
Field Study on Winter Thermal Comfort of Occupants of Nursing Homes in Shandong Province, China


Abstract
:1. Introduction
2. Method
2.1. Description of the Climatology
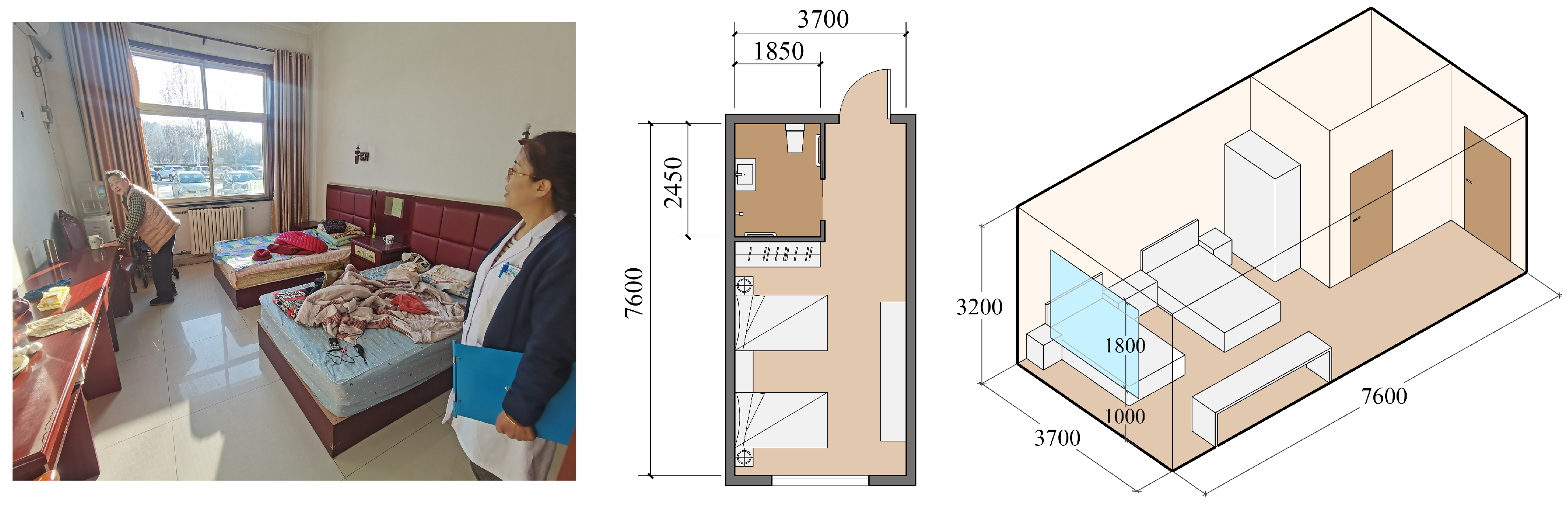
2.2. Nursing Homes’ Information
2.3. Questionnaire Survey
- (1)
- Basic information, such as the time and place of filling out the form, gender, age, and room heating method.
- (2)
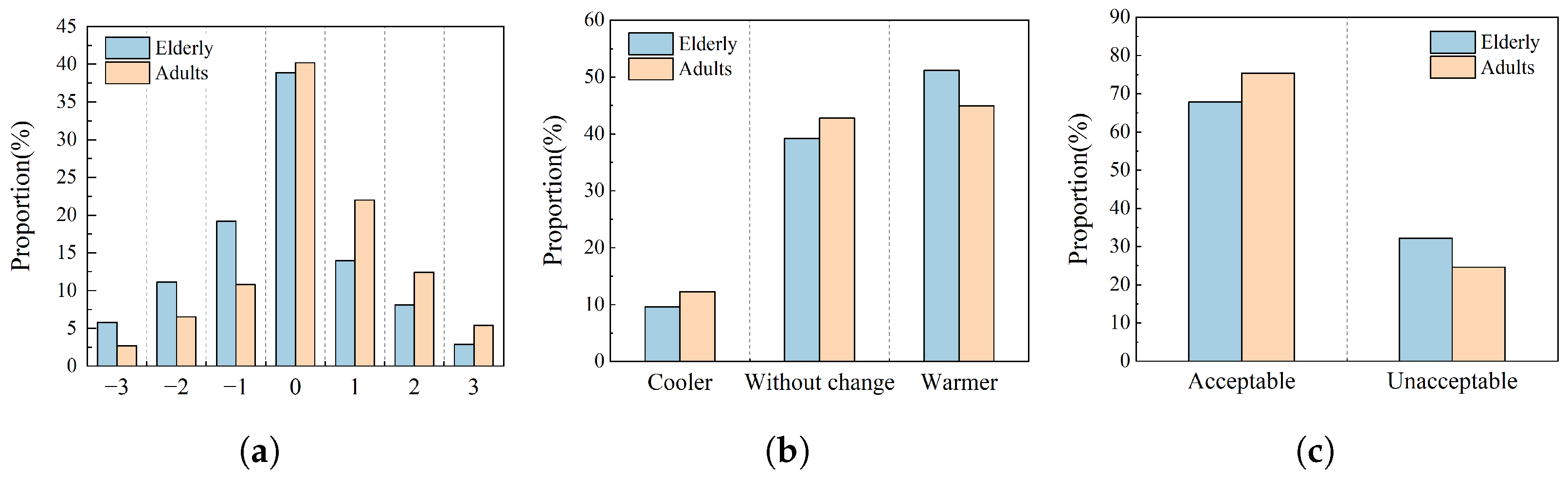
- Thermal comfort conditions, including thermal sensation vote (TSV), thermal preference (P), and thermal acceptability (A). The thermal sensation vote was assessed using the 7-point thermal sensation scale from the ASHRAE 55, thermal preference was assessed using a 3-point scale, and thermal acceptability was assessed using a 2-point scale. Table 1 shows detailed indicators.
- (3)
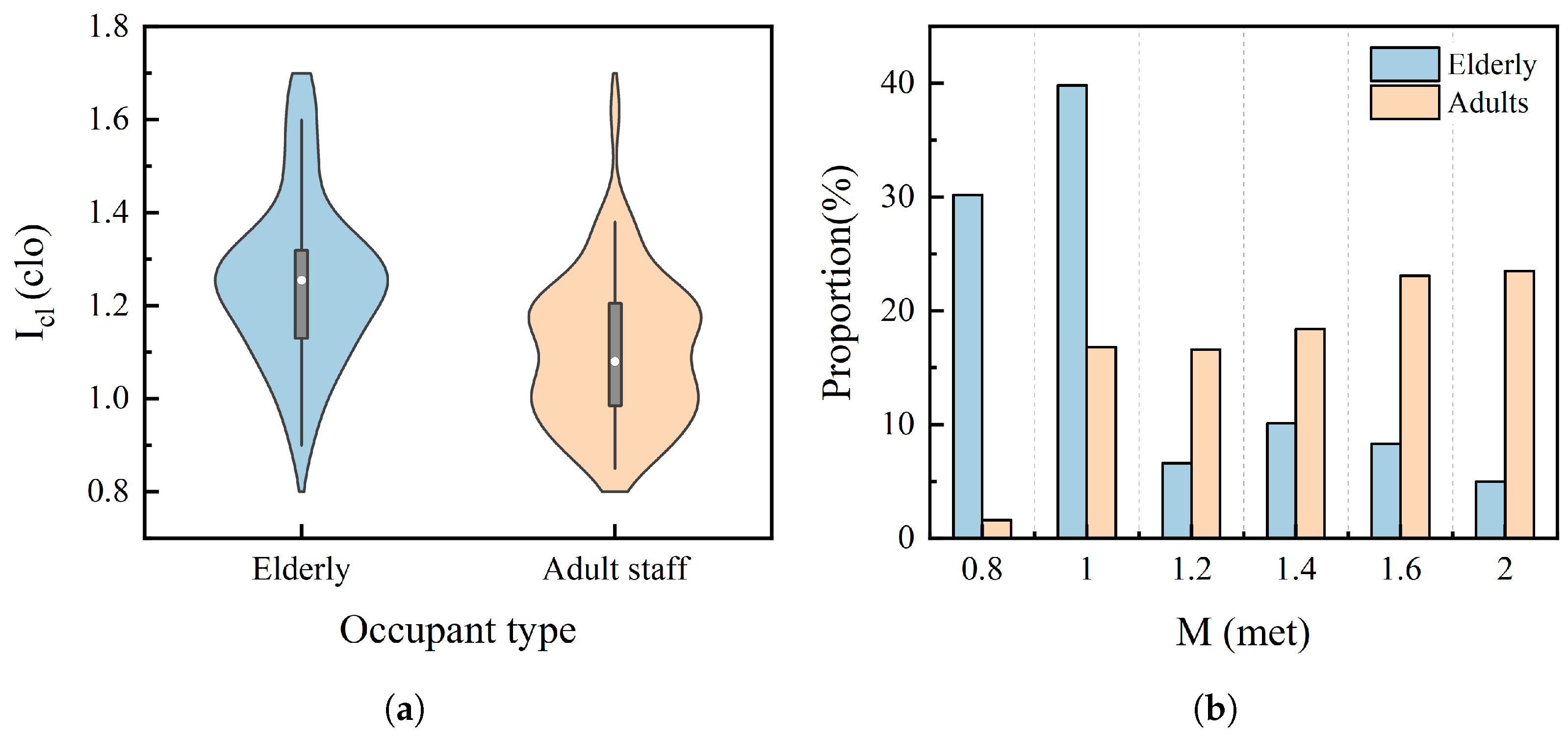
- Clothing and activity conditions.
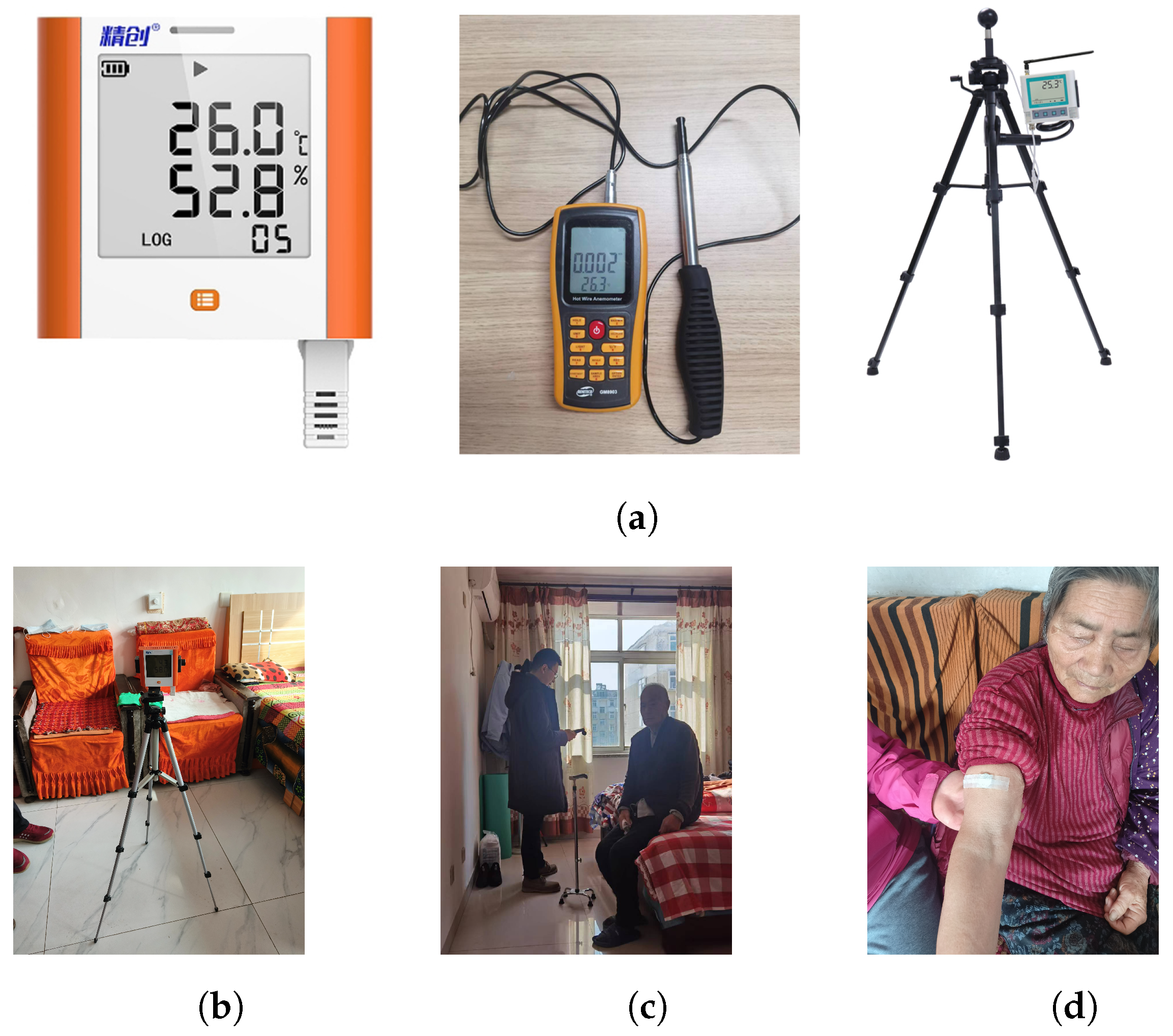
2.4. Parameter Testing and Calculation
2.5. Simulation of Energy Consumption and Carbon Dioxide Emissions
2.6. Data Statistics and Analysis Modeling
3. Results
3.1. Outdoor and Indoor Environmental Conditions
3.2. Thermal Comfort Voting for Different Types of Occupants
3.3. Neutral Temperature and Comfort Zone for Different Types of Occupants
3.4. Applicability of the PMV Model to Occupants
3.5. Preferred Temperatures for Different Types of Occupants
3.6. Influence of Personal Factors on Thermal Comfort
3.7. Influence of Physiological Factors on Thermal Comfort
4. Discussion
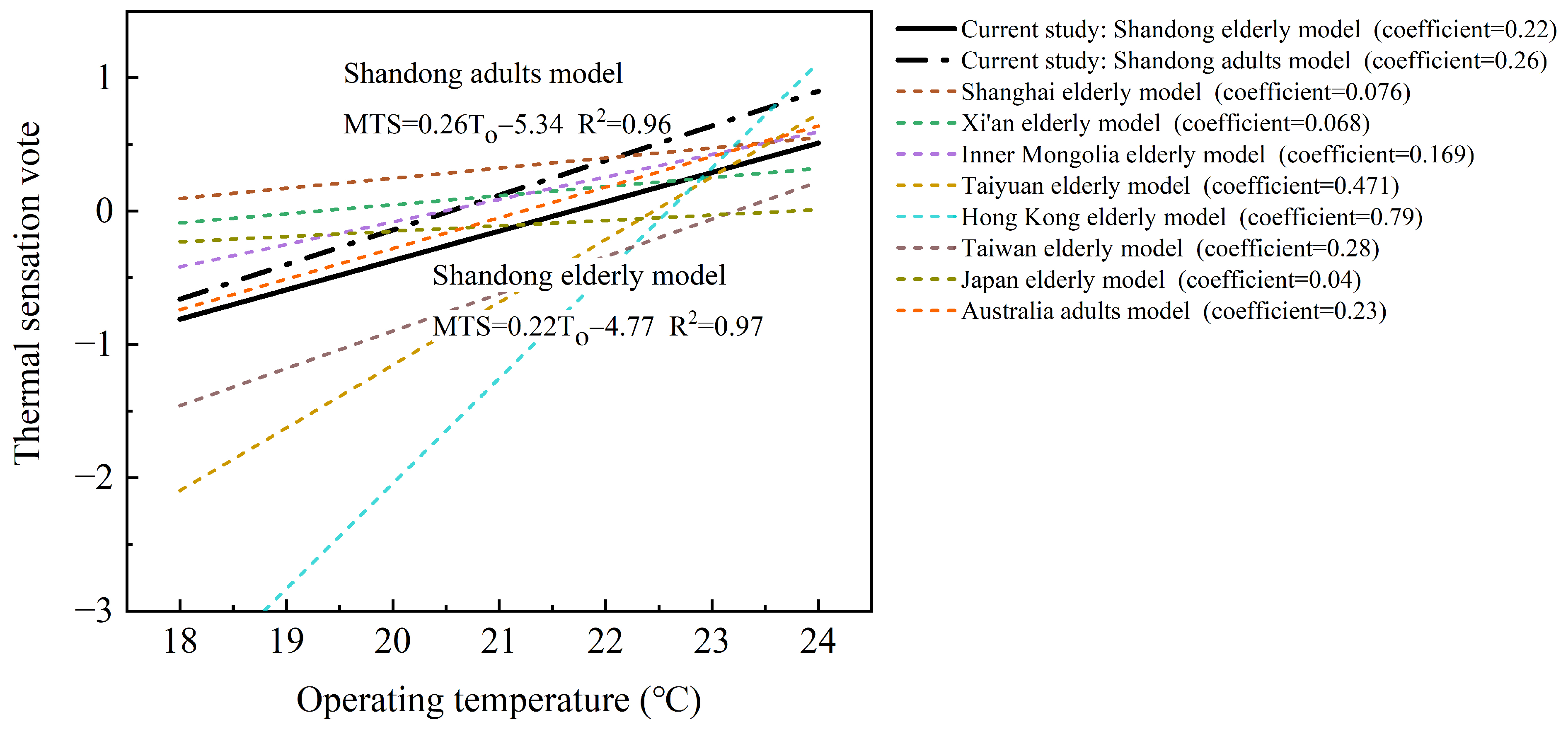
4.1. Comparison with Previous Research Results
4.2. Influence of Thermal Comfort on Energy Consumption and Carbon Emissions
5. Conclusions
- (1)
- The chi-square test shows a significant difference in thermal sensation between the elderly and adults in nursing homes. Under the same environmental conditions, elderly people perceive the thermal environment as cooler than adults. Regression analysis revealed that the measured neutral temperatures for elderly and adult occupants in nursing homes are 21.7 and 20.5 °C, respectively. Their comfortable temperature ranges are 19.4–24.0 °C and 18.6–22.5 °C, respectively. The measured neutral temperature and the limits of the comfortable temperature range for elderly people are both higher than those for adults. The comfortable temperature range for elderly people is broader. This indicates that the elderly have higher demands for thermal environments compared to adults and prefer a warmer environment. Designers can use these parameters to create nursing home spaces with comfortable thermal environments, while managers can assess whether existing facilities meet thermal comfort requirements. Applying the results of this study will enhance the quality of life for nursing home occupants, increase their well-being and productivity, and offer substantial social benefits.
- (2)
- Through regression analysis, the differences in thermal preferences between the elderly and adults were further identified. The preferred temperature for the elderly is 23.8 °C, while the adults’ preferred temperature is lower, at 23.1 °C. However, for both the elderly and adults, the preferred temperature is higher than their respective neutral temperatures by 2.1 and 2.6 °C. This indicates that nursing home occupants in winter prefer a warmer environment than the neutral temperature, reflecting a higher psychological expectation for the thermal environment. Excessively high temperatures can lead to energy waste, so nursing home managers should encourage the elderly to actively adapt to the indoor thermal environment through thermal adaptive behaviors while also enhancing the facility’s insulation performance using passive building technologies to improve sustainability.
- (3)
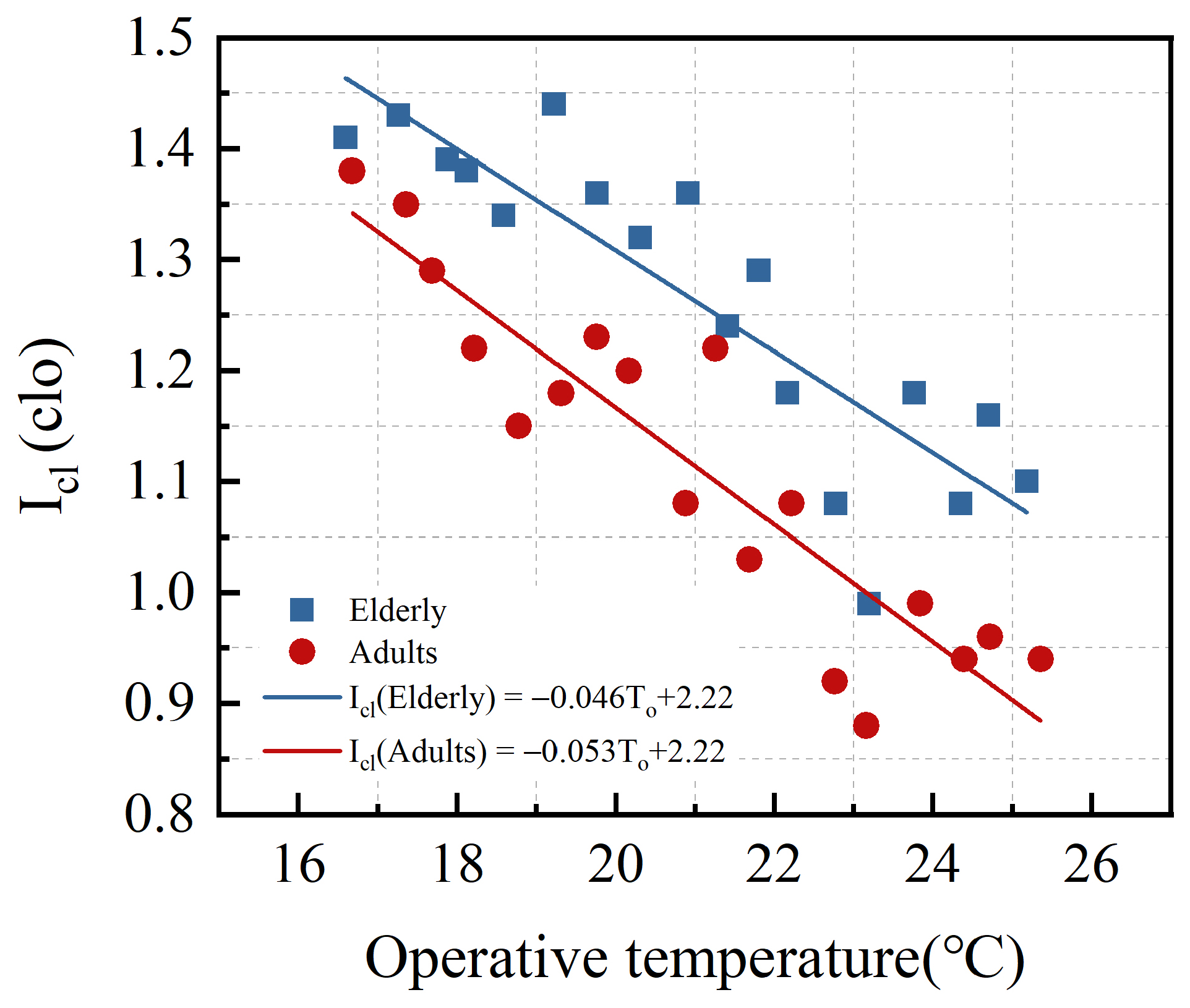
- The adaptive behavior of nursing home occupants to the thermal environment mainly involves adjusting their clothing. By modeling the relationship between clothing insulation and operative temperature, it was found that at the same operative temperature, the clothing insulation of the elderly is higher than that of adults. For each 1 °C increase in operative temperature, the clothing insulation decreases by approximately 0.046 clo for the elderly and 0.053 clo for adults. This proves that the elderly have a higher tolerance for high temperatures than adults and require more clothing to maintain thermal comfort in the same thermal environment. The conclusions of this study can help nursing home staff provide scientific guidance on the daily dressing behavior of the elderly, aiding them in better adapting to the thermal environment and preventing some elderly individuals from being exposed to cold environments for long periods due to inappropriate clothing, thereby reducing health risks.
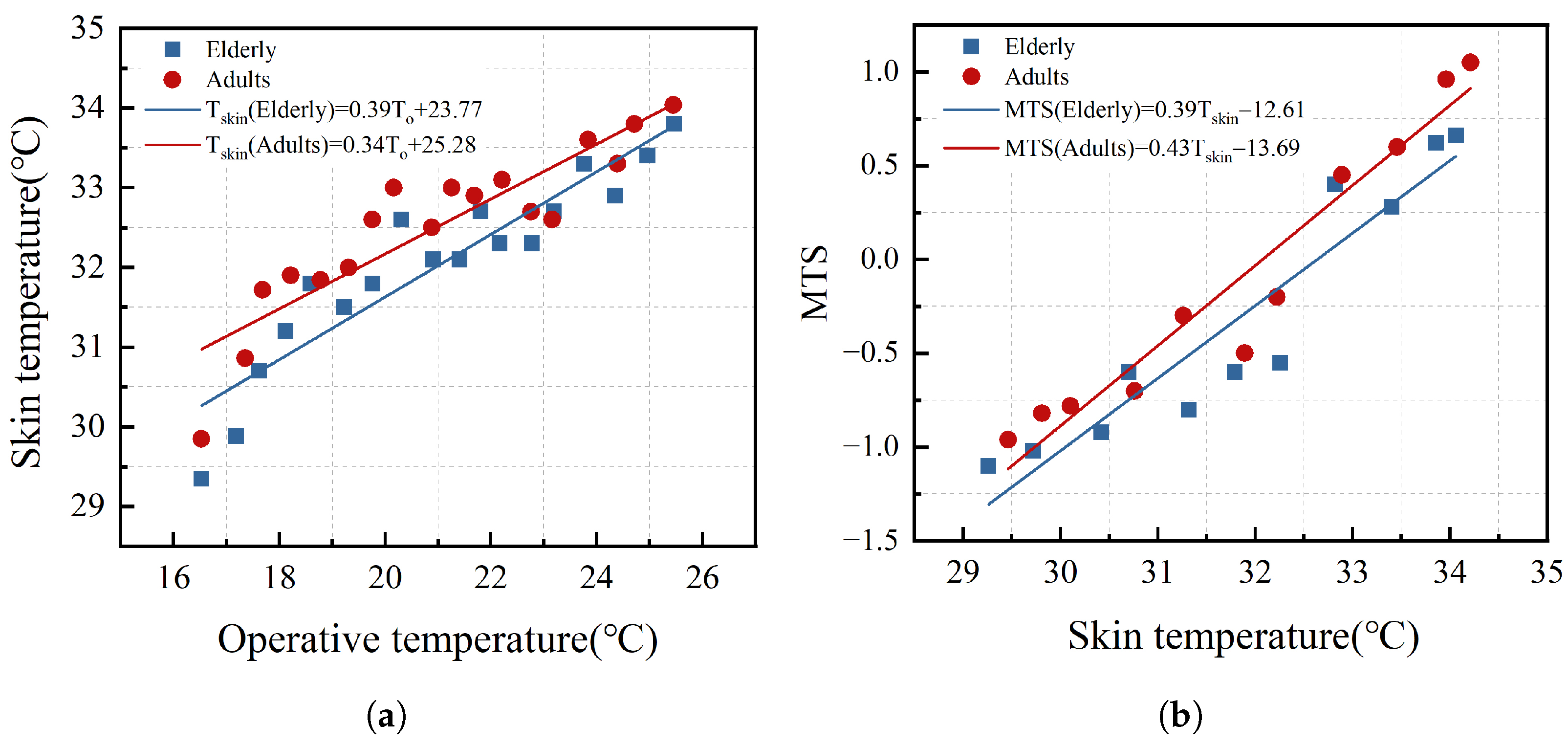
- (4)
- Regression analysis found that there is a correlation between skin temperature and thermal comfort parameters. When the operative temperature is the same, the average skin temperature of the elderly is lower than that of adults. For each 1 °C decrease in operative temperature, the average skin temperature of the elderly and adults decreases by 0.39 and 0.34 °C, respectively. With the same average skin temperature, the MTS value of the elderly is lower than that of adults. For every 1 °C increase in average skin temperature, the MTS increases by 0.39 units for the elderly and 0.43 units for adults. This indicates that the physiological thermal regulation of the elderly slows down, making them less sensitive to changes in skin temperature and feeling colder in the same thermal environment. Therefore, it is recommended that nursing home staff regularly monitor the skin temperature of the elderly during daily care to prevent skin hypothermia caused by inappropriate behavior, reduced thermoregulatory capacity, or illness, which could negatively impact thermal comfort.
- (5)
- The heating set temperature in nursing homes can be controlled within the comfort temperature range. However, energy consumption simulations show that lowering the heating set temperature can reduce energy consumption and carbon emissions. For each 1 °C reduction, the heating energy consumption and carbon emissions in the typical room decrease by 2.3 kWh/°C and 0.8 , respectively, with cuts of 11.1 and 11.9%. Therefore, it is recommended that nursing homes use the lower limit of the comfort temperature range as the actual heating set temperature and adjust the heating temperature according to the primary user groups. The heating set temperature for rooms like bedrooms and activity rooms, which are used primarily by the elderly, can be set to the lower limit of the elderly’s comfort temperature range at 19.4 °C. For rooms such as offices and workspaces used primarily by adult staff, the heating set temperature can be set to the lower limit of the adult comfort temperature range at 18.6 °C. Additionally, on the basis of lowering the heating set temperature, improving the insulation performance of nursing homes through passive building techniques can further reduce energy consumption. Measures that can be taken include adding high-performance insulation layers to roofs and exterior walls, replacing doors and windows with lower heat transfer coefficient, reasonably controlling the window-to-wall area ratio on each facade, and adding sunrooms. Lowering the heating set temperature and improving the building’s insulation performance can effectively reduce energy consumption, offering significant economic and environmental benefits.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Mȩczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ageing and Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 20 June 2023).
- Department of Economic and Social Affairsn. World Population Ageing 2017 Highlights. 2017. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 12 December 2023).
- National Institute on Aging. Census Bureau Releases Report on Aging in Asia. 2022. Available online: https://www.nia.nih.gov/news/census-bureau-releases-report-aging-asia (accessed on 6 December 2023).
- National Bureau of Statistics of China Office of the Leading Group of the State Council for the Seventh National Population Census. Communiqué of the Seventh National Population Census. 2021. Available online: https://www.stats.gov.cn/english/PressRelease/202105/t20210510_1817190.html (accessed on 6 January 2024).
- National Development and Reform Commission. Plan for the Development of National Elderly Care and the Elderly Care Service System during the 14th Five Year Plan Period. 2021. Available online: https://www.ndrc.gov.cn/fggz/fzzlgh/gjjzxgh/202203/t20220325_1320220_ext.html?eqid=822461d80000b67000000006647d59dd. (accessed on 8 January 2024).
- Yang, J.; Nam, I.; Sohn, J.R. The influence of seasonal characteristics in elderly thermal comfort in Korea. Energy Build. 2016, 128, 583–591. [Google Scholar] [CrossRef]
- Salata, F.; Golasi, I.; Petitti, D.; de Lieto Vollaro, E.; Coppi, M.; de Lieto Vollaro, A. Relating microclimate, human thermal comfort and health during heat waves: An analysis of heat island mitigation strategies through a case study in an urban outdoor environment. Sustain. Cities Soc. 2017, 30, 79–96. [Google Scholar] [CrossRef]
- Shchukina, I.; Youm, Y.H.; Ryu, S.; Young, K.; Camell, C.; Dlugos, T.; Artyomov, M.; Dixit, V.; Goldberg, E.; Tsusaka, T. IL-33 causes thermogenic failure in aging by expanding dysfunctional adipose ILC2. Cell Metab. 2021, 33, 2277–2287.e5. [Google Scholar] [CrossRef]
- Xiong, J.; Ma, T.; Lian, Z.; de Dear, R. Perceptual and physiological responses of elderly subjects to moderate temperatures. Build. Environ. 2019, 156, 117–122. [Google Scholar] [CrossRef]
- Jiao, Y.; Yu, Y.; Hu, Y.; Zhang, Q.; Yu, H. Evidence-based Study on the Effects of Indoor Thermal Environment on Physiological Parameters and Health of the Older People in Shanghai Aged Home. Archit. Tech. 2020, 26, 45–49. [Google Scholar]
- Gomez-Acebo, I.; Llorca, J.; Dierssen, T. Cold-related mortality due to cardiovascular diseases, respiratory diseases and cancer: A case-crossover study. Public Health 2013, 127, 252–258. [Google Scholar] [CrossRef]
- Chen, T.H.; Li, X.; Zhao, J.; Zhang, K. Impacts of cold weather on all-cause and cause-specific mortality in Texas, 1990–2011. Environ. Pollut. 2017, 225, 244–251. [Google Scholar] [CrossRef]
- Savaresi, A. The Paris Agreement: A new beginning? J. Energy Nat. Resour. Law 2016, 34, 16–26. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, C.H.; Chen, X.J.; Jia, L.Q.; Guo, X.N.; Chen, R.S.; Zhang, M.S.; Chen, Z.Y.; Wang, H.D. Carbon peak and carbon neutrality in China: Goals, implementation path and prospects. China Geol. 2021, 4, 720–746. [Google Scholar] [CrossRef]
- GBT50176; Thermal Design Code for Civil Building. Ministry of Housing and Urban-Rural Development of the People’s Republic of China, China Architecture and Building Press: Beijing, China, 2016.
- Yang, L.; Yan, H.; Lam, J.C. Thermal comfort and building energy consumption implications—A review. Appl. Energy 2014, 115, 164–173. [Google Scholar] [CrossRef]
- Bienvenido-Huertas, D.; Rubio-Bellido, C.; Farinha, F.; Oliveira, M.J.; Pérez-Ordóñez, J.L. Evaluating the potential of adaptive comfort approach using historic data to reduce energy consumption in buildings in southern Spain. Build. Environ. 2020, 185, 107313. [Google Scholar] [CrossRef] [PubMed]
- ANSI/ASHRAE Standard 55; Thermal Environmental Conditions for Human Occupancy. American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.: Peachtree Corners, GA, USA, 2017.
- ISO 7730; Ergonomics of the Thermal Environment—Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria. International Organization for Standardization: Geneva, Switzerland, 2005.
- EN 16798-1:2019; Energy Performance of Buildings—Ventilation for Buildings—Part 1: Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics. European Committee for Standardization: Brussels, Belgium, 2019.
- Baquero, M.T.; Forcada, N. Thermal comfort of older people during summer in the continental Mediterranean climate. J. Build. Eng. 2022, 54, 104680. [Google Scholar] [CrossRef]
- Zaki, S.A.; Damiati, S.A.; Rijal, H.B.; Hagishima, A.; Abd Razak, A. Adaptive thermal comfort in university classrooms in Malaysia and Japan. Build. Environ. 2017, 122, 294–306. [Google Scholar] [CrossRef]
- Zheng, P.; Wu, H.; Liu, Y.; Ding, Y.; Yang, L. Thermal comfort in temporary buildings: A review. Build. Environ. 2022, 221, 109262. [Google Scholar] [CrossRef]
- GB 50736; Design Code for Heating Ventilation and Air Conditioning of Civil Buildings. Ministry of Housing and Urban-Rural Development of the People’s Republic of China, China Architecture and Building Press: Beijing, China, 2012.
- Jiao, Y.; Yu, H.; Wang, T.; An, Y.; Yu, Y. Thermal comfort and adaptation of the elderly in free-running environments in Shanghai, China. Build. Environ. 2017, 118, 259–272. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, H.; Li, B.; Kosonen, R.; Kong, D.; Zhou, S.; Yao, R. Thermal adaptation of the elderly during summer in a hot humid area: Psychological, behavioral, and physiological responses. Energy Build. 2019, 203, 109450. [Google Scholar] [CrossRef]
- Zhang, Z.; Xiao, Y.; Ren, Z. Study on Heating Status and Thermal Comfort in Rural Areas of Southwest Mountainous Area in Winter: Take Northwest Guizhou as An Example. J. Hum. Settlements West China 2023, 38, 80–86. [Google Scholar]
- Larriva, M.T.B.; Higueras, E. Health risk for older adults in Madrid, by outdoor thermal and acoustic comfort. Urban Clim. 2020, 34, 100724. [Google Scholar] [CrossRef]
- Forcada, N.; Gangolells, M.; Casals, M.; Tejedor, B.; Macarulla, M.; Gaspar, K. Summer thermal comfort in nursing homes in the Mediterranean climate. Energy Build. 2020, 229, 110442. [Google Scholar] [CrossRef]
- Jin, Y.; Wang, F.; Payne, S.R.; Weller, R.B. A comparison of the effect of indoor thermal and humidity condition on young and older adults’ comfort and skin condition in winter. Indoor Built Environ. 2022, 31, 759–776. [Google Scholar] [CrossRef]
- Larriva, M.T.B.; García, E.H. Thermal comfort for the elderly: A systematic review of the scientific literature. Rev. Esp. Geriatr. Gerontol. 2019, 54, 280–295. [Google Scholar] [CrossRef]
- Hughes, C.; Natarajan, S.; Liu, C.; Chung, W.J.; Herrera, M. Winter thermal comfort and health in the elderly. Energy Policy 2019, 134, 110954. [Google Scholar] [CrossRef]
- Sudarsanam, N.; Kannamma, D. Investigation of summertime thermal comfort at the residences of elderly people in the warm and humid climate of India. Energy Build. 2023, 291, 113151. [Google Scholar] [CrossRef]
- Forcada, N.; Gangolells, M.; Casals, M.; Tejedor, B.; Macarulla, M.; Gaspar, K. Field study on thermal comfort in nursing homes in heated environments. Energy Build. 2021, 244, 111032. [Google Scholar] [CrossRef]
- Hwang, R.L.; Chen, C.P. Field study on behaviors and adaptation of elderly people and their thermal comfort requirements in residential environments. Indoor Air 2010, 20, 235–245. [Google Scholar] [CrossRef]
- Tartarini, F.; Cooper, P.; Fleming, R. Thermal perceptions, preferences and adaptive behaviours of occupants of nursing homes. Build. Environ. 2018, 132, 57–69. [Google Scholar] [CrossRef]
- Liu, G.; Cen, C.; Zhang, Q.; Liu, K.; Dang, R. Field study on thermal comfort of passenger at high-speed railway station in transition season. Build. Environ. 2016, 108, 220–229. [Google Scholar] [CrossRef]
- Jia, C.; Zhang, Z.; Wang, M.; Han, S.; Cao, J.; Rong, Y.; Du, C. Investigation on indoor thermal environment of industrial heritage during the cooling season and its impacts on thermal comfort. Case Stud. Therm. Eng. 2023, 52, 103769. [Google Scholar] [CrossRef]
- Li, H.; Xu, G.; Chen, J.; Duan, J. Investigating the adaptive thermal comfort of the elderly in rural mutual aid homes in central inner mongolia. Sustainability 2022, 14, 6802. [Google Scholar] [CrossRef]
- GB/T 50785; Evaluation Standard for Indoor Thermal Environment in Civil Buildings. Ministry of Housing and Urban-Rural Development of the People’s Republic of China, China Architecture and Building Press: Beijing, China, 2012.
- Liang, S.; Xie, Y.; Chen, Y.; Cheng, Y.; Zhang, H. Field study on inpatient’s thermal comfort in general ward in winter. Build. Sci. 2022, 38, 144–152. [Google Scholar]
- Kharvari, F. An empirical validation of daylighting tools: Assessing radiance parameters and simulation settings in Ladybug and Honeybee against field measurements. Sol. Energy 2020, 207, 1021–1036. [Google Scholar] [CrossRef]
- Yan, H.; Yan, K.; Ji, G. Optimization and prediction in the early design stage of office buildings using genetic and XGBoost algorithms. Build. Environ. 2022, 218, 109081. [Google Scholar] [CrossRef]
- Kainaga, T.; Sagisaka, K.; Yamada, R.; Nakaya, T. A case study of a nursing home in nagano, Japan: Field survey on thermal comfort and building energy simulation for future climate change. Energies 2022, 15, 936. [Google Scholar] [CrossRef]
- Fanger, P.O. Assessment of man’s thermal comfort in practice. Occup. Environ. Med. 1973, 30, 313–324. [Google Scholar] [CrossRef]
- Lai, D.; Zhou, X.; Chen, Q. Measurements and predictions of the skin temperature of human subjects on outdoor environment. Energy Build. 2017, 151, 476–486. [Google Scholar] [CrossRef]
- Tian, X.; Shi, L.; Wang, Z.; Liu, W. A thermal comfort evaluation model based on facial skin temperature. Build. Environ. 2023, 235, 110244. [Google Scholar] [CrossRef]
- Zhou, S.; Li, B.; Du, C.; Liu, H.; Wu, Y.; Hodder, S.; Chen, M.; Kosonen, R.; Ming, R.; Ouyang, L.; et al. Opportunities and challenges of using thermal comfort models for building design and operation for the elderly: A literature review. Renew. Sustain. Energy Rev. 2023, 183, 113504. [Google Scholar] [CrossRef]
- Jiao, Y.; Yu, H.; Yu, Y.; Wang, Z.; Wei, Q. Adaptive thermal comfort models for homes for older people in Shanghai, China. Energy Build. 2020, 215, 109918. [Google Scholar] [CrossRef]
- Zheng, W.; Shao, T.; Lin, Y.; Wang, Y.; Dong, C.; Liu, J. A field study on seasonal adaptive thermal comfort of the elderly in nursing homes in Xi’an, China. Build. Environ. 2022, 208, 108623. [Google Scholar] [CrossRef]
- Liu, X.; Yue, P. Investigation and study on winter indoor thermal environment of reconstructed nursing homes for the elderly in Taiyuan. Heat. Vent. Air Cond. 2019, 49, 120–127. [Google Scholar]
- Tao, Y.; Gou, Z.; Yu, Z.; Fu, J.; Chen, X. The challenge of creating age-friendly indoor environments in a high-density city: Case study of Hong Kong’s care and attention homes. J. Build. Eng. 2020, 30, 101280. [Google Scholar] [CrossRef]
- Tartarini, F.; Cooper, P.; Fleming, R. Thermal environment and thermal sensations of occupants of nursing homes: A field study. Procedia Eng. 2017, 180, 373–382. [Google Scholar] [CrossRef]
- Forcada, N.; Gangolells, M.; Casals, M.; Tejedor, B.; Macarulla, M.; Gaspar, K. Field study on adaptive thermal comfort models for nursing homes in the Mediterranean climate. Energy Build. 2021, 252, 111475. [Google Scholar] [CrossRef]
- GB 55015; General Code for Energy Efficiency and Renewable Energy Application in Buildings. Ministry of Housing and Urban-Rural Development of the People’s Republic of China, China Architecture and Building Press: Beijing, China, 2021.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Question | Scale |
|---|---|---|
| TSV | How do you feel at this moment? | −3 Cold, −2 Cool, −1 Slightly cool, 0 Neutral, +1 Slightly warm, +2 Warm, +3 Hot |
| P | What would you prefer at this moment? | −1 Cooler, 0 Without change, +1 Warmer |
| A | Is the thermal environment acceptable at this moment? | 1 Acceptable, 0 Unacceptable |
| Activity | Reclining | Seated–TV/Chatting | Seated–Filing | Standing–Relax | Standing–Walking about | Standing–House Cleaning |
|---|---|---|---|---|---|---|
| M (met) | 0.8 | 1.0 | 1.2 | 1.4 | 1.6 | 2.0 |
| Room | Bedroom | Activity Room | Medical Room | Office and Workspace | Public Spaces (Corridors, Foyers, etc.) |
|---|---|---|---|---|---|
| Number of elderly people | 525 | 62 | 32 | 0 | 109 |
| Number of adult staff | 41 | 28 | 30 | 101 | 26 |
| Test Parameters | Testing Instruments | Testing Instruments |
|---|---|---|
| Air temperature () Relative humidity () | Elitech GSP-8A temperature and humidity recorder | Air temperature: Range: −40–85 °C; Precision: ±0.3 °C; Resolution ratio: 0.1 °C |
| Relative humidity: Range: 10–90%; Precision: ±3%; Resolution ratio: 0.1% | ||
| Air velocity () | Benetech thermal anemometer | Range: 0.001–30 m/s; Precision: ±2%; Resolution ratio: 0.001 m/s |
| Globe temperature () | RS-HQ globe temperature recorder | Range: −20–60 °C; Precision: ±0.2 °C; Resolution ratio: 0.1 °C |
| Skin temperature () | Ibutton temperature recorder | Range: −40–85 °C; Precision: ±0.5 °C; Resolution ratio: 0.0625 °C |
| No. | Parameter | (°C) | (%) | (m/s) | (°C) | (°C) | (%) |
|---|---|---|---|---|---|---|---|
| No. 1 nursing home | Mean | 20.6 | 25.5 | 0.02 | 20.3 | 0 | 57.2 |
| Max | 23 | 33.4 | 0.11 | 22.9 | 5.6 | 67.7 | |
| Min | 18.3 | 19.5 | 0 | 18.2 | −3.5 | 49.6 | |
| SD | 0.7 | 2.1 | 0.01 | 0.6 | 1.9 | 4.6 | |
| No. 2 nursing home | Mean | 17.9 | 29.4 | 0.03 | 18.2 | 0.8 | 55.4 |
| Max | 19.3 | 38.7 | 0.13 | 19.9 | 6.2 | 70.1 | |
| Min | 16.1 | 20.9 | 0.01 | 16.1 | −4.5 | 41.8 | |
| SD | 0.6 | 2.9 | 0.02 | 0.8 | 2.1 | 6.8 | |
| No. 3 nursing home | Mean | 21.3 | 28.5 | 0.04 | 21 | 2.9 | 49.4 |
| Max | 26.5 | 33.2 | 0.14 | 25.9 | 7.6 | 67.5 | |
| Min | 19.7 | 21.3 | 0.02 | 19.6 | −2.9 | 37.8 | |
| SD | 1.3 | 1.6 | 0.03 | 1.2 | 2.3 | 7.1 | |
| No. 4 nursing home | Mean | 20.1 | 29.8 | 0.03 | 20.1 | 1.2 | 53.4 |
| Max | 24.2 | 42.3 | 0.12 | 23.8 | 6.1 | 68.2 | |
| Min | 18.3 | 26.6 | 0.01 | 18 | −6.9 | 42 | |
| SD | 1.2 | 2.8 | 0.01 | 1.1 | 2.4 | 5.9 | |
| No. 5 nursing home | Mean | 22.3 | 25 | 0.03 | 22 | 0.9 | 48.2 |
| Max | 24.9 | 32 | 0.14 | 24.6 | 6.7 | 65.8 | |
| Min | 20.7 | 18.4 | 0.01 | 20.8 | −5.3 | 40.8 | |
| SD | 0.8 | 2.1 | 0.01 | 0.6 | 2.2 | 6.1 | |
| No. 6 nursing home | Mean | 21.5 | 28.4 | 0.02 | 21 | 1.1 | 55.3 |
| Max | 22.9 | 35.6 | 0.11 | 22.9 | 6.8 | 67.9 | |
| Min | 20.1 | 20.4 | 0.01 | 19.8 | −4.6 | 42.6 | |
| SD | 0.5 | 2.2 | 0.01 | 0.6 | 2.2 | 5.1 |
| Chi-Square Test | Value | df | Asymptotic Significance (2-Sided) |
|---|---|---|---|
| Pearson chi-square | 25.417 a | 6 | 0 |
| Likelihood ratio | 25.735 | 6 | 0 |
| Linear-by-linear association | 22.49 | 1 | 0 |
| No. of valid cases | 954 | - | - |
| Type | M (met) | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Max | Min | Mean | SD | Max | Min | |
| Elderly | 1.25 | 0.17 | 1.66 | 0.9 | 1.09 | 0.32 | 2 | 0.8 |
| Adults | 1.1 | 0.15 | 1.62 | 0.85 | 1.48 | 0.36 | 2 | 0.8 |
| Reference | Location | No. of Samples and Age Range | Thermal Comfort Regression Model | Neutral Temperature |
|---|---|---|---|---|
| Jiao Y. et al. [50] | Shanghai, China | 1040, 70–95 | MTS = 0.076 − 1.273 | 16.8 °C |
| Zheng W. et al. [51] | Xi’an, China | 834, 60–96 | TSV = 0.068 − 1.312 | 19.4 °C |
| Li H. et al. [40] | Inner Mongolia Province, China | 216, 60–93 | MTS = 0.169 − 3.461 | 20.52 °C |
| Liu X. et al. [52] | Taiyuan, China | 120, 60–90+ | MTS = 0.471 − 10.575 | 22.4 °C |
| Tao Y. et al. [53] | Hong Kong, China | 181, 65–85 | TSV = 0.79 − 17.844 | 22.6 °C |
| Hwang et al. [36] | Taiwan, China | 87, 60–82 | MTS = 0.28 − 6.5 | 23.2 °C |
| Tatsuki K. et al. [45] | Japan | 66, 69–96 | TSV = 0.04 − 0.95 | 23.8 °C |
| Forcada N. et al. [55] | Spain | 1482 elderly and 439 non-elderly | - | Elderly: 22.7 °C Non-elderly: 21.8 °C |
| Tartarini F. et al. [37,54] | Australia | 322 elderly (65+) and 187 non-elderly (<65) | Elderly: not obtained Non-elderly: TSV = 0.23−4.88 | Elderly: not obtained Non-elderly: 21.2 °C |
| Parameter | Value | Parameter | Value |
|---|---|---|---|
| Area | 2 | External wall heat transfer coefficient | 0.45 W/·K |
| Depth-to-width ratio | 2.1 | External window heat transfer coefficient | 2.0 W/·K |
| Height | 3.2 | Occupant density | 0.06 people/ |
| Window-to-wall ratio | 0.32 | Lighting power | 3 W/ |
| Window height | 1.8 | Equipment power | 7 W/ |
| Elderly | Adults | |||||
|---|---|---|---|---|---|---|
| Heating set temperature | Lower limit of range: 19.4 °C | Neutral temperature: 21.7 °C | Upper limit of range: 24.0 °C | Lower limit of range: 18.6 °C | Neutral temperature: 20.5°C | Upper limit of range: 22.5 °C |
| Energy consumption (kWh/) | 15.6 | 20.8 | 26.4 | 13.9 | 18.1 | 22.7 |
| Carbon emissions (kg/) | 5 | 6.7 | 8.4 | 4.4 | 5.8 | 7.3 |
| Heating Set Temperature | Room |
|---|---|
| The lower limit of the elderly comfort temperature range: 19.4 °C | Elderly rooms, activity rooms, dining halls, etc. |
| The lower limit of the adult comfort temperature range: 18.6 °C | Offices, workrooms, medical rooms, etc. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sun, N.; Ding, X.; Bi, J.; Cui, Y. Field Study on Winter Thermal Comfort of Occupants of Nursing Homes in Shandong Province, China. Buildings 2024, 14, 2881. https://doi.org/10.3390/buildings14092881
Sun N, Ding X, Bi J, Cui Y. Field Study on Winter Thermal Comfort of Occupants of Nursing Homes in Shandong Province, China. Buildings. 2024; 14(9):2881. https://doi.org/10.3390/buildings14092881
Chicago/Turabian StyleSun, Ninghan, Xin Ding, Jialin Bi, and Yanqiu Cui. 2024. "Field Study on Winter Thermal Comfort of Occupants of Nursing Homes in Shandong Province, China" Buildings 14, no. 9: 2881. https://doi.org/10.3390/buildings14092881