

Low Interferon-γ Levels in Cord and Peripheral Blood of Pregnant Women Infected with SARS-CoV-2
 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection
2.3. Biochemical Determination
2.4. Determination of Interferon-γ (IFN-γ) and Anti-IFN-γ Antibodies
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Characteristics of the Newborns
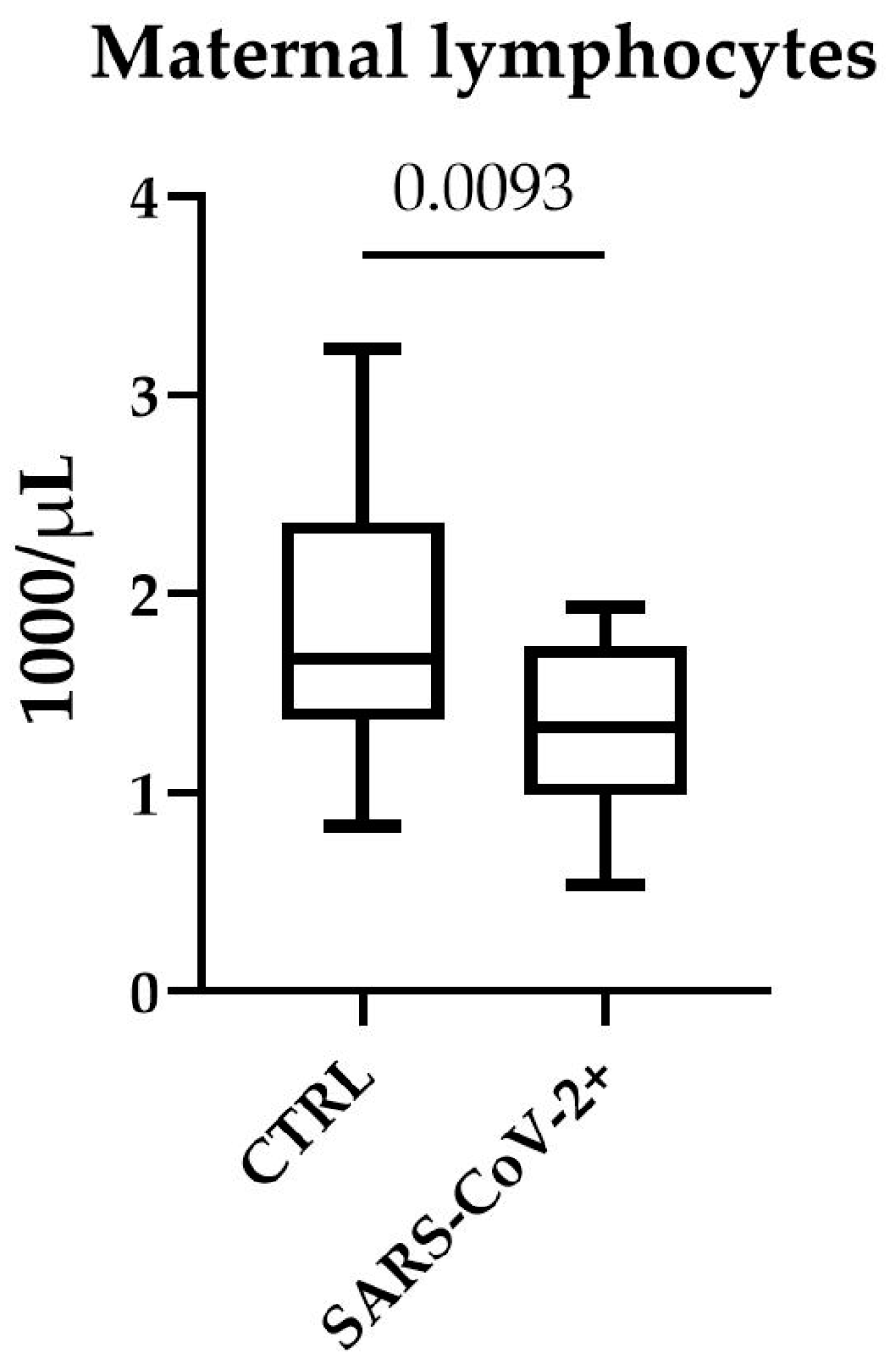
3.3. Effect of SARS-CoV-2 Infection on Blood Cell Count and CRP in Pregnant Women
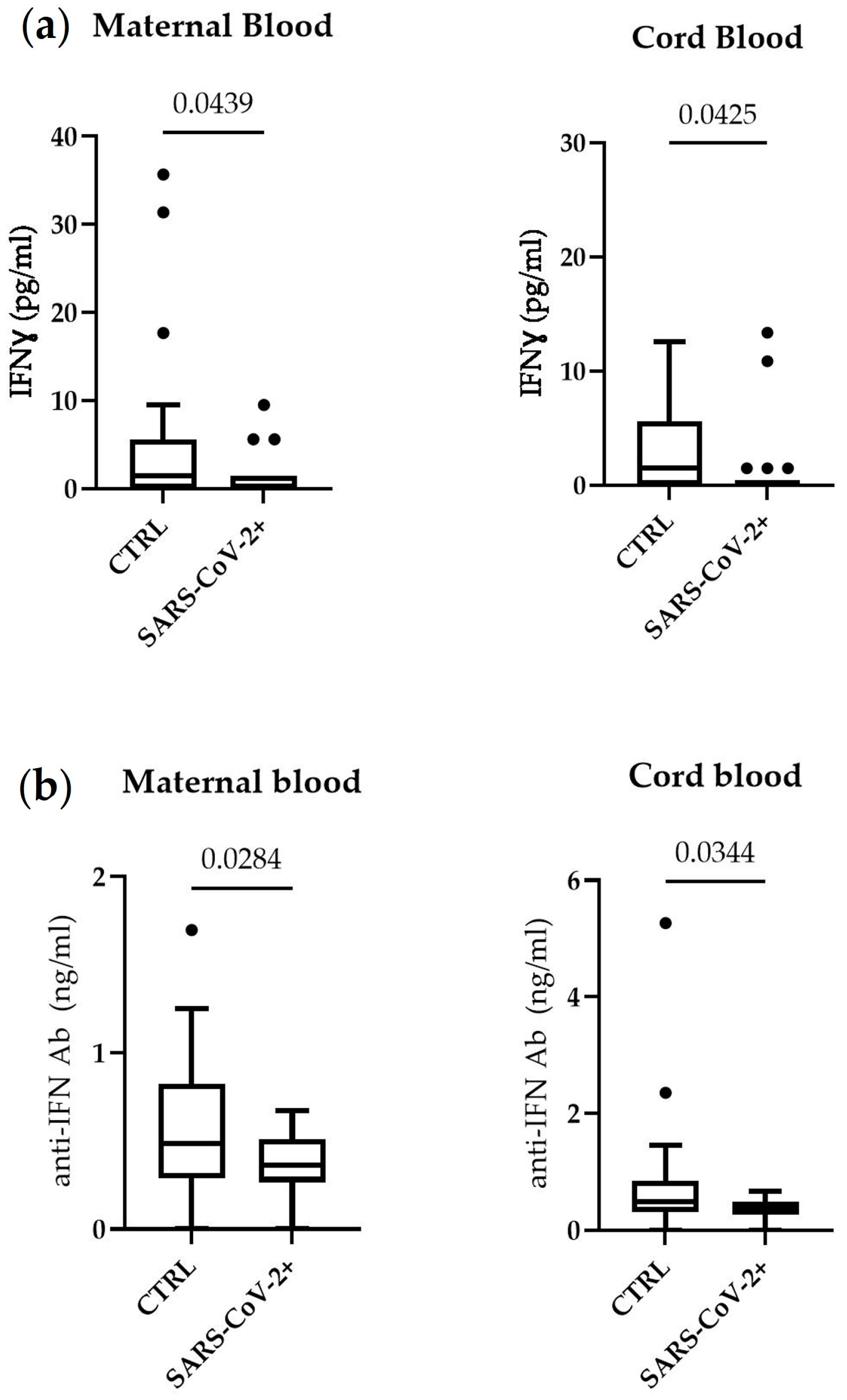
3.4. Measurement of IFN-γ and Anti IFN-γ Antibodies in Serum and Cord Blood of Mothers Affected by COVID-19
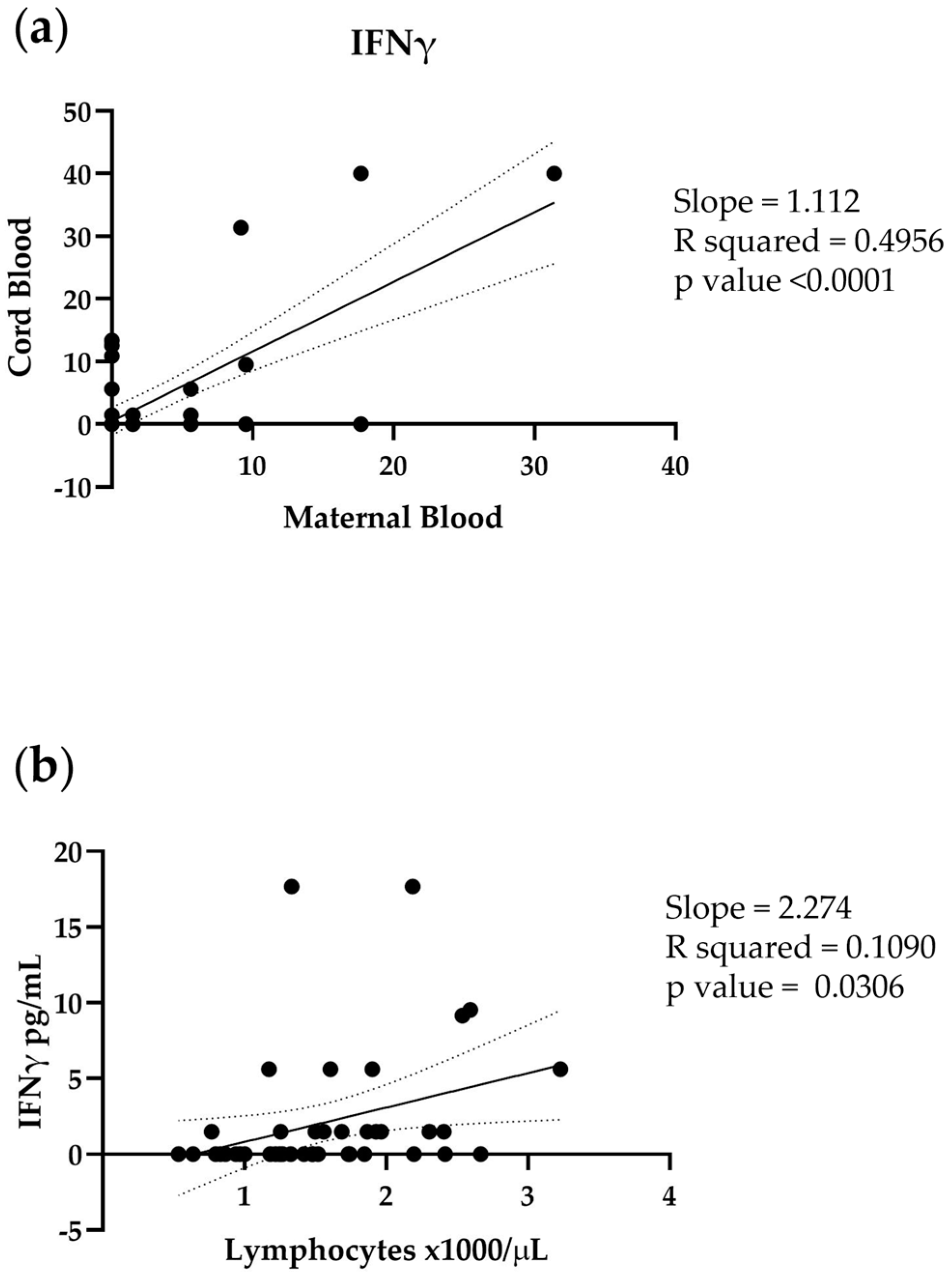
3.5. Correlation between IFN-γ Cord Blood and Maternal Blood
3.6. Correlation between Maternal IFN-γ and Maternal Lymphocyte Count
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.-M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Forouzesh, M.; Rahimi, A.; Valizadeh, R.; Dadashzadeh, N.; Mirzazadeh, A. Clinical display, diagnostics and genetic implication of novel Coronavirus (COVID-19) epidemic. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4607–4615. [Google Scholar] [PubMed]
- Chakraborty, I.; Maity, P. COVID-19 outbreak: Migration, effects on society, global environment and prevention. Sci. Total Environ. 2020, 728, 138882. [Google Scholar] [CrossRef] [PubMed]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. Severe acute respiratory syndrome-related coronavirus: The species and its viruses—A statement of the Coronavirus Study Group. BioRxiv 2020. [CrossRef] [Green Version]
- Wang, J.; Jiang, M.; Chen, X.; Montaner, L.J. Cytokine storm and leukocyte changes in mild versus severe SARS-CoV-2 infection: Review of 3939 COVID-19 patients in China and emerging pathogenesis and therapy concepts. J. Leukoc. Biol. 2020, 108, 17–41. [Google Scholar] [CrossRef]
- Azkur, A.K.; Akdis, M.; Azkur, D.; Sokolowska, M.; van de Veen, W.; Bruggen, M.-C.; O’Mahony, L.; Gao, Y.; Nadeau, K.; Akdis, C.A. Immune response to SARS-CoV-2 and mechanisms of immunopathological changes in COVID-19. Allergy 2020, 75, 1564–1581. [Google Scholar] [CrossRef]
- Zhu, J.; Zhong, Z.; Ji, P.; Li, H.; Li, B.; Pang, J.; Zhang, J.; Zhao, C. Clinicopathological characteristics of 8697 patients with COVID-19 in China: A meta-analysis. Fam. Med. Community Health 2020, 8, e000406. [Google Scholar] [CrossRef]
- Coopersmith, C.M.; Antonelli, M.; Bauer, S.R.; Deutschman, C.S.; Evans, L.E.; Ferrer, R.; Hellman, J.; Jog, S.; Kesecioglu, J.; Kissoon, N.; et al. The Surviving Sepsis Campaign: Research Priorities for Coronavirus Disease 2019 in Critical Illness. Crit. Care Med. 2021, 49, 598–622. [Google Scholar] [CrossRef]
- Gupta, A.; Madhavan, M.V.; Sehgal, K.; Nair, N.; Mahajan, S.; Sehrawat, T.S.; Bikdeli, B.; Ahluwalia, N.; Ausiello, J.C.; Wan, E.Y.; et al. Extrapulmonary manifestations of COVID-19. Nat. Med. 2020, 26, 1017–1032. [Google Scholar] [CrossRef]
- Mor, G.; Aldo, P.; Alvero, A.B. The unique immunological and microbial aspects of pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef]
- Murphy, S.P.; Tayade, C.; Ashkar, A.A.; Hatta, K.; Zhang, J.; Croy, B.A. Interferon Gamma in Successful Pregnancies. Biol. Reprod. 2009, 80, 848–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, S.A.; Smulian, J.C.; Lednicky, J.A.; Wen, T.S.; Jamieson, D.J. Coronavirus Disease 2019 (COVID-19) and pregnancy: What obstetricians need to know. Am. J. Obstet. Gynecol. 2020, 222, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Cardenas, I. The Immune System in Pregnancy: A Unique Complexity. Am. J. Reprod. Immunol. 2010, 63, 425–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LoMauro, A.; Aliverti, A. Respiratory physiology in pregnancy and assessment of pulmonary function. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 85, 3–16. [Google Scholar] [CrossRef]
- De Luca, C.; Gragnano, G.; Conticell, F.; Cennamo, M.; Pisapia, P.; Terraccino, D.; Malapelle, U.; Montella, E.; Triassi, M.; Troncone, G.; et al. Evaluation of a fully closed real time PCR platform for the detection of SARS-CoV-2 in nasopharyngeal swabs: A pilot study. J. Clin. Pathol. 2022, 75, 551–554. [Google Scholar] [CrossRef]
- Tanacan, A.; Yazihan, N.; Erol, S.A.; Anuk, A.T.; Yetiskin, F.D.Y.; Biriken, D.; Ozgu-Erdinc, A.; Keskin, H.L.; Tekin, O.M.; Sahin, D. The impact of COVID-19 infection on the cytokine profile of pregnant women: A prospective case-control study. Cytokine 2021, 140, 155431. [Google Scholar] [CrossRef] [PubMed]
- Hadjadj, J.; Yatim, N.; Barnabei, L.; Corneau, A.; Boussier, J.; Smith, N.; Péré, H.; Charbit, B.; Bondet, V.; Chenevier-Gobeaux, C.; et al. Impaired type I interferon activity and inflammatory responses in severe COVID-19 patients. Science 2020, 369, 718–724. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Chakraborty, R.K.; Burns, B. Systemic Inflammatory Response Syndrome, in StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Yazdanpanah, F.; Hamblin, M.R.; Rezaei, N. The immune system and COVID-19: Friend or foe? Life Sci. 2020, 256, 117900. [Google Scholar] [CrossRef] [PubMed]
- Cabaro, S.; D’Esposito, V.; Di Matola, T.; Sale, S.; Cennamo, M.; Terracciano, D.; Parisi, V.; Oriente, F.; Portella, G.; Beguinot, F.; et al. Cytokine signature and COVID-19 prediction models in the two waves of pandemics. Sci. Rep. 2021, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.K.-F.; Wu, H.; Yan, H.; Ma, S.; Wang, L.; Zhang, M.; Tang, X.; Temperton, N.; Weiss, R.A.; Brenchley, J.M.; et al. T Cell Responses to Whole SARS Coronavirus in Humans. J. Immunol. 2008, 181, 5490–5500. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, Z.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Curbelo, J.; Bueno, S.L.; Galván-Román, J.M.; Ortega-Gómez, M.; Rajas, O.; Fernández-Jiménez, G.; Vega-Piris, L.; Rodríguez-Salvanes, F.; Arnalich, B.; Díaz, A.; et al. Correction: Inflammation biomarkers in blood as mortality predictors in community-acquired pneumonia admitted patients: Importance of comparison with neutrophil count percentage or neutrophil-lymphocyte ratio. PLoS ONE 2019, 14, e0212915. [Google Scholar] [CrossRef]
- Lazear, H.M.; Schoggins, J.W.; Diamond, M.S. Shared and Distinct Functions of Type I and Type III Interferons. Immunity 2019, 50, 907–923. [Google Scholar] [CrossRef]
- Casazza, R.L.; Lazear, H.M.; Miner, J.J. Protective and Pathogenic Effects of Interferon Signaling During Pregnancy. Viral Immunol. 2020, 33, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Fasouliotis, S.J.; Spandorfer, S.D.; Witkin, S.S.; Schattman, G.; Liu, H.C.; Roberts, J.E.; Rosenwaks, Z. Maternal serum levels of interferon-gamma and interleukin-2 soluble receptor-alpha predict the outcome of early IVF pregnancies. Hum. Reprod. 2004, 19, 1357–1363. [Google Scholar] [CrossRef]
- Ain, R.; Canham, L.N.; Soares, M.J. Gestation stage-dependent intrauterine trophoblast cell invasion in the rat and mouse: Novel endocrine phenotype and regulation. Dev. Biol. 2003, 260, 176–190. [Google Scholar] [CrossRef] [Green Version]
- Ashkar, A.A.; Di Santo, J.P.; Croy, B.A. Interferon gamma contributes to initiation of uterine vascular modification, decidual integrity, and uterine natural killer cell maturation during normal murine pregnancy. J. Exp. Med. 2000, 192, 259–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Browne, S.K.; Zaman, R.; Sampaio, E.P.; Jutivorakool, K.; Rosen, L.B.; Ding, L.; Pancholi, M.J.; Yang, L.M.; Priel, D.L.; Uzel, G.; et al. Anti-CD20 (rituximab) therapy for anti-IFN-gamma autoantibody-associated nontuberculous myco-bacterial infection. Blood 2012, 119, 3933–3939. [Google Scholar] [CrossRef] [PubMed]
- Nagamura, N.; Imada, T. Anti-interferon-gamma autoantibody related disseminated nontuberculous mycobacteriosis with pathological features of immunoglobulin G4-related disease. Immunol. Med. 2022, 45, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.-S.; Gong, Y.-N.; Chi, C.-Y.; Hsieh, S.-Y.; Chen, W.-T.; Ku, C.-L.; Cheng, H.-T.; Lin, L.; Sung, C.M. Gut microbiome profiles and associated metabolic pathways in patients of adult-onset immunodeficiency with anti-interferon-gamma autoantibodies. Sci. Rep. 2022, 12, 1–11. [Google Scholar] [CrossRef]
- Ivashkiv, L.B. IFNγ: Signalling, epigenetics and roles in immunity, metabolism, disease and cancer immunotherapy. Nat. Rev. Immunol. 2018, 18, 545–558. [Google Scholar] [CrossRef]
- La Rocca, C.; Carbone, F.; Longobardi, S.; Matarese, G. The immunology of pregnancy: Regulatory T cells control maternal immune tolerance toward the fetus. Immunol. Lett. 2014, 162, 41–48. [Google Scholar] [CrossRef]
- Aoki, A.; Sakagami, T.; Yoshizawa, K.; Shima, K.; Toyama, M.; Tanabe, Y.; Moro, H.; Aoki, N.; Watanabe, S.; Koya, T.; et al. Clinical Significance of Interferon-gamma Neutralizing Autoantibodies Against Disseminated Nontuberculous Mycobacterial Disease. Clin. Infect. Dis. 2018, 66, 1239–1245. [Google Scholar] [CrossRef]
- Ishii, T.; Tamura, A.; Matsui, H.; Nagai, H.; Akagawa, S.; Hebisawa, A.; Ohta, K. Disseminated Mycobacterium avium complex infection in a patient carrying autoantibody to interferon-gamma. J. Infect. Chemother. 2013, 19, 1152–1157. [Google Scholar] [CrossRef]
- Koya, T.; Tsubata, C.; Kagamu, H.; Koyama, K.-I.; Hayashi, M.; Kuwabara, K.; Itoh, T.; Tanabe, Y.; Takada, T.; Gejyo, F. Anti-interferon-gamma autoantibody in a patient with disseminated Mycobacterium avium complex. J. Infect. Chemother. 2009, 15, 118–122. [Google Scholar] [CrossRef]
- Deng, J.; Ma, Y.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Association of Infection with Different SARS-CoV-2 Variants during Pregnancy with Maternal and Perinatal Outcomes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15932. [Google Scholar] [CrossRef] [PubMed]
- Minisha, F.; Farrell, T.; Abuyaqoub, S.; Rahim, A.A.; Ahmed, H.; Omer, M.; Abraham, M.; Teunissen, F.; Gassim, M. Q-PRECIOUS group Maternal risk factors of COVID-19-affected pregnancies: A comparative analysis of symptomatic and asymptomatic COVID-19 from the Q-PRECIOUS registry. Qatar Med. J. 2022, 2022, 52. [Google Scholar] [CrossRef] [PubMed]
- Asalkar, M.R.; Thakkarwad, S.M.; Bacchewad, R.P.; Sharma, N.H. Perinatal Outcome in Maternal COVID-19 infection at a Tertiary care Institute- A cross Sectional Study. J. Obstet. Gynecol. India 2022, 1–9. [Google Scholar] [CrossRef]
- Liu, H.; Shi, J.; Fok, K.L.; Chen, H. The N501Y Mutation of SARS-CoV-2 Spike Protein Impairs Spindle Assembly in Mouse Oocytes. Reprod. Sci. 2022, 29, 2842–2846. [Google Scholar] [CrossRef] [PubMed]
- Yamasoba, D.; Kimura, I.; Nasser, H.; Morioka, Y.; Nao, N.; Ito, J.; Uriu, K.; Tsuda, M.; Zahradnik, J.; Shirakawa, K.; et al. Virological characteristics of the SARS-CoV-2 Omicron BA.2 spike. Cell 2022, 185, 2103–2115.e19. [Google Scholar] [CrossRef] [PubMed]
- Washington, N.L.; Gangavarapu, K.; Zeller, M.; Bolze, A.; Cirulli, E.T.; Schiabor Barrett, K.M.; Larsen, B.B.; Anderson, C.; White, S.; Cassens, T.; et al. Emergence and rapid transmission of SARS-CoV-2 B.1.1.7 in the United States. Cell 2021, 184, 2587–2594.e2587. [Google Scholar] [CrossRef]
- Marjanovic, S.; Romanelli, R.J.; Ali, G.-C.; Leach, B.; Bonsu, M.; Rodriguez-Rincon, D.; Ling, T. COVID-19 Genomics UK (COG-UK) Consortium: Final Report. Rand. Health Q. 2022, 9, 24. [Google Scholar] [CrossRef]
- Volz, E.; Mishra, S.; Chand, M.; Berrett, J.C.; Johnson, R.; Geidelberg, L.; Hinsley, W.R.; Laydon, D.J.; Dabrera, G.; O’Toole, A.; et al. Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature 2021, 593, 266–269. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SAR-CoV-2- Negative | SARS-CoV-2- Positive | p Value | |
|---|---|---|---|
| Age (years) | 33.5 ± 5.4 | 31.1 ± 4.2 | 0.0881 |
| BMI (kg/m2) | 29.3 [25.7; 32.9] | 26.6 [22.5; 30.7] | 0.1896 |
| Comorbidity | 4 (16%) | 1 (4.2%) | 0.3487 |
| Parity | 0.0865 | ||
| One | 5 (20%) | 12 (50%) | |
| Two | 11 (44%) | 7 (29.2%) | |
| Three or more | 9 (36%) | 5 (20.8%) | |
| COVID-19 symptoms | |||
| Presence of symptoms | |||
| No | 17 (70.8%) | ||
| Yes | 7 (29.2%) | ||
| Fever | 1 (14.3%) | ||
| Mild respiratory symptoms | 6 (85.7%) | ||
| Anosmia | 2 (28.6%) | ||
| Gastro-intestinal symptoms | 2 (28.6%) | ||
| Dyspnea | 0 | ||
| Pregnancy associated complications | |||
| Gestational hypertension | 0 | 1 (4.16%) | 0.4898 |
| Preeclampsia | 0 | 0 | |
| Gestational diabetes mellitus | 0 | 0 | |
| Neonatal outcomes | |||
| SARS-CoV-2 infection | 0 | 0 | |
| Prematurity | 1 (4%) | 1 (4.16%) | |
| Apgar score | 0.0828 | ||
| ≥9 | 16 (64%) | 8 (33.3%) | |
| 8 | 7 (28%) | 14 (58.3%) | |
| ≤7 | 2 (8%) | 2 (8.4%) | |
| Data are expressed as median and range [25% percentile; 75% percentile] or as the number of cases (%). Age is expressed as media ± SD. BMI: body mass index. | |||
| Characteristic | Children Born to SARS-CoV-2-Negative Mothers | Children Born to SARS-CoV-2-Positive Mothers | p Value |
|---|---|---|---|
| Weight | 3.2 ± 0.489 Kg | 3.1 ± 0.536 Kg | 0.5879 |
| Length | 49.53 ± 1.48 cm | 49 ± 1.82 cm | 0.5384 |
| Head Circumferences | 34.18 ± 1.31 cm | 35 ± 1.08 cm | 0.2525 |
| SARS-CoV-2- Negative | SARS-CoV-2- Positive | p Value | |
|---|---|---|---|
| PCR (mg/L) | 5.5 (2.6; 7) | 4.8 (2.3; 13.7) | 0.76 b |
| WBC (×1000/μL) | 10 (7.3; 12.42) | 9.5 (6.63; 12.38) | 0.78 a |
| Neutrophils (×1000/μL) | 7.05 (5.30; 9.23) | 6.92 (4.7; 9.1) | 0.87 a |
| Lymphocytes (×1000/μL) | 1.67 (1.48; 2.31) | 1.3 (1; 1.7) | 0.0093 a |
| Monocytes (×1000/μL) | 0.54 (0.34; 0.72) | 0.51 (0.34; 0.62) | 0.42 a |
| Platelets (×1000/μL) | 201 (165.7; 246.75) | 198.5 (179.2; 251.5) | 0.66 a |
| Results are expressed as median and range [25% percentile; 75% percentile]— a: unpaired t-test; b: Mann–Whitney U test | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cennamo, M.; La Civita, E.; Sarno, L.; Carbone, G.; Di Somma, S.; Cabaro, S.; Troisi, J.; Sirico, A.; Improda, F.P.; Guida, M.; et al. Low Interferon-γ Levels in Cord and Peripheral Blood of Pregnant Women Infected with SARS-CoV-2. Microorganisms 2023, 11, 223. https://doi.org/10.3390/microorganisms11010223
Cennamo M, La Civita E, Sarno L, Carbone G, Di Somma S, Cabaro S, Troisi J, Sirico A, Improda FP, Guida M, et al. Low Interferon-γ Levels in Cord and Peripheral Blood of Pregnant Women Infected with SARS-CoV-2. Microorganisms. 2023; 11(1):223. https://doi.org/10.3390/microorganisms11010223
Chicago/Turabian StyleCennamo, Michele, Evelina La Civita, Laura Sarno, Gianluigi Carbone, Sarah Di Somma, Serena Cabaro, Jacopo Troisi, Angelo Sirico, Francesco Paolo Improda, Maurizio Guida, and et al. 2023. "Low Interferon-γ Levels in Cord and Peripheral Blood of Pregnant Women Infected with SARS-CoV-2" Microorganisms 11, no. 1: 223. https://doi.org/10.3390/microorganisms11010223