. According to statistics from the Swedish Sports Confederation in 2016, this relative-age effect persists throughout life, despite more starting than ending with sport each year [18].
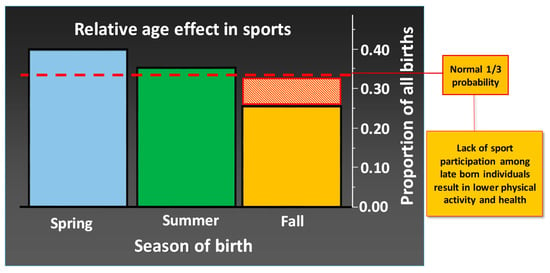
Figure 6.
The figure shows the distribution of 7597 children aged 10 years and younger who in 2014 were registered as active in one particular, individual sport in Sweden (data compiled from the Swedish Sport Confederation, www.rf.se). Spring, Summer, and Fall represent January–April, May–August, and September–December, respectively.
When summarize, the positive and negative aspects of sport at a young age can be divided into three categories: (1) Personal identification, (2) social competence, and (3) physiological capacity, briefly summarized in Table 5. A comprehensive analysis of what is now popularly known as “physical literacy” has recently been published [187].
7.3. Relevance of Sports
Sports can make children and young people develop both physically and mentally and contribute with health benefits if planned and executed exercise/training considers the person’s own capacities, social situation, and biological as well as psychological maturation. In children and adolescents, it is especially important to prevent sports-related injuries and health problems, as a number of these problems are likely to remain long into adulthood, sometimes for life. Comprehensive training is recommended, which does not necessarily mean that you have to participate in various sports. What is required is diverse training within every sport and club. Research shows that participation in various sports simultaneously during childhood and adolescence is most favorable for healthy and lifelong participation [8,173,188,189].
8. Sport’s Effects on the Health of Adults and the Elderly
Adults who stop participating in sports reduce their physical activity and have health risks equal to people who have neither done sports nor been physical [190,191]. Lack of adherence to exercise programs is a significant hindrance in achieving health goals and general physical activity recommendations in adults and the elderly [192]. While several socioeconomic factors are related to exercise adherence, it is imperative that trainers and health care providers are informed about factors that can be modulated, such as intervention intensity (not to high), duration (not too long), and supervision, important for higher adherence, addressed more in depth by Rivera-Torres, Fahey and Rivera [192].
Healthy aging is dependent on many factors, such as the absence of disease, good physical and mental health, and social commitment (especially through team sports or group activities) [193]. Increased morbidity with age may be partly linked to decreased physical activity. Thus, remaining or becoming active later in life is strongly associated with healthy aging [194]. With increased age, there is less involvement in training and competition (Figure 4), and only 20% of adults in Sweden are active, at least to some extent, in sports clubs, and the largest proportion of adults who exercise do it on their own. The following sections describes effects beyond what is already provided for children and youths.
8.1. Positive Aspects
Participation in sports, with or without competition, promotes healthy behavior and a better quality of life [166]. Exclusion from sports at a young age appears to have long-term consequences, as the previously described relative age effect (Figure 6) remains even for master athletes (Malm, Jakobsson, and Julin, unpublished data). Because master athletes show better health than their peers [95], actions should be taken to include adults and elderly individuals who earlier in life were excluded from, or never started with sport [195]. As we age, physical activity at a health-enhancing intensity is not enough to maintain all functions. Higher intensity is required, best comprising competition-oriented training [196,197]. One should not assume that high-intensity exercise cannot be initiated by the elderly [198]. Competitive sports, or training like a competitive athlete as an adult, can be one important factor to counter the loss of physical ability with aging [199]. In this context, golf can be one example of a safe form of exercise with high adherence for older adults and the elderly, resulting in increased aerobic performance, metabolic function, and trunk strength [200,201].
8.2. Negative Aspects
Increased morbidity (e.g., cardiovascular disease) with aging is seen also among older athletes [202] and is associated with the same risk factors as in the general population [203]. An increased risk of cardiovascular disease among adults (master) compared to other populations has been found [204]. Unfortunately, the designs and interpretations of these studies have been criticized, and the incidence of cardiac arrest in older athletes is unclear [205]. In this context, the difference between competitive sports aiming to optimize performance and recreational sports has to be taken into account, where the former is more likely to induce negative effects due to high training loads and/or impacts during training and games. Although high-intensity training even for older athletes is positive for aerobic performance, it does not prevent the loss of motor units [206].
Quality of life is higher in sporting adults compared to those who do not play sports, but so is the risk of injury. When hit by injury, adults and young alike may suffer from psychological disorders such as depression [207], but with a longer recovery time in older individuals [208]. As with young athletes, secession of training at age 50 years and above reduces blood flow in the brain, including the hippocampus, possibly related to long-term decline in mental capacity [209].
8.3. Relevance of Sport
As for children and young people, many positive health aspects come through sport also for adults and the elderly [210]. Sport builds bridges between generations, a potential but not elucidated drive for adults’ motivation for physical activity. The percentage of adults participating in competitive sports has increased in Sweden since 2010, from about 20 percent to 30 percent of all of those who are physically active [18], a trend that most likely provides better health for the group in the 30–40 age group and generations to come.
9. Recommendations for Healthy Sport
- 1. Plan exercise, rest, and social life. For health-promoting and healthy-aging physical activity, refer to general guidelines summarized in this paper: Aerobic exercise three times a week, muscle-strengthening exercise 2–3 times a week.
- 2. Set long-term goals.
- 3. Adopt a holistic performance development including physiological, medical, mental, and psychosocial aspects.
- 4. Monitor physiological health over time:
- ○
- a. Exercise load (time, intensity, volume);
- ○
- b. Recovery (sleep, resting heart rate, appetite, estimated fatigue, etc.);
- ○
- c. Sickness (when–where–how, type of infections, how long one is ill, etc.);
- ○
- d. Repeat type- and age-specific physical tests with relevant evaluation and feedback;
- ○
- e. Frequency of injuries and causes.
- 5. Monitor mental health over time:
- ○
- a. Motivation for training, competition, and socializing;
- ○
- b. Personal perception of stress, anxiety, depression, alienation, and self-belief;
- ○
- c. Repeat type- and age-specific psychological tests with relevant evaluation and feedback.
- 6. Register and interpret signs of overtraining, such as reduced performance over time, while maintaining or increasing exercise load.
Author Contributions
C.M. and A.J. conceived and designed the review. C.M., A.J., J.J. and interpreted the data and drafted the manuscript. J.J. edited the manuscript, tables, and figures. All authors approved the final version.
Funding
This work was supported by the Swedish Sports Confederation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef] [PubMed]
- Nowak, P.F. Amateur Sports of the Elderly: A Chance for Health and a Higher Quality of Life. Adv. Aging Res. 2014, 3, 222–229. [Google Scholar] [CrossRef]
- Fraser-Thomas, J.; Strachan, L. Personal developemnt and performance? In Health and Elite Sport: Is High Performance Sport a Healthy Pursuit? Baker, J., Safai, P., Fraser-Thomas, J., Eds.; Routledge Research in Sport, Culture and Society; Taylor & Francis Group: Londond, UK, 2015. [Google Scholar]
- Lopez Villalba, F.J.; Rodriguez Garcia, P.L.; Garcia Canto, E.; Perez Soto, J.J. Relationship between sport and physical activity and alcohol consumption among adolescents students in Murcia (Spain). Arch. Argent. Pediatr. 2016, 114, 101–106. [Google Scholar] [CrossRef]
- Elofsson, S.; Blomdahl, U.; Åkesson, M.; Lengheden, L. Dricker ungdomar i idrotsförening mindre alkohol än de som inte är med i en idrotsförening? Stockholm stads idrottsförvalnintg: Stockholm, Sweden, 2014. [Google Scholar]
- Kjonniksen, L.; Anderssen, N.; Wold, B. Organized youth sport as a predictor of physical activity in adulthood. Scand. J. Med. Sci. Sports 2009, 19, 646–654. [Google Scholar] [CrossRef]
- Khan, K.M.; Thompson, A.M.; Blair, S.N.; Sallis, J.F.; Powell, K.E.; Bull, F.C.; Bauman, A.E. Sport and exercise as contributors to the health of nations. Lancet 2012, 380, 59–64. [Google Scholar] [CrossRef]
- Howie, E.K.; McVeigh, J.A.; Smith, A.J.; Straker, L.M. Organized Sport Trajectories from Childhood to Adolescence and Health Associations. Med. Sci. Sports Exerc. 2016, 48, 1331–1339. [Google Scholar] [CrossRef]
- Rice, S.M.; Purcell, R.; De Silva, S.; Mawren, D.; McGorry, P.D.; Parker, A.G. The Mental Health of Elite Athletes: A Narrative Systematic Review. Sports Med. 2016, 46, 1333–1353. [Google Scholar] [CrossRef]
- Schwellnus, M.; Soligard, T.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.J.; Gleeson, M.; Hagglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 2) International Olympic Committee consensus statement on load in sport and risk of illness. Br. J. Sports Med. 2016, 50, 1043–1052. [Google Scholar] [CrossRef]
- Soligard, T.; Schwellnus, M.; Alonso, J.M.; Bahr, R.; Clarsen, B.; Dijkstra, H.P.; Gabbett, T.; Gleeson, M.; Hagglund, M.; Hutchinson, M.R.; et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br. J. Sports Med. 2016, 50, 1030–1041. [Google Scholar] [CrossRef] [PubMed]
- Joy, E.; Kussman, A.; Nattiv, A. 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. Br. J. Sports Med. 2016, 50, 154–162. [Google Scholar] [CrossRef]
- Brenner, J.S. Overuse injuries, overtraining, and burnout in child and adolescent athletes. Pediatrics 2007, 119, 1242–1245. [Google Scholar] [CrossRef]
- Clark, A.; Mach, N. Exercise-induced stress behavior, gut-microbiota-brain axis and diet: A systematic review for athletes. J. Int. Soc. Sports Nutr. 2016, 13, 43. [Google Scholar] [CrossRef]
- Lang, M.; Hartill, M. Safeguarding, Child Protection and Abuse in Sport: International Perspectives in Research, Policy and Practice; Taylor & Francis: Abingdon-on-Thames, UK, 2014. [Google Scholar]
- Pontzer, H.; Durazo-Arvizu, R.; Dugas, L.R.; Plange-Rhule, J.; Bovet, P.; Forrester, T.E.; Lambert, E.V.; Cooper, R.S.; Schoeller, D.A.; Luke, A. Constrained Total Energy Expenditure and Metabolic Adaptation to Physical Activity in Adult Humans. Curr. Biol. 2016, 26, 410–417. [Google Scholar] [CrossRef]
- Engström, L.-M. Barns och ungdomars idrottsvanor i förändring. Svensk Idrottsforskning: Organ för Centrum för Idrottsforskning 2004, 4, 10–15. [Google Scholar]
- The Swedish Sports Confederation. Sport statisitcs [Idrotten i siffror}; Confederation, T.S.S., Ed.; The Swedish Sports Confederation: Stockholm, Sweden, 2015. [Google Scholar]
- SCB. Levnadsförhållanden: Fritid 2006-2007 [Living Conditions: Recreation 2006-2007]; 118; Statistics Sweden: Stockholm, Sweden, 2009.
- Swedish National Institute of Publich Health Physical Activity in the Prevention and Treatment of Disease (FYSS); Swedish National Institute of Publich Health, and Swedish Professional Associations for Physical Activity: Järna, Sweden, 2017.
- WHO. Physical activity. Available online: http://www.who.int/topics/physical_activity/en/ (accessed on 19 November 2017).
- US Department of Human Services. Physical Activity Guidelines Advisory Committee report, 2008. To the Secretary of Health and Human Services. Part A: Executive Summary; 0029-6643; US Department of Human Services: Washington, DC, USA, 2009; pp. 114–120.
- Publich Health Agency of Sweden. Vad är Fysisk Aktivitet? [What Is Physical Activity?]; Publich Health Agency of Sweden: Solna, Sweden, 2016; Volume 2016.
- Swedish Research Council for Sport Science (CIF). Sport Relevance [Idrottsrelevans]; Swedish Research Council for Sport Science (CIF): Stockholm, Sweden, 2016; Volume 2016.
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively measured sedentary time, physical activity, and metabolic risk: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef]
- Matthews, C.E.; George, S.M.; Moore, S.C.; Bowles, H.R.; Blair, A.; Park, Y.; Troiano, R.P.; Hollenbeck, A.; Schatzkin, A. Amount of time spent in sedentary behaviors and cause-specific mortality in US adults. Am. J. Clin. Nutr. 2012, 95, 437–445. [Google Scholar] [CrossRef]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Ratzlaff, C.R.; Doerfling, P.; Steininger, G.; Koehoorn, M.; Cibere, J.; Liang, M.; Wilson, D.R.; Esdaile, J.; Kopec, J. Lifetime trajectory of physical activity according to energy expenditure and joint force. Arthritis Care Res. 2010, 62, 1452–1459. [Google Scholar] [CrossRef] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, CD011279. [Google Scholar] [CrossRef]
- Liberman, K.; Forti, L.N.; Beyer, I.; Bautmans, I. The effects of exercise on muscle strength, body composition, physical functioning and the inflammatory profile of older adults: A systematic review. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 30–53. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr. Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Wilson, J.M.; Lowery, R.P.; Krieger, J.W. Muscular adaptations in low-versus high-load resistance training: A meta-analysis. Eur. J. Sport Sci. 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations Between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals Across the Lifespan: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef] [PubMed]
- Timperio, A.; Salmon, J.; Rosenberg, M.; Bull, F.C. Do logbooks influence recall of physical activity in validation studies? Med. Sci. Sports Exerc. 2004, 36, 1181–1186. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- McEwen, B.S. Stressed or stressed out: What is the difference? J. Psychiatry Neurosci. Jpn. 2005, 30, 315–318. [Google Scholar]
- Selye, H. Stress and the general adaptation syndrome. Br. Med. J. 1950, 1, 1383–1392. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef] [PubMed]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Ronnestad, B.R.; Ellefsen, S.; Nygaard, H.; Zacharoff, E.E.; Vikmoen, O.; Hansen, J.; Hallen, J. Effects of 12 weeks of block periodization on performance and performance indices in well-trained cyclists. Scand. J. Med. Sci. Sports 2014, 24, 327–335. [Google Scholar] [CrossRef]
- Ahtiainen, J.P.; Walker, S.; Peltonen, H.; Holviala, J.; Sillanpaa, E.; Karavirta, L.; Sallinen, J.; Mikkola, J.; Valkeinen, H.; Mero, A.; et al. Heterogeneity in resistance training-induced muscle strength and mass responses in men and women of different ages. Age 2016, 38, 10. [Google Scholar] [CrossRef]
- Davidsen, P.K.; Gallagher, I.J.; Hartman, J.W.; Tarnopolsky, M.A.; Dela, F.; Helge, J.W.; Timmons, J.A.; Phillips, S.M. High responders to resistance exercise training demonstrate differential regulation of skeletal muscle microRNA expression. J. Appl. Physiol. (Bethesda Md. 1985) 2011, 110, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Timmons, J.A. Variability in training-induced skeletal muscle adaptation. J. Appl. Physiol. (Bethesda Md. 1985) 2011, 110, 846–853. [Google Scholar] [CrossRef] [PubMed]
- Vollaard, N.B.; Constantin-Teodosiu, D.; Fredriksson, K.; Rooyackers, O.; Jansson, E.; Greenhaff, P.L.; Timmons, J.A.; Sundberg, C.J. Systematic analysis of adaptations in aerobic capacity and submaximal energy metabolism provides a unique insight into determinants of human aerobic performance. J. Appl. Physiol. (Bethesda Md. 1985) 2009, 106, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Venezia, A.C.; Roth, S.M. Recent Research in the Genetics of Exercise Training Adaptation. Med. Sport Sci. 2016, 61, 29–40. [Google Scholar] [CrossRef]
- Porter, C.; Reidy, P.T.; Bhattarai, N.; Sidossis, L.S.; Rasmussen, B.B. Resistance Exercise Training Alters Mitochondrial Function in Human Skeletal Muscle. Med. Sci. Sports Exerc. 2015, 47, 1922–1931. [Google Scholar] [CrossRef]
- Verdijk, L.B.; Snijders, T.; Holloway, T.M.; J, V.A.N.K.; LJ, V.A.N.L. Resistance Training Increases Skeletal Muscle Capillarization in Healthy Older Men. Med. Sci. Sports Exerc. 2016, 48, 2157–2164. [Google Scholar] [CrossRef]
- Mujika, I.; Padilla, S. Detraining: Loss of training-induced physiological and performance adaptations. Part I: Short term insufficient training stimulus. Sports Med. 2000, 30, 79–87. [Google Scholar] [CrossRef]
- Gundersen, K. Muscle memory and a new cellular model for muscle atrophy and hypertrophy. J. Exp. Biol. 2016, 219, 235–242. [Google Scholar] [CrossRef]
- Leonard, W.R. Size counts: Evolutionary perspectives on physical activity and body size from early hominids to modern humans. J. Phys. Act. Health 2010, 7 (Suppl. 3), S284–S298. [Google Scholar] [CrossRef]
- Leonard, W.R.; Robertson, M.L. Nutritional requirements and human evolution: A bioenergetics model. Am. J. Hum. Biol. 1992, 4, 179–195. [Google Scholar] [CrossRef]
- Cordain, L.; Gotshall, R.W.; Eaton, S.B.; Eaton, S.B., 3rd. Physical activity, energy expenditure and fitness: An evolutionary perspective. Int. J. Sports Med. 1998, 19, 328–335. [Google Scholar] [CrossRef]
- SCB. Levnadsförhållanden: Fritid 1976-2002 [Levnadsförhållanden: Fritid 2006-2007 [Living conditions: Recreation 1976-2002]]; 103; Statistics Sweden: Stockholm, Sweden, 2004.
- Church, T.S.; Thomas, D.M.; Tudor-Locke, C.; Katzmarzyk, P.T.; Earnest, C.P.; Rodarte, R.Q.; Martin, C.K.; Blair, S.N.; Bouchard, C. Trends over 5 decades in U.S. occupation-related physical activity and their associations with obesity. PLoS ONE 2011, 6, e19657. [Google Scholar] [CrossRef]
- The Public Health Agency of Sweden. Children’s and Youth’s Pattern of Movement; The Public Health Agency of Sweden: Solna, Sweden 2019.
- Holt, N.L.; Neely, K.C.; Slater, L.G.; Camire, M.; Cote, J.; Fraser-Thomas, J.; MacDonald, D.; Strachan, L.; Tamminen, K.A. A grounded theory of positive youth development through sport based on results from a qualitative meta-study. Int. Rev. Sport Exerc. Psychol. 2017, 10, 1–49. [Google Scholar] [CrossRef]
- Andersen, L.B.; Mota, J.; Di Pietro, L. Update on the global pandemic of physical inactivity. Lancet 2016, 388, 1255–1256. [Google Scholar] [CrossRef]
- Das, P.; Horton, R. Physical activity-time to take it seriously and regularly. Lancet 2016, 388, 1254–1255. [Google Scholar] [CrossRef]
- Kujala, U.M.; Kaprio, J.; Sarna, S.; Koskenvuo, M. Relationship of leisure-time physical activity and mortality: The Finnish twin cohort. JAMA 1998, 279, 440–444. [Google Scholar] [CrossRef]
- Hills, A.P.; Street, S.J.; Byrne, N.M. Physical Activity and Health: “What is Old is New Again”. Adv. Food Nutr. Res. 2015, 75, 77–95. [Google Scholar] [CrossRef] [PubMed]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; Berrington de Gonzalez, A.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Internal Med. 2015, 175, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Scientific Report; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- Blair, S.N. Physical inactivity and cardiovascular disease risk in women. Med. Sci. Sports Exerc. 1996, 28, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef]
- Wegner, M.; Helmich, I.; Machado, S.; Nardi, A.E.; Arias-Carrion, O.; Budde, H. Effects of exercise on anxiety and depression disorders: Review of meta- analyses and neurobiological mechanisms. CNS Neurol. Disorders Drug Targets 2014, 13, 1002–1014. [Google Scholar] [CrossRef]
- Bennett, K.; Manassis, K.; Duda, S.; Bagnell, A.; Bernstein, G.A.; Garland, E.J.; Miller, L.D.; Newton, A.; Thabane, L.; Wilansky, P. Preventing Child and Adolescent Anxiety Disorders: Overview of Systematic Reviews. Depress Anxiety 2015, 32, 909–918. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Vancampfort, D.; Rosenbaum, S.; Firth, J.; Cosco, T.; Veronese, N.; Salum, G.A.; Schuch, F.B. An examination of the anxiolytic effects of exercise for people with anxiety and stress-related disorders: A meta-analysis. Psychiatry Res. 2017, 249, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Knochel, C.; Oertel-Knochel, V.; O’Dwyer, L.; Prvulovic, D.; Alves, G.; Kollmann, B.; Hampel, H. Cognitive and behavioural effects of physical exercise in psychiatric patients. Progr. Neurobiol. 2012, 96, 46–68. [Google Scholar] [CrossRef] [PubMed]
- Craig, D.M.; Ashcroft, S.P.; Belew, M.Y.; Stocks, B.; Currell, K.; Baar, K.; Philp, A. Utilizing small nutrient compounds as enhancers of exercise-induced mitochondrial biogenesis. Front. Physiol. 2015, 6. [Google Scholar] [CrossRef]
- Wilson, M.G.; Ellison, G.M.; Cable, N.T. Basic science behind the cardiovascular benefits of exercise. Heart 2015, 101, 758–765. [Google Scholar] [CrossRef]
- Hellsten, Y.; Nyberg, M. Cardiovascular Adaptations to Exercise Training. Compr. Physiol. 2015, 6, 1–32. [Google Scholar] [CrossRef]
- Wilson, J.M.; Loenneke, J.P.; Jo, E.; Wilson, G.J.; Zourdos, M.C.; Kim, J.S. The effects of endurance, strength, and power training on muscle fiber type shifting. J. Strength Cond. Res. 2012, 26, 1724–1729. [Google Scholar] [CrossRef]
- Cadore, E.L.; Pinto, R.S.; Bottaro, M.; Izquierdo, M. Strength and endurance training prescription in healthy and frail elderly. Aging Dis. 2014, 5, 183–195. [Google Scholar] [CrossRef]
- Tofthagen, C.; Visovsky, C.; Berry, D.L. Strength and balance training for adults with peripheral neuropathy and high risk of fall: Current evidence and implications for future research. Oncol. Nurs. Forum. 2012, 39, E416–E424. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.I.; An, D.H. Effects of a Fall Prevention Exercise Program on Muscle Strength and Balance of the Old-old Elderly. J. Phys. Ther. Sci. 2014, 26, 1771–1774. [Google Scholar] [CrossRef] [PubMed]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.J.; Smart, N.A. Effect of exercise training on endothelial function in heart failure patients: A systematic review meta-analysis. Int. J. Cardiol. 2017, 231, 234–243. [Google Scholar] [CrossRef]
- Nielsen, J.; Gejl, K.D.; Hey-Mogensen, M.; Holmberg, H.C.; Suetta, C.; Krustrup, P.; Elemans, C.P.H.; Ortenblad, N. Plasticity in mitochondrial cristae density allows metabolic capacity modulation in human skeletal muscle. J. Physiol. 2017, 595, 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and skeletal muscle glucose uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef] [PubMed]
- Marson, E.C.; Delevatti, R.S.; Prado, A.K.; Netto, N.; Kruel, L.F. Effects of aerobic, resistance, and combined exercise training on insulin resistance markers in overweight or obese children and adolescents: A systematic review and meta-analysis. Prev. Med. 2016, 93, 211–218. [Google Scholar] [CrossRef]
- Way, K.L.; Hackett, D.A.; Baker, M.K.; Johnson, N.A. The Effect of Regular Exercise on Insulin Sensitivity in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Diabetes Metab. J. 2016, 40, 253–271. [Google Scholar] [CrossRef] [PubMed]
- Conn, V.S.; Koopman, R.J.; Ruppar, T.M.; Phillips, L.J.; Mehr, D.R.; Hafdahl, A.R. Insulin Sensitivity Following Exercise Interventions: Systematic Review and Meta-Analysis of Outcomes Among Healthy Adults. J. Prim Care Community Health 2014, 5, 211–222. [Google Scholar] [CrossRef]
- Schuch, F.B.; Deslandes, A.C.; Stubbs, B.; Gosmann, N.P.; Silva, C.T.; Fleck, M.P. Neurobiological effects of exercise on major depressive disorder: A systematic review. Neurosci. Biobehav. Rev. 2016, 61, 1–11. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Sui, X.; Rosenbaum, S.; Firth, J.; Richards, J.; Ward, P.B.; Stubbs, B. Are lower levels of cardiorespiratory fitness associated with incident depression? A systematic review of prospective cohort studies. Prev. Med. 2016, 93, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Zahl, T.; Steinsbekk, S.; Wichstrom, L. Physical Activity, Sedentary Behavior, and Symptoms of Major Depression in Middle Childhood. Pediatrics 2017, 139. [Google Scholar] [CrossRef]
- Colaianni, G.; Mongelli, T.; Colucci, S.; Cinti, S.; Grano, M. Crosstalk Between Muscle and Bone Via the Muscle-Myokine Irisin. Curr. Osteoporos. Rep. 2016, 14, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Giangregorio, L.M.; McGill, S.; Wark, J.D.; Laprade, J.; Heinonen, A.; Ashe, M.C.; MacIntyre, N.J.; Cheung, A.M.; Shipp, K.; Keller, H.; et al. Too Fit to Fracture: Outcomes of a Delphi consensus process on physical activity and exercise recommendations for adults with osteoporosis with or without vertebral fractures. Osteoporos. Int. 2015, 26, 891–910. [Google Scholar] [CrossRef] [PubMed]
- Papa, E.V.; Dong, X.; Hassan, M. Resistance training for activity limitations in older adults with skeletal muscle function deficits: a systematic review. Clin. Interv. Aging. 2017, 12, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Casonatto, J.; Goessler, K.F.; Cornelissen, V.A.; Cardoso, J.R.; Polito, M.D. The blood pressure-lowering effect of a single bout of resistance exercise: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2016, 23, 1700–1714. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, H.V.; Johnson, B.T.; Huedo-Medina, T.B.; Livingston, J.; Forsyth, K.C.; Kraemer, W.J.; Farinatti, P.T.V.; Pescatello, L.S. Dynamic Resistance Training as Stand-Alone Antihypertensive Lifestyle Therapy: A Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e003231. [Google Scholar] [CrossRef] [PubMed]
- Ettehad, D.; Emdin, C.A.; Kiran, A.; Anderson, S.G.; Callender, T.; Emberson, J.; Chalmers, J.; Rodgers, A.; Rahimi, K. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet 2016, 387, 957–967. [Google Scholar] [CrossRef]
- Chen, Y.C.; Tsai, J.C.; Liou, Y.M.; Chan, P. Effectiveness of endurance exercise training in patients with coronary artery disease: A meta-analysis of randomised controlled trials. Eur. J. Cardiovasc. Nurs. 2017, 16, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Bachi, A.L.; Rocha, G.A.; Sprandel, M.C.; Ramos, L.R.; Gravina, C.F.; Pithon-Curi, T.C.; Vaisberg, M.; Maranhao, R.C. Exercise Training Improves Plasma Lipid and Inflammatory Profiles and Increases Cholesterol Transfer to High-Density Lipoprotein in Elderly Women. J. Am. Geriatr. Soc. 2015, 63, 1247–1249. [Google Scholar] [CrossRef]
- Climstein, M.; Walsh, J.; Debeliso, M.; Heazlewood, T.; Sevene, T.; Adams, K. Cardiovascular risk profiles of world masters games participants. J. Sports Med. Phys. Fitness 2018, 58, 489–496. [Google Scholar]
- Anstey, K.J.; Ashby-Mitchell, K.; Peters, R. Updating the Evidence on the Association between Serum Cholesterol and Risk of Late-Life Dementia: Review and Meta-Analysis. J. Alzheimers Dis. 2017, 56, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Stoedefalke, K. Effects of exercise training on blood lipids and lipoproteins in children and adolescents. J. Sports Sci. Med. 2007, 6, 313–318. [Google Scholar] [PubMed]
- Hvid, L.G.; Strotmeyer, E.S.; Skjodt, M.; Magnussen, L.V.; Andersen, M.; Caserotti, P. Voluntary muscle activation improves with power training and is associated with changes in gait speed in mobility-limited older adults - A randomized controlled trial. Exp. Gerontol. 2016, 80, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.M.; Davis, N.; Sands, S.A.; Whittington, R.A.; Sun, L.S. Physical Activity and Cognitive Development: A Meta-Analysis. J. Neurosurg. Anesthesiol. 2016, 28, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Ludyga, S.; Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Puhse, U. Acute effects of moderate aerobic exercise on specific aspects of executive function in different age and fitness groups: A meta-analysis. Psychophysiology 2016, 53, 1611–1626. [Google Scholar] [CrossRef]
- Dinoff, A.; Herrmann, N.; Swardfager, W.; Liu, C.S.; Sherman, C.; Chan, S.; Lanctot, K.L. The Effect of Exercise Training on Resting Concentrations of Peripheral Brain-Derived Neurotrophic Factor (BDNF): A Meta-Analysis. PLoS ONE 2016, 11, e0163037. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S. Exercise and Sleep: A Systematic Review of Previous Meta-analyses And A Meta-analysis: 284 Board #121 June 1, 9: 30 AM - 11: 00 AM. Med. Sci. Sports Exerc. 2016, 48, 68–69. [Google Scholar] [CrossRef]
- Kandola, A.; Hendrikse, J.; Lucassen, P.J.; Yucel, M. Aerobic Exercise as a Tool to Improve Hippocampal Plasticity and Function in Humans: Practical Implications for Mental Health Treatment. Front. Hum. Neurosci. 2016, 10, 373. [Google Scholar] [CrossRef]
- Smith, G.E. Healthy Cognitive Aging and Dementia Prevention. Am. Psychol. 2016, 71, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, J. Neuroplasticity and Clinical Practice: Building Brain Power for Health. Front. Psychol. 2016, 7, 1118. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.M.; Nolan, Y.M. Neuroinflammation negatively affects adult hippocampal neurogenesis and cognition: Can exercise compensate? Neurosci. Biobehav. Rev. 2016, 61, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Boraxbekk, C.J.; Salami, A.; Wahlin, A.; Nyberg, L. Physical activity over a decade modifies age-related decline in perfusion, gray matter volume, and functional connectivity of the posterior default-mode network-A multimodal approach. Neuroimage 2016, 131, 133–141. [Google Scholar] [CrossRef]
- Dhabhar, F.S. Effects of stress on immune function: The good, the bad, and the beautiful. Immunol. Res. 2014, 58, 193–210. [Google Scholar] [CrossRef]
- Brodin, P.; Davis, M.M. Human immune system variation. Nat. Rev. Immunol. 2017, 17, 21–29. [Google Scholar] [CrossRef]
- Gjevestad, G.O.; Holven, K.B.; Ulven, S.M. Effects of Exercise on Gene Expression of Inflammatory Markers in Human Peripheral Blood Cells: A Systematic Review. Curr. Cardiovasc. Risk Rep. 2015, 9, 34. [Google Scholar] [CrossRef]
- Runhaar, J.; Bierma-Zeinstra, S.M. Should exercise therapy for chronic musculoskeletal conditions focus on the anti-inflammatory effects of exercise? Br. J. Sports Med. 2016. [Google Scholar] [CrossRef]
- Codella, R.; Luzi, L.; Inverardi, L.; Ricordi, C. The anti-inflammatory effects of exercise in the syndromic thread of diabetes and autoimmunity. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3709–3722. [Google Scholar] [PubMed]
- Mika, A.; Fleshner, M. Early-life exercise may promote lasting brain and metabolic health through gut bacterial metabolites. Immunol. Cell Biol. 2016, 94, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Kenfield, S.A.; Jimenez, A. Exercise-induced biochemical changes and their potential influence on cancer: A scientific review. Br. J. Sports Med. 2016. [Google Scholar] [CrossRef]
- Marchesi, J.R.; Adams, D.H.; Fava, F.; Hermes, G.D.; Hirschfield, G.M.; Hold, G.; Quraishi, M.N.; Kinross, J.; Smidt, H.; Tuohy, K.M.; et al. The gut microbiota and host health: A new clinical frontier. Gut 2016, 65, 330–339. [Google Scholar] [CrossRef]
- McKercher, C.; Sanderson, K.; Schmidt, M.D.; Otahal, P.; Patton, G.C.; Dwyer, T.; Venn, A.J. Physical activity patterns and risk of depression in young adulthood: A 20-year cohort study since childhood. Soc. Psych. Psych. Epid. 2014, 49, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- von Martels, J.Z.; Sadaghian Sadabad, M.; Bourgonje, A.R.; Blokzijl, T.; Dijkstra, G.; Faber, K.N.; Harmsen, H.J. The role of gut microbiota in health and disease: In vitro modeling of host-microbe interactions at the aerobe-anaerobe interphase of the human gut. Anaerobe 2017, 44, 3–12. [Google Scholar] [CrossRef]
- Bogdanis, G.C. Effects of physical activity and inactivity on muscle fatigue. Front. Physiol. 2012, 3, 142. [Google Scholar] [CrossRef]
- Eriksson, A. Strength Training and Anabolic Steroids: A Comparative Study of the Vastus Lateralis, a Thigh Muscle and the Trapezius, a Shoulder Muscle, of Strength-Trained Athletes. Ph.D. Thesis, Umeå University, Umeå, Sweden, 2006. [Google Scholar]
- Eriksson, A.; Kadi, F.; Malm, C.; Thornell, L.E. Skeletal muscle morphology in power-lifters with and without anabolic steroids. Histochem. Cell Biol. 2005, 124, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Alkema, L.; Black, R.E.; Boerma, J.T.; Collins, G.S.; Ezzati, M.; Grove, J.T.; Hogan, D.R.; Hogan, M.C.; Horton, R.; et al. Guidelines for Accurate and Transparent Health Estimates Reporting: The GATHER statement. Lancet 2016, 388, e19–e23. [Google Scholar] [CrossRef]
- Borde, R.; Hortobagyi, T.; Granacher, U. Dose-Response Relationships of Resistance Training in Healthy Old Adults: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 1693–1720. [Google Scholar] [CrossRef] [PubMed]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. The Effects of Resistance Exercise Training on Anxiety: A Meta-Analysis and Meta-Regression Analysis of Randomized Controlled Trials. Sports Med. 2017, 47, 2521–2532. [Google Scholar] [CrossRef]
- Keilani, M.; Hasenoehrl, T.; Baumann, L.; Ristl, R.; Schwarz, M.; Marhold, M.; Sedghi Komandj, T.; Crevenna, R. Effects of resistance exercise in prostate cancer patients: A meta-analysis. Support. Care Cancer 2017, 25, 2953–2968. [Google Scholar] [CrossRef]
- Yamamoto, S.; Hotta, K.; Ota, E.; Mori, R.; Matsunaga, A. Effects of resistance training on muscle strength, exercise capacity, and mobility in middle-aged and elderly patients with coronary artery disease: A meta-analysis. J. Cardiol. 2016, 68, 125–134. [Google Scholar] [CrossRef]
- Mammen, G.; Faulkner, G. Physical activity and the prevention of depression: A systematic review of prospective studies. Am. J. Prev. Med. 2013, 45, 649–657. [Google Scholar] [CrossRef]
- Csapo, R.; Alegre, L.M. Effects of resistance training with moderate vs heavy loads on muscle mass and strength in the elderly: A meta-analysis. Scand. J. Med. Sci. Sports 2016, 26, 995–1006. [Google Scholar] [CrossRef]
- Churchward-Venne, T.A.; Tieland, M.; Verdijk, L.B.; Leenders, M.; Dirks, M.L.; de Groot, L.C.; van Loon, L.J. There Are No Nonresponders to Resistance-Type Exercise Training in Older Men and Women. J. Am. Med. Dir. Assoc. 2015, 16, 400–411. [Google Scholar] [CrossRef]
- Garcia-Hermoso, A.; Ramirez-Velez, R.; Ramirez-Campillo, R.; Peterson, M.D.; Martinez-Vizcaino, V. Concurrent aerobic plus resistance exercise versus aerobic exercise alone to improve health outcomes in paediatric obesity: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 52, 161–166. [Google Scholar] [CrossRef]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.; van Berckel, B.N.; Scheltens, P.; Scherder, E.J.; van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef]
- Chung, C.L.; Thilarajah, S.; Tan, D. Effectiveness of resistance training on muscle strength and physical function in people with Parkinson’s disease: A systematic review and meta-analysis. Clin. Rehabil. 2016, 30, 11–23. [Google Scholar] [CrossRef]
- Kang, H.; Lu, J.; Xu, G. The effects of whole body vibration on muscle strength and functional mobility in persons with multiple sclerosis: A systematic review and meta-analysis. Mult. Scler. Relat. Disord. 2016, 7, 1–7. [Google Scholar] [CrossRef]
- Portugal, E.M.; Vasconcelos, P.G.; Souza, R.; Lattari, E.; Monteiro-Junior, R.S.; Machado, S.; Deslandes, A.C. Aging process, cognitive decline and Alzheimer’s disease: Can strength training modulate these responses? CNS & Neurol. Disorders Drug Targets 2015, 14, 1209–1213. [Google Scholar]
- Bacchi, E.; Negri, C.; Zanolin, M.E.; Milanese, C.; Faccioli, N.; Trombetta, M.; Zoppini, G.; Cevese, A.; Bonadonna, R.C.; Schena, F.; et al. Metabolic effects of aerobic training and resistance training in type 2 diabetic subjects: A randomized controlled trial (the RAED2 study). Diabetes Care 2012, 35, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Beckhove, P.; Owen, R.; Debus, J.; Wiskemann, J.; et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef] [PubMed]
- Ciolac, E.G.; Rodrigues-da-Silva, J.M. Resistance Training as a Tool for Preventing and Treating Musculoskeletal Disorders. Sports Med. 2016, 46, 1239–1248. [Google Scholar] [CrossRef]
- Castrogiovanni, P.; Trovato, F.M.; Szychlinska, M.A.; Nsir, H.; Imbesi, R.; Musumeci, G. The importance of physical activity in osteoporosis. From the molecular pathways to the clinical evidence. Histol. Histopathol. 2016, 31, 1183–1194. [Google Scholar] [CrossRef]
- Johansson, J.; Nordstrom, A.; Nordstrom, P. Greater Fall Risk in Elderly Women Than in Men Is Associated With Increased Gait Variability During Multitasking. J. Am. Med. Dir. Assoc. 2016, 17, 535–540. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Lamb, S.E.; Gates, S.; Cumming, R.G.; Rowe, B.H. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2009, Cd007146. [Google Scholar] [CrossRef]
- Svantesson, U.; Jones, J.; Wolbert, K.; Alricsson, M. Impact of Physical Activity on the Self-Perceived Quality of Life in Non-Frail Older Adults. J. Clin. Med. Res. 2015, 7, 585–593. [Google Scholar] [CrossRef]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength: A quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef]
- Csapo, R.; Gormasz, C.; Baron, R. Functional performance in community-dwelling and institutionalized elderly women. Wiener Klinische Wochenschrift 2009, 121, 383–390. [Google Scholar] [CrossRef]
- Mayer, F.; Scharhag-Rosenberger, F.; Carlsohn, A.; Cassel, M.; Muller, S.; Scharhag, J. The intensity and effects of strength training in the elderly. Deutsches Arzteblatt Int. 2011, 108, 359–364. [Google Scholar] [CrossRef]
- Stewart, V.H.; Saunders, D.H.; Greig, C.A. Responsiveness of muscle size and strength to physical training in very elderly people: A systematic review. Scand. J. Med. Sci. Sports 2014, 24, e1–10. [Google Scholar] [CrossRef]
- Physical Activities Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008; Department of Health and Human Services: Washington, DC, USA, 2008.
- Olesen, J.; Gustavsson, A.; Svensson, M.; Wittchen, H.U.; Jonsson, B. The economic cost of brain disorders in Europe. Eur. J. Neurol. 2012, 19, 155–162. [Google Scholar] [CrossRef]
- Josefsson, T.; Lindwall, M.; Archer, T. Physical exercise intervention in depressive disorders: Meta-analysis and systematic review. Scand. J. Med. Sci. Sports 2014, 24, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, S.; Tiedemann, A.; Sherrington, C.; Curtis, J.; Ward, P.B. Physical activity interventions for people with mental illness: A systematic review and meta-analysis. J. Clin. Psychiatry 2014, 75, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Aberg, M.A.; Waern, M.; Nyberg, J.; Pedersen, N.L.; Bergh, Y.; Aberg, N.D.; Nilsson, M.; Kuhn, H.G.; Toren, K. Cardiovascular fitness in males at age 18 and risk of serious depression in adulthood: Swedish prospective population-based study. Br. J. Psychiatry 2012, 201, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Carroll, D.D.; Blanck, H.M.; Serdula, M.K.; Brown, D.R. Obesity, physical activity, and depressive symptoms in a cohort of adults aged 51 to 61. J. Aging Health 2010, 22, 384–398. [Google Scholar] [CrossRef] [PubMed]
- Adamson, B.C.; Ensari, I.; Motl, R.W. Effect of exercise on depressive symptoms in adults with neurologic disorders: A systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Agudelo, L.Z.; Femenia, T.; Orhan, F.; Porsmyr-Palmertz, M.; Goiny, M.; Martinez-Redondo, V.; Correia, J.C.; Izadi, M.; Bhat, M.; Schuppe-Koistinen, I.; et al. Skeletal muscle PGC-1alpha1 modulates kynurenine metabolism and mediates resilience to stress-induced depression. Cell 2014, 159, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Kassow, M.; Deusser, M.; Thiel, C.; Otterbein, S.; Montag, C.; Reuter, M.; Banzer, W.; Kaiser, J. Physical Exercise during Encoding Improves Vocabulary Learning in Young Female Adults: A Neuroendocrinological Study. PLoS ONE 2013, 8, e64172. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M.; et al. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Winter, B.; Breitenstein, C.; Mooren, F.C.; Voelker, K.; Fobker, M.; Lechtermann, A.; Krueger, K.; Fromme, A.; Korsukewitz, C.; Floel, A.; et al. High impact running improves learning. Neurobiol. Learn. Mem. 2007, 87, 597–609. [Google Scholar] [CrossRef]
- Oppezzo, M.; Schwartz, D.L. Give your ideas some legs: The positive effect of walking on creative thinking. J. Exp. Psychol. 2014, 40, 1142–1152. [Google Scholar] [CrossRef]
- Kramer, A.F.; Marquez, D.X.; McAuley, E.; Kim, J.S.; Erickson, K.I.; Hu, L.; Scalf, P.E.; Prakash, R.; Colcombe, S.J.; Elavsky, S. Aerobic Exercise Training Increases Brain Volume in Aging Humans. J. Gerontol. 2006, 61, 1166–1170. [Google Scholar] [CrossRef]
- Spielman, L.J.; Little, J.P.; Klegeris, A. Physical activity and exercise attenuate neuroinflammation in neurological diseases. Brain Res. Bull. 2016, 125, 19–29. [Google Scholar] [CrossRef]
- Soundy, A.; Freeman, P.; Stubbs, B.; Probst, M.; Roskell, C.; Vancampfort, D. The Psychosocial Consequences of Sports Participation for Individuals with Severe Mental Illness: A Metasynthesis Review. Adv. Psychiatry 2015, 2015, 8. [Google Scholar] [CrossRef]
- Hassmen, P.; Koivula, N.; Uutela, A. Physical exercise and psychological well-being: A population study in Finland. Prev. Med. 2000, 30, 17–25. [Google Scholar] [CrossRef]
- Coakley, J. Youth Sports: What Counts as “Positive Development?”. J. Sport Soc. Issues 2011, 35, 306–324. [Google Scholar] [CrossRef]
- Seligman, M.E.P. Positive Health. Appl. Psychol. 2008, 57, 3–18. [Google Scholar] [CrossRef]
- Rongen, F.; Cobley, S.; McKenna, J.; Till, K. Talent identification and development. In Health and Elite Sport: Is High Performance Sport a Healthy Pursuit? Baker, J., Safai, P., Fraser-Thomas, J., Eds.; Routledge Research in Sport, Culture and Society; Taylor & Francis Group: London, UK, 2015. [Google Scholar]
- Baker, J.; Fraser-Thomas, J.; Dionigi, R.A.; Horton, S. Sport participation and positive development in older persons. Eur. Rev. Aging Phys. Act. 2010, 7, 3–12. [Google Scholar] [CrossRef]
- Walsh, D.W. Sport as a Resource Caravan: Examining the Role and Efficacy of Sport as a Resource Provider for Adults in Transition. Ph.D. Thesis, University of Texas at Austin, Austin, TX, USA, 2014. [Google Scholar]
- Rehn, A.; Möller, A. Den organiserade idrottens betydelse för spontanidrott; Gymnastik- och Idrottshögskolan: Stockholm, Sweden, 2011. [Google Scholar]
- Ratzlaff, C.R. Good news, bad news: Sports matter but occupational and household activity really matter - sport and recreation unlikely to be a panacea for public health. Br. J. Sports Med. 2012, 46, 699–701. [Google Scholar] [CrossRef]
- Lewis, C.J.; Reeves, M.J.; Roberts, S.J. Improving the physical and mental well-being of typically hard-to-reach men: An investigation of the impact of the Active Rovers project. Sport Soc. 2017, 20, 258–268. [Google Scholar] [CrossRef]
- Dunleavy, N. Proposed cuts to sport and recreation could hinder health of northern communities. CMAJ. 2008, 178, 1129. [Google Scholar] [CrossRef]
- Kim, J.; Kim, M.; Henderson, K.A.; Han, A.; Park, S.H. Serious engagement in sport and health benefits among Korean immigrants in the USA. Int. J. Qual. Stud. Health Well-Being 2016, 11, 31340. [Google Scholar] [CrossRef]
- Perrier, M.J.; Shirazipour, C.H.; Latimer-Cheung, A.E. Sport participation among individuals with acquired physical disabilities: Group differences on demographic, disability, and Health Action Process Approach constructs. Disabil. Health J. 2015, 8, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Engström, L.-M. Who is physically active? Cultural capital and sports participation from adolescence to middle age—A 38-year follow-up study. Phys. Educ. Sport Pedagog. 2008, 13, 319–343. [Google Scholar] [CrossRef]
- Brenner, J.S.; Council On Sports Medicine and Fitness. Sports Specialization and Intensive Training in Young Athletes. Pediatrics 2016, 138. [Google Scholar] [CrossRef]
- LaPrade, R.F.; Agel, J.; Baker, J.; Brenner, J.S.; Cordasco, F.A.; Cote, J.; Engebretsen, L.; Feeley, B.T.; Gould, D.; Hainline, B.; et al. AOSSM Early Sport Specialization Consensus Statement. Orthop. J. Sports Med. 2016, 4, 2325967116644241. [Google Scholar] [CrossRef]
- Tan, V.P.; Macdonald, H.M.; Kim, S.; Nettlefold, L.; Gabel, L.; Ashe, M.C.; McKay, H.A. Influence of physical activity on bone strength in children and adolescents: A systematic review and narrative synthesis. J. Bone Miner. Res. 2014, 29, 2161–2181. [Google Scholar] [CrossRef] [PubMed]
- Timmons, B.W.; Leblanc, A.G.; Carson, V.; Connor Gorber, S.; Dillman, C.; Janssen, I.; Kho, M.E.; Spence, J.C.; Stearns, J.A.; Tremblay, M.S. Systematic review of physical activity and health in the early years (aged 0-4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 773–792. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Roberts, K.C.; Thompson, W. Is adherence to the Canadian 24-Hour Movement Behaviour Guidelines for Children and Youth associated with improved indicators of physical, mental, and social health? Appl. Physiol. Nutr. Metab. 2017, 42, 725–731. [Google Scholar] [CrossRef]
- Fedewa, M.V.; Gist, N.H.; Evans, E.M.; Dishman, R.K. Exercise and insulin resistance in youth: A meta-analysis. Pediatrics 2014, 133, e163–e174. [Google Scholar] [CrossRef]
- Jayanthi, N.; Pinkham, C.; Dugas, L.; Patrick, B.; Labella, C. Sports specialization in young athletes: Evidence-based recommendations. Sports Health 2013, 5, 251–257. [Google Scholar] [CrossRef]
- Wattie, N.; Schorer, J.; Baker, J. The relative age effect in sport: A developmental systems model. Sports Med. 2015, 45, 83–94. [Google Scholar] [CrossRef]
- Delorme, N.; Raspaud, M. The relative age effect in young French basketball players: A study on the whole population. Scand. J. Med. Sci. Sports 2009, 19, 235–242. [Google Scholar] [CrossRef]
- Fumarco, L.; Gibbs, B.G.; Jarvis, J.A.; Rossi, G. The relative age effect reversal among the National Hockey League elite. PLoS ONE 2017, 12, e0182827. [Google Scholar] [CrossRef]
- Geithner, C.A.; Molenaar, C.; Henriksson, T.; Fjellman-Wiklund, A. Relative Age Effects in Women’s Ice Hockey. Women Sport Phys. Act. J. 2018, 26, 124–133. [Google Scholar] [CrossRef]
- Gerdin, G.; Hedberg, M.; Hageskog, C.A. Relative Age Effect in Swedish Male and Female Tennis Players Born in 1998(-)2001. Sports 2018, 6, 38. [Google Scholar] [CrossRef]
- Jones, C.; Visek, A.J.; Barron, M.J.; Hyman, M.; Chandran, A. Association between relative age effect and organisational practices of American youth football. J. Sports Sci. 2018, 1–8. [Google Scholar] [CrossRef]
- Edwards, L.C.; Bryant, A.S.; Keegan, R.J.; Morgan, K.; Cooper, S.M.; Jones, A.M. ‘Measuring’ Physical Literacy and Related Constructs: A Systematic Review of Empirical Findings. Sports Med. 2017. [Google Scholar] [CrossRef]
- Bahr, R. Demise of the fittest: Are we destroying our biggest talents? Br. J. Sports Med. 2014, 48, 1265–1267. [Google Scholar] [CrossRef]
- Kenttä, G.; Svensson, M. Idrottarens återhämtningsbok, fysiologiska, psykologiska och näringsmässiga fakta för snabb och effektiv återhämtning; SISU Idrottsböcker: Stockholm, Sweden, 2008. [Google Scholar]
- Blair, S.N.; Kohl, H.W., 3rd; Barlow, C.E.; Paffenbarger, R.S., Jr.; Gibbons, L.W.; Macera, C.A. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA 1995, 273, 1093–1098. [Google Scholar] [CrossRef]
- Paffenbarger, R.S., Jr.; Kampert, J.B.; Lee, I.M.; Hyde, R.T.; Leung, R.W.; Wing, A.L. Changes in physical activity and other lifeway patterns influencing longevity. Med. Sci. Sports Exerc. 1994, 26, 857–865. [Google Scholar] [CrossRef]
- Rivera-Torres, S.; Fahey, T.D.; Rivera, M.A. Adherence to Exercise Programs in Older Adults: Informative Report. Gerontol. Geriatr. Med. 2019, 5, 2333721418823604. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Hamer, M.; Lavoie, K.L.; Bacon, S.L. Taking up physical activity in later life and healthy ageing: The English longitudinal study of ageing. Br. J. Sports Med. 2014, 48, 239–243. [Google Scholar] [CrossRef]
- Cobley, S.; Baker, J.; Wattie, N.; McKenna, J. Annual age-grouping and athlete development: A meta-analytical review of relative age effects in sport. Sports Med. 2009, 39, 235–256. [Google Scholar] [CrossRef]
- Unhjem, R.; Nygard, M.; van den Hoven, L.T.; Sidhu, S.K.; Hoff, J.; Wang, E. Lifelong strength training mitigates the age-related decline in efferent drive. J. Appl. Physiol. (Bethesda Md. 1985) 2016, 121, 415–423. [Google Scholar] [CrossRef]
- Power, G.A.; Allen, M.D.; Gilmore, K.J.; Stashuk, D.W.; Doherty, T.J.; Hepple, R.T.; Taivassalo, T.; Rice, C.L. Motor unit number and transmission stability in octogenarian world class athletes: Can age-related deficits be outrun? J. Appl. Physiol. (Bethesda Md. 1985) 2016, 121, 1013–1020. [Google Scholar] [CrossRef]
- Matelot, D.; Schnell, F.; Kervio, G.; Ridard, C.; Thillaye du Boullay, N.; Wilson, M.; Carre, F. Cardiovascular Benefits of Endurance Training in Seniors: 40 is not too Late to Start. Int. J. Sports Med. 2016, 37, 625–632. [Google Scholar] [CrossRef]
- Lepers, R.; Stapley, P.J. Master Athletes Are Extending the Limits of Human Endurance. Front. Physiol. 2016, 7, 613. [Google Scholar] [CrossRef]
- Parkkari, J.; Natri, A.; Kannus, P.; Manttari, A.; Laukkanen, R.; Haapasalo, H.; Nenonen, A.; Pasanen, M.; Oja, P.; Vuori, I. A controlled trial of the health benefits of regular walking on a golf course. Am. J. Med. 2000, 109, 102–108. [Google Scholar] [CrossRef]
- Broman, G.; Johnsson, L.; Kaijser, L. Golf: A high intensity interval activity for elderly men. Aging Clin. Exp. Res. 2004, 16, 375–381. [Google Scholar] [CrossRef]
- Kiss, O.; Sydo, N.; Vargha, P.; Edes, E.; Merkely, G.; Sydo, T.; Merkely, B. Prevalence of physiological and pathological electrocardiographic findings in Hungarian athletes. Acta Physiol. Hung. 2015, 102, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Shapero, K.; Deluca, J.; Contursi, M.; Wasfy, M.; Weiner, R.B.; Lewis, G.D.; Hutter, A.; Baggish, A.L. Cardiovascular Risk and Disease Among Masters Endurance Athletes: Insights from the Boston MASTER (Masters Athletes Survey to Evaluate Risk) Initiative. Sports Med. Open 2016, 2, 29. [Google Scholar] [CrossRef] [PubMed]
- Yankelson, L.; Sadeh, B.; Gershovitz, L.; Werthein, J.; Heller, K.; Halpern, P.; Halkin, A.; Adler, A.; Steinvil, A.; Viskin, S. Life-threatening events during endurance sports: Is heat stroke more prevalent than arrhythmic death? J. Am. Coll. Cardiol. 2014, 64, 463–469. [Google Scholar] [CrossRef]
- Strimel, W.J.; O’Riordan, M.J. Sudden cardiac arrest in long distance races: Considering the full context. J. Am. Coll. Cardiol. 2015, 65, 407–408. [Google Scholar] [CrossRef][Green Version]
- Piasecki, M.; Ireland, A.; Coulson, J.; Stashuk, D.W.; Hamilton-Wright, A.; Swiecicka, A.; Rutter, M.K.; McPhee, J.S.; Jones, D.A. Motor unit number estimates and neuromuscular transmission in the tibialis anterior of master athletes: Evidence that athletic older people are not spared from age-related motor unit remodeling. Physiol. Rep. 2016, 4. [Google Scholar] [CrossRef]
- Moreira, N.B.; Mazzardo, O.; Vagetti, G.C.; De Oliveira, V.; De Campos, W. Quality of life perception of basketball master athletes: Association with physical activity level and sports injuries. J. Sports Sci. 2016, 34, 988–996. [Google Scholar] [CrossRef]
- Haigh, E.A.P.; Bogucki, O.E.; Sigmon, S.T.; Blazer, D.G. Depression Among Older Adults: A 20-Year Update on Five Common Myths and Misconceptions. Am. J. Geriatr. Psychiatry 2018, 26, 107–122. [Google Scholar] [CrossRef]
- Alfini, A.J.; Weiss, L.R.; Leitner, B.P.; Smith, T.J.; Hagberg, J.M.; Smith, J.C. Hippocampal and Cerebral Blood Flow after Exercise Cessation in Master Athletes. Front. Aging Neurosci. 2016, 8, 184. [Google Scholar] [CrossRef]
- Lazarus, N.R.; Harridge, S.D.R. Declining performance of master athletes: Silhouettes of the trajectory of healthy human ageing? J. Physiol. 2017, 595, 2941–2948. [Google Scholar] [CrossRef]









© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).