1. Introduction
Hospitals represent one of the most complex building types combining several functions operating 24/7—emergency rooms, operating rooms, divisions, long and short stay rooms, laboratories, etc., and, of course, different bedroom typologies. The interaction between the functions as well as a wide network of technological systems strongly contribute to increase this complexity which influences the ageing of the building at different levels: On the one hand, services and equipments are strictly necessary to keep adequate service level and indoor comfort conditions, but the adopted technologies often update very quickly and require constant maintenance and replacement; on the other hand, the progresses in the medical field impact on the space use and arrangement requiring some transformation and adaptations without which the hosted activities can be totally interrupted.
Thus, retrofitting hospitals is a very challenging action especially when delivered in historic buildings that were adapted during their lifespan to new standards, equipment, and functions dealing with medical objectives and also with energy savings issues. In many cases, the renovation action regards the service network and particularly Heating Ventilation and Air-Conditioning (HVAC) and the toilets cells, but it sometimes involves an extensive rehabilitation of the building that aims to improve its general quality and energy efficiency according to EU Energy Building Performance Directives.
Among the several research fields with which hospitals can be associated, there are three specific issues of great interest that are connected with the architectural sector:
Energy: The huge amount of energy demand (heating, cooling, operating, etc.) and the related management requires effective monitoring and audit strategies to define use profiles and to drive adequate retrofitting measures;
Environmental, pollution and thermal comfort: It is assumed that the environmental quality and comfort of operating and other key rooms must meet optimal service level;
Management: The scheduling and organization of retrofitting actions have to ensure the continuity of services with relation to use while taking into account the building site conditions.
Energy savings measures are widely researched in the scientific literature and, with relation to hospitals, Hirest’s [
1] pioneering studies, evidencing that “hospitals are the most energy-intensive building in the commercial sector”, are of particular interest and relevance. Assuming most of energy demand depends on heating and cooling [
2], a study by Fifield et al. [
3] compares the energy efficiency of several options dealing with the typical modularity of the hospital typology. A key related reflection is that energy costs are embedded in the general budget provided by the National Health Service when hospitals operate under the public umbrella and in the general budget as well in the case of the private sector, thus high energy costs mean a reduction of the budget availability for medical and health purposes.
Energy retrofitting is consequently aimed at both reducing energy demand and increasing available resources for health services while maintaining or improving the quality of indoor conditions referred to thermal comfort, pollution level, usability, healthiness. As described by Ascione et al. [
4,
5] retrofitting actions may be addressed to better insulate the building envelope or to improve/replace HVAC system according to a cost-optimization strategy. A consistent number of studies regarding indoor thermal condition in operating rooms and related use of HVAC system [
6] [
7,
8] as well as researches on patients’ perception of indoor thermal comfort [
9,
10,
11,
12,
13] are largely available in the scientific literature. An interesting study from Derks et al. [
14] focuses instead on the hospital nurse personnel perception of indoor thermal comfort while Narollahi [
15] reports a more general and useful literature review about thermal comfort in hospitals. The World Health Organization (WHO) provides a shared and accepted definition of Health and thermal comfort [
16]. About energy consumption, Garci-Sanz-Calced and Gomez-Ghaparro [
17,
18] describe a quantitative analysis of final energy and of the role of maintenance management in hospitals in Spain.
The related issue concerning Indoor Air Quality (IAQ) concerns two main research branches: (a) the detection, measuring and prediction of potential pollutant sources from patients, equipment, and hospital personnel [
19,
20]; (b) HVAC systems architecture and functions with reference to the capacity of treating and controlling indoor air quality in operating rooms, surgeries, and other key divisions [
21]. On this topic, Mendez [
22] highlighted the importance of studying dust and pollutant distribution using computational fluid-dynamics (CFD).
This paper reports the methodology and the outcomes of a study run on an existing hospital undergoing a deep retrofitting with the purpose of optimizing actions and supporting the decision making process, considering the constraints related to limiting the disruption for end-users and patients, maintaining the services active, and proceeding with separate interventions according to a step by step strategy. The general approach is to analyze the technological obsolescence of the building influencing the energy demand and comfort condition levels in order to compare the starting position with the expected one after renovation and measure the improvements while defining priorities to bridge the current gaps. The conventional renovation strategy operates by insulating the building envelope, working on the roof and the façades from the outside to reduce the interaction with the hospital’s everyday activities; however, in the specific case, it is not possible to alter the façades because they are listed by the preservation agency. Furthermore, the huge surface involved suggests dividing the works into sectors according to dedicated budget tranches.
2. Aim of Research
The study is aimed to explore a feasible solution to optimize the results while ensuring a general coherency to the whole retrofitting process under one vision umbrella. In order to speed up the process, the general layout of the whole building is divided into sectors (corresponding to the main wings of the volume) and levels (corresponding to the floors). The scope is to identify the most typical operative conditions that recur in the whole building. The very specific functions such as surgery rooms or technical rooms were excluded and—considering a total coverage of 70%—the conventional bedroom of the bed wards was definitely selected as typical room to be assumed as basic unit to be parametrically replicated for modeling purposes. This way, a good level of detail in analyzing the renovation options can be achieved, and then, it can be projected very quickly on the whole building. It is assumed and agreed with the building manager that the rooms with very specific functions require dedicated interventions. This choice allows that the impacts on the whole building be planned, modified, and finally achieved according to a scheduled sequence of works sector by sector. The scope of the study is to provide effective tools to drive the assessment of retrofitting options of the hospital divisions with the purpose of improving indoor comfort and energy savings, operating interventions sector by sector according to a strategy tuned on a basic building unit.
A model of the basic bedroom in its current status was modeled to be later compared with some retrofitting options analyzing the deriving outcomes. This approach allows to easily replicate and scale the process on the building as a whole, defining some retrofitting scenarios that can be compared according to shared premises and parameters. The basic bedroom unit is defined by recurring elements such as structural features, size, window geometry and characteristics, services and equipment that are assumed as attributes, which are replicated in each floor of each wing of each sector. The HVAC system is instead referred to each sector. The request from the hospital administration was to focus on the building characteristics and particularly the building envelope; therefore, it was decided not to include the HVAC update as investigation parameter. The same goes for the artificial lighting, electrical power, elevators, and all the installations, which are of course part of the renovation plan but are assumed as constants for the purpose of this study.
Consequently, supported by the above-mentioned scientific literature and following the ISO 13790 standards, the research boundaries excluded the study of air quality and HVAC in the considered scenarios. They simply belong to a different decision-making branch dealing with quality of healthcare and cleaning management.
The adopted methodological approach is thought to assess the impacts on the whole system, while varying a limited number of parameters (keeping other factors as constants) in its typical basic unit, and to calibrate the optimal energy saving option and indoor comfort with a limited time and resource investment.
3. Case Study
The research is applied to a specific case study: the S.Orsola-Malpighi polyclinic hospital in Bologna (
Figure 1), in the north of Italy (
Figure 2). Following a traditional model dating back to the early 1900, this hospital is organized in several pavilions (each of them is dedicated to a specific medical division/department) placed in a large plot embedded in the city, quite close to the historic center. In 2015, the hospital management unit launched a general renovation plan aimed to improve the functional and energy performances of the complex as a whole, foreseeing the retrofitting of several pavilions and the replacement of others with new, highly-efficient buildings. In addition, a tri-generation plant was installed to serve all the site and almost cover its usual energy demand. The brief coming from the hospital management unit was to provide effective strategies to support the retrofitting actions, particularly as the pavilion (or a part of it) is a building listed by the preservation agency. This particular condition represents a very challenging task which is still to be explored in the scientific literature concerning the hospital typology.
The study focuses on Pavilion 4 (obstetric and gynecologic division) which was erected in 1934 according to a neoclassic design (and this is the reason why it is partially listed and its façades cannot be altered) and then extended in 1997, adding a new wing (that is not included in the study) for hosting the principal surgery unit of the division. The main constructive features of the building can be listed as structural bearing clay masonry 42 cm thick (Uav = 0.98 W/m2K), composite concrete floor slabs (Uav = 1.43 W/m2K), and double-glazed timber framed window (Uav = 2.20 W/m2K).
According to the brief, the retrofitting options have to comply with the following requisites:
- (a)
Do not interrupt the activities hosted in the pavilion;
- (b)
Reduce the disruption for the end users at the minimum planning a rotation of the beds during the work phases;
- (c)
Meet the budget constraints according to schedule.
Following the described methodological approach, a typical bedroom (for the scope of the study the administration allowed to use room n° 15 at the first floor as test room) was selected as basic unit. The room (
Figure 3a,b) has a surface of 36 m
2, with a window of 1.2 × 1.5, without en suite bathroom (not fulfilling the current national rules) and is now used to host three patients. It is south facing, but orientation of the rooms varies according to the H shaped geometry of the building without any structured device for natural light control. Bedroom capacity varies from two to four people depending on the room geometry and original partitions. The goal of the administration is to standardize the bedrooms for hosting three people, completely updating the installations and including en suite bathrooms to totally comply with national standards and remarkably improve the offer quality. A blind system is required for daylight control purpose in order to avoid orientation may affect the perceived comfort quality of the room. All these elements are assumed as constant in the design brief and are not the objective of the specific study.
Once the starting conditions were carefully analyzed it was agreed that new bedrooms are obtained merging two adjacent rooms (in the test room n° 14 and n° 15).
Figure 4 provides the final proposed layout of the new typical bedroom. The total number of bedrooms will be balanced by moving other functions in the middle of the ward or in the central body of the building.
Some basic renovation actions include partition and existing services removal, cleaning, and preparation for installing the new partitions (dry system based) and services distribution, bathroom unit integration, etc. The specific retrofitting actions that are assumed as key variables by the study deals with:
Insulation of the external walls creating a new inner drywall 13.5 cm thick including a rockwool insulation layer (λ = 0.038 W/mK);
Replacement of the existing window with a more performing PVC ones (Uw = 1.2 W/m2K)
The costs per each single unit room are estimated to be €23,000, excepting integration of new services and equipments (lighting, safety sensors, HVAC unit) and creation of a suspended plasterboard acoustic insulation on ceiling.
4. Research Method
The research methodology includes two parallel actions: On the one hand, the basic unit is modeled and monitored to analyze its indoor thermal comfort; on the other, the energy performance level of the whole building is calculated according to the simulated scenarios, comparing also related time and costs. The very first phase was the existing room model calibration: Once the basic unit has been modeled, the model was validated comparing the outcomes with the data provided by a sensor located in room 15 (test room) in order to obtain the original indoor microclimate and operative temperature. Then, during the second phase, an energy saving simulation was conducted comparing the improvements coming from each renovation scenario on the whole building with the starting position. The third phase was addressed to optimizing the room comfort improvement coherently with the outcomes of the best energy-saving scenario and to calculate the deriving operative temperature.
4.1. Building Energy Performance Improvement (Energy Retrofitting Scenarios)
The energy performance of the building was calculated according to Directive 2010/31/UE (Energy Building Performance Directive) and correlate CEN Umbrella and EN ISO 13790 standards, as resume in Italian standards UNITS 11300 [
23]. Calculations were performed on the building as a whole at is original condition (starting position) considering its constructive and technical characteristics, its volume and surface, services typology, and climatic data of the site. Only thermo-physics parameters (conductivity and transmittance) are reported because they have a direct impact on energy saving so technological solution should be change or adapted, following hospital management decision, without any effect on energy efficiency results (it was agreed to keep them constant in the study).
The main retrofitting actions are (step by step):
- (a)
Roof insulation with a rock wool (λ = 0.036 W/mK) layer;
- (b)
Replacement of the existing windows with high performing PVC ones (Uw = 1.2 W/m2K);
- (c)
Insulation of the external walls creating a new inner drywall 13.5 cm thick including a rockwool insulation layer (λ = 0.038 W/mK);
- (d)
Integration of new services and equipment including CMV and replacement of existing radiator with fan coils, to reduce building energy need for heating/cooling by natural ventilation.
Retrofitting actions are simulated according to three scenarios, corresponding to different renovation intensities and expected savings:
Scenario 1: Only roof insulation (a) is considered and the works do not create any impact on the pavilion activities and patients stay;
Scenario 2: Roof insulation (a) is combined with façade insulation (c) and window replacement (b) in order to obtain an extensive improvement of the building envelope as a whole (a + b + c). Works require to rotate patients in the beds sector by sector altering the usual pavilion activity;
Scenario 3: A new CMV (d) is added to scenario 2 (a + b + c + d) requiring patients to be relocated to a different sector while works are completed.
Time and costs increase from scenarios 1 to 3 as well as the achieved energy savings and indoor comfort improvements.
Figure 5 reports and compares intervention costs, yearly cost savings, Simple Pay Back value, works duration, impacts and energy performance level associated to each scenario. The Simple Pay Back (SPB) values following standard EN 15459-1 [
24] with an inflation rate of 3% that includes the energy inflation rate and discount rate 1.5%. Cost of materials following price list by Chamber of Commerce of Bologna and energy cost by ARERA the Italian Regulatory Authority for Energy, Networks and Environment.
4.2. Indoor Thermal Comfort and Model Calibration
With reference to the assessment of basic unit room indoor thermal comfort, the starting conditions of room 15 (test room) were modeled as a benchmark, and then, the renovated room design was modeled to analyze the improvements (taking into account some differences occurred due to the different geometry and feature derived by the functional renovation). The two conditions were compared by (a) in-situ monitoring of the microclimate indoor [air temperature (°C), relative humidity (%), air speed (m/s) and by (b) energy plus [
25] modeling using OpenStudio interface (
http://nrel.github.io/OpenStudio-user-documentation/) [
26,
27].
Monitoring took place on 24 November 2017 from 10 to 13 using a microclimatic station HD 32.2 Microclima WBGT-PMV-PPD Index produced by DeltaOHM. The device had a limited size (28 × 4.5 × 4 cm), it was almost noiseless, and stood on a tripod at 1 m height. Indoor air temperature (°C, Pt100 accuracy: ±0.1 °C), relative humidity (accuracy: ±2%), and air speed (m/s) were monitored in the test room. The device was located on a table next to the door (h = 100 cm). Acquired data were stored in a memory card and then elaborated with other software and drivers. In the specific case, the sensor detected 758 measurers on intervals of 15 s.
Permission to put the datalogger in the room with the patients was given by the hospital administration for a very limited period of time to not disturb their stay (and it asked to exactly explain the purpose and the modalities of monitoring to them). Thus, it was agreed the measuring for model validation purposes would take place on 24 November for no more than 3 h. The acquired data are reliable enough for the scope of the study which is definitely a speed and parametric evaluation approach.
The model has been calibrated comparing the data acquired with ASHRAE Guideline 14 [
28,
29] range.
Figure 6 describes the regression line R
2 and
Table 1 reports the outcomes of model calibration: in the first column, statistical index denomination; the second column reports the reference values following ASHRAE Guideline 14 range, and the third column reports result values from comparison between model results and on-site monitoring data. The results show that, despite the reduced time interval, the model is validated for the purpose of comparing the proposed retrofitting scenarios.
Starting from the basic model the Scenario 3 improvements have been added including the new rock wool insulation layer (13.5 cm thick with λ = 0.038 W/mK) and window replacement with PVC profiles (Uw = 1.2 W/m2K).
5. Results and Discussion
In this section, the results concerning energy savings and thermal comfort are separately discussed.
5.1. Energy Saving Results
Table 2 evidences that, despite the limited investment and the relative fast intervention, scenario 1 produces very limited impacts on energy performance level (EP index) and energy savings. Scenarios 2 and 3 are more expensive and time consuming but ensure relevant improvements. Scenario 3 leads Ep index to less than 1/7 of the original one with very high yearly energy savings. Much more important, in terms of appeal for the hospital management unit, its payback time requires only 3 additional years to the 9 of scenario 1. With a cost increase around 8% compared to scenario 2, scenario 3 allows to reduce the EP index of 75% representing the most convenient and effective combination of retrofitting actions.
5.2. Indoor Microclimate Improvement
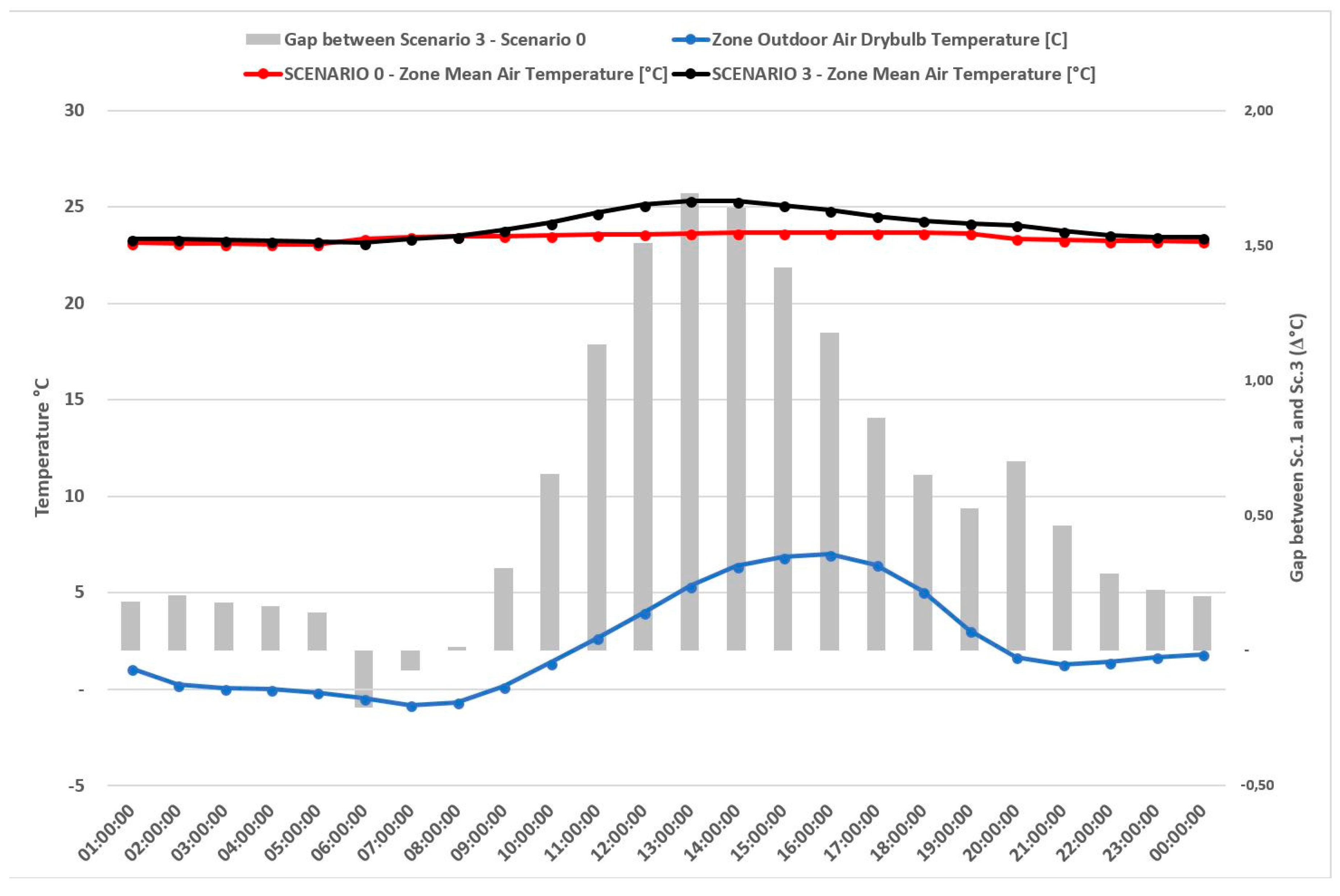
The validated model (par 4.2) of the starting position allows to compare the scenarios microclimate and particularly the one of scenario 3 which is assumed as the optimal configuration. Indoor microclimate is analyzed focusing on operative temperature (°C) trends during a typical day of the winter period.
The graph, in
Figure 7, shows the effects that retrofitting actions of scenario 3 would produce if completed. It can be noticed that, assuming the heating system as a constant, in scenario 3 operative temperature is increased by +1.5 °C during the central hours of the day compared to starting position (scenario 0). It has to be remembered that set-point temperature in hospitals is 22 °C ± 2 °C. Furthermore, looking at the outdoor temperature trends, it can be argued that this increase is not simply influenced by possible solar gain but it takes also into account possible internal gain.
Despite some limitations assumed by the simulations, the adopted methodology allows to achieve a quite reliable estimation of the retrofitting impacts, keeping an eye on both the energy savings and the thermal comfort, without modeling the whole building in detail. The parametric evaluation based on the typical unit room is flexible enough to accept some adjustment and refine the process during the design phase and is not heavily time and resource consuming, effectively supporting the decision-making process of the hospital administration and management office.
6. Conclusions
This study was aimed to demonstrate the effectiveness of the methodological approach based on a parametric evaluation that, starting from the typical unit room, is scaled to the whole building, reducing time and resources required to support the decision making and the design phase, supporting retrofitting process of existing buildings in the hospital sector. The parametric approach was chosen according to the initial brief of the hospital administration and took carefully into account the constraints and limits of the existing building at its starting conditions. Once an architectural basic unit is defined (the basic hospital bedroom in this specific case), it can be parametrically replicated to cover the whole building to calculate the global energy performances and estimate the total costs of interventions. This approach can be easily transferred to other sectors and building typologies where a basic architectural and replicable unit can be found.
Several solutions can be explored according to different retrofitting scenarios that keep the thermal indoor comfort of the most convenient and effective energy saving measures as a marker of the design solution quality, assuming that, in hospital typology, optimal indoor comfort conditions cannot be simply associated with the set-point values.
Past research experiences of the research team, involving public administration and wider interest groups [
30], demonstrated that technical information and data must be adequately and easily communicated and the different options visually compared because the numerical data are not always completely understood by decision makers and final users. The most relevant barriers to the application of parametric methodology are related to the need to consider non-technical priorities: budget availabilities, intervention schedule, etc.; and all elements require that the methodology be flexible, especially during the phase in which scenarios are compared, and that some simplified graphs or visualization concerning the different options be provided to simplify the output to nontechnical people during the decision making process. The proposed methodology ensures choosing within a easy to understand framework that usually makes the process fluid and shared with most of the involved subjects.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}