
Using Modern Contraception While Wanting a Child: What Does Contraceptive Over-Use Mean for the Human Rights-Based Approach in Burkina Faso? Insights from PMA2020 Data


Abstract
1. Introduction
2. Materials and Methods
2.1. Data
2.2. Variables
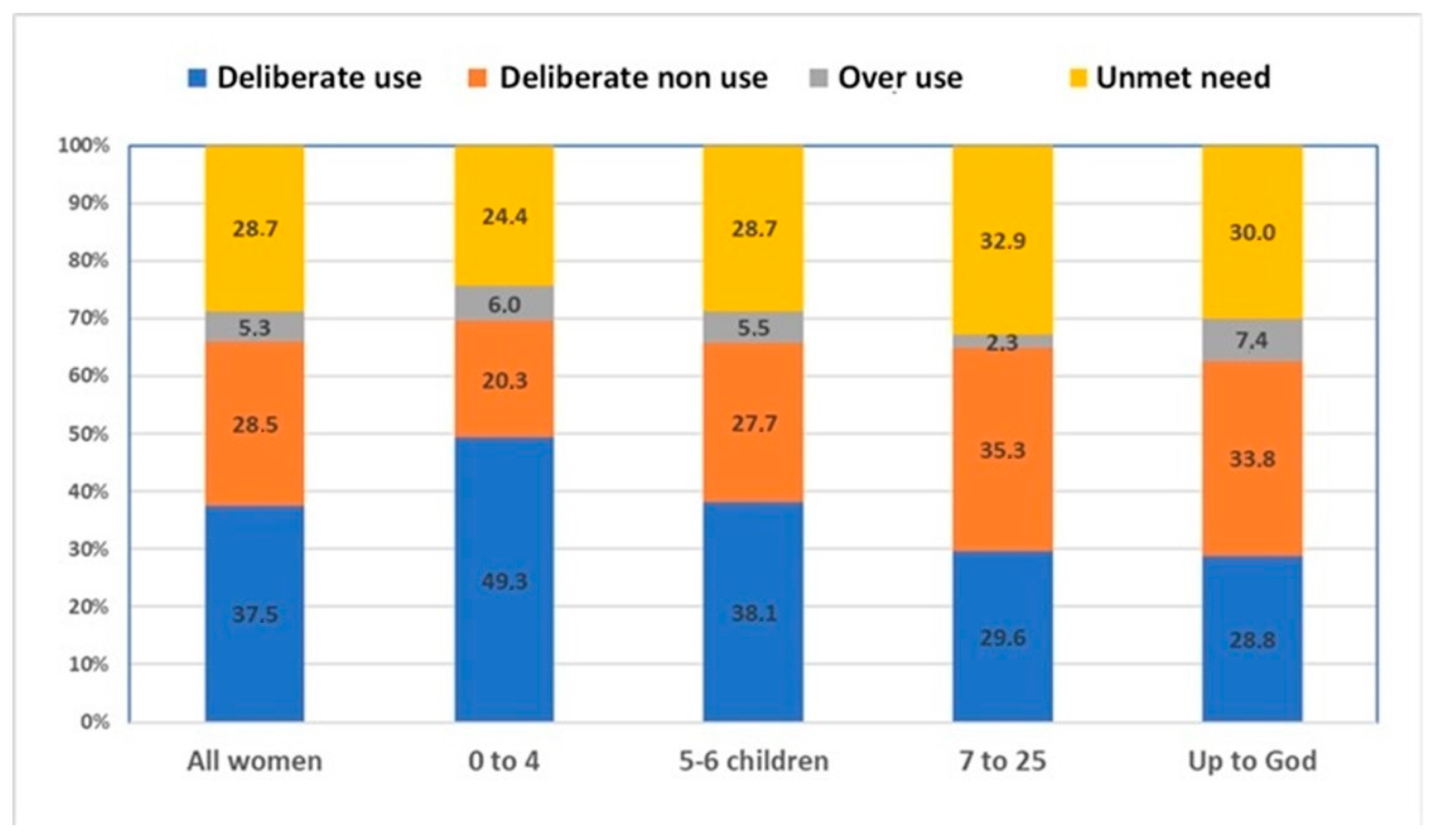
- Deliberate use: women who do not want another child or wish to postpone pregnancy for more than 12 months and are using modern contraception;
- Deliberate non-use: women who want another child within 12 months and are not using modern contraception;
- Overuse: women who want another child within 12 months but are using modern contraception;
- Unmet need: women who do not want another child or want to postpone childbearing for more than 12 months but are not using modern contraceptives.
2.3. Analyses
3. Results
3.1. Sample Distribution and Prevalence of Overuse by Women’s Characteristics
3.2. Factors Associated with the Overuse of a Modern Contraceptive
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bendix, Daniel, Ellen E. Foley, Anne Hendrixson, and Susanne Schultz. 2020. Targets and technologies: Sayana Press and Jadelle in contemporary population policies. Gender, Place & Culture 27: 351–69. [Google Scholar]
- Berelson, Bernard. 1969. Beyond family planning. Studies in Family Planning 1: 1–16. [Google Scholar] [CrossRef]
- Boydell, Victoria Jane. 2010. The Social Life of the Pill: An Ethnography of Contraceptive Pill Users in a Central London Family Planning Clinic. London: London School of Economics and Political Science (United Kingdom). [Google Scholar]
- Bradley, Sarah E.K., and John B. Casterline. 2014. Understanding unmet need: History, theory, and measurement. Studies in Family Planning 45: 123–50. [Google Scholar] [CrossRef] [PubMed]
- Bradley, Sarah E.K., Trevor N. Croft, Joy D. Fishel, and Charles F. Westoff. 2012. Revising Unmet Need for Family Planning. Calverton: ICF. [Google Scholar]
- Casterline, John B., A. E. Perez, and A. E. Biddlecom. 1997. Factors underlying unmet need for family planning in the Philippines. Studies in Family Planning 28: 173–91. [Google Scholar] [CrossRef]
- Casterline, John B., and Laila O. El-Zeini. 2007. The estimation of unwanted fertility. Demography 44: 729–45. [Google Scholar] [CrossRef] [PubMed]
- Chiappero-Martinetti, Enrica, and Sridhar Venkatapuram. 2014. The capability approach: A framework for population studies. African Population Studies 28: 708–20. [Google Scholar] [CrossRef]
- Cleland, John, Sarah Harbison, and Iqbal H. Shah. 2014. Unmet Need for Contraception: Issues and Challenges. Studies in Family Planning 45: 105–22. [Google Scholar] [CrossRef]
- Drabo, Seydou. 2020. Beyond ‘family planning’—Local realities on contraception and abortion in Ouagadougou, Burkina Faso. Social Sciences 9: 212. [Google Scholar] [CrossRef]
- Gastineau, Bénédicte, Lina Rakotoson, and Frédérique Andriamaro. 2016. L’indicateur des Objectifs du Millénaire pour le développement. Mondes en Développement 2: 79–93. [Google Scholar] [CrossRef]
- Gnoth, C., D. Godehardt, E. Godehardt, P. Frank-Herrmann, and G. Freundl. 2003. Time to pregnancy: Results of the German prospective study and impact on the management of infertility. Human Reproduction 18: 1959–66. [Google Scholar] [CrossRef]
- Grace, Karen Trister, and Violence Jocelyn C. Anderson. 2018. Reproductive coercion: A systematic review. Trauma, & Abuse 19: 371–90. [Google Scholar]
- Grubb, Laura K., Rebecca M. Beyda, Mona A. Eissa, and Laura J. Benjamins. 2018. A contraception quality improvement initiative with detained young women: Counseling, initiation, and utilization. Journal of Pediatric and Adolescent Gynecology 31: 405–10. [Google Scholar] [CrossRef] [PubMed]
- Howett, Rebecca, Alida M. Gertz, Tiroyaone Kgaswanyane, Gregory Petro, Lesego Mokganya, Sifelani Malima, Tshego Maotwe, Melanie Pleaner, and Chelsea Morroni. 2019. Closing the gap: Ensuring access to and quality of contraceptive implant removal services is essential to rights-based contraceptive care. African Journal of Reproductive Health 23: 19–26. [Google Scholar] [PubMed]
- ICPD. 1994. International Conference on Population and Development-ICPD-Programme of Action. New York: UNFPA. [Google Scholar]
- INSD. 2020. Résultats Préliminaires du 5e RGPH. Available online: http://cns.bf/IMG/pdf/rapport_preliminaire_rgph_2019.pdf (accessed on 5 June 2024).
- Machiyama, Kazuyo, John B. Casterline, Joyce N. Mumah, Fauzia Akhter Huda, Francis Obare, George Odwe, Caroline W. Kabiru, Sharifa Yeasmin, and John Cleland. 2017. Reasons for unmet need for family planning, with attention to the measurement of fertility preferences: Protocol for a multi-site cohort study. Reproductive Health 14: 23. [Google Scholar] [CrossRef]
- Mauldin, W. P. 1965. Fertility studies: Knowledge, attitude, and practice. Studies in Family Planning 1: 1–10. [Google Scholar] [CrossRef]
- McNamee, Paul, Laura Ternent, and Julia Hussein. 2009. Barriers in accessing maternal healthcare: Evidence from low-and middle-income countries. Expert Review of Pharmacoeconomics & Outcomes Research 9: 41–48. [Google Scholar]
- Ministère de la Santé. 2017. Plan National d’Accélération de Planification Familiale du Burkina Faso 2017–2020. Available online: http://www.healthpolicyplus.com/ns/pubs/8212-8375_PNAPF.pdf (accessed on 16 March 2021).
- Moreau, Caroline, Mridula Shankar, Stephane Helleringer, and Stanley Becker. 2019. Measuring unmet need for contraception as a point prevalence. BMJ Global Health 4: e001581. [Google Scholar] [CrossRef]
- Ononokpono, Dorothy Ngozi, Clifford Obby Odimegwu, Eunice Imasiku, and Sunday Adedini. 2013. Contextual determinants of maternal health care service utilization in Nigeria. Women & Health 53: 647–68. [Google Scholar]
- Peytrignet, Marie-Claire. 2019. Fertility Regulation in Sub-Saharan Africa: The Role of Marital Sexual Inactivity. Ph.D. thesis, University of Geneva, Geneva, Switzerland. [Google Scholar]
- PMA2020/BURKINA FASO. 2017. Résumé des Principaux Indicateurs en Planification Familiale Pour la 4ème Vague de Collecte. Baltimore: John Hopkins. [Google Scholar]
- PMA2020/BURKINA FASO. 2019. Key Family Planning Indicators: December 2018—January 2019 (Round 6). Baltimore: John Hopkins. [Google Scholar]
- Raj, Anita, Arnab Dey, Namratha Rao, Jennifer Yore, Lotus McDougal, Nandita Bhan, Jay G. Silverman, Katherine Hay, Edwin E. Thomas, Rebecka Lundgren, and et al. 2024. The EMERGE framework to measure empowerment for health and development. Social Science & Medicine 351: 116879. [Google Scholar]
- RamaRao, Saumya, and Anrudh K. Jain. 2015. Aligning goals, intents, and performance indicators in family planning service delivery. Studies in Family Planning 46: 97–104. [Google Scholar] [CrossRef]
- Robeyns, Ingrid. 2003. Sen’s capability approach and gender inequality: Selecting relevant capabilities. Feminist Economics 9: 61–92. [Google Scholar] [CrossRef]
- Rossier, Clémentine, and Jamaica Corker. 2017. Contemporary Use of Traditional Contraception in sub-Saharan Africa. Population and Development Review 43: 192–215. [Google Scholar] [CrossRef]
- Rossier, Clémentine, Sarah E. Bradley, John Ross, and William Winfrey. 2015. Reassessing unmet need for family planning in the postpartum period. Studies in Family Planning 46: 355–67. [Google Scholar] [CrossRef] [PubMed]
- Sanabria, Emilia. 2016. Plastic Bodies: Sex Hormones and Menstrual Suppression in Brazil. Durham: Duke University Press. [Google Scholar]
- Senderowicz, Leigh. 2019. “I was obligated to accept”: A qualitative exploration of contraceptive coercion. Social Science & Medicine 239: 112531. [Google Scholar]
- Senderowicz, Leigh. 2020. Contraceptive autonomy: Conceptions and measurement of a novel family planning indicator. Studies in Family Planning 51: 161–76. [Google Scholar] [CrossRef] [PubMed]
- Silverman, Jay G., and Anita Raj. 2014. Intimate partner violence and reproductive coercion: Global barriers to women’s reproductive control. PLoS Medicine 11: e1001723. [Google Scholar] [CrossRef] [PubMed]
- Solo, Julie, and Mario Festin. 2019. Provider bias in family planning services: A review of its meaning and manifestations. Global Health: Science and Practice 7: 371–85. [Google Scholar] [CrossRef]
- Speizer, Ilene S. 2006. Using strength of fertility motivations to identify family planning program strategies. International Family Planning Perspectives 32: 185–91. [Google Scholar] [CrossRef]
- Strasser, Julia, Liz Borkowski, Megan Couillard, Amy Allina, and Susan F. Wood. 2017. Access to removal of long-acting reversible contraceptive methods is an essential component of high-quality contraceptive care. Women’s Health Issues 27: 253–55. [Google Scholar] [CrossRef]
- Teixeira, Maria, Nathalie Bajos, and Agnès Guillaume. 2015. l’équipe ECAF. 2015 De la Contraception Hormonale en Afrique de l’Ouest: Effets Secondaires et Usages à la Marge. Paris: Anthropologie du Médicament au Sud. La Pharmaceuticalisation à ses Marges, pp. 181–95. [Google Scholar]
- Timæus, Ian M., and Tom A. Moultrie. 2008. On postponement and birth intervals. Population and Development Review 34: 483–510. [Google Scholar] [CrossRef]
- Westoff, Charles F., and Akinrinola Bankole. 1995. Unmet Need: 1990–1994. Calverton: Macro International. [Google Scholar]
- Wollum, Alexandra, Corrina Moucheraud, Amon Sabasaba, and Jessica D. Gipson. 2024. Removal of long-acting reversible contraceptive methods and quality of care in Dar es Salaam, Tanzania: Client and provider perspectives from a secondary analysis of cross-sectional survey data from a randomized controlled trial. PLOS Global Public Health 4: e0002810. [Google Scholar] [CrossRef] [PubMed]
- Zan, Lonkila Moussa, Clémentine Rossier, and Caroline Moreau. 2024. Zan, Lonkila Moussa, Clémentine Rossier, and Caroline Moreau. 2024. Measuring Cognitive and Psychosocial Accessibility to Modern Contraception: A Comprehensive Framework. Health 16: 578–91. [Google Scholar] [CrossRef]

{kind=link}
| Functioning | |
| Contraceptive behaviors | Deliberate use, Deliberate non-use, Overuse, Unmet needs |
| Capability set | |
| The ability to: | - choose an ideal number of children |
| - decide on another childbearing: “Once you have a first child, you can decide when to have another one?” Responses: 1 = strongly disagree, 2 = disagree, 3 = indifferent/doubtful, 4 = agree, 5 = strongly agree. | |
| - decide on what to do with FP: “You are (would be) able to choose what to do about family planning without considering what your husband/partner tells you to do”. Responses: 1 = strongly disagree, 2 = disagree, 3 = indifferent/doubtful, 4 = agree, 5 = strongly agree. | |
| Endowments/conversion factors | |
| Individual level | Age; Education; Marital status; Number of children; Type of contraceptive (for users); Method decision maker (for users) |
| Household level | - Household wealth tercile - Place of residence |
| Contextual level | Level of family planning acceptance (five questions) - “Do you agree with couples who use a method to avoid a pregnancy?” - “Does your partner/husband agree with couples who use a method to avoid a pregnancy?” - “Do you agree with a man or a woman who use contraception to avoid a pregnancy?” - “Do you agree with a couple who use contraception to try to space the births of their children?” - “Do you agree with a couple who use contraception to try to limit the number of children they will have?” Responses: 1 = strongly disagree, 2 = disagree, 3 = indifferent/doubtful, 4 = agree, 5 = strongly agree. |
| Level of fertility support (five questions) - “Do you agree if a woman still carries a child on her back, she should not get pregnant?” - “Do you agree if your older daughter is pregnant, you should not be pregnant yourself?” - “Do you agree that a woman who uses a method to avoid a pregnancy will not have the number of children God chose for her?” - “Do you agree that using a method to avoid a pregnancy encourages having sex before marriage?” - “Do you agree that using a method to avoid a pregnancy encourages having sex outside of marriage (adultery)?” Responses: 1 = strongly disagree, 2 = disagree, 3 = indifferent/doubtful, 4 = agree, 5 = strongly agree. | |
| Sample Distribution | Proportion of Overuse | ||||
|---|---|---|---|---|---|
| Variables | Categories | Frequencies (n) | Percentages (%) | ||
| Functioning | Contraceptive behavior | Deliberate use | 784 | 37.5 | - |
| Deliberate non-use | 541 | 28.5 | - | ||
| Overuse | 140 | 5.3 | - | ||
| Unmet need | 509 | 28.7 | - | ||
| Capability | Ideal number of children | 0 to 4 | 661 | 26.4 | 6.0 |
| 5 to 6 | 625 | 34.2 | 5.5 | ||
| 7 to 25 | 345 | 21.9 | 2.3 | ||
| Up to God/DNK | 339 | 17.5 | 7.4 | ||
| Can decide when to have another child | Do not agree/doubtful | 636 | 33.3 | 5.5 | |
| Agree/strongly agree | 1338 | 66.7 | 5.1 | ||
| Can decide alone what to do with FP | Do not agree/doubtful | 1490 | 74.8 | 5.2 | |
| Agree/strongly agree | 484 | 25.2 | 5.5 | ||
| Endowment/ Conversion factors | Age group | 15–24 | 677 | 34.5 | 5.9 |
| 25–39 | 1039 | 52.6 | 5.3 | ||
| 40–49 | 258 | 12.9 | 3.4 | ||
| Education | No education | 1055 | 63.8 | 3.8 | |
| Primary | 351 | 16.2 | 5.1 | ||
| Secondary or higher | 568 | 20.0 | 10.0 | ||
| Place of residence | Rural | 1064 | 77.8 | 3.9 | |
| Urban | 910 | 22.2 | 9.9 | ||
| Wealth tercile | Lower | 522 | 36.5 | 3.0 | |
| Middle | 488 | 32.4 | 3.5 | ||
| Higher | 964 | 31.1 | 9.9 | ||
| Number of children | No child | 284 | 11.9 | 6.3 | |
| One to Three | 964 | 44.7 | 6.9 | ||
| Four or more | 726 | 43.4 | 3.3 | ||
| Marital status | Not in union | 329 | 11.9 | 12.2 | |
| In Union | 1645 | 88.1 | 4.3 | ||
| Community-level FP acceptance | Low | 670 | 31.3 | 6.2 | |
| Middle | 648 | 36.0 | 6.1 | ||
| High | 656 | 32.8 | 3.5 | ||
| Community-level of fertility support | Low | 717 | 40.5 | 4.0 | |
| Middle | 619 | 34.5 | 4.6 | ||
| High | 638 | 25.0 | 8.3 | ||
| Total number of women | 1974 | 100.0 | 5.3 | ||
| Women’s Characteristics | OR of Overuse among All Women | OR of Overuse among Users of a Modern Method |
|---|---|---|
| OR [95% CI] (p-Value) | OR [95% CI] (p-Value) | |
| Ideal number of children (Ref = 0–4) | ||
| 5 to 6 | 1.55 [0.9–2.67] (0.111) | 1.59 [0.95–2.66] (0.079) |
| 7 to 25 | 0.82 [0.4–1.68] (0.587) | 0.94 [0.44–2.01] (0.865) |
| Up to God | 2.04 [1.07–3.89] (0.029) | 2.42 [1.24–4.73] (0.01) |
| Can decide on another child (Réf = Disagree) | ||
| Agree | 0.89 [0.54–1.48] (0.665) | 0.9 [0.54–1.49] (0.673) |
| Can decide what to do with FP (Réf = Disagree) | ||
| Agree | 1.13 [0.66–1.95] (0.655) | 0.85 [0.44–1.63] (0.626) |
| Age (Ref = 15–24) | ||
| 25–39 | 1.21 [0.69–2.14] (0.503) | 0.9 [0.46–1.76] (0.761) |
| 40–49 | 0.77 [0.31–1.9] (0.567) | 0.54 [0.19–1.51] (0.239) |
| Education (Ref = No education) | ||
| Primary | 1 [0.5–1.96] (0.991) | 1.07 [0.54–2.12] (0.836) |
| Secondary or higher | 1.47 [0.85–2.53] (0.167) | 1.08 [0.62–1.86] (0.795) |
| Household wealth (Ref = Low tercile) | ||
| Middle | 1.14 [0.52–2.49] (0.742) | 1.11 [0.5–2.45] (0.797) |
| Higher | 2.71 [1.56–4.71] (0) | 2.84 [1.55–5.23] (0.001) |
| Marital status (Ret = Not in union) | ||
| In Union | 0.42 [0.25–0.69] (0.001) | 0.68 [0.38–1.21] (0.19) |
| Community FP * acceptance (Ref = Low) | ||
| Middle | 0.85 [0.5–1.45] (0.558) | 0.64 [0.37–1.13] (0.127) |
| High | 0.67 [0.34–1.31] (0.238) | 0.49 [0.24–1] (0.05) |
| Community-level fertility support (Ref = Low) | ||
| Middle | 1.03 [0.54–1.99] (0.922) | 1.1 [0.57–2.11] (0.775) |
| High | 1.24 [0.73–2.1] (0.418) | 1.16 [0.67–2.01] (0.605) |
| Type of methods (Ref = Short-term) | ||
| Long-acting | 1.43 [0.89–2.29] (0.141) | |
| Decision of FP use (Ref = Self) | ||
| Joint/partner/provider | 0.6 [0.38–0.95] (0.028) | |
| Method information level (Ref: low) | ||
| Middle | 0.49 [0.29–0.83] (0.008) | |
| High | 0.8 [0.46–1.42] (0.448) | |
| N | 1974 | 924 |
| Wald chi2 | 78.3 | 79.62 |
| p-value | 0.000 | 0.000 |
| LR test (compared to the empty model) chi 2 | 54.803 | 60.341 |
| LR test p-value | 0.000 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zan, M.L.; Sauvain-Dugerdil, C.; Rossier, C. Using Modern Contraception While Wanting a Child: What Does Contraceptive Over-Use Mean for the Human Rights-Based Approach in Burkina Faso? Insights from PMA2020 Data. Soc. Sci. 2024, 13, 447. https://doi.org/10.3390/socsci13090447
Zan ML, Sauvain-Dugerdil C, Rossier C. Using Modern Contraception While Wanting a Child: What Does Contraceptive Over-Use Mean for the Human Rights-Based Approach in Burkina Faso? Insights from PMA2020 Data. Social Sciences. 2024; 13(9):447. https://doi.org/10.3390/socsci13090447
Chicago/Turabian StyleZan, Moussa Lonkila, Claudine Sauvain-Dugerdil, and Clémentine Rossier. 2024. "Using Modern Contraception While Wanting a Child: What Does Contraceptive Over-Use Mean for the Human Rights-Based Approach in Burkina Faso? Insights from PMA2020 Data" Social Sciences 13, no. 9: 447. https://doi.org/10.3390/socsci13090447
APA StyleZan, M. L., Sauvain-Dugerdil, C., & Rossier, C. (2024). Using Modern Contraception While Wanting a Child: What Does Contraceptive Over-Use Mean for the Human Rights-Based Approach in Burkina Faso? Insights from PMA2020 Data. Social Sciences, 13(9), 447. https://doi.org/10.3390/socsci13090447