

Dementia Prevalence and Onchocerca volvulus Infection among Rural Elderly Persons in the Ntui Health District, Cameroon: A Population-Based Study
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population and Sampling
2.3. Data Collection Tools
2.3.1. Cognitive Assessment
2.3.2. Sleep Assessment
2.4. Study Procedures
2.5. Data Management and Analysis
2.6. Ethical Considerations
3. Results
3.1. Participant Characteristics
3.2. Clinical Findings in Participants
3.2.1. Overall Clinical Findings
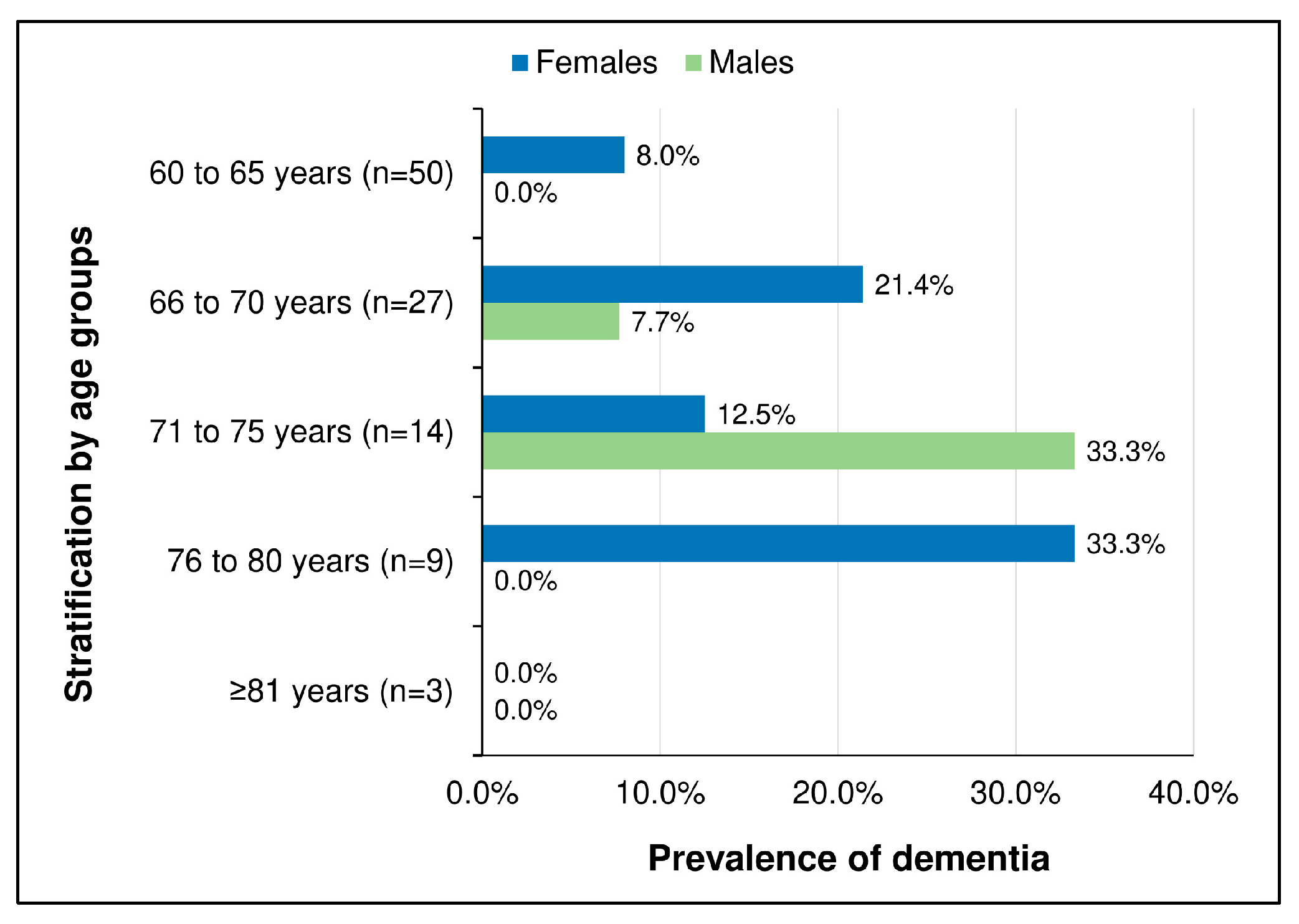
3.2.2. Prevalence of Dementia
3.3. Factors Associated with CSID Cognitive Score
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Bank. World Bank Open Data. Available online: https://data.worldbank.org/country/ZG (accessed on 15 April 2023).
- Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 25 January 2023).
- Jorm, A.F.; Jolley, D. The Incidence of Dementia: A Meta-Analysis. Neurology 1998, 51, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Wimo, A.; Aboderin, I.; Guerchet, M.; Prince, M.; Amoakoh-Coleman, M.; Ezeah, P.; Lloyd-Sherlock, P.; Uwakwe, R.; Mayston, R.; Akinyemi, R.; et al. Dementia in Sub-Saharan Africa: Challenges and Opportunities. Ph.D. Thesis, Alzheimer’s Disease International, Quincy, MA, USA, 2017. [Google Scholar]
- Mavrodaris, A.; Powell, J.; Thorogood, M. Prevalences of Dementia and Cognitive Impairment among Older People in Sub-Saharan Africa: A Systematic Review. Bull. World Health Organ. 2013, 91, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.; Maestre, G.; Mahinrad, S.; Acosta, D.M.; Akinyemi, R.O.; Alladi, S.; Allegri, R.F.; Arshad, F.; Babalola, D.O.; Baiyewu, O.; et al. The 2022 Symposium on Dementia and Brain Aging in Low- and Middle-income Countries: Highlights on Research, Diagnosis, Care, and Impact. Alzheimer’s Dement. 2024, 20, 4290–4314. [Google Scholar] [CrossRef] [PubMed]
- Maestre, G.; Carrillo, M.; Kalaria, R.; Acosta, D.; Adams, L.; Adoukonou, T.; Akinwande, K.; Akinyemi, J.; Akinyemi, R.; Akpa, O.; et al. The Nairobi Declaration—Reducing the Burden of Dementia in Low- and Middle-income Countries (LMICs): Declaration of the 2022 Symposium on Dementia and Brain Aging in LMICs. Alzheimer’s Dement. 2023, 19, 1105–1108. [Google Scholar] [CrossRef] [PubMed]
- Tianyi, F.L.; Agbor, V.N.; Njamnshi, A.K.; Atashili, J. Factors Associated with the Prevalence of Cognitive Impairment in a Rural Elderly Cameroonian Population: A Community-Based Study in Sub-Saharan Africa. Dement. Geriatr. Cogn. Disord. 2019, 47, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Guerchet, M.; M’belesso, P.; Mouanga, A.M.; Bandzouzi, B.; Tabo, A.; Houinato, D.S.; Paraïso, M.N.; Cowppli-Bony, P.; Nubukpo, P.; Aboyans, V.; et al. Prevalence of Dementia in Elderly Living in Two Cities of Central Africa: The EDAC Survey. Dement. Geriatr. Cogn. Disord. 2010, 30, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Njamnshi, A.K.; Djientcheu, V.d.P.; Fonsah, J.Y.; Yepnjio, F.N.; Njamnshi, D.M.; Muna, W.F. The International HIV Dementia Scale Is a Useful Screening Tool for HIV-Associated Dementia/Cognitive Impairment in HIV-Infected Adults in Yaoundé-Cameroon. JAIDS J. Acquir. Immune Defic. Syndr. 2008, 49, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Kanmogne, G.D.; Kuate, C.T.; Cysique, L.A.; Fonsah, J.Y.; Eta, S.; Doh, R.; Njamnshi, D.M.; Nchindap, E.; Franklin, D.R.; Ellis, R.J.; et al. HIV-Associated Neurocognitive Disorders in Sub-Saharan Africa: A Pilot Study in Cameroon. BMC Neurol. 2010, 10, 60. [Google Scholar] [CrossRef] [PubMed]
- Njamnshi, A.K.; Zoung-Kanyi Bissek, A.C.; Ongolo-Zogo, P.; Tabah, E.N.; Lekoubou, A.Z.; Yepnjio, F.N.; Fonsah, J.Y.; Kuate, C.T.; Angwafor, S.A.; Dema, F.; et al. Risk Factors for HIV-Associated Neurocognitive Disorders (HAND) in Sub-Saharan Africa: The Case of Yaoundé-Cameroon. J. Neurol. Sci. 2009, 285, 149–153. [Google Scholar] [CrossRef]
- Kanmogne, G.D.; Fonsah, J.Y.; Tang, B.; Doh, R.F.; Kengne, A.M.; Umlauf, A.; Tagny, C.T.; Nchindap, E.; Kenmogne, L.; Franklin, D.; et al. Effects of HIV on Executive Function and Verbal Fluency in Cameroon. Sci. Rep. 2018, 8, 17794. [Google Scholar] [CrossRef]
- Kanmogne, G.D.; Fonsah, J.Y.; Umlauf, A.; Moul, J.; Doh, R.F.; Kengne, A.M.; Tang, B.; Tagny, C.T.; Nchindap, E.; Kenmogne, L.; et al. Attention/Working Memory, Learning and Memory in Adult Cameroonians: Normative Data, Effects of HIV Infection and Viral Genotype. J. Int. Neuropsychol. Soc. 2020, 26, 607–623. [Google Scholar] [CrossRef] [PubMed]
- Kanmogne, G.D.; Fonsah, J.Y.; Umlauf, A.; Moul, J.; Doh, R.F.; Kengne, A.M.; Tang, B.; Tagny, C.T.; Nchindap, E.; Kenmogne, L.; et al. Effects of HIV Infection, Antiretroviral Therapy, and Immune Status on the Speed of Information Processing and Complex Motor Functions in Adult Cameroonians. Sci. Rep. 2020, 10, 14016. [Google Scholar] [CrossRef]
- Sipilä, P.N.; Heikkilä, N.; Lindbohm, J.V.; Hakulinen, C.; Vahtera, J.; Elovainio, M.; Suominen, S.; Väänänen, A.; Koskinen, A.; Nyberg, S.T.; et al. Hospital-Treated Infectious Diseases and the Risk of Dementia: A Large, Multicohort, Observational Study with a Replication Cohort. Lancet Infect. Dis. 2021, 21, 1557–1567. [Google Scholar] [CrossRef]
- Chesnais, C.B.; Nana-Djeunga, H.C.; Njamnshi, A.K.; Lenou-Nanga, C.G.; Boullé, C.; Bissek, A.-C.Z.-K.; Kamgno, J.; Colebunders, R.; Boussinesq, M. The Temporal Relationship between Onchocerciasis and Epilepsy: A Population-Based Cohort Study. Lancet Infect. Dis. 2018, 18, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Siewe Fodjo, J.N.; Njamnshi, W.Y.; Ngarka, L.; Nfor, L.N.; Ayuk, C.; Mundih, N.N.; Ekwoge, H.T.; Nganchfu, K.; Njamnshi, K.G.; Yerema, R.; et al. Association Between Ov16 Seropositivity and Neurocognitive Performance Among Children in Rural Cameroon: A Pilot Study. J. Pediatr. Neuropsychol. 2021, 7, 192–202. [Google Scholar] [CrossRef]
- Chesnais, C.B.; Bizet, C.; Campillo, J.T.; Njamnshi, W.Y.; Bopda, J.; Nwane, P.; Pion, S.D.; Njamnshi, A.K.; Boussinesq, M. A Second Population-Based Cohort Study in Cameroon Confirms the Temporal Relationship between Onchocerciasis and Epilepsy. Open Forum Infect. Dis. 2020, 7, ofaa206. [Google Scholar] [CrossRef]
- Brattig, N.W.; Cheke, R.A.; Garms, R. Onchocerciasis (River Blindness)—More than a Century of Research and Control. Acta Trop. 2021, 218, 105677. [Google Scholar] [CrossRef]
- Njamnshi, A.K.; Bissek, A.-C.Z.-K.; Etya’ale, D. Onchocerciasis: Neurological Involvement. In Neglected Tropical Diseases and Conditions of the Nervous System; Bentivoglio, M., Cavalheiro, E.A., Kristensson, K., Patel, N.B., Eds.; Springer: New York, NY, USA, 2014; pp. 147–164. ISBN 978-1-4614-8099-0. [Google Scholar]
- Hotterbeekx, A.; Namale Ssonko, V.; Oyet, W.; Lakwo, T.; Idro, R. Neurological Manifestations in Onchocerca Volvulus Infection: A Review. Brain Res. Bull. 2019, 145, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Colebunders, R.; Njamnshi, A.K.; Menon, S.; Newton, C.R.; Hotterbeekx, A.; Preux, P.-M.; Hopkins, A.; Vaillant, M.; Siewe Fodjo, J.N. Onchocerca Volvulus and Epilepsy: A Comprehensive Review Using the Bradford Hill Criteria for Causation. PLoS Negl. Trop. Dis. 2021, 15, e0008965. [Google Scholar] [CrossRef]
- World Health Organization. Elimination of Human Onchocerciasis: Progress Report, 2022–2023; Weekly Epidemiological Record; WHO: Geneva, Switzerland, 2023; pp. 572–582.
- Siewe Fodjo, J.N.; Ngarka, L.; Njamnshi, W.Y.; Enyong, P.A.; Zoung-Kanyi Bissek, A.-C.; Njamnshi, A.K. Onchocerciasis in the Ntui Health District of Cameroon: Epidemiological, Entomological and Parasitological Findings in Relation to Elimination Prospects. Parasites Vectors 2022, 15, 444. [Google Scholar] [CrossRef]
- Kuete, T.; Mbuagbaw, J.; Kollo, B.; Kitobo, E.; Same-Ekobo, A. Distribution Des Filarioses Dans Une Zone de Transition Savane-Forêt Du Cameroun, Impact Sur La Prise En Charge: Cas de l’Aire de Santé de Ntui, Département Du Mbam et Kim. J. Cameroon Acad. Sci. 2009, 8, 11–16. [Google Scholar]
- Makou Tsapi, E.; Guemgne Togjom, F.; Gamago, G.-A.; Wabo Pone, J.; Djuikwo Teukeng, F.F. Prevalence of Onchocerciasis after Seven Years of Continuous Community-Directed Treatment with Ivermectin in the Ntui Health District, Centre Region, Cameroon. Pan. Afr. Med. J. 2020, 36, 180. [Google Scholar] [CrossRef] [PubMed]
- Ngarka, L.; Siewe Fodjo, J.N.; Ambomatei, C.; Njamnshi, W.Y.; Taryunyu Njamnshi, J.N.; Nfor, L.N.; Mengnjo, M.K.; Njamnshi, A.K. Epidemiology of Epilepsy and Relationship with Onchocerciasis Prevalence in Villages of the Ntui Health District of Cameroon. Epilepsy Behav. 2023, 142, 109184. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.S.; Ogunniyi, A.O.; Hendrie, H.C.; Osuntokun, B.O.; Hui, S.L.; Musick, B.S.; Rodenberg, C.A.; Unverzagt, F.W.; Guerje, O.; Baiyewu, O. A Cross-cultural Community-Based Study of Dementias: Methods and Performance of the Survey Instrument, Indianapolis, USA., and Ibadan, Nigeria. Int. J. Methods Psychiatr. Res. 1996, 6, 129–142. [Google Scholar] [CrossRef]
- Hall, K.S.; Gao, S.; Emsley, C.L.; Ogunniyi, A.O.; Morgan, O.; Hendrie, H.C. Community Screening Interview for Dementia (CSID); Performance in Five Disparate Study Sites. Int. J. Geriatr. Psychiatry 2000, 15, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Kerodal, A.G.; Jewell, L.M.; Kent-Wilkinson, A.; Peacock, S.; O’Connell, M.; Wormith, J.S. Modifying the Community Screening Instrument for Dementia (CSID) for an Institutional Setting; Centre for Forensic Behavioural Science and Justice Studies, University of Saskatchewan: Saskatoon, SK, Canada, 2020. [Google Scholar]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh Sleep Quality Index as a Screening Tool for Sleep Dysfunction in Clinical and Non-Clinical Samples: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Azzam, D.; Ronquillo, Y. Snellen Chart. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Beam, C.R.; Kaneshiro, C.; Jang, J.Y.; Reynolds, C.A.; Pedersen, N.L.; Gatz, M. Differences Between Women and Men in Incidence Rates of Dementia and Alzheimer’s Disease. J. Alzheimers Dis. 2018, 64, 1077–1083. [Google Scholar] [CrossRef]
- Musyimi, C.W.; Ndetei, D.M.; Muyela, L.A.; Masila, J.; Farina, N. Dementia Screening in Rural Kenya: The Prevalence and Impact of Screening Positive for Dementia. Neuroepidemiology 2024, 58, 174–181. [Google Scholar] [CrossRef]
- Venketasubramanian, N. A Comparative Study of Three Dementia Screening Instruments (CSI-D, CMMSE, and ECAQ) in a Multi-Ethnic Asian Population. Healthcare 2024, 12, 410. [Google Scholar] [CrossRef]
- Njamnshi, A.K.; Mengnjo, M.K.; Mbong, E.N.; Chokote, E.T.; Nfor, L.N.; Ngarka, L.; Kingue, S. Sleep Patterns and Risk of Cognitive Impairment in Hypertensive Patients in Yaounde, Cameroon, Sub-Saharan Africa. J. Neurol. Sci. 2015, 357, e97. [Google Scholar] [CrossRef]
- Callixte, K.-T.; Clet, T.B.; Jacques, D.; Faustin, Y.; François, D.J.; Maturin, T.-T. The Pattern of Neurological Diseases in Elderly People in Outpatient Consultations in Sub-Saharan Africa. BMC Res. Notes 2015, 8, 159. [Google Scholar] [CrossRef] [PubMed]
- Kengne, A.P.; Dzudie, A.; Dongmo, L. Epidemiological Features of Degenerative Brain Diseases as They Occurred in Yaounde Referral Hospitals over a 9-Year Period. Neuroepidemiology 2006, 27, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Atashili, J.; Gaynes, B.N.; Pence, B.W.; Tayong, G.; Kats, D.; O’donnell, J.K.; Ndumbe, P.M.; Njamnshi, A.K. Prevalence, Characteristics and Correlates of a Positive-Dementia Screen in Patients on Antiretroviral Therapy in Bamenda, Cameroon: A Cross-Sectional Study. BMC Neurol. 2013, 13, 86. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Espinosa, I.; Díaz-Orueta, U. Cognitive Screening Instruments for Older Adults with Low Educational and Literacy Levels: A Systematic Review. J. Appl. Gerontol. 2022, 41, 1222–1231. [Google Scholar] [CrossRef] [PubMed]
- Idro, R.; Ogwang, R.; Anguzu, R.; Akun, P.; Ningwa, A.; Abbo, C.; Giannoccaro, M.P.; Kubofcik, J.; Mwaka, A.D.; Nakamya, P.; et al. Doxycycline for the Treatment of Nodding Syndrome: A Randomised, Placebo-Controlled, Phase 2 Trial. Lancet Glob. Health 2024, 12, e1149–e1158. [Google Scholar] [CrossRef] [PubMed]
- Njamnshi, A.; Agbor, C.A.; Mah, E.; Ngarka, L.; Angwafor, S.; Njamnshi, W.Y.; Nfor, L.; Tabah, E.; Sayong, P.; Ruffieux, N.; et al. Neurocognitive Impairment and Epilepsy in School-Aged Children after Severe Malaria in a Malaria Endemic Area. J. Neurol. Sci. 2021, 429, 118933. [Google Scholar] [CrossRef]
- Siewe Fodjo, J.N.; Yembe, W.N.; Ngarka, L.; Taryunyu, J.N.N.; Domche, A.; Kongnyu, A.N. PA-35 ”Slash and Clear” as an Effective Vector Control Technique for Onchocerciasis in Cameroon. In Proceedings of the Abstracts of the EDCTP 11th Forum 2023, Paris, France, 7–10 November 2023; BMJ Global Health: Paris, France, 2023; Volume 8. [Google Scholar]
- Siewe Fodjo, J.N.; Ekukole, S.; Njamnshi, J.T.; Njamnshi, W.Y.; Njamnshi, K.G.; Ngarka, L.; Njamnshi, A.K. Community Perceptions of Blackfly Nuisance and Acceptability of the “Slash and Clear” Vector Control Approach in the Ntui Health District of Cameroon: A Qualitative Study. Int. J. Environ. Res. Public Health 2024, 21, 658. [Google Scholar] [CrossRef] [PubMed]
- Domche, A.; Nana Djeunga, H.C.; Nwane, P.B.; Njitchouang, G.R.; Nono Fesuh, B.; Njiokou, F.; Jacob, B.; Pion, S.D.; Kamgno, J. Significant Reduction of Blackfly Densities in Persistent Onchocerciasis Area following Pilot Implementation of an Environment Friendly Approach (Slash and Clear). Sci. Rep. 2024, 14, 408. [Google Scholar] [CrossRef]
- Otuyama, L.J.; Oliveira, D.; Locatelli, D.; Machado, D.d.A.; Noto, A.R.; Galduróz, J.C.F.; Prince, M.J.; Ferri, C.P. Tobacco Smoking and Risk for Dementia: Evidence from the 10/66 Population-Based Longitudinal Study. Aging Ment. Health 2020, 24, 1796–1806. [Google Scholar] [CrossRef]
- Chimbala, L.; Nabuzoka, D.; Paul, R. Factors Associated with Snuff Usage and Its Neurocognitive Effects among Women in Ndola Urban, Zambia. Med. J. Zamb. 2020, 47, 25–32. [Google Scholar]
- Hajat, C.; Stein, E.; Ramstrom, L.; Shantikumar, S.; Polosa, R. The Health Impact of Smokeless Tobacco Products: A Systematic Review. Harm. Reduct. J. 2021, 18, 123. [Google Scholar] [CrossRef] [PubMed]
- Sreedharan, S.; Kamath, M.P.; Khadilkar, U.; Hegde, M.C.; Kumar, R.M.; Mudunuri, R.R.; Tripuraneni, S.C. Effect of Snuff on Nasal Mucosa. Am. J. Otolaryngol. 2005, 26, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, K.; Husain, S.; Vidyasagaran, A.; Readshaw, A.; Mishu, M.P.; Sheikh, A. Global Burden of Disease Due to Smokeless Tobacco Consumption in Adults: An Updated Analysis of Data from 127 Countries. BMC Med. 2020, 18, 222. [Google Scholar] [CrossRef] [PubMed]
- Spira, A.P.; Chen-Edinboro, L.P.; Wu, M.N.; Yaffe, K. Impact of Sleep on the Risk of Cognitive Decline and Dementia. Curr. Opin. Psychiatry 2014, 27, 478–483. [Google Scholar] [CrossRef]
- Njamnshi, A.K.; Hiag, A.B.; Mbanya, J.C. From Research to Policy: The Development of a National Diabetes Control Programme in Cameroon. Diabetes Voice 2006, 51, 18–21. [Google Scholar]
- World Health Organization. Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders 2022–2031. Available online: https://www.who.int/publications/m/item/intersectoral-global-action-plan-on-eepilepsy-and-other-neurological-disorders-2022-2031 (accessed on 15 April 2023).


{kind=link}
{kind=link}
| Characteristics | Findings |
|---|---|
| All participants: n (%) | 103 (100%) |
| Village: n (%) | |
| Ehondo | 7 (6.8%) |
| Essougli | 30 (29.1%) |
| Nachtigal | 39 (37.9%) |
| Ndjame | 27 (26.2%) |
| Age: mean (standard deviation) | 67.0 (6.1) |
| Sex: n (%) | |
| Female | 54 (52.4%) |
| Male | 49 (47.6%) |
| Profession: n (%) | |
| Farmer | 94 (91.3%) |
| Housewife | 5 (4.85%) |
| Business | 2 (1.9%) |
| Construction | 2 (1.9%) |
| Education level: n (%) | |
| None | 13 (12.6%) |
| Primary, incomplete | 60 (58.3%) |
| Primary, completed | 23 (22.3%) |
| Secondary | 7 (6.8%) |
| Marital status: n (%) | |
| Married | 60 (58.3%) |
| Divorced/Widowed | 38 (36.9%) |
| Single | 5 (4.9%) |
| History of alcohol consumption: n (%) | 79 (76.7%) |
| History of tobacco consumption: n (%) | |
| Smoking cigarettes | 13 (12.6%) |
| Inhaling tobacco powder | 17 (16.5%) |
| None of the above | 73 (70.9%) |
| History of illicit drugs use: n (%) | 0 (0%) |
| Known to have hypertension: n (%) | 27 (26.2%) |
| Known to have epilepsy: n (%) | 0 (0%) |
| Known to have diabetes: n (%) | 0 (0%) |
| Known history of stroke: n (%) | 2 (1.9%) |
| Clinical Characteristics | Findings | N * |
|---|---|---|
| Body Mass Index: mean (SD) | 22.7 (4.4) | 103 |
| Systolic blood pressure: mean (SD) | 139 (26.3) | 103 |
| Diastolic blood pressure: mean (SD) | 82.1 (17.4) | 103 |
| Palpable nodules: n (%) | 13 (12.6%) | 103 |
| Itching: n (%) | 75 (72.8%) | 103 |
| Depigmentation: n (%) | 5 (4.9%) | 103 |
| Snellen’s score for visual acuity: mean (SD) | 5.67 (2.8) | 91 |
| Sleep quality | 84 | |
| Good Sleep, PSQI score ≤ 5: n (%) | 54 (64.3%) | |
| Poor Sleep, PSQI score > 5: n (%) | 30 (35.7%) | |
| Positive skin snips: n (%) | 15 (17.9%) | 84 |
| Microfilarial load in positive skin snips: Mean (SD) | 14.1 (19.6) | 15 |
| Ov16 seropositivity: n (%) | 41 (62.1%) | 66 |
| Exposed | Unexposed | p-Value | n | |
|---|---|---|---|---|
| Using skin snip positivity only for onchocerciasis exposure | ||||
| Participants with dementia (CSID ≤ 29.5): n (%) | 3/15 (20.0%) | 6/69 (8.7%) | 0.198 | 84 |
| Participants without dementia (CSID > 29.5): n (%) | 12/15 (80.0%) | 63/69 (91.3%) | ||
| CSID score: Mean (Standard Deviation) | 36.2 (8.0) | 38.6 (7.6%) | 0.303 | 84 |
| Using Ov16 seropositivity only for onchocerciasis exposure | ||||
| Participants with dementia (CSID ≤ 29.5): n (%) | 5/41 (12.2%) | 1/25 (4.0%) | 0.396 | 66 |
| Participants without dementia (CSID > 29.5): n (%) | 36/41 (87.8%) | 24/25 (96.0%) | ||
| CSID score: Mean (Standard Deviation) | 37.7 (7.8) | 40.0 (7.8) | 0.259 | 66 |
| Using skin snips positivity and/or Ov16 serolopositivity for onchocerciasis exposure | ||||
| Participants with dementia (CSID ≤ 29.5): n (%) | 6/46 (13.0%) | 4/49 (8.2%) | 0.516 | 95 |
| Participants without dementia (CSID > 29.5): n (%) | 40/46 (87.0%) | 45/49 (91.8%) | ||
| CSID score: Mean (Standard Deviation) | 37.6 (7.7) | 39.3 (7.9) | 0.289 | 95 |
| Model * Covariates | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Positive skin snip | −3.399 (−6.805 to 0.007) | 0.055 |
| Age | 0.005 (−0.213 to 0.223) | 0.964 |
| Male sex | 4.775 (1.997 to 7.553) | 0.001 |
| Education | ||
| None | Reference | |
| Primary, incomplete | 3.565 (−0.742 to 7.871) | 0.109 |
| Primary, complete | 4.498 (−0.2153 to 9.212) | 0.066 |
| Secondary | 8.654 (2.0870 to 15.222) | 0.012 |
| Body mass index | 0.130 (−0.1434 to 0.404) | 0.354 |
| Visual acuity (Snellen score) | 1.122 (0.644 to 1.600) | <0.001 |
| Poor sleep quality (PQSI > 5) | 1.828 (−0.828 to 4.485) | 0.182 |
| Alcohol consumption | 0.369 (−2.910 to 3.647) | 0.826 |
| Tobacco consumption | ||
| No | Reference | |
| Inhaled tobacco | −5.441 (−9.137 to −1.744) | 0.005 |
| Cigarettes | −0.596 (−4.5005 to 3.308) | 0.766 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Njamnshi, W.Y.; Siewe Fodjo, J.N.; Njamnshi, K.G.; Ngarka, L.; Mengnjo, M.K.; Nfor, L.N.; Tsasse, M.A.F.; Njamnshi, J.N.T.; Maestre, G.; Cavazos, J.E.; et al. Dementia Prevalence and Onchocerca volvulus Infection among Rural Elderly Persons in the Ntui Health District, Cameroon: A Population-Based Study. Pathogens 2024, 13, 568. https://doi.org/10.3390/pathogens13070568
Njamnshi WY, Siewe Fodjo JN, Njamnshi KG, Ngarka L, Mengnjo MK, Nfor LN, Tsasse MAF, Njamnshi JNT, Maestre G, Cavazos JE, et al. Dementia Prevalence and Onchocerca volvulus Infection among Rural Elderly Persons in the Ntui Health District, Cameroon: A Population-Based Study. Pathogens. 2024; 13(7):568. https://doi.org/10.3390/pathogens13070568
Chicago/Turabian StyleNjamnshi, Wepnyu Yembe, Joseph Nelson Siewe Fodjo, Kongnyu Gamnsi Njamnshi, Leonard Ngarka, Michel K. Mengnjo, Leonard N. Nfor, Martine A. F. Tsasse, Julius N. Taryunyu Njamnshi, Gladys Maestre, Jose E. Cavazos, and et al. 2024. "Dementia Prevalence and Onchocerca volvulus Infection among Rural Elderly Persons in the Ntui Health District, Cameroon: A Population-Based Study" Pathogens 13, no. 7: 568. https://doi.org/10.3390/pathogens13070568