
Medical Imaging in the Diagnosis of Schistosomiasis: A Review

 ,
,  , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. X-rays, Ultrasound, and Computed Tomography Findings
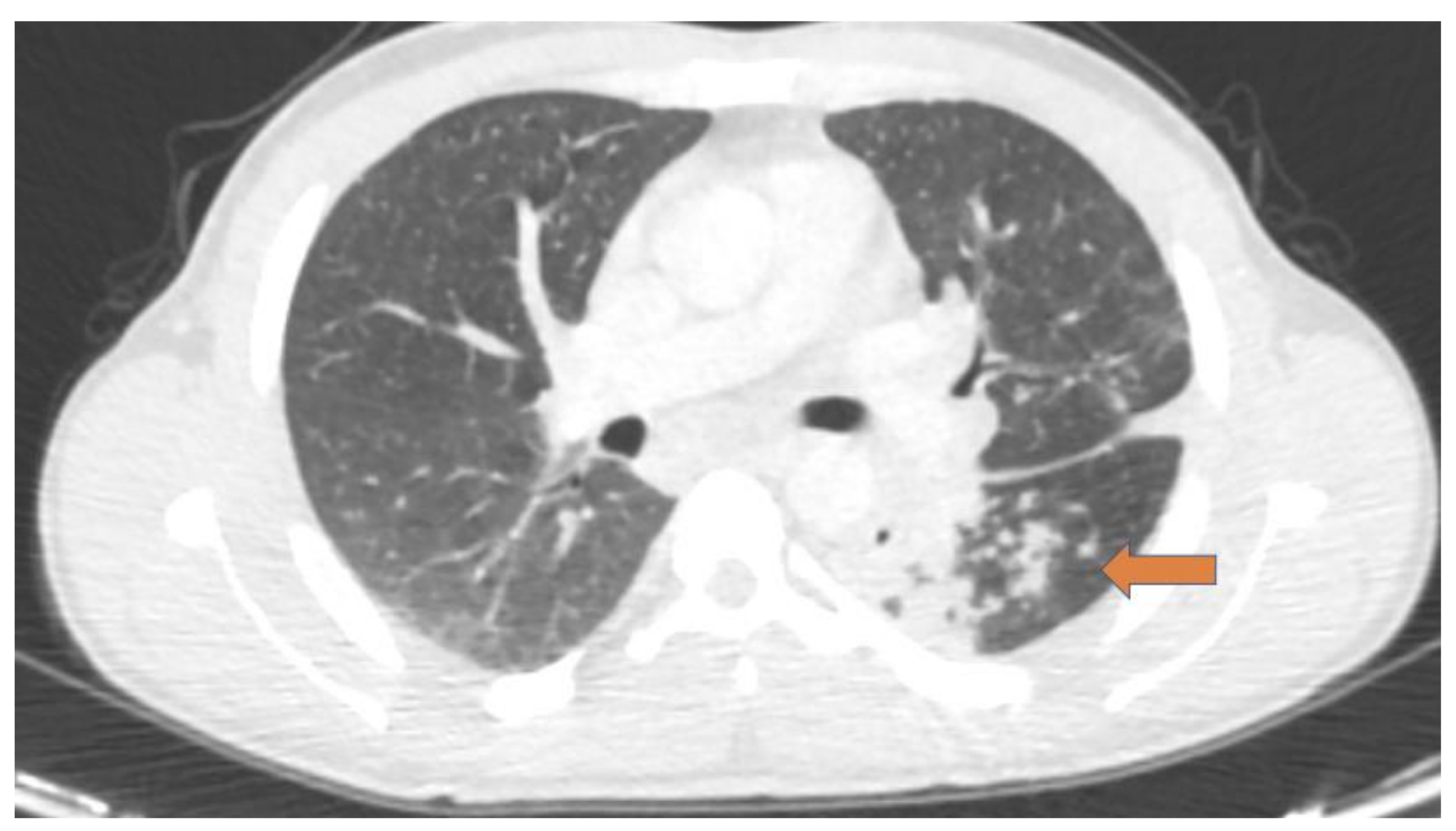
2.1. Pulmonary Schistosomiasis
2.2. Hepatointestinal Schistosomiasis
2.3. Genitourinary Schistosomiasis
2.4. Central Nervous System Schistosomiasis
3. Magnetic Resonance Imaging Findings
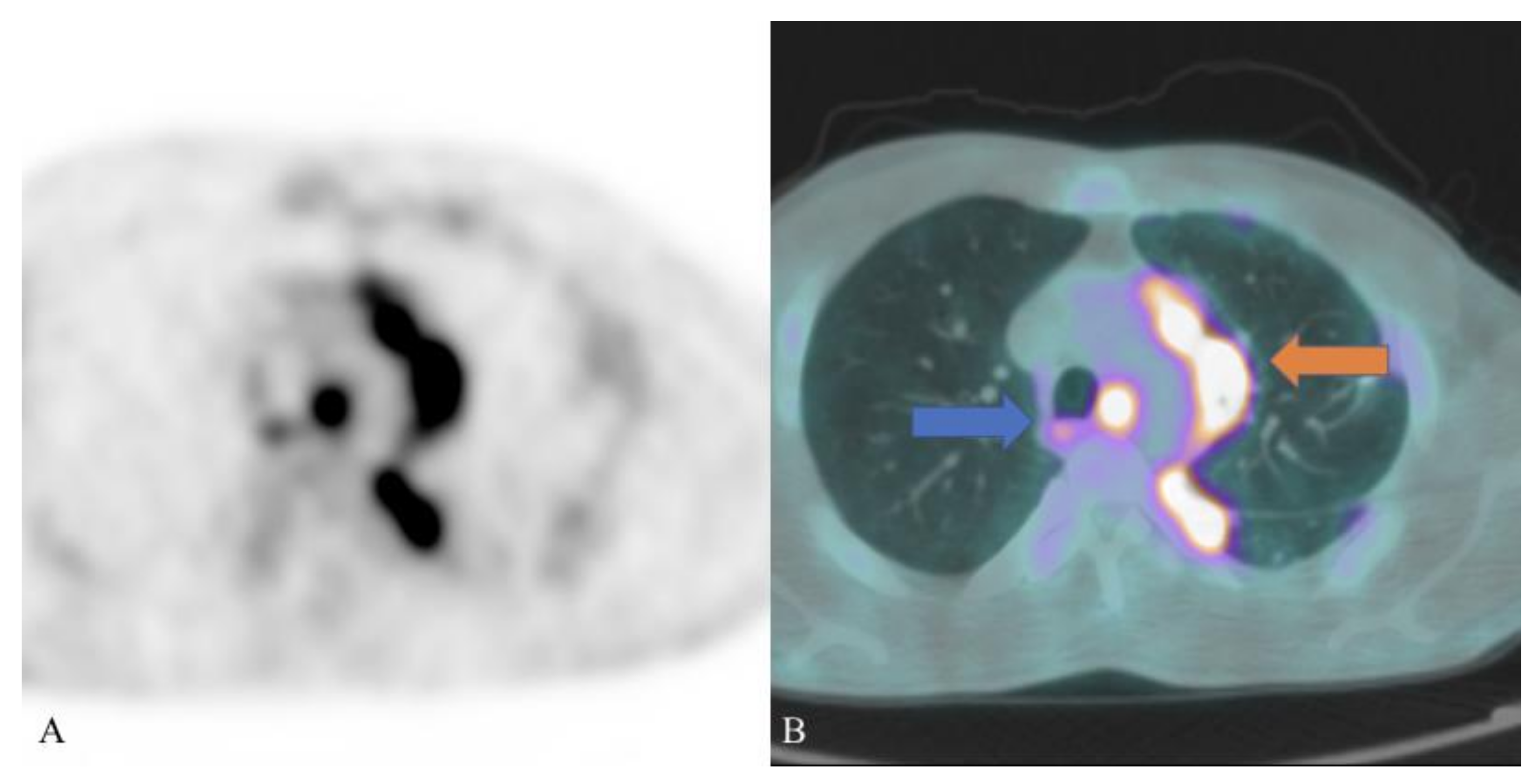
4. PET/CT Findings
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McManus, D.P.; Dunne, D.W.; Sacko, M.; Utzinger, J.; Vennervald, B.J.; Zhou, X.N. Schistosomiasis. Nat. Rev. Dis. Primers 2018, 4, 13. [Google Scholar] [CrossRef]
- Coltart, C.; Whitty, C.J.M. Schistosomiasis in non-endemic countries. Clin. Med. 2015, 15, 67–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roure, S.; Valerio, L.; Pérez-Quilez, O.; Fernandez-Rivas, G.; Martinez-Cuevas, O.; Alcantara-Roman, A.; Viasus, D.; Pedro-Botet, M.L.; Sabrià, M.; Clotet, B. Epidemiological, clinical, diagnostic and economic features of an immigrant population of chronic schistosomiasis sufferers with long-term residence in a nonendemic country (North Metropolitan area of Barcelona, 2002–2016). PLoS ONE 2017, 12, e0185245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nepal, P.; Ojili, V.; Songmen, S.; Batchala, P.; Kumar, D.; Nagar, A.M. Multisystem imaging review of human schistosomiasis: Characteristic imaging findings. Clin. Imaging 2019, 54, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, Y.; Hirooka, M.; Tanaka, T.; Sunago, K.; Yukimoto, A.; Imai, Y.; Watanabe, T.; Ishihara, T.; Yoshida, O.; Yamamoto, Y.; et al. Schistosomiasis diagnosed using laparoscopy and colonoscopy. Intern. Med. 2019, 58, 2495–2499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemann, T.; Marti, H.P.; Duhnsen, S.H.; Bongartz, G. Pulmonary schistosomiasis—Imaging features. J. Radiol. Case Rep. 2010, 4, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, N. Schistosomiasis and hookworm infection in humans: Disease burden, pathobiology and anthelmintic vaccines. Parasitol. Int. 2020, 75, 102051. [Google Scholar] [CrossRef] [PubMed]
- Lindner, T.; Stenzel, J.; Koslowski, N.; Hohn, A.; Glass, A.; Schwarzenböck, S.M.; Krause, B.J.; Vollmar, B.; Reisinger, E.C.; Sombetzki, M. Anatomical MRI and [18F] FDG PET/CT imaging of Schistosoma mansoni in a NMRI mouse model. Sci. Rep. 2020, 10, 17343. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.G.; Vickers, D.; Olds, G.R.; Shah, S.M.; McManus, D.P. Katayama syndrome. Lancet Infect. Dis. 2007, 7, 218–224. [Google Scholar] [CrossRef]
- Gobbi, F.; Buonfrate, D.; Angheben, A.; Bisoffi, Z. Restaging pulmonary schistosomiasis. Am. J. Trop. Med. Hyg. 2019, 100, 1049–1051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Oliveira, L.S.; Kuzma, G.S.P.; Costa, L.C.V.; João, P.R.D. Schistosomal myeloradiculopathy in a non-endemic area. Rev. Paul. Pediatr. 2020, 38, e2018232. [Google Scholar] [CrossRef] [Green Version]
- Zheng, B.; Zhang, J.; Chen, H.; Nie, H.; Miller, H.; Gong, Q.; Liu, C. T lymphocyte-mediated liver immunopathology of schistosomiasis. Front. Immunol. 2020, 11, 61. [Google Scholar] [CrossRef] [Green Version]
- Cimini, A.; Ricci, M.; Chiaravalloti, A.; Crocco, A.; Russo, F.; Schillaci, O. A rare case of pulmonary schistosomiasis: 18F-fluorodeoxyglucose positron emission tomography/computed tomography findings. Indian J. Nucl. Med. 2020, 35, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Gryseels, B. Schistosomiasis. Infect. Dis. Clin. N. Am. 2012, 26, 383–397. [Google Scholar] [CrossRef]
- Potters, I.; Van Duffel, L.; Broeckx, G.; Bottieau, E. Intestinal schistosomiasis: A very long-lived tropical parasite. Clin. Microbiol. Infect. 2019, 25, 696–698. [Google Scholar] [CrossRef] [PubMed]
- Masi, B.; Perles-Barbacaru, T.A.; Bernard, M.; Viola, A. Clinical and preclinical imaging of hepatosplenic schistosomiasis. Trends Parasitol. 2020, 36, 206–226. [Google Scholar] [CrossRef]
- Shen, J.; Yuan, L.; Sun, Y.; Jiang, X.; Shao, X. Case report: Multiple schistosomiasis japonica cerebral granulomas without gastrointestinal system involvement: Report of two cases and review of literature. Am. J. Trop. Med. Hyg. 2020, 102, 1376–1381. [Google Scholar] [CrossRef]
- Chauvin, A.; Ghazali, A.; Le Jeunne, C.; Plaisance, P.; Szwebel, T.A.; Costedoat-Chalumeau, N.; Beubon, F.; Reiner, P.; Paugam, A.; Paule, R. Acute paraplegia due to schistosomiasis: An uncommon cause in developed countries. J. Neurovirol. 2019, 25, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Verjee, M.A. Schistosomiasis: Still a cause of significant morbidity and mortality. Res. Rep. Trop. Med. 2019, 10, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Vale, N.; Gouveia, M.J.; Rinaldi, G.; Brindley, P.J.; Gartner, F.; Correia da Costa, J.M. Praziquantel for schistosomiasis: Single-Drug metabolism revisited, mode of action, and resistance. Antimicrob. Agents Chemother. 2017, 61, e02582–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thummar, H.G.; Vithlani, H.I.; Suthar, P.P.; John, D.R.; Thummar, N.; Chauhan, H. A rare case of schistosomiasis (bilharzia) of the bladder in a non-endemic area. Pol. J. Radiol. 2017, 82, 376–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, M.G.; Cunha, A.F.A.; Peralta, J.M. The advances in molecular and new point-of-care (poc) diagnosis of schistosomiasis pre- and post-praziquantel use: In the pursuit of more reliable approaches for low endemic and non-endemic areas. Front. Immunol. 2019, 10, 858. [Google Scholar] [CrossRef] [PubMed]
- Gray, D.J.; Ross, A.G.; Li, Y.S.; McManus, D.P. Diagnosis and management of schistosomiasis. BMJ 2011, 342, d2651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomari, E.; Piubelli, C.; Perandin, F.; Bisoffi, Z. Digital PCR: A new technology for diagnosis of parasitic infections. Clin. Microbiol. Infect. 2019, 25, 1510–1516. [Google Scholar] [CrossRef] [PubMed]
- Foti, G.; Gobbi, F.; Angheben, A.; Faccioli, N.; Cicciò, C.; Carbognin, G.; Buonfrate, D. Radiographic and HRCT imaging findings of chronic pulmonary schistosomiasis: Review of 10 consecutive cases. BJR Case Rep. 2019, 5, 20180088. [Google Scholar] [CrossRef]
- Gobbi, F.; Buonfrate, D.; Angheben, A.; Beltrame, A.; Bassetti, M.; Bertolaccini, L.; Bogina, G.; Caia, S.; Duranti, S.; Gobbo, M.; et al. Pulmonary nodules in African migrants caused by chronic schistosomiasis. Lancet Infect. Dis. 2017, 17, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Zhang, J.; Zheng, T.; Chen, H.; Nie, H.; Zheng, B.; Gong, Q. The role of microRNAs in the pathogenesis, grading and treatment of hepatic fibrosis in schistosomiasis. Parasites Vectors 2019, 12, 611. [Google Scholar] [CrossRef] [Green Version]
- Olveda, D.U.; Olveda, R.M.; Lam, A.K.; Chau, T.N.P.; Li, Y.; Gisparil, A.D., 2nd; Ross, A.G.P. Utility of diagnostic imaging in the diagnosis and management of schistosomiasis. Clin. Microbiol. 2014, 3, 142. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Tseng, Y.; Xu, N.; Yin, X.; Xie, X.; Zhang, L.; Wu, W.; Zhu, W.; Wu, W.; Yao, J.; et al. Evaluation of transient elastography in assessing liver fibrosis in patients with advanced schistosomiasis japonica. Parasitol. Int. 2018, 67, 302–308. [Google Scholar] [CrossRef]
- Lee, D.; Shaffer, K. Concentric rings: Updated CT appearance of hepatic schistosomiasis mansoni. Radiol. Case Rep. 2015, 7, 134–139. [Google Scholar]
- Araki, T.; Hayakawa, K.; Okada, J.; Hayashi, S.; Uchiyama, G.; Yamada, K. Hepatic schistosomiasis japonica identified by CT. Radiology 1985, 157, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Rabello, A.L.T.; Pinto-Silva, R.A.; Rocha, R.S.; Katz, N. Abdominal ultrasonography in acute clinical schistosomiasis mansoni. Am. J. Trop. Med. Hyg. 1994, 50, 748–752. [Google Scholar] [CrossRef]
- Cesmeli, E.; Vogelaers, D.; Voet, D.; Duyck, P.; Peleman, R.; Kunnen, M.; Afschrift, M. Ultrasound and CT changes of liver parenchyma in acute schistosomiasis. Br. J. Radiol. 1997, 70, 758–760. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.C.; Chiang, J.H.; Chou, Y.H.; Rubesin, S.E.; Wu, H.P.; Jeng, W.C.; Hsu, C.C.; Tiu, C.M.; Chang, T. Intestinal schistosomiasis japonica: CT-pathologic correlation. Radiology 1994, 193, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.; Zhang, W.; Wang, P.J. CT manifestation of abdomen and its pathology of patients with chronic schistosomiasis. Chin. J. Schistosomiasis Control (Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi) 2012, 24, 200–202. [Google Scholar]
- Valluru, B.; Zhou, Z.; Sah, D.; Du, W.; Ali, M.O.; Adam, A.A.; Zhang, L.; Wang, J.J. Analysis of CT characteristics in the diagnosis of Schistosoma japonicum associated appendicitis with clinical and pathological correlation: A diagnostic accuracy study. Jpn. J. Radiol. 2020, 38, 178–191. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, K.; Birnie, B.W.; Garraway, N. Large bowel obstruction secondary to schistosomiasis-related colonic stricture. Int. J. Surg. Case Rep. 2020, 74, 209–213. [Google Scholar] [CrossRef]
- Pollack, H.M.; Banner, M.P.; Martinez, L.O.; Hodson, C.J. Diagnostic considerations in urinary bladder wall calcification. AJR Am. J. Roentgenol. 1981, 136, 791–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shebel, H.M.; Elsayes, K.M.; Abou El Atta, H.M.; Elguindy, Y.M.; El-Diasty, T.A. Genitourinary schistosomiasis: Life cycle and radiologic-pathologic findings. Radiographics 2012, 32, 1031–1046. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Botelho, M.C.; Holtfreter, M.C.; Akpata, R.; El Scheich, T.; Neumayr, A.; Brunetti, E.; Hatz, C.; Dong, Y.; Dietrich, C.F. Ultrasound assessment of schistosomiasis. Z. Gastroenterol. 2016, 54, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Botelho, M.C.; Alves, H.; Richter, J. Halting Schistosoma haematobium-associated bladder cancer. Int. J. Cancer Manag. 2017, 10, e9430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouprêt, M.; Neuzillet, Y.; Pignot, G.; Compérat, E.; Audenet, F.; Houédé, N.; Larré, S.; Masson-Lecomte, A.; Colin, P.; Brunelle, S.; et al. French ccAFU guidelines-update 2018–2020: Bladder cancer. Prog. Urol. 2019, 28, R48–R80. [Google Scholar] [CrossRef]
- Lorca, J.; Hevia, V.; Nicolás, V.D.; González, A.; Sánchez Guerrero, C.; Burgos Revilla, F.J. Minimmally invasive resolution of a left ureteral stenosis after Schistosoma haematobium infection. Urol. Case Rep. 2019, 25, 100889. [Google Scholar] [CrossRef] [PubMed]
- Pal, P.O.; Smith, R.D.; Allen, S.; Ratynska, M.; Edwards, S.; Gothard, P.; Logan, S. Schistosomiasis—A disobedient ureter, a disobedient diagnosis. J. Endourol. Case Rep. 2017, 3, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Kayuni, S.; Lampiao, F.; Makaula, P.; Juziwelo, L.; Lacourse, E.J.; Reinhard-Rupp, J.; Leutscher, P.D.C.; Stothard, J.R. A systematic review with epidemiological update of male genital schistosomiasis (MGS): A call for integrated case management across the health system in sub-Saharan Africa. Parasite Epidemiol. Control. 2018, 4, e00077. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Bertelli, E.; Savi, E.; Verna, S.; Zammarchi, L.; Tilli, M.; Rinaldi, F.; Pradella, S.; Agostini, S.; Miele, V. Ultrasound findings in urogenital schistosomiasis: A pictorial essay. J. Ultrasound 2020, 23, 195–205. [Google Scholar] [CrossRef]
- Hotez, P.J.; Engels, D.; Gyapong, M.; Ducker, C.; Malecela, M.N. Female genital schistosomiasis. N. Engl. J. Med. 2019, 381, 2493–2495. [Google Scholar] [CrossRef]
- Coyle, C.M. Schistosomiasis of the nervous system. Handb. Clin. Neurol. 2013, 114, 271–281. [Google Scholar]
- El Beltagi, A.; Salem, K.; Hanoun, M. Neuro-schistosomiasis with palm tree contrast enhancement pattern, a report of three cases, and review of literature. BJR Case Rep. 2020, 7, 20200053. [Google Scholar] [CrossRef]
- Vale, T.C.; Oliveira, M.M.; de Sousa-Pereira, S.R.; Lambertucci, J.R.; Gusmão, S.N.S. Diffuse pseudotumoral cerebral Schistosomiasis mansoni: A new form of presentation. Arq. Bras. Neurocir. 2011, 30, 186–189. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.Y.; Zhao, S.; Wei, Y. Cerebral schistosomiasis: MRI features with pathological correlation. Acta Radiol. 2021, 62, 646–652. [Google Scholar] [CrossRef]
- Suthiphosuwan, S.; Lin, A.; Gao, A.F.; Munoz, D.G.; Spears, J.; Bharata, A. Delayed presentation of cerebral schistosomiasis presenting as a tumor-like brain lesion. Neuroradiol. J. 2018, 31, 395–398. [Google Scholar] [CrossRef]
- Huang, J.; Luo, J.; Peng, J.; Yang, T.; Zheng, H.; Mao, C. Cerebral schistosomiasis: Diffusion-weighted imaging helps to differentiate from brain glioma and metastasis. Acta Radiol. 2017, 58, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Adeel, A.A. Spinal cord schistosomiasis. Sudan J. Paediatr. 2015, 15, 23–28. [Google Scholar] [PubMed]
- Bezerra, A.S.; D’Ippolito, G.; Caldana, R.P.; Leopoldino, D.D.; Batista, G.R.; Borges, D.R.; de Jesus Lopes Filho, G.; Ahmed, M. Differentiating cirrhosis and chronic hepatosplenic schistosomiasis using MRI. AJR Am. J. Roentgenol. 2008, 190, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Lambertucci, J.R. Revisiting the concept of hepatosplenic schistosomiasis and its challenges using traditional and new tools. Rev. Soc. Bras. Med. Trop. 2014, 47, 130–136. [Google Scholar] [CrossRef] [Green Version]
- Bilgin, S.S.; Toprak, H.; Seker, M. Imaging findings of hepatosplenic schistosomiasis: A case report. Radiol. Case Rep. 2016, 11, 152–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, J.; Stojkovic, M.; Kauczor, J.U.; Junghanss, T.; Weber, T.F. Performance of magnetic resonance susceptibility-weighted imaging for detection of calcifications in patients with hepatic echinococcosis. J. Comput. Assist. Tomogr. 2018, 42, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.N.; Higa, H.C.M.; Rondina, R.G.; Miranda, M.M.L.; Kaddoun, M.L.; Santos, M.C.F.L.S.; Souza, R.S.M. Testicular schistosomiasis as differential diagnosis for testicular nodules: A case report. Rev. Soc. Bras. Med. Trop. 2015, 48, 501–503. [Google Scholar] [CrossRef] [Green Version]
- Becker, J.; Schwarzenböck, S.M.; Krause, B.J. FDG PET hybrid imaging. Recent Results Cancer Res. 2020, 216, 625–667. [Google Scholar]
- Feng, H.; Wang, X.; Chen, J.; Cui, J.; Gao, T.; Gao, Y.; Zeng, W. Nuclear imaging of glucose metabolism: Beyond 18F-FDG. Contrast Media Mol. Imaging 2019, 2019, 7954854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamar, F.; Buscombe, J.; Chiti, A.; Christian, P.E.; Delbeke, D.; Donohoe, K.J.; Israel, O.; Martin-Comin, J.; Signore, A. EANM/SNMMI guideline for 18F-FDG use in inflammation and infection. J. Nucl. Med. 2013, 54, 647–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bueding, E. Carbohydrate metabolism of schistosoma mansoni. J. Gen. Physiol. 1950, 33, 475–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, N.; Balkman, J.D.; Wang, J.; Wilson, D.L.; Lee, Z.; King, C.L.; Basilion, J.P. In Vivo imaging of schistosomes to assess disease burden using positron emission tomography (PET). PLoS Negl. Trop. Dis. 2010, 4, e827. [Google Scholar] [CrossRef] [Green Version]
- Ye, S.; Wang, W.L.; Zhao, K. F-18 FDG hypermetabolism in mass-forming focal pancreatitis and old hepatic schistosomiasis with granulomatous inflammation misdiagnosed by PET/CT imaging. Int. J. Clin. Exp. Pathol. 2014, 7, 6339–6344. [Google Scholar]
- Altinyay, M.E.; Alharthi, A.; Alassiri, A.H.; Syed, G.M.S. 18F-FDG hypermetabolism in spinal cord schistosomiasis. Clin. Nucl. Med. 2016, 41, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Daghigh, A.; Grüner, J.M.; Mørup, P. Intestinal FDG-PET/CT imaging of an Eritrean with schistosomiasis seen in Denmark. Eur. J. Hybrid. Imaging 2019, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segall, G.; Delbeke, D.; Stabin, M.G.; Even-Sapir, E.; Fair, J.; Sajdak, R.; Smith, G.T. SNM practice guideline for sodium 18F-fluoride PET/CT bone scans 1.0. J. Nucl. Med. 2010, 51, 1813–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Chen, L.; Wan, Q.; Chen, Y. 18F-NaF PET/CT Finding in a Patient with Abdominal Discomfort After Schistosomiasis. Clin. Nucl. Med. 2018, 43, 183–185. [Google Scholar] [CrossRef]
- Lentz, B.; Fong, T.; Rhyne, R.; Risko, N. A systematic review of the cost-effectiveness of ultrasound in emergency care settings. Ultrasound J. 2021, 13, 16. [Google Scholar] [CrossRef]
- Richter, J. Evolution of schistosomiasis-induced pathology after therapy and interruption of exposure to schistosomes: A review of ultrasonographic studies. Acta Trop. 2000, 77, 111–131. [Google Scholar] [CrossRef]
- Stella, M.; Martínez, S.M.; Crespo, G.; Navasa, M.; Forns, X. Noninvasive assessment of liver fibrosis. Hepatology 2011, 53, 325–335. [Google Scholar]
- Ozturk, A.; Grajo, J.R.; Dhyani, M.; Anthony, B.W.; Samir, A.E. Principles of ultrasound elastography. Abdom. Radiol. 2018, 43, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Stopsack, K.H.; Cerhan, J.R. Cumulative doses of ionizing radiation from computed tomography: A population-based study. Mayo Clin. Proc. 2019, 94, 2011–2021. [Google Scholar] [CrossRef]
- Huynh, K.; Baghdanian, A.H.; Baghdanian, A.A.; Sun, D.S.; Pallav Kolli, K.; Zagoria, R.J. Updated guidelines for intravenous contrast use for CT and MRI. Emerg. Radiol. 2020, 27, 115–126. [Google Scholar] [CrossRef]
- Wen, S.C.H.; Anderson, R.; Ryan, M.M.; Kumbla, S.; Wray, A.; Steer, A. Pediatric neuroschistosomiasis: A case report and review of the literature. J. Pediatr. Infect. Dis. Soc. 2019, 8, 489–491. [Google Scholar] [CrossRef]
- Detzler, J.; Backes, H.; Guldner, J. Radiculomyelopathy in schistosomiasis. Nervenarzt 2018, 89, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Lambertucci, J.R.; Mamede, M.; Pereira, T.A. In Vivo MRI assessment of experimental schistosomiasis. Trends Parasitol. 2016, 32, 3–5. [Google Scholar] [CrossRef]
- Stojkovic, M.; Müller, J.; Junghanss, T.; Weber, T.F. Radiological diagnoses in the context of emigration: Infectious diseases. RoFo 2018, 190, 121–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masi, B.; Parles-Barbacaru, T.A.; Laprie, C.; Dessein, H.; Bernard, M.; Dessein, A.; Viola, A. In Vivo MRI Assessment of Hepatic and Splenic Disease in a Murine Model of Schistosomiasis. PLoS Negl. Trop. Dis. 2015, 9, e0004036. [Google Scholar]
- Kung, B.T.; Seraj, S.M.; Zadeh, M.Z.; Rojulpote, C.; Kothekar, E.; Ayubcha, C.; Ng, K.S.; Ng, K.K.; Au-Yong, T.K.; Werner, T.J.; et al. An update on the role of 18F-FDG-PET/CT in major infectious and inflammatory diseases. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 255–273. [Google Scholar] [PubMed]
- Treglia, G. Diagnostic performance of 18F-FDG PET/CT in infectious and inflammatory diseases according to published meta-analyses. Contrast Media Mol. Imaging 2019, 2019, 3018349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skelly, P.J. The use of imaging to detect schistosomes and diagnose schistosomiasis. Parasite Immunol. 2013, 35, 295–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaushik, A.; Jaimini, A.; Tripathi, M.; D’Souza, M.; Sharma, R.; Mondal, A.; Mishra, A.K.; Dwarakanath, B.S. Estimation of radiation dose to patients from 18FDG whole body PET/CT investigations using dynamic PET scan protocol. Indian J. Med. Res. 2015, 142, 721–731. [Google Scholar]
- Chiaravalloti, A.; Filippi, L.; Ricci, M.; Cimini, A.; Schillaci, O. Molecular Imaging in Pediatric Brain Tumors. Cancers 2019, 11, 1853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eychenne, R.; Bouvry, C.; Bourgeois, M.; Loyer, P.; Benoist, E.; Lepareur, N. Overview of radiolabeled somatostatin analogs for cancer imaging and therapy. Molecules 2020, 25, 4012. [Google Scholar] [CrossRef]
- Vorster, M.; Maes, A.; van de Wiele, C.; Sathekge, M. Gallium-68 PET: A powerful generator-based alternative to infection and inflammation imaging. Semin. Nucl. Med. 2016, 46, 436–447. [Google Scholar] [CrossRef]
- Cimini, A.; Ricci, M.; Chiaravalloti, A.; Filippi, L.; Schillaci, O. Theragnostic aspects and radioimmunotherapy in pediatric tumors. Int. J. Mol. Sci. 2020, 21, 3849. [Google Scholar] [CrossRef]
- Cuccurullo, V.; Di Stasio, G.D.; Prisco, M.R.; Mansi, L. Is there a clinical usefulness for radiolabeled somatostatin analogues beyond the consolidated role in NETs? Indian J. Radiol Imaging 2017, 27, 509–516. [Google Scholar]
- Marín-Martínez, L.; Kyriakos, G.; Sánchez-Gutiérrez, D. Pseudotumoral form of schistosomiasis mimicking neuroendocrine tumor: A case report and brief review of the differential diagnosis of retroperitoneal masses. Pan Afr. Med. J. 2020, 37, 186. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Pan, Q.; Yang, X.; Peng, H.; Peng, L.; Zhang, W.; Li, F. Fibroblast activation protein-targeted PET/CT with 68 Ga-FAPI for Imaging IgG4-Related Disease: Comparison to 18F-FDG PET/CT. J. Nucl. Med. 2021, 62, 266–271. [Google Scholar]
- Zhou, Y.; Yang, X.; Liu, H.; Luo, W.; Liu, H.; Lv, T.; Wang, J.; Qin, J.; Ou, S.; Chen, Y. Value of [68Ga]Ga-FAPI-04 imaging in the diagnosis of renal fibrosis. Eur. J. Nucl. Med. Mol. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimini, A.; Ricci, M.; Gigliotti, P.E.; Pugliese, L.; Chiaravalloti, A.; Danieli, R.; Schillaci, O. Medical Imaging in the Diagnosis of Schistosomiasis: A Review. Pathogens 2021, 10, 1058. https://doi.org/10.3390/pathogens10081058
Cimini A, Ricci M, Gigliotti PE, Pugliese L, Chiaravalloti A, Danieli R, Schillaci O. Medical Imaging in the Diagnosis of Schistosomiasis: A Review. Pathogens. 2021; 10(8):1058. https://doi.org/10.3390/pathogens10081058
Chicago/Turabian StyleCimini, Andrea, Maria Ricci, Paola Elda Gigliotti, Luca Pugliese, Agostino Chiaravalloti, Roberta Danieli, and Orazio Schillaci. 2021. "Medical Imaging in the Diagnosis of Schistosomiasis: A Review" Pathogens 10, no. 8: 1058. https://doi.org/10.3390/pathogens10081058
APA StyleCimini, A., Ricci, M., Gigliotti, P. E., Pugliese, L., Chiaravalloti, A., Danieli, R., & Schillaci, O. (2021). Medical Imaging in the Diagnosis of Schistosomiasis: A Review. Pathogens, 10(8), 1058. https://doi.org/10.3390/pathogens10081058