
Crimean-Congo Hemorrhagic Fever Virus: An Emerging Threat in Europe with a Focus on Epidemiology in Spain



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Documentary Sources
2.3. Used Descriptors
2.4. Selection Criteria
3. Characteristics of the Crimean Congo Hemorrhagic Fever Virus
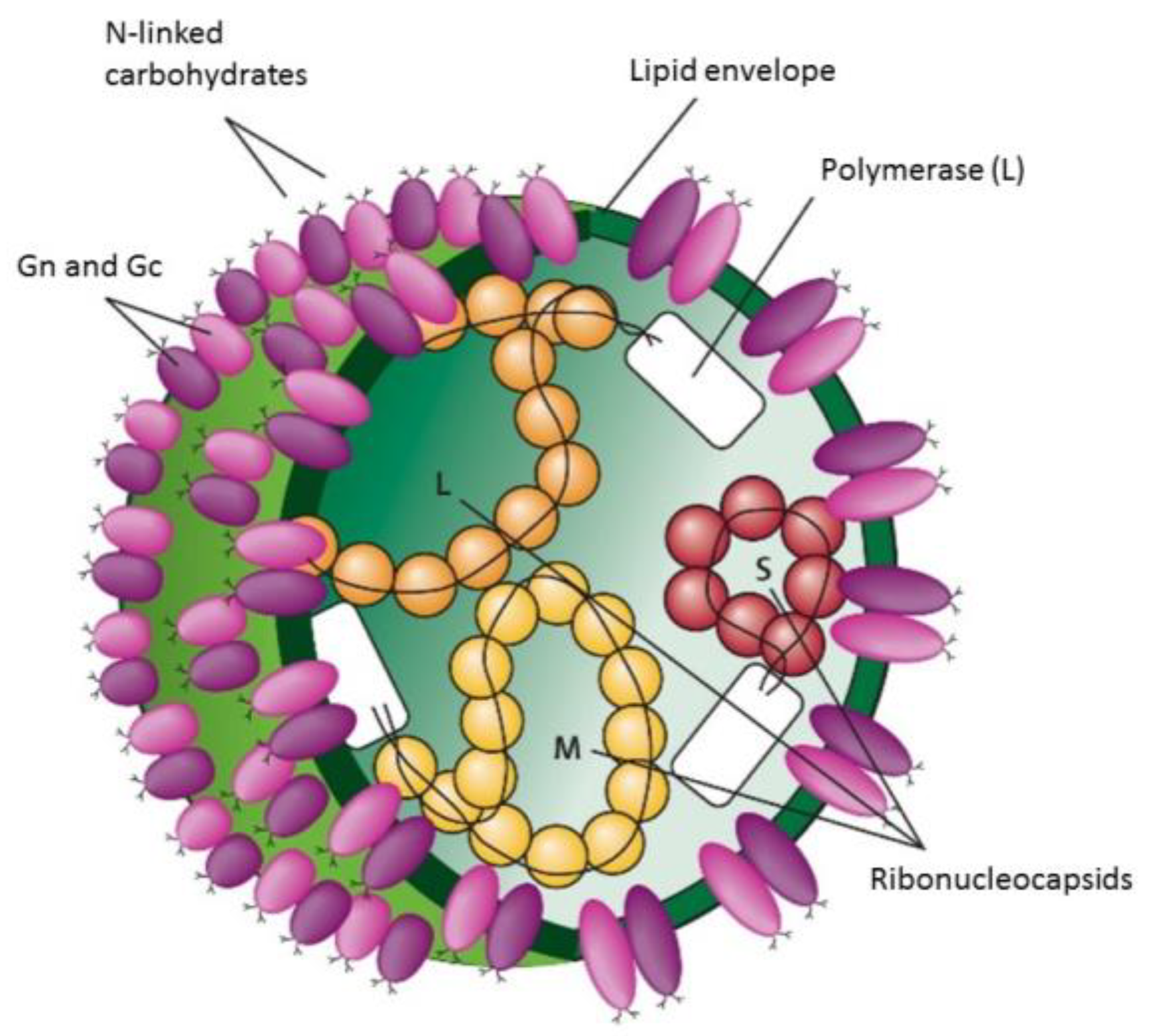
3.1. Structure
3.2. Genetics
4. Epidemiology
- a.
- Bulgaria
- b.
- Hungary
- c.
- Greece
- d.
- United Kingdom
- e.
- Sweden
- f.
- France
- g.
- Germany
- h.
- Italy
Epidemiology in Spain
5. Pathogenicity
6. Diagnosis of Crimean-Congo Hemorrhagic Fever Virus Infection
- Cell Culture
- Antibody Detection
- Molecular Methods
7. Treatment and Prevention
7.1. Treatment
7.2. Prevention
8. Discussion
9. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Ergönül, O. Crimean-Congo haemorrhagic fever. Lancet Infect Dis. 2006, 6, 203–214. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Crimean-Congo Haemorrhagic Fever. 2022. Available online: https://www.who.int/es/news-room/fact-sheets/detail/crimean-congo-haemorrhagic-fever (accessed on 10 February 2024).
- Negredo, A.; de la Calle-Prieto, F.; Palencia-Herrejón, E.; Mora-Rillo, M.; Astray-Mochales, J.; Sánchez-Seco, M.P.; Lopez, E.B.; Menárguez, J.; Fernández-Cruz, A.; Sánchez-Artola, B.; et al. Autochthonous Crimean–Congo Hemorrhagic Fever in Spain. N. Engl. J. Med. 2017, 377, 154–161. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Andonova, L.; Andraghetti, R.; Bouloy, M.; Ergonul, O.; Jongejan, F.; Kalvatchev, N.; Nichol, S.; Niedrig, M.; Platonov, A.; et al. Crimean-Congo hemorrhagic fever in Europe: Current situation calls for preparedness. Euro Surveill. 2010, 15, 19504. [Google Scholar] [CrossRef]
- Febrer-Sendra, B.; Fernández-Soto, P.; García-Bernalt Diego, J.; Crego-Vicente, B.; Negredo, A.; Muñor-Bellido, J.L.; Belhassen-García, M.; Sánchez-Seco, M.P.; Muro, A. A Novel RT-LAMP for the Detection of Different Genotypes of Crimean–Congo Haemorrhagic Fever Virus in Patients from Spain. Int. J. Mol. Sci. 2023, 24, 6411. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.J.; Vincent, M.J.; Nichol, S.T. Characterization of the Glycoproteins of Crimean-Congo Haemorrhagic Fever Virus. J. Virol. 2002, 76, 7263–7275. [Google Scholar] [CrossRef] [PubMed]
- Ramírez de Arellano, E.; Hernández, L.; Goyanes, M.J.; Arsuaga, M.; Fernández Cruz, A.; Negredo, A.; Sánchez-Seco, M.P. Phylogenetic characterization of Crimean-Congo hemorrhagic fever virus, Spain. Emerg. Infect. Dis. 2017, 23, 2078–2080. [Google Scholar] [CrossRef]
- Monsalve Arteaga, L.; Muñoz Bellido, J.L.; Negredo, A.I.; García Criado, J.; Vieira Lista, M.C.; Sánchez Serrano, J.Á.; Santiago, M.B.V.; Bernús, A.L.; de Ory Manchón, F.; Seco, M.P.S.; et al. New circulation of genotype V of Crimean-Congo haemorrhagic fever virus in humans from Spain. PLoS Negl. Trop. Dis. 2021, 15, e0009197. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Crimean-Congo haemorrhagic fever infection. In Annual Epidemiological Report for 2021; ECDC: Stockholm, Sweden, 2024. [Google Scholar]
- Shahhosseini, N.; Wong, G.; Babuadze, G.; Camp, J.V.; Ergonul, O.; Kobinger, G.P.; Chinikar, S.; Nowotny, N. Crimean-congo hemorrhagic fever virus in asia, africa and europe. Microorganisms 2021, 9, 1907. [Google Scholar] [CrossRef]
- Angela, F.; Christof, S.J.; Marco, D.N.; Alastair, D.; Ilaria, C.; Gianvito, L.; Domenico, B.; Paula, C.-S.; Paolo, T. Epidemic intelligence data of Crimean-Congo haemorrhagic fever, European Region, 2012 to 2022: A new opportunity for risk mapping of neglected diseases. Euro Surveill. 2023, 28, 2200542. [Google Scholar] [CrossRef]
- Mancuso, E.; Toma, L.; Polci, A.; d’Alessio, S.G.; Di Luca, M.; Orsini, M.; Di Domenico, M.; Marcacci, M.; Mancini, G.; Spina, F.; et al. Crimean-Congo Hemorrhagic Fever Virus Genome in Tick from Migratory Bird, Italy. Emerg. Infect. Dis. 2019, 25, 1418–1420. [Google Scholar] [CrossRef]
- Spengler, J.R.; Bergeron, É.; Rollin, P.E. Seroepidemiological Studies of Crimean-Congo Hemorrhagic Fever Virus in Domestic and Wild Animals. PLoS Negl. Trop. Dis. 2016, 10, e0004210. [Google Scholar] [CrossRef] [PubMed]
- De Liberato, C.; Frontoso, R.; Magliano, A.; Montemaggiori, A.; Autorino, G.L.; Sala, M.; Bosworth, A.; Scicluna, M.T. Monitoring for the possible introduction of Crimean-Congo haemorrhagic fever virus in Italy based on tick sampling on migratory birds and serological survey of sheep flocks. Prev. Vet. Med. 2018, 149, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Papa, A.; Dalla, V.; Papadimitriou, E.; Kartalis, G.N.; Antoniadis, A. Emergence of Crimean-Congo haemorrhagic fever in Greece. Clin. Microbiol. Infect. 2010, 16, 843–847. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Crimean-Congo Haemorrhagic Fever. Available online: https://www.ecdc.europa.eu/en/crimean-congo-haemorrhagic-fever/surveillance/cases-eu-since-2013 (accessed on 10 April 2024).
- Celina, S.S.; Černý, J.; Samy, A.M. Mapping the potential distribution of the principal vector of Crimean-Congo haemorrhagic fever virus Hyalomma marginatum in the Old World. PLoS Negl. Trop. Dis. 2023, 17, e0010855. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. The Spatial Distribution of Crimean-Congo Haemorrhagic Fever in Europe and Its Neighbours; ECDC: Stockholm, Sweden, 2023. [Google Scholar]
- Kunchev, A.; Kojouharova, M. Probable cases of Crimean-Congo-haemorrhagic fever in Bulgaria: A preliminary report. Euro Surveill. 2008, 13, 18845. [Google Scholar] [CrossRef]
- Hornok, S.; Horváth, G. First report of adult Hyalomma marginatum rufipes (vector of Crimean-Congo haemorrhagic fever virus) on cattle under a continental climate in Hungary. Parasit. Vectors 2012, 5, 170. [Google Scholar] [CrossRef]
- England, M.E.; Phipps, P.; Medlock, J.M.; Atkinson, P.M.; Atkinson, B.; Hewson, R.; Gale, P. Hyalomma ticks on northward migrating birds in southern Spain: Implications for the risk of entry of Crimean-Congo haemorrhagic fever virus to Great Britain. J. Vector Ecol. 2016, 41, 128–134. [Google Scholar] [CrossRef]
- Grandi, G.; Chitimia-Dobler, L.; Choklikitumnuey, P.; Strube, C.; Springer, A.; Albihn, A.; Jaenson, T.G.T.; Omazic, A. First records of adult Hyalomma marginatum and H. rufipes ticks (Acari: Ixodidae) in Sweden. Ticks Tick Borne Dis. 2020, 11, 101403. [Google Scholar] [CrossRef]
- Bonnet, S.; Baize, S.; Bertagnoli, S.; Falchi, A.; Figoni, J.; Hoch, T.; Moutailler, S.; Raffetin, A.; René-Martellet, M.; Stachurski, F.; et al. Analyse des Risques pour la Santé Humaine et Animale Liés aux Tiques du Genre Hyalomma en France; Anses: Paris, France, 2023; pp. 143–160. [Google Scholar]
- Bernard, C.; Kukla, C.J.; Rakotoarivony, I.; Duhayon, M.; Stachurski, F.; Huber, K.; Giupponi, C.; Zortman, I.; Holzmuller, P.; Pollet, T.; et al. Detection of Crimean–Congo haemorrhagic fever virus in Hyalomma marginatum ticks, southern France, May 2022 and April 2023. Eurosurveillance 2024, 29, 2400023. [Google Scholar] [CrossRef]
- Kampen, H.; Poltz, W.; Hartelt, K.; Wölfel, R.; Faulde, M. Detection of a questing Hyalomma marginatum marginatum adult female (Acari, Ixodidae) in southern Germany. Exp. Appl. Acarol. 2007, 43, 227–231. [Google Scholar] [CrossRef]
- Estrada-Peña, A.; Palomar, A.M.; Santibáñez, P.; Sánchez, N.; Habela, M.A.; Portillo, A.; Romero, L.; Oteo, J.A. Crimean-Congo haemorrhagic fever virus in ticks, Southwestern Europe. Emerg. Infect. Dis. 2012, 18, 179–180. [Google Scholar] [CrossRef]
- Centro de Coordinación de Alertas y Emergencias Sanitarias. Informe de Situación y Evaluación del Riesgo de Transmisión del Virus de la Fiebre Hemorrágica de Crimea-Congo en España. Ministerio de Sanidad, Consumo y Bienestar Social. Julio 2019. Available online: https://www.sanidad.gob.es/areas/alertasEmergenciasSanitarias/situacionRiesgo/docs/ER_FHCC.pdf (accessed on 27 March 2024).
- Negredo, A.; Sánchez-Ledesma, M.; Llorente, F.; Pérez-Olmeda, M.; Belhassen-García, M.; González-Calle, D.; Sánchez-Seco, M.P.; Jiménez-Clavero, M.Á. Retrospective identification of early autochthonous case of crimean-Congo hemorrhagic fever, Spain, 2013. Emerg. Infect. Dis. 2021, 27, 1754–1756. [Google Scholar] [CrossRef]
- EFE. Muere en Salamanca el Hombre de Avanzada Edad con Fiebre Hemorrágica de Crimea-Congo. El Mundo 2024. Available online: https://www.elmundo.es/ciencia-y-salud/salud/2024/05/03/663494d8e4d4d89d218b45ae.html (accessed on 3 May 2024).
- Diario Médico. Madrid Activa el Protocolo de Actuación Ante el Primer Caso de Fiebre Hemorrágica Crimea-Congo. 23 de Julio 2024. Available online: http://www.diariomedico.com/medicina/enfermedades-infecciosas/madrid-activa-protocolo-actuacion-primer-caso-fiebre-hemorragica-crimea-congo.html (accessed on 30 July 2024).
- Centro Nacional de Epidemiología; Instituto de Salud Carlos III. Informe Epidemiológico Sobre la Situación de la Fiebre Hemorrágica de Crimea-Congo en España. Años 2016 a 2023. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/archivos%20A-Z/Fiebre_Hemorr%C3%A1gica_Crimea_Congo/INFORME_RENAVE_FHCC%202016-2023_final.pdf (accessed on 27 March 2024).
- Frías, M.; Fischer, K.; Castro-Scholten, S.; Bost, C.; Cano-Terriza, D.; Risalde, M.Á.; Acevedo, P.; Jiménez-Ruiz, S.; Sadeghi, B.; Groschup, M.H.; et al. Epidemiologic Survey of Crimean-Congo Hemorrhagic Fever Virus in Suids, Spain. Emerg. Infect. Dis. 2024, 30, 984–990. [Google Scholar] [CrossRef]
- Swanepoel, R.; Gill, D.E.; Shepherd, A.J.; Leman, P.A.; Mynhardt, J.H.; Harvey, S. The Clinical Pathology of Crimean-Congo Hemorrhagic Fever. Rev. Infect. Dis. 1989, 11, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Raabe, V.N. Diagnostic Testing for Crimean-Congo Hemorrhagic Fever. J. Clin. Microbiol. 2020, 58, e01580-19. [Google Scholar] [CrossRef] [PubMed]
- Tasdelen Fisgin, N.; Ergonul, O.; Doganci, L.; Tulek, N. The role of ribavirin in the therapy of crimean-congo hemorrhagic fever: Early use is promising. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 929–933. [Google Scholar] [CrossRef] [PubMed]
- Ergönül, Ö.; Çelikbaş, A.; Dokuzoǧuz, B.; Eren, Ş.; Baykam, N.; Esener, H. Characteristics of Patients with Crimean-Congo Hemorrhagic Fever in a Recent Outbreak in Turkey and Impact of Oral Ribavirin Therapy. Clin. Infect. Dis. 2004, 39, 284–287. [Google Scholar] [CrossRef]
- Shrivastava, N.; Kumar, J.S.; Yadav, P.; Sharma, S.; Shete, A.M.; Jain, R.; Shrivastava, A.; Dash, P.K. Development and evaluation of indirect antibody ELISA assay for early diagnosis and surveillance of Crimean-Congo hemorrhagic fever infection in humans. Virus Res. 2022, 313, 198717. [Google Scholar] [CrossRef]
- Shepherd, A.J.; Swanepoel, R.; Leman, P.A.; Shepherd, S.P. Comparison of Methods for Isolation and Titration of Crimean-Congo Hemorrhagic Fever virus. J. Clin. Microbiol. 1986, 24, 654–656. [Google Scholar] [CrossRef]
- Burt, F.J.; Leman, P.A.; Abbott, J.C.; Swanepoel, R. Serodiagnosis of Crimean-Congo Haemorrhagic Fever. Epidemiol. Infect. 1994, 113, 551–562. [Google Scholar] [CrossRef]
- Drosten, C.; Kümmerer, B.M.; Schmitz, H.; Günther, S. Molecular diagnostics of viral hemorrhagic fevers. Antiviral Res. 2003, 57, 61–87. [Google Scholar] [CrossRef] [PubMed]
- Ergonul, O. Treatment of Crimean-Congo hemorrhagic fever. Antiviral Res. 2008, 78, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Oestereich, L.; Rieger, T.; Neumann, M.; Bernreuther, C.; Lehmann, M.; Krasemann, S.; Wurr, S.; Emmerich, P.; de Lamballerie, X.; Ölschläger, S.; et al. Evaluation of Antiviral Efficacy of Ribavirin, Arbidol, and T-705 (Favipiravir) in a Mouse Model for Crimean-Congo Hemorrhagic Fever. PLoS Negl. Trop. Dis. 2014, 8, e2804. [Google Scholar] [CrossRef] [PubMed]
- Dreshaj, S.; Ahmeti, S.; Ramadani, N.; Dreshaj, G.; Humolli, I.; Dedushaj, I. Current situation of Crimean-Congo hemorrhagic fever in Southeastern Europe and neighboring countries: A public health risk for the European Union? Travel Med. Infect. Dis. 2016, 14, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Papa, A.; Tsiodras, S.; Dalla, V.; Maltezos, E.; Antoniadis, A. Crimean-Congo hemorrhagic fever in Greece: A public health perspective. Int. J. Infect. Dis. 2009, 13, 713–716. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | TOTAL |
|---|---|---|---|---|---|---|---|---|---|
| Bulgaria | 2 | 6 | 2 | 1 | 0 | 2 | 0 | 0 | 13 |
| Greece | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Spain | 0 | 2 | 0 | 3 | 2 | 2 | 1 | 4 | 14 |
| Case | Year 1 | Month 1 | Province | Transmission | Risk Factor | Age | Death |
|---|---|---|---|---|---|---|---|
| 1 | 2013 | May | Ávila | Tick | Rural walk | 32 | No |
| 2 | 2016 | August | Ávila | Tick | Rural walk | 62 | Yes |
| 3 | 2016 | August | Madrid | Nosocomial 2 | Healthcare worker | 50 | No |
| 4 | 2018 | July | Badajoz | Tick | Hunting | 74 | Yes |
| 5 | 2018 | July | Salamanca | Tick | Farm animal | 53 | No |
| 6 | 2020 | June | Salamanca | Tick | Rural walk | 69 | No |
| 7 | 2020 | June | Salamanca | Tick | Animals | 53 | No |
| 8 | 2020 | August | Salamanca | Tick | Gardens | 69 | Yes |
| 9 | 2021 | April | Salamanca | Tick | Livestock farmer | 59 | No |
| 10 | 2021 | June | Leon | Tick | Rural walk | 29 | No |
| 11 | 2022 | June | Leon | Unknown | Environmental agent | 51 | Yes |
| 12 | 2022 | July | Leon | Tick | Hunting | 49 | No |
| 13 | 2023 | June | Salamanca | Tick | Unknown | 66 | No |
| 14 | 2024 | April | Salamanca | Tick | Rural walk | - | Yes |
| 15 | 2024 | July | Toledo | Tick | Rural walk | 74 | Yes |
| 16 | 2024 | July | Seville | Tick | Rural walk | 46 | No |
| 17 | 2024 | August | Caceres | Tick | - | 65 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eslava, M.; Carlos, S.; Reina, G. Crimean-Congo Hemorrhagic Fever Virus: An Emerging Threat in Europe with a Focus on Epidemiology in Spain. Pathogens 2024, 13, 770. https://doi.org/10.3390/pathogens13090770
Eslava M, Carlos S, Reina G. Crimean-Congo Hemorrhagic Fever Virus: An Emerging Threat in Europe with a Focus on Epidemiology in Spain. Pathogens. 2024; 13(9):770. https://doi.org/10.3390/pathogens13090770
Chicago/Turabian StyleEslava, María, Silvia Carlos, and Gabriel Reina. 2024. "Crimean-Congo Hemorrhagic Fever Virus: An Emerging Threat in Europe with a Focus on Epidemiology in Spain" Pathogens 13, no. 9: 770. https://doi.org/10.3390/pathogens13090770