1. Introduction
Neglected tropical diseases (NTDs) such as schistosomiasis (also known as bilharziasis) and soil-transmitted helminths (STHs, also known as intestinal worms) remain major public health problems in many parts of the world [
1]. Schistosomiasis mainly affects people living in the tropics and sub-tropics, particularly the poor and most deprived communities [
2]. Globally, about 252 million people were estimated to be infected with schistosomiasis in 2015 [
3], and from these, the sub-Saharan region constitutes more than 90% of the disease burden [
2]. Likewise, STHs are the most widespread neglected tropical disease; worldwide more than 1.5 billion people are infected with
Ascaris lumbricoides,
Trichuris trichiura (whipworms), and/or hookworm in over 100 endemic countries, together accounting for a major burden of parasitic disease worldwide [
4].
Schistosomiasis is endemic in Ethiopia, and intestinal schistosomiasis, caused by
Schistosoma mansoni, is the most common type of schistosomiasis in the country. About 37.3 million people are currently living in areas where schistosomiasis is endemic in Ethiopia [
5]. STHs infections are also widely distributed. Ethiopia is listed among the top five sub-Saharan countries with the highest prevalence of STHs—second, third, and fourth highest for ascariasis, hookworm infection, and trichiurasis, respectively [
6]. About 79 million people are currently living in STHs-endemic areas that require preventive chemotherapy [
7]. Although all age groups can have schistosomiasis and STHs infections, most infections occur in pre-school and school-aged children.
Schistosomiasis and STHs are more common in rural and disadvantaged urban populations with poor sanitation and lack of a safe water supply. Schistosomiasis is transmitted by contact with infected freshwater [
4]. STHs is transmitted by the ingestion of eggs and contact with contaminated water and soil [
8]. STHs are transmitted through eggs present in human feces, which contaminate the soil in areas where sanitation is poor. School-aged children are at increased risk of schistosomiasis and STHs infection due to a high level of exposure resulting from contact with water and soil while swimming and playing [
9].
Schistosomiasis causes anemia, stunting, fatigue, and diminished physical fitness in children and may also negatively impact cognitive abilities [
10]. The severity of morbidity increases as the disease interacts with other parasitic infections like STHs. These parasitic infections are associated with malnutrition, which can negatively impact the quality of life, especially in settings with extreme poverty affecting future growth and development [
10,
11].
The primary strategy recommended by WHO for the control and elimination of schistosomiasis and STHs infections is through preventive chemotherapy (PC) to all at-risk populations, including school-age children [
12]. The large-scale public health intervention involves the administration of praziquantel and albendazole/mebendazole against schistosomiasis and STHs, respectively, to all populations at risk. Annual distribution of praziquantel is recommended in areas where the prevalence is greater than 50%, every two years where the prevalence is between 10−50%, and twice during their primary school age where the prevalence is less than 10% [
13].
The WHO and its member states, including Ethiopia, have aimed to control and eliminate schistosomiasis infections as a public health problem by 2020 and 2025, respectively [
14]. The NTD roadmap of WHO also aimed, by 2020, to eliminate STHs as a public health problem, defined as <1% of the at-risk population having an infection of moderate or high intensity [
4]. Surveillance studies to assess the outcome of long-term program implementation in reducing the disease burden is important to inform policymakers to revise control and elimination strategies to these diseases as public health problems by 2020 and beyond. Since 2014, the national NTD program of Ethiopia has been implementing targeted school-based mass drug administration (MDA) containing praziquantel and albendazole annually in regions with moderate to high prevalence of schistosomiasis and STHs infections [
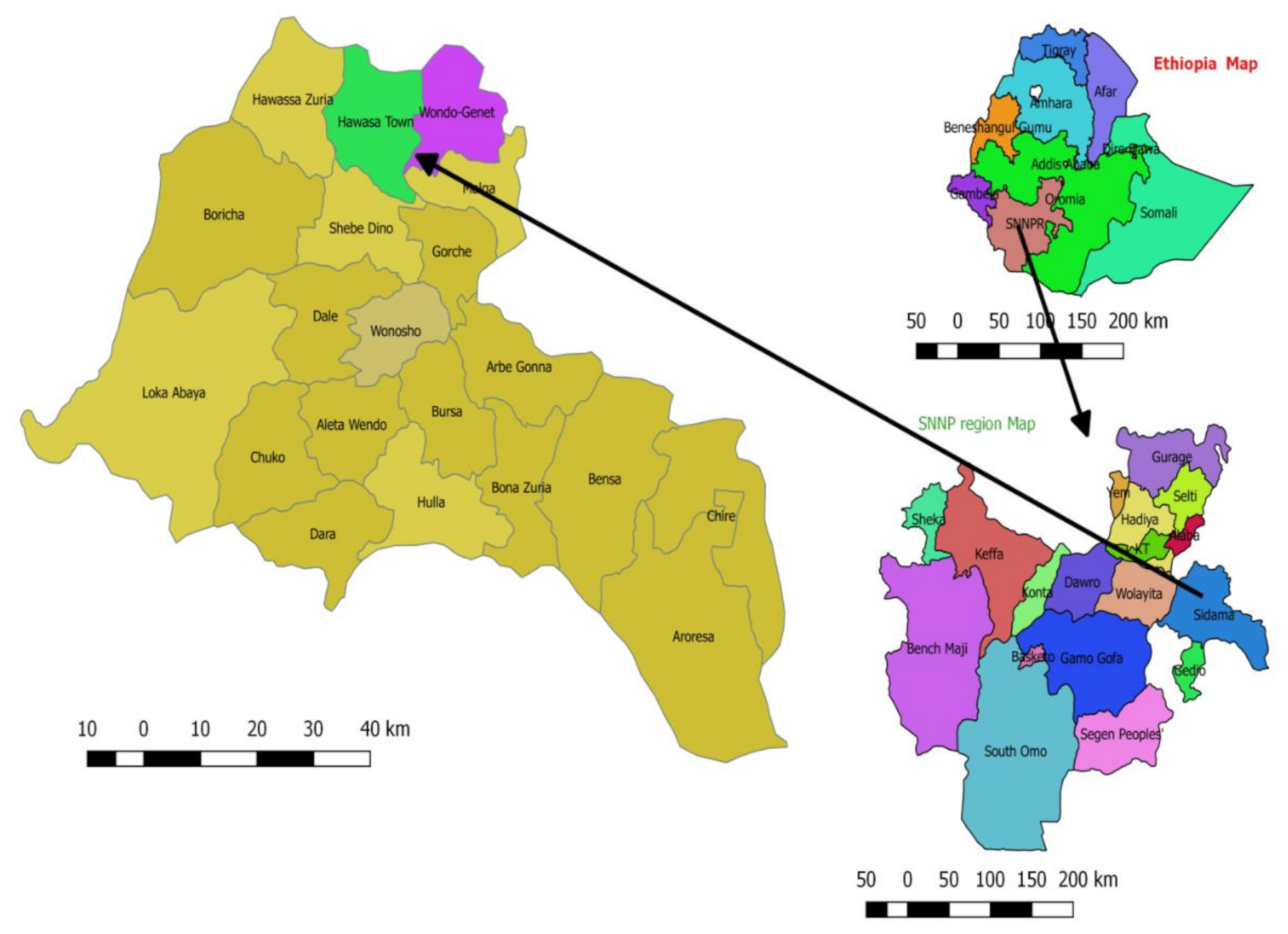
7]. However, no assessment was done on the effectiveness of the implemented interventions. Surveillance data after program implementation to evaluate the impact of long-term PC in reducing the disease burden in endemic countries is critical for evidence-based decision-making. In the current study, we investigated the prevalence, intensity, rates of parasite co-infections, and associated factors of intestinal schistosomiasis and STHs in primary school children in two rural districts of Southern Ethiopia. According to the pre MDA data from the national mapping of NTDs conducted in 2013/2014, both study districts were classified as high prevalence endemic areas (with prevalence of >50%) for both schistosomiasis and STHs [
15].
3. Discussion
We conducted a school-based cross-sectional study to assess infection prevalence, intensity, and associated risk factors of S. mansoni and STHs in two rural districts of southern Ethiopia after implementing five rounds of preventive chemotherapy through the national NTD program. Our main results include the following: i) the overall prevalence of S. mansoni infection was 25.8% (ranging between study schools from 11.6% to 54.1%); ii) there was a high overall prevalence of STHs infection (54.7%), with significant variations between schools ranging from 30.6% to 71.0%; iii) a significant correlation was found between S. mansoni and STHs, in particular with T. trichiura; iii) while school location is a significant predictor of both S. mansoni and STHs infection, younger age was an additional significant risk factor for STHs infection. The prevalence of parasite infection significantly varied by the residence area, age, sex, and study schools of participants. To our knowledge, this is the most extensive study to evaluate the status of S. mansoni and STH infections after the implementation of multiple rounds of mass drug administration (MDA) in Ethiopia and sub-Saharan Africa at large.
The overall infection rate among children infected at least with one parasite (either STHs or
S. mansoni) was 64.2% (54.9% at Hawella Tula and 76.1% at Wondo Gennet district). The prevalence of infection with at least one parasite significantly varied between the four study schools, namely 37.1% at Finchawa, 57.2% at Bushulo, 68.2% at Kidus Pawulos, and the highest (76.1%) at Wosha primary schools. The current prevalence of infection with at least one parasite at the Hawella Tula district (54.9%) showed a decreasing trend compared to previous reports of 91.5% in 2007 [
16] and 69.7% in 2015 [
17]. Program intervention to control infection, including preventive chemotherapy implemented by the Ministry of Health, has resulted in a progressive decline in infection prevalence.
The prevalence of
S. mansoni infection observed in the two study districts was 25.8%; however, the prevalence significantly varied among the schools, with the highest prevalence observed at Kidus Pawulos School (54.1%) and the lowest observed at Finchawa School (11.6%). District-wise there was no significant variation between Hawella Tula district (24.6%) and Wondo Gennet district (27.3%). Although the prevalence of
S. mansoni infection varies significantly between the three schools in Hawella Tula district, the overall prevalence rate observed in our study shows a progressive decrease from previous reports in 2007 (73.7%) [
16] and in 2015 from the same district (31%) [
17]. Similarly, the prevalence of
S. mansoni infection in the Wondo Gennet district decreased from 74.9% in 2012 [
18] and 59.9% in 2014 [
19] when compared to the current findings of 27.3% in 2019. This progressive decline in infection prevalence may indicate the impact of control measures, including the implementation of PC in the study areas. However, the current prevalence of 54.1% that was observed at Kidus Pawulos school in this study is much higher than the previously reported 31% in 2015 from the same village. During our data collection, lack of clean water supply for drinking, poor hygiene and sanitation care, and inadequate access to clean toilets were noted. This observation calls for the integration of other environmental control measures such as access to adequate water, sanitation, and hygiene (WASH), and providing health education on basic hygiene and sanitation for behavioral change.
The NTD roadmap set by the WHO targets the control of schistosomiasis, defined as achieving less than 5% of heavy-intensity infection by 2020, and to eliminate schistosomiasis as a public health problem, defined as reaching <1% prevalence of heavy-intensity infections in school-aged children (5–14 years old) by 2025 [
14]. The overall heavy-intensity infection (1.4%) for
S. mansoni infection in this study is near the WHO 2020 target. However, the observed heavy-intensity infection rate at the most affected school (4.6% in Kidus Pawlos) may indicates that the
S. mansoni infection is still a major public health problem at the study area, and the WHO target to control schistosomiasis by 2020 may be difficult to achieve. Nearly 30% of the infected children from the two most affected schools (Kidus Pawulos and Wosha) had a moderate- or high-intensity prevalence of
S. mansoni infection (
Table 4). This may indicate the presence of hotspots for the continuous transmission of infection in the study area. Hence, additional interventions are urgently needed for the prevention of transmission by treating other high-risk groups, improving hygiene and sanitation, and providing a safe water supply [
8] instead of relying on single control measures as are currently implemented by the program.
S. mansoni infection was significantly associated with the dwelling area of children and schools. The children from Tula and Wosha kebeles had the highest prevalence of intestinal schistosomiasis infection, and the dwelling area was significantly associated with
S. mansoni infection. Similarly, children attending Kidus Pawulos primary school also had the highest prevalence of intestinal schistosomiasis, and the school was significantly associated with
S. mansoni infection. This association is explained by the reason that children living in these areas have high water contact due to the proximity of their dwellings area to Lake Hawassa and local water sources at Wondo Genet. The distribution of
S. mansoni infection was not gender- or age-associated, which was in agreement with a study conducted in Sanja town [
20] and in studies conducted in Madagascar [
21] and northwestern Tanzania [
22]. This similarity might show that school-aged children, irrespective of their gender and age differences, have equal exposure to contaminated water in their areas.
The overall infection rates of STHs observed in this study was 54.7%, with a significant difference among schools ranging from 30.6% at Finchawa to 71% at Wosha schools. The prevalence also greatly varies among the two study districts, with 42% at Hawella Tula and 71% at Wondo Gennet. The observed STHs infection rates at Hawella Tula district showed a decrease from the previous study reports of 52.4% in 2015. Three soil-transmitted helminths, i.e.,
A. lumbricoides,
T. trichiura, and hookworm, were predominantly detected. This finding is in agreement with one previous study conducted in one of the study districts (Hawella Tula) in 2015 [
17].
A. lumbricoides was the most prevalent STHs followed by
T. trichiura and hookworm infections in both study districts. The high prevalence of STHs observed in the study area might be attributed to the unhygienic use of sugarcane by children, as sugar cane is commonly planted in the study areas. In contrast to the present findings, hookworm infection was found to be predominant in previous studies conducted in different parts of Ethiopia [
23,
24]. The lower prevalence of hookworm infection observed in the present study might be associated with a decreased less habit of walking barefoot.
The co-infection observed in this study showed 1–4 parasite species were detected per one study participant. Most children harbored double infection with two parasites, and the predominant observed double infections were
A. lumbricoides with
T. trichiura with the total co-infection rate exceeding 30%. Over 61.6% of
S. mansoni-infected children had an infection with at least one STH, perhaps due to similarity in the risk of infection for these parasitic helminths. In children, this co-infection of schistosomiasis and STHs can cause different morbidities like anemia, fatigue, poor growth, and poor cognitive development. These morbidities result in poor school attendance, poor concentration in class, and poor academic performance, which can negatively affect the quality of life of children, impacting their future growth and development [
10,
11,
25,
26].
The WHO intervention program intends to eliminate STH as a public health problem in children by 2020. WHO defines STHs as a public health problem when more than 1% of the at-risk population has an infection of moderate or high intensity, and its control requires the delivery of one or more public health interventions [
4]. Even though the prevalence of STHs infection observed in this study showed a slight decrease from previous reports, the observed high-intensity (1.4%) and moderate-intensity (14.3%) prevalence for
A. lumbricoides indicates that the national NTD program is far from achieving the target to eliminate STH as a public health problem by 2020. Thus, focusing on the implementation of PC alone may not be adequate, and integration of other control measures, including surveillance of drug efficacy and identifying transmission hotspots for targeted intervention, is urgently needed. Furthermore, since the overall STHs prevalence in the two study districts is >50%, we recommend implantation of biannual MDA for both pre-school and school-age children as well as women of childbearing age as per the recommendation of WHO guideline [
27].


 ,
, 



{kind=link}
{kind=link}
{kind=link}