

Molecular Characterization of Bacterial Agents Causing External Ocular Infections Isolates of Patients in a Third Level Hospital

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Study Population with External Ocular Infection
2.3. Isolation of Bacteria from External Ocular Infection Cases
2.4. Bacterial Identification by Mass Spectrometry MALDI-TOF
2.5. Susceptibility/Resistance Assays
2.6. mecA Gene and Mobile Genetic Element SCCmec Characterization
2.7. icaA and icaD Gene Detection in Staphylococcus Strains
2.8. In Vitro Biofilms Formation in icaA+/icaD+ Strains
2.9. Statistical Analysis
3. Results
3.1. Study Population with Ophthalmic Infection
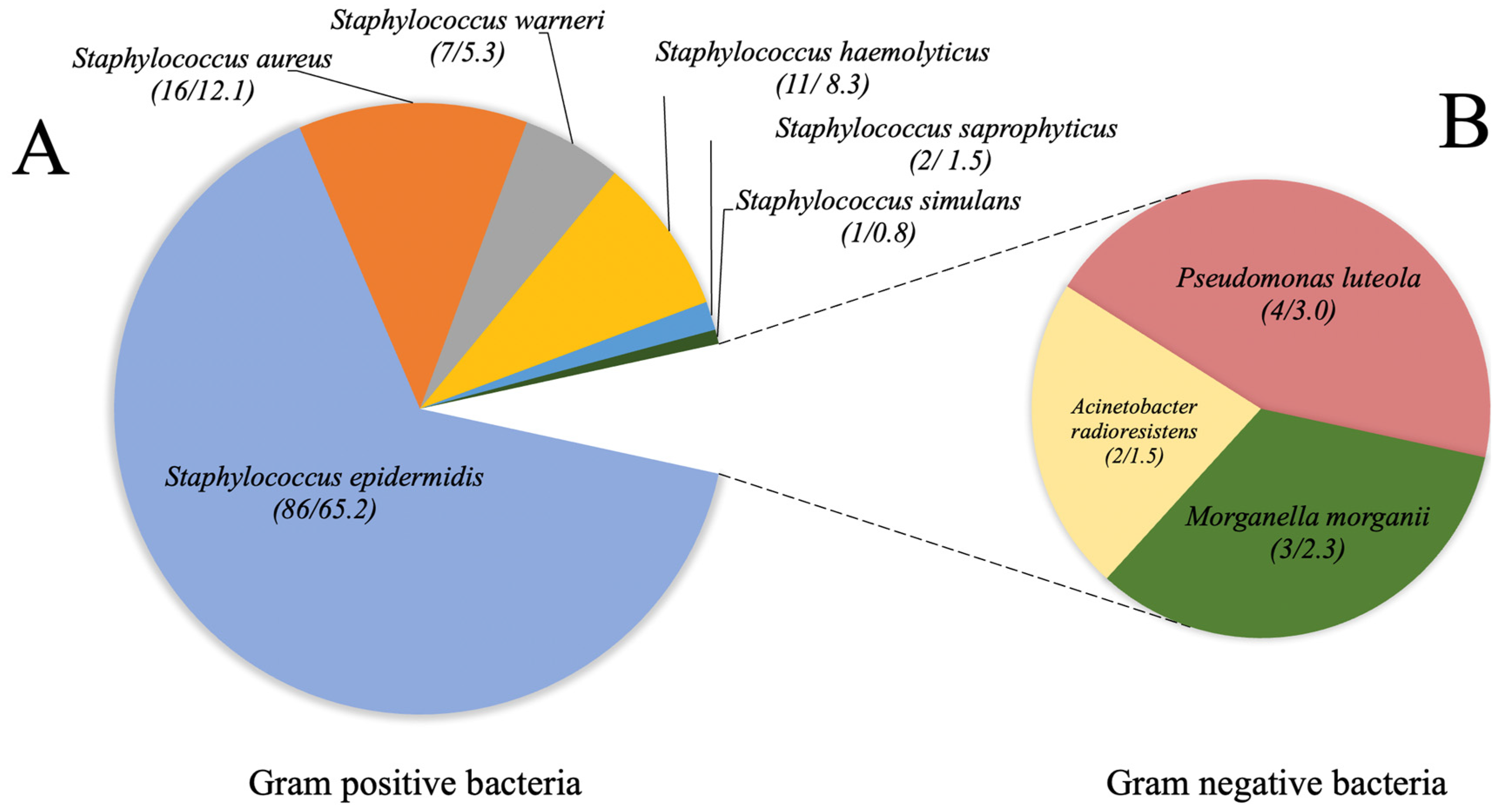
3.2. Bacterial Identification by Mass Spectrometry MALDI-TOF
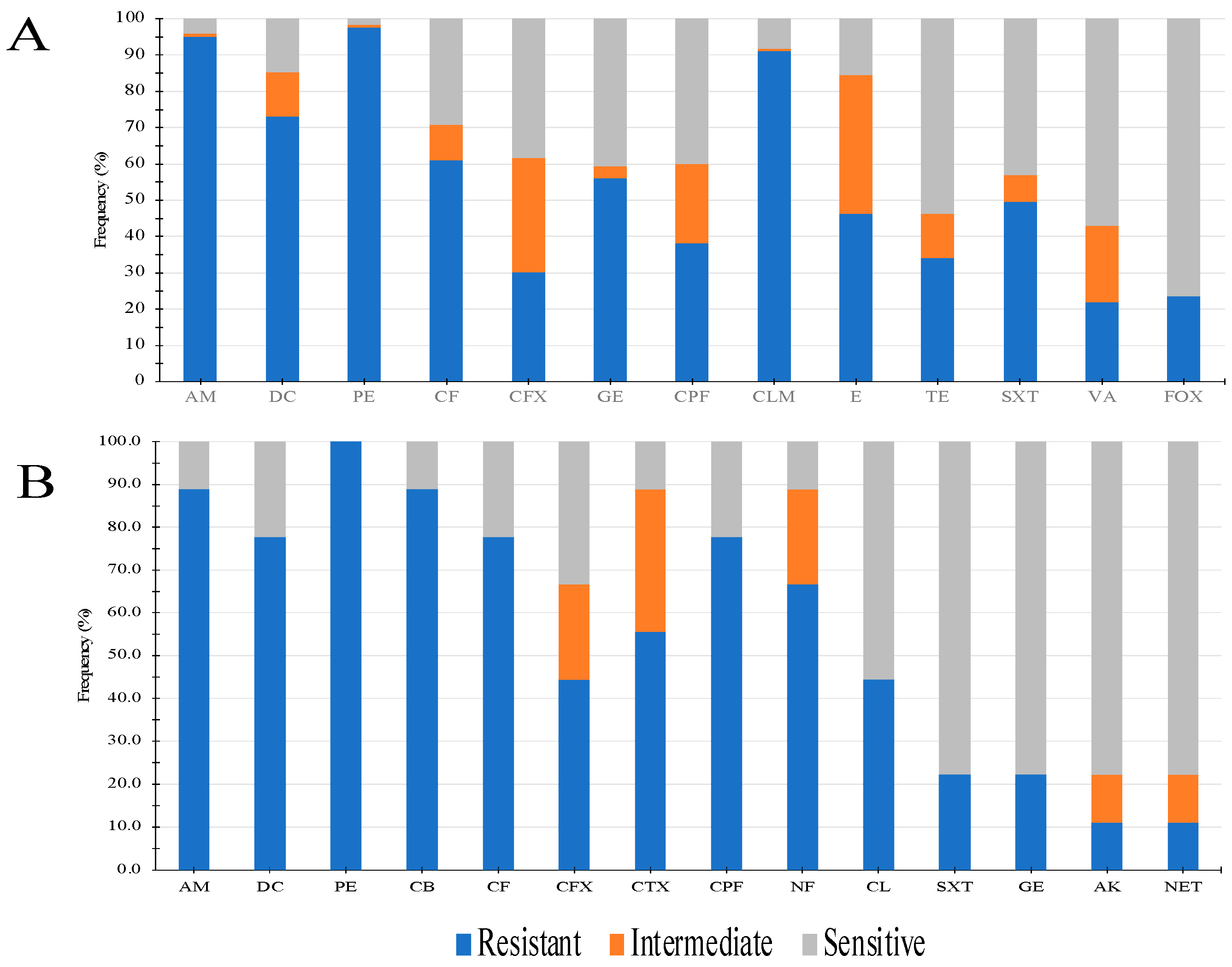
3.3. Susceptibility/Resistance Assays
3.4. mecA Gene and Mobile Genetic Element SCCmec Characterization
3.5. icaA and icaD Gene Detection and Biofilm Formation in Staphylococcus
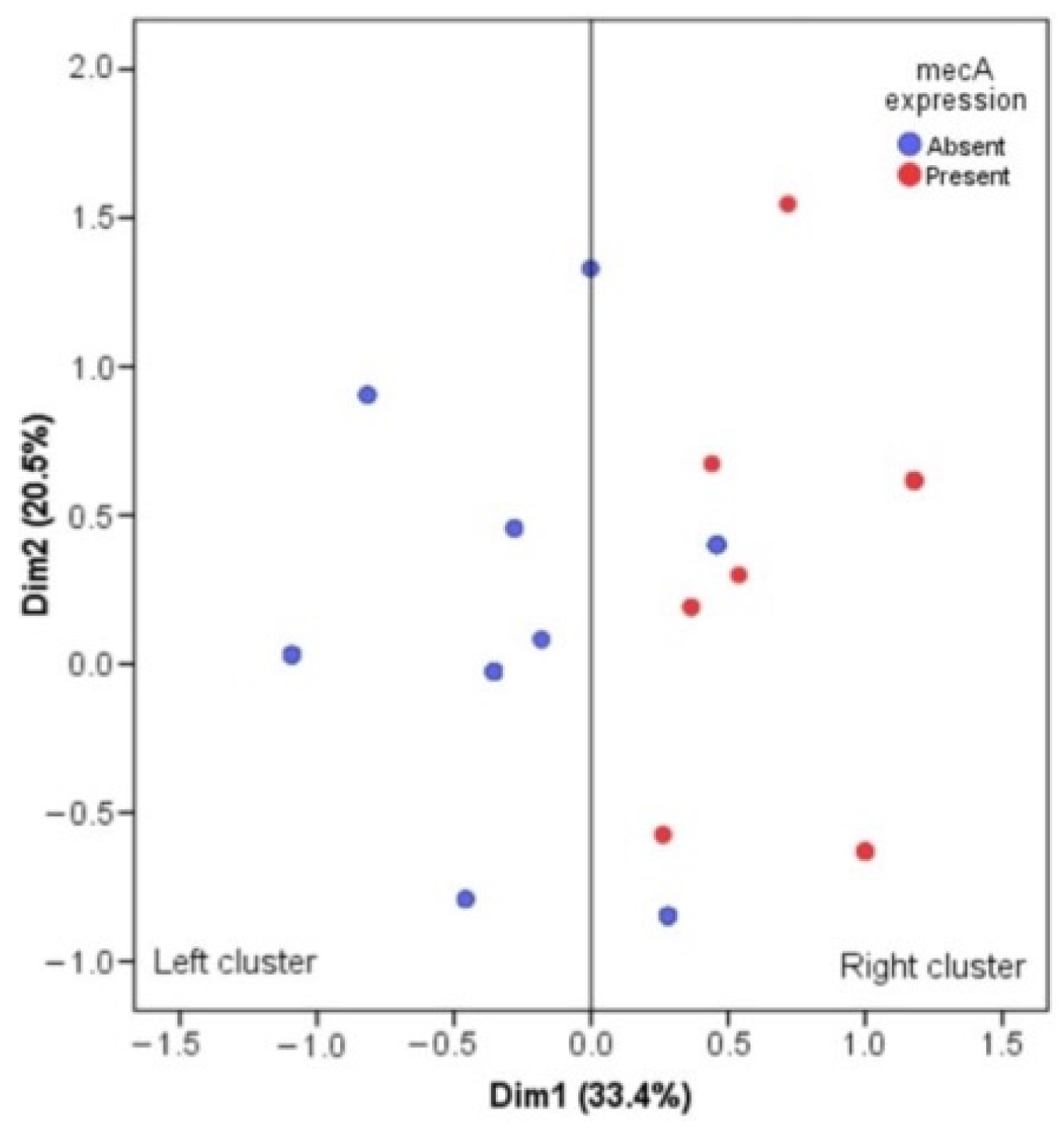
3.6. Multiple Correspondence Analysis for mecA Gene and Antimicrobial Resistance
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abroug, N.; Khairallah, M.; Zina, S.; Ksiaa, I.; Amor, H.B.; Attia, S.; Jelliti, B.; Khochtali, S.; Khairallah, M. Ocular Manifestations of Emerging Arthropod-Borne Infectious Diseases. J. Curr. Ophthalmol. 2021, 33, 227–235. [Google Scholar] [PubMed]
- Petrillo, F.; Pignataro, D.; Di Lella, F.M.; Reibaldi, M.; Fallico, M.; Castellino, N.; Parisi, G.; Trotta, M.C.; D’Amico, M.; Santella, B.; et al. Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections. Antibiotics 2021, 10, 527. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, A.A.; Ali, M.M.; Zenebe, M.H. Bacterial etiology of ocular and periocular infections, antimicrobial susceptibility profile and associated factors among patients attending eye unit of Shashemene comprehensive specialized hospital, Shashemene, Ethiopia. BMC Ophthalmol. 2020, 20, 124. [Google Scholar] [CrossRef] [PubMed]
- Astley, R.A.; Mursalin, M.H.; Coburn, P.S.; Livingston, E.T.; Nightengale, J.W.; Bagaruka, E.; Hunt, J.J.; Callegan, M.C. Ocular Bacterial Infections: A Ten-Year Survey and Review of Causative Organisms Based on the Oklahoma Experience. Microorganisms 2023, 11, 1802. [Google Scholar] [CrossRef]
- Hemavathi; Sarmah, P.; Shenoy, P. Profile of microbial isolates in ophthalmic infections and antibiotic susceptibility of the bacterial isolates: A study in an eye care hospital, Bangalore. J. Clin. Diagn. Res. 2014, 8, 23–25. [Google Scholar]
- Teweldemedhin, M.; Gebreyesus, H.; Atsbaha, A.H.; Asgedom, S.W.; Saravanan, M. Bacterial profile of ocular infections: A systematic review. BMC Ophthalmol. 2017, 17, 212. [Google Scholar] [CrossRef]
- Shimizu, Y.; Toshida, H.; Honda, R.; Matsui, A.; Ohta, T.; Asada, Y.; Murakami, A. Prevalence of drug resistance and culture-positive rate among microorganisms isolated from patients with ocular infections over a 4-year period. Clin. Ophthalmol. 2013, 7, 695–702. [Google Scholar]
- Sharma, A.; Taniguchi, J. Review: Emerging strategies for antimicrobial drug delivery to the ocular surface: Implications for infectious keratitis. Ocul. Surf. 2017, 15, 670–679. [Google Scholar] [CrossRef]
- Manente, R.; Santella, B.; Pagliano, P.; Santoro, E.; Casolaro, V.; Borrelli, A.; Capunzo, M.; Galdiero, M.; Franci, G.; Boccia, G. Prevalence and Antimicrobial Resistance of Causative Agents to Ocular Infections. Antibiotics 2022, 11, 463. [Google Scholar] [CrossRef]
- Li, J.J.; Yi, S.; Wei, L. Ocular Microbiota and Intraocular Inflammation. Front. Immunol. 2020, 23, 609765. [Google Scholar] [CrossRef]
- Xue, W.; Li, J.J.; Zou, Y.; Zou, B.; Wei, L. Microbiota and Ocular Diseases. Front. Cell Infect. Microbiol. 2021, 11, 1047. [Google Scholar] [CrossRef] [PubMed]
- Arjunan, P.; Swaminathan, R. Do oral pathogens inhabit the eye and play a role in ocular diseases? J. Clin. Med. 2022, 11, 2938. [Google Scholar] [CrossRef] [PubMed]
- Iwalokun, B.A.; Oluwadun, A.; Akinsinde, K.A.; Niemogha, M.T.; Nwaokorie, F.O. Bacteriologic and plasmid analysis of etiologic agents of conjunctivitis in Lagos, Nigeria. J. Ophthalmic Inflamm. Infect. 2011, 1, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Summaiya, M.; Neeta, K.; Sangita, R. Ocular infections: Rational approach to antibiotic therapy. Natl. J. Med. Res. 2012, 2, 22–24. [Google Scholar]
- Kaliamurthy, J.; Kalavathy, C.M.; Parmar, P.; Nelson, J.C.A.; Thomas, P.A. Spectrum of bacterial keratitis at a tertiary eye care centre in India. BioMed Res. Int. 2013, 2013, 181564. [Google Scholar] [CrossRef]
- Dias, C.; Gonçalves, M.; João, A. Epidemiological study of hospital-acquired bacterial conjunctivitis in a level III neonatal unit. Sci. World J. 2013, 2013, 163582. [Google Scholar] [CrossRef]
- Callegan, M.C.; Cochran, D.C.; Kane, S.T.; Ramadan, R.T.; Chodosh, J.; McLean, C.; Stroman, D.W. Virulence factor profiles and antimicrobial susceptibilities of ocular bacillus isolates. Curr. Eye Res. 2006, 31, 693–702. [Google Scholar] [CrossRef]
- Jayasudha, R.; Narendran, V.; Manikandan, P.; Prabagaran, S.R. Identification of polybacterial communities in patients with postoperative, posttraumatic, and endogenous endophthalmitis through 16S rRNA gene libraries. J. Clin. Microbiol. 2014, 52, 1459–1466. [Google Scholar] [CrossRef]
- Ayehubizu, Z.; Mulu, W.; Biadglegne, F. Common bacterial causes of external ocular infections, associated risk factors and antibiotic resistance among patients at ophthalmology unit of Felege Hiwot Referral Hospital, Northwest Ethiopia: A cross-sectional study. J. Ophthalmic Inflamm. Infect. 2021, 11, 7. [Google Scholar] [CrossRef]
- Haile, Z.; Mengist, H.M.; Dilnessa, T. Bacterial isolates, their antimicrobial susceptibility pattern, and associated factors of external ocular infections among patients attending eye clinic at Debre Markos Comprehensive Specialized Hospital, Northwest Ethiopia. PLoS ONE 2022, 17, e0277230. [Google Scholar] [CrossRef]
- Faridi, A.; Kareshk, A.T.; Fatahi-Bafghi, M.; Ziasistani, M.; Ghahraman, M.R.K.; Seyyed-Yousefi, S.Z.; Shakeri, N.; Kalantar-Neyestanaki, D. Detection of methicillin-resistant Staphylococcus aureus (MRSA) in clinical samples of patients with external ocular infection. Iran. J. Microbiol. 2018, 10, 215–219. [Google Scholar] [PubMed]
- Chen, Y.L.; Kang, E.Y.; Yeh, L.K.; Ma, D.H.K.; Tan, H.Y.; Chen, H.C.; Hung, K.H.; Huang, Y.C.; Hsiao, C.H. Clinical features and molecular characteristics of methicillin-susceptible Staphylococcus aureus ocular infection in Taiwan. Antibiotics 2021, 10, 1445. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standard Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing, 31st ed.; CLSI Supplement M100; CLSI: Wayne, PA, USA, 2022; ISBN 978-1-68440-105-5. [Google Scholar]
- Acosta-Pérez, G.; Rodríguez-Ábrego, G.; Longoria-Revilla, E.; Castro-Mussot, M.E. Evaluación de cuatro métodos para la detección de Staphylococcus aureus meticilino-resistente de muestras clínicas en un hospital regional. Salud Publ. Mex. 2012, 54, 1–6. [Google Scholar]
- Boye, K.; Bartels, M.D.; Andersen, I.S.; Møller, J.A.; Westh, H. A new multiplex PCR for easy screening of methicillin-resistant Staphylococcus aureus SCCmec types I-V. Clin. Microbiol. Infect. 2007, 13, 725–727. [Google Scholar] [CrossRef]
- Rohde, H.; Knobloch, J.K.; Horstkotte, M.A.; Mack, D. Correlation of Staphylococcus aureus icaADBC genotype and biofilm expression phenotype. J. Clin. Microbiol. 2001, 39, 4595–4596. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.D.; Simpson, W.A.; Younger, J.J.; Baddour, L.M.; Barrett, F.F.; Melton, D.M.; Beachey, E.H. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: A quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbiol. 1985, 22, 996–1006. [Google Scholar] [CrossRef]
- Hess, D.J.; Henry-Stanley, M.J.; Wells, C.L. Gentamicin promotes Staphylococcus aureus biofilms on silk suture. J. Surg. Res. 2011, 170, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Mukwanseke, E.; Kilangalanga, J.; Lutete, F.; Hopkins, A.; Guthoff, R.F.; Frech, S. Ocular morbidity-A critical analysis to improve outpatient services in an eye department in a Sub-Saharan megacity. J. Clin. Med. 2021, 10, 3791. [Google Scholar] [CrossRef]
- Bastola, P.; Dahal, P. Ocular Morbidity among Patients Visiting the Department of Ophthalmology during the Coronavirus Disease 2021 Pandemic at a Tertiary Care Hospital: A Descriptive Cross-sectional Study. J. Nepal Med. Assoc. 2021, 59, 1219–1224. [Google Scholar] [CrossRef]
- Putnam, C.M. Diagnosis and management of blepharitis: An optometrist’s perspective. Clin. Optom. 2016, 8, 71–78. [Google Scholar] [CrossRef]
- Dias, M.R.; Guaresch, B.L.V.; Borges, C.R.; Biazim, D.F.; Casagrande, D.; Luz, R.A. Blepharitis: Epidemiology, etiology, clinical presentations, treatment and evolution of our patients. Rev. Bras. Oftalmol. 2019, 78, 300–303. [Google Scholar]
- Junk, A.K.; Lukacs, A.; Kampik, A. Topical administration of metronidazole gel as an effective therapy alternative in chronic Demodex blepharitis—A case report. Klin. Monbl. Augenheilkd. 1998, 213, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Safonova, T.N.; Kintyukhina, N.P. Treatment of chronic posterior blepharitis after allogeneic hematopoietic stem cell transplantation (a case report). Vestn. Oftalmol. 2020, 136, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Takai, S.Y.; Yamagami, A.; Iwasa, M.; Inoue, K.; Wakakura, M. A Case of Herpes Zoster Ophthalmicus with Multiple Delayed Ocular Complications. Cureus 2023, 15, e37134. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.M.; Brown, G.C.; Sharma, S.; Hollands, H.; Landy, J. Quality of life and systemic comorbidities in patients with ophthalmic disease. Br. J. Ophthalmol. 2002, 86, 8–11. [Google Scholar] [CrossRef]
- Flores-Páez, L.A.; Zenteno, J.C.; Alcántar-Curiel, M.D.; Vargas-Mendoza, C.F.; Rodríguez-Martínez, S.; Cancino-Diaz, M.E.; Jan-Roblero, J.; Cancino-Diaz, J.C. Molecular and phenotypic characterization of Staphylococcus epidermidis isolates from healthy conjunctiva and a comparative analysis with isolates from ocular infection. PLoS ONE 2015, 10, e0135964. [Google Scholar] [CrossRef] [PubMed]
- Getahun, E.; Gelaw, B.; Assefa, A.; Assefa, Y.; Amsalu, A. Bacterial pathogens associated with external ocular infections alongside eminent proportion of multidrug resistant isolates at the University of Gondar Hospital, northwest Ethiopia. BMC Ophthalmol. 2017, 17, 151. [Google Scholar] [CrossRef]
- Juárez-Verdayes, M.A.; Reyes-López, M.A.; Cancino-Díaz, M.E.; Muñoz-Salas, S.; Rodríguez-Martínez, S.; de la Serna, F.J.; Hernández-Rodríguez, C.H.; Cancino-Díaz, J.C. Isolation, vancomycin resistance and biofilm production of Staphylococcus epidermidis from patients with conjunctivitis, corneal ulcers, and endophthalmitis. Rev. Latinoam. Microbiol. 2006, 48, 238–246. [Google Scholar]
- Chiang, M.C.; Chern, E. Ocular surface microbiota: Ophthalmic infectious disease and probiotics. Front. Microbiol. 2022, 13, 952473. [Google Scholar] [CrossRef]
- Matysiak, A.; Kabza, M.; Karolak, J.A.; Jaworska, M.M.; Rydzanicz, M.; Ploski, R.; Szaflik, J.P.; Gajecka, M. Characterization of ocular surface microbial profiles revealed discrepancies between conjunctival and corneal microbiota. Pathogens 2021, 10, 405. [Google Scholar] [CrossRef]
- Song, J.; Huang, Y.F.; Zhang, W.J.; Chen, X.F.; Guo, Y.M. Ocular diseases: Immunological and molecular mechanisms. Int. J. Ophthalmol. 2016, 9, 780–788. [Google Scholar] [PubMed]
- Martín Algarra, L.V.; Sánchez Rocha, M.C.; Roldón Correa, G.; Rodríguez, M.F. Perfil de resistencia antimicrobiana de bacterias aisladas de infecciones y de la microbiota ocular. Cienc. Tecnol. Salud Vis. Ocul. 2018, 16, 33–44. [Google Scholar] [CrossRef]
- Dang, S. Entendiendo la Resistencia de Antibióticos en Relación con Infecciones Oculares [Internet]. American Academy of Ophthalmology. 2017. Available online: https://www.aao.org/salud-ocular/noticias/resistencia-de-antibioticos-infecciones-oculares (accessed on 30 September 2023).
- González-Sotero, J.; Rojas-Álvarez, E.; Correa-Rojas, O.; Iviricu-Tielves, R. Resistencia antimicrobiana en oftalmología. Rev. Mex. Oftalmol. 2011, 85, 148–155. [Google Scholar]
- Naimi, T.S.; LeDell, K.H.; Como-Sabetti, K.; Borchardt, S.M.; Boxrud, D.J.; Etienne, J.; Johnson, S.K.; Vandenesch, F.; Fridkin, S.; O’Boyle, C.; et al. Comparison of community- and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 2003, 290, 2976–2984. [Google Scholar] [CrossRef]
- Tsuji, B.T.; Rybak, M.J.; Cheung, C.M.; Amjad, M.; Kaatz, G.W. Community- and health care-associated methicillin-resistant Staphylococcus aureus: A comparison of molecular epidemiology and antimicrobial activities of various agents. Diagn. Microbiol. Infect. Dis. 2007, 58, 41–47. [Google Scholar] [CrossRef]
- Panda, S.; Kar, S.; Choudhury, R.; Sharma, S.; Singh, D.V. Development and evaluation of hexaplex PCR for rapid detection of methicillin, cadmium/zinc and antiseptic-resistant staphylococci, with simultaneous identification of PVL-positive and -negative Staphylococcus aureus and coagulase negative staphylococci. FEMS Microbiol. Lett. 2014, 352, 114–122. [Google Scholar] [CrossRef]
- García, A.; Martínez, C.; Juárez, R.I.; Téllez, R.; Paredes, M.A.; Herrera, M.D.R.; Giono, S. Methicillin resistance and biofilm production in clinical isolates of Staphylococcus aureus and coagulase-negative Staphylococcus in México. Biomedica 2019, 39, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Omidi, M.; Firoozeh, F.; Saffari, M.; Sedaghat, H.; Zibaei, M.; Khaledi, A. Ability of biofilm production and molecular analysis of spa and ica genes among clinical isolates of methicillin-resistant Staphylococcus aureus. BMC Res. Notes 2020, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- François, P.; Schrenzel, J.; Götz, F. Biology and Regulation of Staphylococcal Biofilm. Int. J. Mol. Sci. 2023, 24, 5218. [Google Scholar] [CrossRef]
- Schechter, B.A.; Sheppard, J.D.; Sanfilippo, C.M.; DeCory, H.H.; Asbell, P.A. An evaluation of staphylococci from ocular surface infections treated empirically with topical besifloxacin: Antibiotic resistance, molecular characteristics, and clinical outcomes. Ophthalmol. Ther. 2020, 9, 159–173. [Google Scholar] [CrossRef]
- Gupta, M.; Durand, M.L.; Sobrin, L. Vancomycin resistance in ocular infections. Int. Ophthalmol. Clin. 2011, 51, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Deguchi, H.; Kitazawa, K.; Kayukawa, K.; Kondoh, E.; Fukumoto, A.; Yamasaki, T.; Kinoshita, S.; Sotozono, C. The trend of resistance to antibiotics for ocular infection of Staphylococcus aureus, coagulase-negative staphylococci, and Corynebacterium compared with 10-years previous: A retrospective observational study. PLoS ONE 2018, 13, e0203705. [Google Scholar] [CrossRef]
- Naik, A.U.; Prakash, V.J.; Susvar, P.; Therese, K.L.; Parameswari, C.K. Postoperative endophthalmitis due to Pseudomonas luteola: First reported case of acute and virulent presentation from a tertiary eye care center in South India. Indian J. Ophthalmol. 2018, 66, 1200–1202. [Google Scholar] [PubMed]
- Datta, P.; Gupta, M.; Kumari, P.; Gupta, V.; Narang, S.; Chander, J. Post-Traumatic Endophthalmitis Due to Acinetobacter radioresistens: Virulence Potential of Commensal Bacteria. Infect. Disord. Drug Targets 2020, 20, 556–558. [Google Scholar] [CrossRef]
- Carruth, B.P.; Wladis, E.J. Orbital abscess from dacryocystitis caused by Morganella morganii. Orbit 2013, 32, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Bale, B.I.; Elebesunu, E.E.; Manikavasagar, P.; Agwuna, F.O.; Ogunkola, I.O.; Sow, A.U.; Lucero-Prisno, D.E. Antibiotic resistance in ocular bacterial infections: An integrative review of ophthalmic chloramphenicol. Trop. Med. Health 2023, 51, 15. [Google Scholar] [CrossRef] [PubMed]
- Vera Vidal, V.; Suarez Olivares, A.T.; Ruiz Miranda, M.; Pascual Vera, H. Antibioticoterapia en oftalmología. Medisan 2011, 15, 1598–1608. [Google Scholar]
- Year, H.; Ok, V.; Kuet, F.L.K.; Dahane, N.; Ariey, F.; Hasseine, L.; Delaunay, P.; Martiano, D.; Marty, P.; Bourges, J.L. PCR and culture for diagnosis of Acanthamoeba keratitis. Br. J. Ophthalmol. 2021, 105, 1302–1306. [Google Scholar] [CrossRef]
- Nishiwaki-Dantas, M.C.; de Abreu, M.T.; de Melo, C.M.; Romero, I.L.; Neto, R.B.; Dantas, P.E. Direct fluorescent antibody assay and polymerase chain reaction for the detection of Chlamydia trachomatis in patients with vernal keratoconjunctivitis. Clinics 2011, 66, 2013–2018. [Google Scholar] [CrossRef]
- Sugita, S.; Takase, H.; Nakano, S. Role of Recent PCR Tests for Infectious Ocular Diseases: From Laboratory-Based Studies to the Clinic. Int. J. Mol. Sci. 2023, 24, 8146. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Primer | Molecular Target | Sequence (5′→3′) | Size (bp) | References |
|---|---|---|---|---|
| mecA plus | mecA | TGGCTATCGTGTCACAATCG | 310 | [24] |
| mecA minus | CTGGAACTTGTTGAGCAGAG | |||
| 16S plus | 16S rRNA | AGGAGGTGATCCAACCGCA | 370 | |
| 16S menos | AACTGGAAGAAGGTGGGGAT | |||
| b | ccrA2-B | ATTGCCTTGATAATAGCCYTCT | 937 | [25] |
| a | TAAAGGCATCAATGCACAAACAC | |||
| ccrCF | ccrC | CGTCTATTACAAGATGTTAAGGATAAT | 518 | |
| ccrCR | CCTTTATAGACTGGATTATTCAAAATAT | |||
| 1272F1 | IS1272 | GCCACTCATAACATATGGAA | 415 | |
| 1272R1 | CATCCGAGTGAAACCCAAA | |||
| 5RmecA | mecA-IS431 | TATACCAAACCCGACAACTAC | 359 | |
| 5R431 | CGGCTACAGTGATAACATCC | |||
| icaAF | icaA | ACACTTGCTGGCGCAGTCAA | 188 | [26] |
| icaAR | TCTGGAACCAACATCCAACA | |||
| icaDF | icaD | ATGGTCAAGCCCAGACAGAG | 900 | |
| icaDR | AGTATTTTCAATGTTTAAAGCAA |
| Sign/Symptom | n (%) | C.I. 95% |
|---|---|---|
| Asymptomatic | 6 (5.45) | (1.21–9.69) |
| Itchy | 49 (44.5) | (35.21–53.79) |
| Tearing | 7 (6.4) | (1.83–10.97) |
| Secretion | 14 (12.7) | (6.49–18.92) |
| Burning | 17 (15.5) | (8.74–22.26) |
| Decreased visual acuity | 6 (5.5) | (1.24–9.76) |
| Foreign body feeling | 29 (26.4) | (18.16–34.64) |
| Conjunctival hyperaemia | 8 (7.3) | (2.44–12.16) |
| Pain | 6 (5.5) | (1.21–9.69) |
| Others | 6 (5.5) | (1.21–9.69) |
| Comorbidities or Antecedent | n (%) | C.I. 95% |
|---|---|---|
| No comorbidities | 20 (18.2) | (10.99–25.41) |
| Diabetes mellitus type 2 | 36 (32.7) | (23.93–41.47) |
| Cancer | 11 (10.0) | (4.39–15.61) |
| Systemic arterial hypertension | 34 (30.9) | (22.26–39.54) |
| Autoimmune diseases | 17 (15.5) | (8.74–22.26) |
| Ocular surgery | 29 (26.4) | (18.16–34.64) |
| Other ocular pathologies | 41 (37.3) | (28.26–46.34) |
| Specie of Staphylococcus | mecA Gene | SCCmec n (%) | |
|---|---|---|---|
| III | IV | ||
| Staphylococcus epidermidis (n = 19) | + | 12 (63.1) | 7 (36.9) |
| Staphylococcus haemolyticus (n = 6) | + | 5 (83.3) | 1 (16.7) |
| Staphylococcus aureus (n = 3) | + | 1 (33.3) | 2 (66.6) |
| Staphylococcus warneri (n = 1) | + | 1 (100) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durán-Manuel, E.M.; Bello-López, J.M.; Salinas-Bobadilla, A.D.; Vargas-De-León, C.; Nieto-Velázquez, N.G.; Moreno-Eutimio, M.A.; Pastelin-Palacios, R.; Calzada-Mendoza, C.C.; Blanco-Hernández, D.M.R. Molecular Characterization of Bacterial Agents Causing External Ocular Infections Isolates of Patients in a Third Level Hospital. Pathogens 2023, 12, 1294. https://doi.org/10.3390/pathogens12111294
Durán-Manuel EM, Bello-López JM, Salinas-Bobadilla AD, Vargas-De-León C, Nieto-Velázquez NG, Moreno-Eutimio MA, Pastelin-Palacios R, Calzada-Mendoza CC, Blanco-Hernández DMR. Molecular Characterization of Bacterial Agents Causing External Ocular Infections Isolates of Patients in a Third Level Hospital. Pathogens. 2023; 12(11):1294. https://doi.org/10.3390/pathogens12111294
Chicago/Turabian StyleDurán-Manuel, Emilio Mariano, Juan Manuel Bello-López, Aranza Denisse Salinas-Bobadilla, Cruz Vargas-De-León, Nayeli Goreti Nieto-Velázquez, Mario Adán Moreno-Eutimio, Rodolfo Pastelin-Palacios, Claudia Camelia Calzada-Mendoza, and Dulce Milagros Razo Blanco-Hernández. 2023. "Molecular Characterization of Bacterial Agents Causing External Ocular Infections Isolates of Patients in a Third Level Hospital" Pathogens 12, no. 11: 1294. https://doi.org/10.3390/pathogens12111294
APA StyleDurán-Manuel, E. M., Bello-López, J. M., Salinas-Bobadilla, A. D., Vargas-De-León, C., Nieto-Velázquez, N. G., Moreno-Eutimio, M. A., Pastelin-Palacios, R., Calzada-Mendoza, C. C., & Blanco-Hernández, D. M. R. (2023). Molecular Characterization of Bacterial Agents Causing External Ocular Infections Isolates of Patients in a Third Level Hospital. Pathogens, 12(11), 1294. https://doi.org/10.3390/pathogens12111294