
In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2


 , , ,
, , ,
Abstract
:1. Introduction
2. Method
2.1. Participant Enrollment
2.2. Sample Collection and SARS-CoV-2 Detection
2.3. Statistical Analysis
3. Results
3.1. Sensitivity of Sample Specimens at Diagnosis
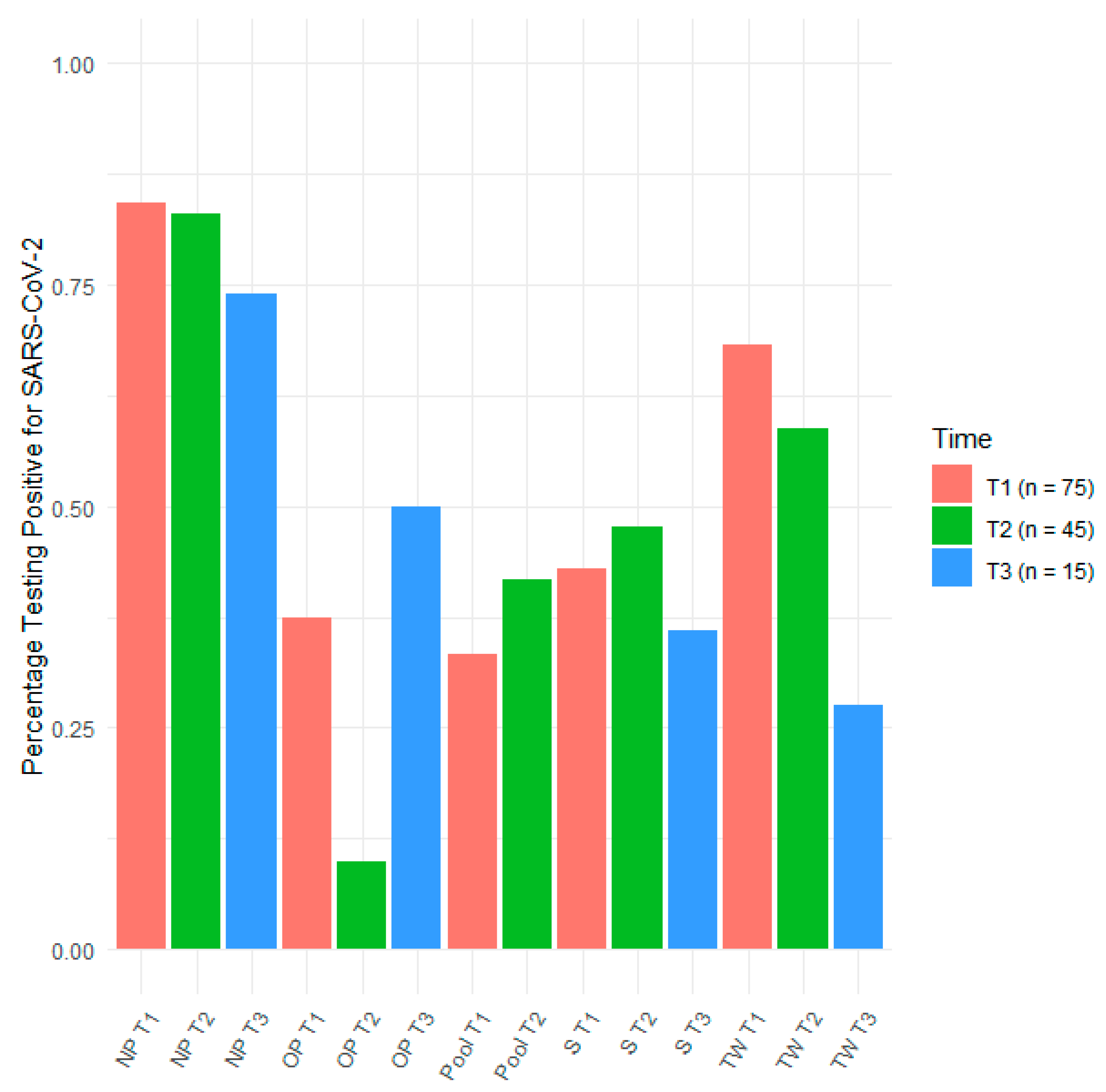
3.2. Sensitivity of Sampling Methods over Time
3.3. Interspecimen Reliability Measurements
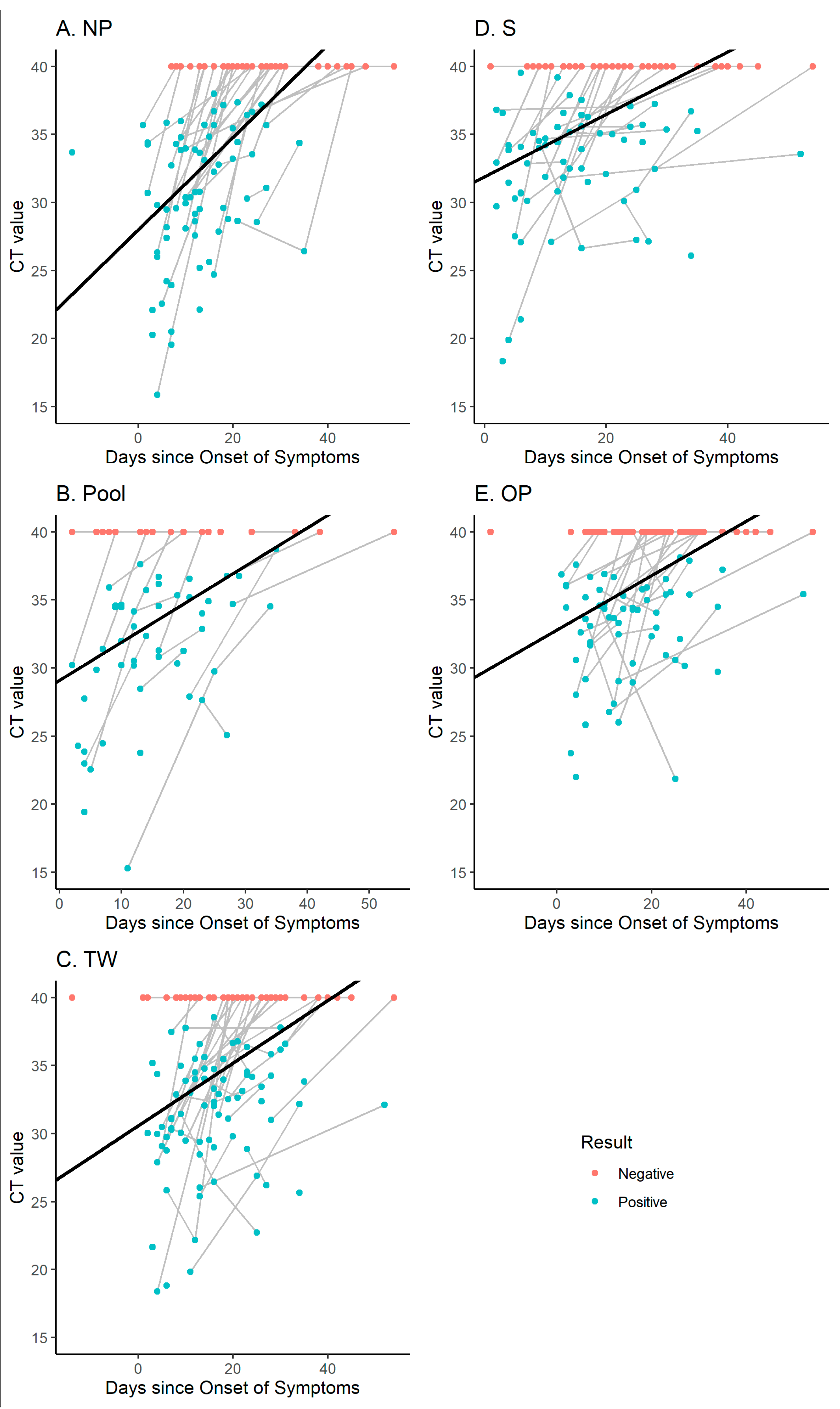
3.4. Correlation between Symptoms and SARS-CoV-2 Detection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fang, F.C.; Benson, C.A.; Del Rio, C.; Edwards, K.M.; Fowler, V.G.; Fredricks, D.N.; Limaye, A.P.; Murray, B.E.; Naggie, S.; Pappas, P.G.; et al. COVID-19-Lessons Learned and Questions Remaining. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, 2225–2240. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, T.; Pigazzini, S.; Degenhardt, F.; Cordioli, M.; Butler-Laporte, G.; Maya-Miles, D.; Bujanda, L.; Bouysran, Y.; Niemi, M.E.; Palom, A.; et al. Age-Dependent Impact of the Major Common Genetic Risk Factor for COVID-19 on Severity and Mortality. J. Clin. Invest. 2021. [Google Scholar] [CrossRef] [PubMed]
- Darcis, G.; Bouquegneau, A.; Maes, N.; Thys, M.; Henket, M.; Labye, F.; Rousseau, A.-F.; Canivet, P.; Desir, C.; Calmes, D.; et al. Long-Term Clinical Follow-up of Patients Suffering from Moderate-to-Severe COVID-19 Infection: A Monocentric Prospective Observational Cohort Study. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 109, 209–216. [Google Scholar] [CrossRef]
- El Moussaoui, M.; Lambert, N.; Maes, N.; Fombellida, K.; Vaira, D.; Moutschen, M.; Darcis, G. Impact of the COVID-19 Pandemic Situation on HIV Care in Liège, Belgium. HIV Res. Clin. Pract. 2021, 22, 63–70. [Google Scholar] [PubMed]
- Blumenthal, D.; Fowler, E.J.; Abrams, M.; Collins, S.R. Covid-19-Implications for the Health Care System. N. Engl. J. Med. 2020, 383, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Darcis, G.; Vaira, D.; Moutschen, M. Impact of Coronavirus Pandemic and Containment Measures on HIV Diagnosis. Epidemiol. Infect. 2020, 148, e185. [Google Scholar] [CrossRef] [PubMed]
- Mak, G.C.K.; Lau, S.S.Y.; Wong, K.K.Y.; Chow, N.L.S.; Lau, C.S.; Lam, E.T.K.; Chan, R.C.W.; Tsang, D.N.C. Evaluation of Rapid Antigen Detection Kit from the WHO Emergency Use List for Detecting SARS-CoV-2. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2020, 134, 104712. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.R.; Savage, T.J.; Wardell, H.; Lee, R.A.; Mathew, A.; Stengelin, M.; Sigal, G.B. Correlation of SARS-CoV-2 Nucleocapsid Antigen and RNA Concentrations in Nasopharyngeal Samples from Children and Adults Using an Ultrasensitive and Quantitative Antigen Assay. J. Clin. Microbiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Wyllie, A.L.; Fournier, J.; Casanovas-Massana, A.; Campbell, M.; Tokuyama, M.; Vijayakumar, P.; Warren, J.L.; Geng, B.; Muenker, M.C.; Moore, A.J.; et al. Saliva or Nasopharyngeal Swab Specimens for Detection of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.-L.; Jiang, Q.; Ye, F.; Li, S.-Q.; Hong, C.; Chen, L.-Y.; Li, S.-Y. Effect of Throat Washings on Detection of 2019 Novel Coronavirus. Clin. Infect. Dis. 2020, 71, 1980–1981. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.; Bond, K.; Zhang, B.; Putland, M.; Williamson, D.A. Saliva as a Noninvasive Specimen for Detection of SARS-CoV-2. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mina, M.J.; Parker, R.; Larremore, D.B. Rethinking Covid-19 Test Sensitivity-A Strategy for Containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef] [PubMed]
- Darcis, G.; Meuris, C.; Kremer, C.; Faes, C.; Hens, N. The Risk of Underestimating the Contribution of Children to SARS-CoV-2 Pandemic. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021. [Google Scholar] [CrossRef] [PubMed]
- Meuris, C.; Kremer, C.; Geerinck, A.; Locquet, M.; Bruyère, O.; Defêche, J.; Meex, C.; Hayette, M.-P.; Duchene, L.; Dellot, P.; et al. Transmission of SARS-CoV-2 After COVID-19 Screening and Mitigation Measures for Primary School Children Attending School in Liège, Belgium. JAMA Netw. Open. 2021, 4, e2128757. [Google Scholar] [CrossRef] [PubMed]
- ORACOL-Malvern Medical Developments Ltd. Available online: https://www.malmed-oracol.co.uk (accessed on 22 December 2020).
- Wang, X.; Tan, L.; Wang, X.; Liu, W.; Lu, Y.; Cheng, L.; Sun, Z. Comparison of Nasopharyngeal and Oropharyngeal Swabs for SARS-CoV-2 Detection in 353 Patients Received Tests with Both Specimens Simultaneously. Int. J. Infect. Dis. 2020, 94, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Collection and Transport System ESwabTM|COPAN Spa. Available online: https://products.copangroup.com/index.php/products/clinical/eswab (accessed on 22 December 2020).
- Struyf, T.; Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Leeflang, M.M.; Spijker, R.; Hooft, L.; Emperador, D.; Dittrich, S.; et al. Signs and Symptoms to Determine If a Patient Presenting in Primary Care or Hospital Outpatient Settings Has COVID-19 Disease. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Malecki, M.; Lüsebrink, J.; Teves, S.; Wendel, A.F. Pharynx Gargle Samples Are Suitable for SARS-CoV-2 Diagnostic Use and Save Personal Protective Equipment and Swabs. Infect. Control. Hosp. Epidemiol. 2020, 11, 1–2. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.-W.; Tsang, O.T.-Y.; Yip, C.C.-Y.; Chan, K.-H.; Wu, T.-C.; Chan, J.M.-C.; Leung, W.-S.; Chik, T.S.-H.; Choi, C.Y.-C.; Kandamby, D.H.; et al. Consistent Detection of 2019 Novel Coronavirus in Saliva. Clin. Infect. Dis. 2020, 71, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | N | N (%) | Mean ± SD | Median (Q1–Q3) | Extremes |
|---|---|---|---|---|---|
| Age (years) | 75 | 63.2 ± 16.7 | 66 (53; 77) | 24; 96 | |
| Sex, Female | 75 | 33 (44.0) | |||
| Positive swab at T1 | |||||
| NP | 70 | 59 (84.3) | 29.7 ± 5.5 | 30.3 (26.3; 34.3) | 13.7; 38.0 |
| Pool | 47 | 39 (83.0) | 30.7 ± 5.4 | 31.3 (27.8; 34.7) | 15.3; 37.6 |
| TW | 73 | 54 (74.0) | 30.8 ± 4.4 | 31.1 (29.1; 34.0) | 18.4; 37.8 |
| S | 66 | 45 (68.2) | 32.4 ± 4.6 | 33.9 (30.7; 35.1) | 18.3; 39.5 |
| OP | 68 | 40 (58.8) | 32.7 ± 3.9 | 34.3 (30.4; 35.7) | 22.0; 37.6 |
| R | 29 | 1 (3.5) | 34.8 | ||
| TW | 42 | 20 (47.6) | 32.7 ± 4.5 | 33.9 (29.6; 36.0) | 22.2; 38.6 |
| Pool | 21 | 9 (42.9) | 32.6 ±3.8 | 32.9 (31.2; 34.9) | 25.1; 38.8 |
| OP | 40 | 15 (37.5) | 33.1 ± 2.9 | 33.7 (30.6; 35.4) | 27.4; 38.1 |
| S | 39 | 14 (35.9) | 33.1 ± 3.4 | 33.3 (30.9; 35.6) | 26.6; 37.9 |
| NP | 40 | 11 (27.5) | 33.0 ± 3.7 | 33.5 (29.2; 36.4) | 26.4; 37.4 |
| Positive swab at T3 | |||||
| TW | 14 | 7 (50.0) | 32.6 ± 4.6 | 34.2 (32.2; 35.8) | 22.7; 36.2 |
| OP | 12 | 5 (41.7) | 32.6 ± 6.2 | 34.5 (33.0; 35.6) | 21.9; 37.9 |
| S | 12 | 4 (33.3) | 34.2 ± 4.7 | 36.1 (31.4; 37.0) | 27.2; 37.3 |
| NP | 10 | 1 (10.0) | 34.4 | ||
| Pool | 1 | 1 (100.0) | 34.5 | ||
| Days between symptom onset and sample collection at T1 | 75 | 12.9 ± 8.8 | 12 (6; 18) | −14; 35 | |
| Days between symptom onset and sample collection at T2 | 45 | 24.5 ± 11.4 | 23 (16; 28) | 8; 54 | |
| Days between symptom onset and sample collection at T3 | 15 | 28.0 ± 7.2 | 28 (22; 31) | 19; 45 | |
| Number of symptoms at T1 | 73 | 4.1 ± 2.1 | 4 (3; 6) | 0; 9 | |
| Number of symptoms at T2 | 28 | 3.1 ± 1.9 | 3 (1.5; 4.5) | 0; 7 | |
| Number of symptoms at T3 | 11 | 2.1 ± 2.0 | 2 (0; 4) | 0; 5 |
| NP | Pool | TW | S | OP | R | |
|---|---|---|---|---|---|---|
| NP | κ = 0.25 [−0.10; 0.59] p = 0.092 | κ = 0.078 [−0.16; 0.32] p = 0.50 | κ = 0.29 [0.06; 0.53] p = 0.0096 | κ = 0.15 [−0.05; 0.35] p = 0.14 | κ = 0.012 [−0.01; 0.04] p = 0.68 | |
| Pool | κ = 0.044 [−0.23; 0.32] p = 0.75 | κ = 0.32 [0.01; 0.63] p = 0.028 | κ = 0.050 [−0.19; 0.29] p = 0.68 | κ = 0.022 [−0.02; 0.07] p = 0.59 | ||
| TW | κ = 0.48 [0.25; 0.72] p < 0.0001 | κ = 0.46 [0.25; 0.67] p < 0.0001 | κ = 0.047 [−0.05; 0.14] p = 0.41 | |||
| S | κ = 0.50 [0.28; 0.72] p < 0.0001 | κ = 0.042 [−0.04; 0.12] p = 0.46 | ||||
| OP | κ = −0.071 [−0.21; 0.07] p = 0.31 |
| Symptoms | T1 (n = 75) | T2 (n = 45) | T3 (n = 15) | ||||
|---|---|---|---|---|---|---|---|
| N | N (%) | N | N (%) | N | N (%) | ||
| Cough | 73 | 47 (64.4) | 28 | 9 (32.1) | 10 | 3 (30.0) | |
| Dyspnea | 73 | 39 (53.4) | 28 | 13 (46.6) | 10 | 4 (40.0) | |
| Sore throat | 73 | 15 (20.6) | 28 | 3 (10.7) | 10 | 0 (0.0) | |
| Rhinorrhea | 73 | 22 (30.1) | 28 | 8 (28.6) | 10 | 2 (20.0) | |
| Stomach aches | 73 | 15 (20.6) | 28 | 0 (0.0) | 10 | 0 (0.0) | |
| Fever | 73 | 16 (21.9) | 28 | 1 (3.6) | 11 | 0 (0.0) | |
| Diarrhea | 73 | 17 (23.3) | 28 | 1 (3.6) | 10 | 1 (10.0) | |
| Muscle pain | 72 | 30 (41.7) | 28 | 8 (28.6) | 10 | 0 (0.0) | |
| Ageusia | 73 | 17 (23.3) | 28 | 10 (35.7) | 10 | 3 (30.0) | |
| Anosmia | 73 | 19 (26.0) | 28 | 9 (32.1) | 10 | 3 (30.0) | |
| Headache | 73 | 28 (38.4) | 28 | 11 (39.3) | 10 | 1 (10.0) | |
| Other symptoms | 73 | 37 (50.7) | 28 | 13 (46.4) | 10 | 6 (60.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Defêche, J.; Azarzar, S.; Mesdagh, A.; Dellot, P.; Tytgat, A.; Bureau, F.; Gillet, L.; Belhadj, Y.; Bontems, S.; Hayette, M.-P.; et al. In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2. Pathogens 2021, 10, 1362. https://doi.org/10.3390/pathogens10111362
Defêche J, Azarzar S, Mesdagh A, Dellot P, Tytgat A, Bureau F, Gillet L, Belhadj Y, Bontems S, Hayette M-P, et al. In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2. Pathogens. 2021; 10(11):1362. https://doi.org/10.3390/pathogens10111362
Chicago/Turabian StyleDefêche, Justine, Samira Azarzar, Alyssia Mesdagh, Patricia Dellot, Amandine Tytgat, Fabrice Bureau, Laurent Gillet, Yasmine Belhadj, Sebastien Bontems, Marie-Pierre Hayette, and et al. 2021. "In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2" Pathogens 10, no. 11: 1362. https://doi.org/10.3390/pathogens10111362
APA StyleDefêche, J., Azarzar, S., Mesdagh, A., Dellot, P., Tytgat, A., Bureau, F., Gillet, L., Belhadj, Y., Bontems, S., Hayette, M.-P., Schils, R., Rahmouni, S., Ernst, M., Moutschen, M., & Darcis, G. (2021). In-Depth Longitudinal Comparison of Clinical Specimens to Detect SARS-CoV-2. Pathogens, 10(11), 1362. https://doi.org/10.3390/pathogens10111362