Abstract
We performed a prospective study to evaluate the diagnostic accuracy of nucleotide matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS) in identifying nontuberculous mycobacterium (NTM) from clinical respiratory samples. A total of 175 eligible patients were prospectively enrolled, including 108 patients diagnosed with NTM pulmonary disease (NTM-PD) and 67 control patients with other diseases. All specimens were subjected to acid-fast staining, liquid culture combined with MPT64 antigen detection, and a nucleotide MALDI-TOF MS assay. NTM cultures were also subjected to the MeltPro Myco assay for species identification. Altogether, the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of nucleotide MALDI-TOF MS were 77.8% (95% CI: 68.6–85.0%), 92.5% (82.8–97.2%), 94.4% (86.8–97.9%), and 72.1% (61.2–81.0%), respectively; these results were not statistically different from the results of culture + MPT64 antigen testing (75.0% [65.6–82.6%], 95.5% [86.6–98.8%], 96.4% [89.2–99.1%], and 70.3% [59.7–79.2%], respectively). In the identification of NTM species, of the 84 nucleotide MALDI-TOF MS positive samples, 77 samples (91.7%) were identified at the species level. Using culture + MeltPro Myco assay as the reference standard, nucleotide MALDI-TOF MS correctly identified 77.8% (63/81) of NTM species. Our results demonstrated that the nucleotide MALDI-TOF MS assay was a rapid single-step method that provided the reliable detection of NTM and identification of NTM species. This new method had the same sensitivity and specificity as the culture + MPT64 antigen method, but was much more rapid.
1. Introduction
Human diseases caused by nontuberculous mycobacteria (NTM) have increased in prevalence worldwide during recent years [1]. For example, a study of NTM pulmonary disease in Canada reported 29.3 cases/100,000 persons for the period of 1998 to 2002 and 41.3 cases/100,000 persons for the period of 2006 to 2010 [2]. In mainland China, a comprehensive review and meta-analysis of qualified data estimated the prevalence of NTM infections prior to 2015 was 6.3% among suspected tuberculosis patients [3,4,5]. Although diseases caused by NTM are not as common as those from the Mycobacterium tuberculosis (MTB) complex, patients with NTM infections typically have a long course of disease and a high rate of drug resistance and treatment failure.
Identification of the species and subspecies responsible for NTM infections is important so that appropriate therapeutic regimens can be administered, and species identification has a clear impact on patient outcome and prognosis [6]. Clinical laboratories use multiple molecular methods for the identification of NTM species, such as nucleic acid hybridization assays, line probe assays, DNA sequencing, real-time PCR, and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), and each method has advantages and limitations [7].
Clinical laboratories commonly use proteomic MALDI-TOF MS, a technique that matches the protein profile of an isolate to a reference dataset. This method can identify pathogens isolated from a single colony at the species level with high efficiency, high accuracy, and low cost, and is therefore commonly used to identify Gram-negative and Gram-positive bacteria, including mycobacteria [8]. Improvements in several specific procedures have increased the discriminatory power of proteomic MALDI-TOF MS. For example, a recent study used proteomic MALDI-TOF MS to distinguish pulmonary tuberculosis in sputum samples and achieved a sensitivity of 80% and a specificity of 89% [9]. Moreover, MALDI-TOF MS can be used to test multiple biological samples, including urine [10,11] and cerebrospinal fluid [12,13]. Nevertheless, proteomic MALDI-TOF MS cannot be used for the identification of NTM at present [8].
Recent studies have used nucleotide MALDI-TOF MS, a new application that is based on unique and characteristic nucleotide profiles, for the identification of mutations that promote cancer [14,15]. Another study reported promising results from the use of this new method for the direct analysis of sputum samples and identification of MTB and mutations related to resistance [16]. Compared with phenotypic measurements of drug resistance, the consistency from nucleotide MALDI-TOF MS was 91.3% for detecting mutations in related genes [16]. However, in terms of the species identification of NTM, data from real-world studies using nucleotide MALDI-TOF MS assays remain scarce.
Considering the high sensitivity, specificity, and accuracy of the nucleotide MALDI-TOF MS assay, we evaluated the accuracy of this method in identifying NTM from clinical respiratory samples.
2. Materials and Methods
2.1. Study Population
Prospective enrollment of patients with suspected NTM pulmonary infections who were admitted to Shanghai Pulmonary Hospital affiliated with Tongji University was performed from November 2020 to October 2021. The inclusion criteria were: (1) age over 14 years; (2) HIV-negativity; (3) pulmonary or systemic symptoms and imaging findings (nodular or cavitary shadows with bronchiectasis accompanied by multiple small nodules) leading to suspicion of NTM pulmonary disease; and (4) NTM pulmonary disease that was not treated during the previous 60 days. The exclusion criteria were: (1) diagnosis with both NTM and MTB infections and (2) inability to expectorate sputum and refusal of a bronchoscopy examination.
The diagnostic criteria for NTM pulmonary disease were according to the American Thoracic Society (ATS) guidelines (2020 edition) [17] and the NTM guideline for China [18]. During hospitalization, every patient was provided with several sputum tubes for other tests, including additional culture and GeneXpert MTB/RIF, after providing the required sputum samples as a routine procedure to improve diagnostic accuracy. A total of 175 patients were included, where 108 patients met the reference diagnostic criteria for NTM pulmonary disease and 67 control patients were diagnosed with non-NTM pulmonary disease.
2.2. Sample Collection
Patients included in the study provided sputum samples at any time within 7 days of hospital admission. Each sputum sample (at least 5 mL) was collected over the course of 16 h. Different sputum samples were subjected to acid-fast staining, BACTEC MGIT 960 culture, and nucleotide MALDI-TOF MS detection.
Patients who were unable to provide sputum samples underwent bronchoscopy to obtain samples of bronchoalveolar lavage fluid (BALF). For collection of a BALF sample, sterile saline was instilled into the site of the lung lesion (based on imaging results) through the bronchoscope, and fluid was recovered into a sterile tube. The obtained sputum and BALF samples were used for subsequent acid-fast staining, BACTEC MGIT 960 culture, and nucleotide MALDI-TOF MS detection. Positive cultures obtained from the MGIT 960 culture were subjected to further analysis. The culture suspension was tested using the MPT64 antigen detection kit, and the culture sediment was identified by multi-color melting curve analysis.
2.3. Acid-Fast Staining, MGIT 960 Culture, MPT64 Antigen Assay, and MeltPro Myco Assay
Each collected specimen was liquefied and centrifuged to obtain a precipitate. The sediment smear was fixed for anti-acid bacilli (AFB) staining, followed by microscopy examination [19].
The specimens were inoculated into MGIT tubes and incubated in the MGIT960 instrument (BACTEC MGIT 960 culture; BD Microbiology Systems, Franklin Lakes, NJ, USA). For a positive culture, the culture supernatant was tested using the MPT64 antigen detection kit (Genesis Corporation, Hangzhou, China), and the culture products were analyzed by multicolor melting curve analysis (MeltPro Myco assay, Zeesan Biotech, Xiamen, China) for species identification exactly according to the instructions. This method can identify 19 NTM species [20].
2.4. Nucleotide MALDI-TOF MS Procedures
The nucleotide MALDI-TOF MS procedure used the Conlight Myco kit, which was established and performed by Shanghai Conlight Medical Laboratory Co., Ltd. (Shanghai, China) as previously described in detail [16,21]. Briefly, this procedure had five steps and can be completed in about 3 days. The first step used the PCR. A PCR mixture (Table S1; 1.3 μL of ddH2O, 0.5 μL of 10× PCR buffer with 20 mM MgCl2, 0.4 μL of 20 mM MgCl2, 0.1 μL of 25 mM dNTP mix, 0.5 μL of 1 μM primer mix, 0.2 μL of 5 U/μL PCR enzyme, and 5 μL of 5 ng/µL DNA template) was added into the wells of a 96-well plate, and PCR was then performed. A blank control (2 µL ddH2O), negative control (2 µL DNA extraction eluate), and positive control were performed at the same time.
The second step used the shrimp alkaline phosphatase (SAP) assay. A 2 µL aliquot of the SAP mixture (1.53 μL of ddH2O, 0.17 μL of SAP buffer, and 0.30 μL of SAP enzyme) was added into each well of a PCR plate, and the total volume was adjusted to 7 µL. The sealed plate was centrifuged at 4000× g for 5 s and then incubated at 37 °C for 40 min and 85 °C for 5 min.
The third step used PCR extension (Tables S2 and S3). A 2 µL aliquot of the iPLEX extension mix (0.62 µL of ddH2O, 0.2 µL of iPLEX buffer, 0.2 µL of iPLEX termination mix, 0.94 µL of extension primer mix, and 0.04 µL of iPLEX enzyme) was added into each well of a PCR plate, followed by the extension reaction.
The fourth step used sample desalination. Clean resin on a 96/15 mg dimple plate was air-dried for at least 10 min. Then, 41 μL of water was added into each well, followed by the application of sealing film and centrifugation (3200× g, 5 min). Then, 15 mg of resin was added to the reaction products according to the manufacturer’s protocol (Agena Bioscience, San Diego, CA, USA). The sealing film was applied, and the contents were mixed by inversion and rotated for 15 min. Centrifugation was then performed at 3200× g for 5 min.
The fifth step used MS. The PCR product was transferred to the SpectroCHIP according to the MassARRAY Nanodispenser operating instructions. Automatic analysis of the results was performed using MassARRAY analysis software (MassArrayTyper Version 4.1) (Figure S1).
2.5. Statistical Analysis
The values for sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy with 95% confidence intervals (CIs) were determined using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). Consistency was determined using the Kappa test, and the results were classified as almost perfect (Kappa ≥ 0.8), substantial (0.6 < Kappa < 0.8), moderate (0.4 < Kappa < 0.6), fair (0.2 < Kappa < 0.4), or slight (Kappa < 0.2). The χ2 test, Fisher’s test, or the t-test was used to verify the significance of differences between the NTM pulmonary disease group and the control group.
2.6. Ethical Approval
All procedures were approved by the Ethics Review Committee of Shanghai Pulmonary Hospital (L21-002). Written informed consent was obtained from all participants upon enrollment. This study was conducted according to the principles of the Declaration of Helsinki of the World Medical Association and according to Good Clinical Practice Guidelines.
3. Results
3.1. Study Design and Characteristics of Enrolled Cases
We evaluated the value of nucleotide MALDI-TOF MS technology in identifying NTM in patients by conducting a prospective study at Shanghai Pulmonary Hospital from November 2020 to October 2021 (Figure 1 and Figure 2). According to the inclusion and exclusion criteria, we enrolled 175 patients with suspected or confirmed NTM pulmonary disease after they provided informed consent. All diagnoses strictly followed the NTM pulmonary disease criteria established by the 2020 ATS clinical practice guideline [17] and the criteria for NTM pulmonary disease in China [18]. There were 108 patients in the NTM pulmonary disease group and 67 patients in non-NTM pulmonary disease (control) group. Each included patient provided sputum samples or a BALF sample, which was subjected to analysis by acid-fast staining, MGIT 960 culture, and nucleotide MALDI-TOF MS. For culture-positive samples, MPT64 antigen detection and multicolor melting curve analyses were also performed; the first test was for NTM detection, and the second test was for NTM species identification (Figure 1).
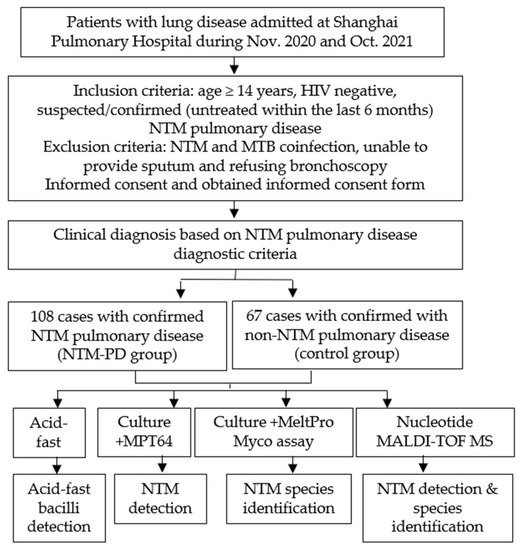
Figure 1.
Study design.
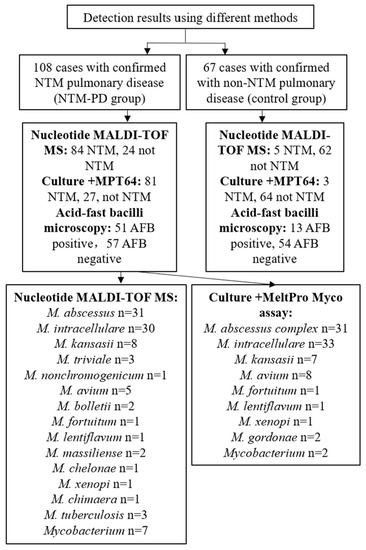
Figure 2.
Results of NTM detection and species identification using different methods.
The NTM pulmonary disease group and the control group had no significant differences in age, gender, or major symptoms. However, the chest CT results showed a higher incidence of nodules (p = 0.010) and bronchiectasis (p = 0.021) in the NTM pulmonary disease group. Additionally, the percentage of sputum samples was greater in the control group (73.1% vs. 51.9%, p = 0.005) (Table 1).

Table 1.
Demographic and clinical characteristics of the NTM pulmonary disease group and the control group.
3.2. Diagnostic Performance of NTM Identification by Nucleotide MALDI-TOF MS
Based on the reference standard of clinical diagnosis, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of nucleotide MALDI-TOF MS for detection of NTM were 77.8% (95% CI: 68.6–85.0%), 92.5% (82.8–97.2%), 94.4% (86.8–97.9%), 72.1% (61.2–81.0%), and 83.4% (76.9–88.5%), respectively. The corresponding values for culture combined with MPT64 antigen detection were 75.0% (65.6–82.6%), 95.5% (86.6–98.8%), 96.4% (89.2–99.1%), 70.3% (59.7–79.2%), and 82.9% (76.3–88.0%), respectively. The corresponding values for acid-fast staining microscopy were 47.2% (37.6–57.0%), 80.6% (68.8–88.9%), 79.7% (67.4–88.3%), 48.7% (39.1–58.3%), and 60.0% (52.3–67.2%), respectively (Table 2). Thus, nucleotide MALDI-TOF MS detection of NTM performed similarly to culture combined with MPT64 antigen detection (no statistically significant differences), but both of these methods were significantly better than acid-fast staining microscopy. Using the Kappa test to assess the consistency of the three methods with the reference standard of clinical diagnosis, the Kappa for culture combined with MPT64 antigen detection was 0.66, and the Kappa for nucleotide MALDI-TOF MS was 0.67, indicating substantial consistency for both methods. However, the Kappa for acid-fast staining microscopy was only 0.25, indicating fair consistency (Table 2).
Table 2.
Diagnostic performance of the AFB, culture + MTP64 antigen, and nucleotide MALDI-TOF MS methods.
We then analyzed the ability of nucleotide MALDI-TOF MS and culture combined with MPT64 antigen testing to detect NTM in patients with positive or negative acid-fast staining microscopy results. In patients with positive acid-fast staining microscopy results, the sensitivity of culture combined with MTP64 antigen detection was 92.2% (80.3–97.5%), the same as nucleotide MALDI-TOF MS. In patients with negative acid-fast staining microscopy results, the sensitivity of culture combined with MTP64 antigen detection was 59.7% (45.8–72.2%) and that of nucleotide MALDI-TOF MS was 64.9% (51.1–76.8%). There were no statistically significant differences in the sensitivity of the two detection methods in patients with either positive or negative acid-fast staining microscopy results (Table 3). The AUCs of the ROC curves for acid-fast staining microscopy, culture combined with MPT64 antigen detection, and nucleotide MALDI-TOF MS were 0.639 (0.556–0.722), 0.853 (0.794–0.911), and 0.852 (0.792–0.911), respectively (Table 2 and Figure 3). The results from nucleotide MALDI-TOF MS detection were consistently comparable to those from culture combined with MPT64 antigen detection, but the nucleotide MALDI-TOF MS technique required significantly less time.
Table 3.
Sensitivity of nucleotide MALDI-TOF MS and culture + MPT64 antigen in detecting NTM pulmonary disease in smear-positive and smear-negative patients.
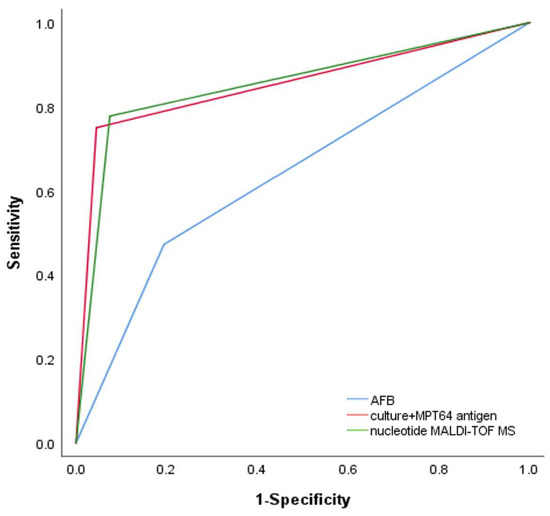
Figure 3.
Receiver operating characteristic (ROC) curves for diagnosis of NTM using AFB (AUC: 0.639, 95% CI: 0.556, 0.722), culture + MPT64 antigen (AUC: 0.853, 95% CI: 0.794, 0.911), and nucleotide MALDI-TOF MS (AUC: 0.852, 95% CI: 0.792, 0.911).
3.3. Identification of NTM Species by Nucleotide MALDI-TOF MS
In theory, nucleotide MALDI-TOF MS can detect any NTM species based on the presence of specific single nucleotide polymorphisms (SNPs). We found that nucleotide MALDI-TOF MS was able to detect most clinically common and disease-associated NTM species. To evaluate its ability to identify NTM species, we performed on samples from the NTM pulmonary disease group. Of the 84 nucleotide MALDI-TOF MS positive samples, we identified 77 samples (91.7%) at the species level. The most common species were M. abscessus (36.9%, 31/84), M. intracellulare (35.7%, 30/84), and M. kansasii (9.5%, 8/84) (Figure 4a). At the same time, we also performed species identification on cultures using a melting curve analysis as the reference standard. Of the 81 culture-positive samples, we identified 79 samples (97.5%) at the species level (total of 8 species), and the most common species were M. intracellulare (40.7%, 33/81), M. abscessus complex (38.3%, 31/81), and M. avium (9.9%, 8/81) (Figure 4b).
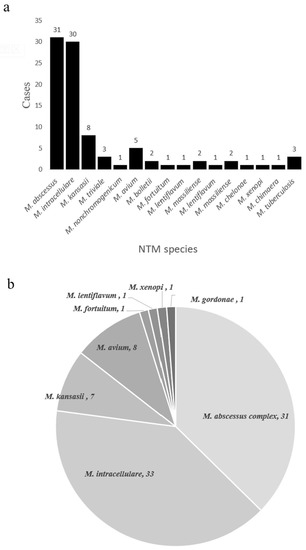
Figure 4.
NTM species identified using the nucleotide MALDI-TOF MS assay (a) and the culture + MeltPro Myco assay (b).
To assess the consistency of bacterial identification from nucleotide MALDI-TOF MS and melting curve analysis, we used 81 culture-positive NTM samples for an in-depth analysis. Among them, 18 samples (22.2%) yielded inconsistent results, including 13 samples (16.0%) that had positive culture results and negative nucleotide MALDI-TOF MS results; five samples (6.2%) had completely inconsistent results with two methods. Two samples were identified as M. avium by culture and melting curve analysis, but nucleotide MALDI-TOF MS detected M. abscessus. Three samples were identified as M. intracellulare by culture and melting curve analysis, but nucleotide MALDI-TOF MS only identified Mycobacterium sp. (Table 4). The consistency rate of the two methods was 77.8% (63/81).
Table 4.
Inconsistency of NTM species identification using different methods.
4. Discussion
The clinical practice guidelines of numerous scientific societies recommend the use of validated molecular or mass spectrometry techniques for the identification of NTM isolates at the species level [17,22]. Nevertheless, proteomic MALDI-TOF MS can only be applied to pure cultures, and achieves better performance when using solid media instead of liquid media [23,24]. A recent study used proteomic MALDI-TOF MS of clinical samples to distinguish MTB from the non-TB but with a lower respiratory tract infection using sputum samples and reported a sensitivity of 80% and a specificity of 89% [9]. Nucleotide MALDI-TOF MS can also identify MTB from raw smear-negative cases, and its reported sensitivity was 61.9% and failure rate was 11.3% [16]. In our setting, nucleotide MALDI-TOF MS had a sensitivity of 77.8% and a specificity of 92.5% in detecting NTM, similar to the method of culture + MPT64 antigen testing. Our sensitivity was 64.9% for smear-negative NTM patients, similar to a prior report [16]. We also found that a single test missed 52.8% of NTM cases by smear and 20.4% of cases by culture. A previous study reported that missed culture-negative patients may progress to NTM lung infection within one year [25]. A positive smear result requires 5000 to 10,000 AFB/µL of sputum and a positive culture result requires 10 to 100 AFB/μL of sputum [26]. However, nucleotide MALDI-TOF MS has a detection limit of only about 10 MTB chromosomal DNA copies [16]. Two other advantages of nucleotide MALDI-TOF MS are that it has the same diagnostic performance as culturing and it is much faster than culture, in that the entire procedure only requires about 3 days.
It should be noted that our results regarding the distribution of different NTM species in China differ from previous studies. A 2013 nationwide survey of China reported the five most frequently isolated NTM species were the M. abscessus complex (36.0%), M. avium-intracellulare complex (34.1%), M. kansasii (9.8%), M. paragordonae (5.4%), and M. lentiflavum (3.2%) [4]. A 2016 systematic review showed that southern China had a significantly higher percentage of rapidly growing mycobacteria than northern China [3]. However, a 2020 study of 17 hospitals in China reported the dominant NTM species was M. intracellulare, followed by the M. abscessus complex [5]. In our study, the major NTM species was M. intracellulare (40.7%) followed by the M. abscessus complex (38.3%). Differences in the years of sample collection and the geographic locations of the study populations might account for these inconsistent results. Nevertheless, we confirmed that the M. avium-intracellulare complex and M. abscessus complex are still the predominant NTM in China.
Our results showed that nucleotide MALDI-TOF MS identified more than one species in 11 of the NTM samples and that two samples each had three NTM species. The MeltPro Myco assay only identified NTM-coinfection in 5 samples. We also identified MTB in three of the nucleotide MALDI-TOF MS samples (Figure 4a); two of these samples were BALF, and they all had a negative result in the GeneXpert MTB/RIF assay. Based on additional laboratory results, we ruled out a diagnosis of MTB in these three patients. False-positive results for MTB are common because dead MTB cannot be detected by culture and because China has a high prevalence of TB. Considering that nucleotide MALDI-TOF MS includes multiple PCR procedures and targets more than one target of MTB, the procedure should be used with caution in the diagnosis of active MTB, especially in patients with previous MTB infections and in patients from regions with a high TB burden. Our nucleotide MALDI-TOF MS results also identified other non-pathogenic species, M. triviale (n = 3) and M. nonchromogenicum (n = 1), which are only rarely responsible for disease in humans. NTM coinfection can lead to a more severe clinical outcome, and a previous study reported the incidence of coinfection was 13.5% [25]. Another study of patients receiving treatment for pulmonary M. abscessus infection reported that those with mixed infections had significantly worse outcomes [27]. It is hard to know if these coinfecting pathogens were clinically relevant or were just incidental and clinically irrelevant infections of the respiratory tract [28]. A repeated culture with an identification procedure is needed to determine if additional patients had coinfections that were undetected by culture [25].
Our study has several limitations. First, the MeltPro Myco test may underestimate NTM coinfection, and this will affect the consistency of the nucleotide MALDI-TOF MS in NTM species identification. Second, we did not perform a sequencing analysis of the five samples in which the two methods identified inconsistent NTM species, and this may have affected our reported consistency rate. Third, sputum cultures and nucleotide MALDI-TOF MS testing were not performed on the same samples, and this could have led to a lack of consistency. This study design required the collection of sputum samples within seven days of admission, and patients were carefully instructed on how to produce sputum samples, but there might have been some subtle differences among patients in the methods of sample collection [29].
5. Conclusions
In summary, nucleotide MALDI-TOF MS provides the rapid and sensitive detection of NTM from a single sputum sample or BALF sample, especially in culture-negative patients. Although nucleotide MALDI-TOF MS identified more species than the MeltPro Myco assay, there are several possible reasons for this difference, so these results should be interpreted with caution.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/microorganisms11081975/s1, Figure S1: Nucleotide MALDI-TOF MS mass spectra for representative species. I: M. avium, II: M. intracellulare, III: M. massiliense, IV: M. kansasii; Table S1: PCR primers used for identification of NTM species; Table S2: Primers used for PCR extension; Table S3: Procedure used for the iPLEX extension reaction.
Author Contributions
Conceptualization, J.G. and W.S.; methodology, X.W.; software, J.Y.; validation, L.Y., X.G. and Y.F.; formal analysis, W.S.; investigation, L.Y.; resources, W.S.; data curation, J.Y.; writing—original draft preparation, L.Y.; writing—review and editing, J.G.; visualization, X.W.; supervision, Y.F. and Q.S.; project administration, L.Y.; funding acquisition, W.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Shanghai Clinical research center for infectious disease (tuberculosis), grant number 19MC1910800, Clinical Research Plan of SHDC, grant number SHDC12022108 and SHDC2020CR6024 and Shanghai Key Clinical Specialty Construction Project (tuberculosis), grant number shslezdzk03001.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank all physicians and laboratory staff at Shanghai Pulmonary Hospital for assistance.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Brode, S.K.; Daley, C.L.; Marras, T.K. The Epidemiologic Relationship between Tuberculosis and Non-Tuberculous Mycobacterial Disease: A Systematic Review. Int. J. Tuberc. Lung Dis. 2014, 18, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Marras, T.K.; Mendelson, D.; Marchand-Austin, A.; May, K.; Jamieson, F.B. Pulmonary Nontuberculous Mycobacterial Disease, Ontario, Canada, 1998–2010. Emerg. Infect. Dis. 2013, 19, 1889–1891. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Liu, P.; Liu, G.; Zhao, L.; Hu, Y.; Wei, G.; Luo, J.; Huang, H. The Prevalence of Non-Tuberculous Mycobacterial Infections in Mainland China: Systematic Review and Meta-Analysis. J. Infect. 2016, 73, 558–567. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-F.; Song, Y.-M.; He, W.-C.; Liu, D.-X.; He, P.; Bao, J.-J.; Wang, X.-Y.; Li, Y.-M.; Zhao, Y.-L. Nontuberculous Mycobacteria in China: Incidence and Antimicrobial Resistance Spectrum from a Nationwide Survey. Infect. Dis. Poverty 2021, 10, 59. [Google Scholar] [CrossRef]
- Tan, Y.; Deng, Y.; Yan, X.; Liu, F.; Tan, Y.; Wang, Q.; Bao, X.; Pan, J.; Luo, X.; Yu, Y.; et al. Nontuberculous Mycobacterial Pulmonary Disease and Associated Risk Factors in China: A Prospective Surveillance Study. J. Infect. 2021, 83, 46–53. [Google Scholar] [CrossRef]
- Chae, H.; Han, S.J.; Kim, S.-Y.; Ki, C.-S.; Huh, H.J.; Yong, D.; Koh, W.-J.; Shin, S.J. Development of a One-Step Multiplex PCR Assay for Differential Detection of Major Mycobacterium Species. J. Clin. Microbiol. 2017, 55, 2736–2751. [Google Scholar] [CrossRef]
- Huh, H.J.; Kim, S.-Y.; Jhun, B.W.; Shin, S.J.; Koh, W.-J. Recent Advances in Molecular Diagnostics and Understanding Mechanisms of Drug Resistance in Nontuberculous Mycobacterial Diseases. Infect. Genet. Evol. 2019, 72, 169–182. [Google Scholar] [CrossRef]
- Hou, T.-Y.; Chiang-Ni, C.; Teng, S.-H. Current Status of MALDI-TOF Mass Spectrometry in Clinical Microbiology. J. Food Drug Anal. 2019, 27, 404–414. [Google Scholar] [CrossRef]
- Dao, T.L.; Hoang, V.T.; Ly, T.D.A.; Lagier, J.C.; Baron, S.A.; Raoult, D.; Parola, P.; Courjon, J.; Marty, P.; Chaudet, H.; et al. Sputum Proteomic Analysis for Distinguishing between Pulmonary Tuberculosis and Non-Tuberculosis Using Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS): Preliminary Results. Clin. Microbiol. Infect. 2021, 27, 1694.e1–1694.e6. [Google Scholar] [CrossRef]
- Li, W.; Sun, E.; Wang, Y.; Pan, H.; Zhang, Y.; Li, Y.; Zhang, X.; Li, C.; Du, L.; Wang, C. Rapid Identification and Antimicrobial Susceptibility Testing for Urinary Tract Pathogens by Direct Analysis of Urine Samples Using a MALDI-TOF MS-Based Combined Protocol. Front. Microbiol. 2019, 10, 1182. [Google Scholar] [CrossRef]
- İlki, A.A.; Özsoy, S.; Gelmez, G.; Aksu, B.; Söyletir, G. An Alternative for Urine Cultures: Direct Identification of Uropathogens from Urine by MALDI-TOF MS. Acta Microbiol. Immunol. Hung. 2020, 67, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Holland, R.D.; Wilkes, J.G.; Rafii, F.; Sutherland, J.B.; Persons, C.C.; Voorhees, K.J.; Lay, J.O. Rapid Identification of Intact Whole Bacteria Based on Spectral Patterns Using Matrix-Assisted Laser Desorption/Ionization with Time-of-Flight Mass Spectrometry. Rapid Commun. Mass Spectrom. 1996, 10, 1227–1232. [Google Scholar] [CrossRef]
- Bishop, B.; Geffen, Y.; Plaut, A.; Kassis, O.; Bitterman, R.; Paul, M.; Neuberger, A. The Use of Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry for Rapid Bacterial Identification in Patients with Smear-Positive Bacterial Meningitis. Clin. Microbiol. Infect. 2018, 24, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Su, K.-Y.; Chen, H.-Y.; Li, K.-C.; Kuo, M.-L.; Yang, J.C.-H.; Chan, W.-K.; Ho, B.-C.; Chang, G.-C.; Shih, J.-Y.; Yu, S.-L.; et al. Pretreatment Epidermal Growth Factor Receptor (EGFR) T790M Mutation Predicts Shorter EGFR Tyrosine Kinase Inhibitor Response Duration in Patients With Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2012, 30, 433–440. [Google Scholar] [CrossRef]
- Su, K.-Y.; Kao, J.-T.; Ho, B.-C.; Chen, H.-Y.; Chang, G.-C.; Ho, C.-C.; Yu, S.-L. Implementation and Quality Control of Lung Cancer EGFR Genetic Testing by MALDI-TOF Mass Spectrometry in Taiwan Clinical Practice. Sci. Rep. 2016, 6, 30944. [Google Scholar] [CrossRef]
- Su, K.Y.; Yan, B.S.; Chiu, H.C.; Yu, C.J.; Chang, S.Y.; Jou, R.; Liu, J.L.; Hsueh, P.R.; Yu, S.L. Rapid Sputum Multiplex Detection of the M. Tuberculosis Complex (MTBC) and Resistance Mutations for Eight Antibiotics by Nucleotide MALDI-TOF MS. Sci. Rep. 2017, 7, 41486. [Google Scholar] [CrossRef]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J.; Andrejak, C.; Böttger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of Nontuberculous Mycobacterial Pulmonary Disease: An Official ATS/ERS/ESCMID/IDSA Clinical Practice Guideline. Clin. Infect. Dis. 2020, 71, 905–913. [Google Scholar] [CrossRef]
- Chinese Medical Association Tuberculosis Branch. Guideline for Diagnosis and Treatment of Nontuberculous mycobacteria Disease (2020 Edition). Chin. J. Tuberc. Respir. Dis. 2020, 43, 918–946. [Google Scholar] [CrossRef]
- Forbes, B.A.; Hall, G.S.; Miller, M.B.; Novak, S.M.; Rowlinson, M.C.; Salfinger, M.; Somoskövi, A.; Warshauer, D.M.; Wilson, M.L. Practical Guidance for Clinical Microbiology Laboratories: Mycobacteria. Clin. Microbiol. Rev. 2018, 31, e00038-17. [Google Scholar] [CrossRef]
- Xu, Y.; Liang, B.; Du, C.; Tian, X.; Cai, X.; Hou, Y.; Li, H.; Zheng, R.; Li, J.; Liu, Y.; et al. Rapid Identification of Clinically Relevant Mycobacterium Species by Multicolor Melting Curve Analysis. J. Clin. Microbiol. 2019, 57, e01096-18. [Google Scholar] [CrossRef]
- Wu, X.; Tan, G.; Yang, J.; Guo, Y.; Huang, C.; Sha, W.; Yu, F. Prediction of Mycobacterium Tuberculosis Drug Resistance by Nucleotide MALDI-TOF-MS. Int. J. Infect. Dis. 2022, 121, 47–54. [Google Scholar] [CrossRef]
- Haworth, C.S.; Banks, J.; Capstick, T.; Fisher, A.J.; Gorsuch, T.; Laurenson, I.F.; Leitch, A.; Loebinger, M.R.; Milburn, H.J.; Nightingale, M.; et al. British Thoracic Society Guidelines for the Management of Non-Tuberculous Mycobacterial Pulmonary Disease (NTM-PD). Thorax 2017, 72, ii1–ii64. [Google Scholar] [CrossRef]
- Buchan, B.W.; Riebe, K.M.; Timke, M.; Kostrzewa, M.; Ledeboer, N.A. Comparison of MALDI-TOF MS With HPLC and Nucleic Acid Sequencing for the Identification of Mycobacterium Species in Cultures Using Solid Medium and Broth. Am. J. Clin. Pathol. 2014, 141, 25–34. [Google Scholar] [CrossRef][Green Version]
- Leyer, C.; Gregorowicz, G.; Mougari, F.; Raskine, L.; Cambau, E.; de Briel, D. Comparison of Saramis 4.12 and IVD 3.0 Vitek MS Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry for Identification of Mycobacteria from Solid and Liquid Culture Media. J. Clin. Microbiol. 2017, 55, 2045–2054. [Google Scholar] [CrossRef]
- Naito, K.; Noguchi, S.; Yatera, K.; Kawanami, T.; Yamasaki, K.; Fukuda, K.; Ikegami, H.; Akata, K.; Kido, T.; Sakamoto, N.; et al. Coinfection with Multiple Nontuberculous Mycobacteria as a Possible Exacerbating Factor in Pulmonary Nontuberculous Mycobacteriosis: Clone Library Analysis Using the 16S Ribosomal RNA Gene. Chest 2020, 158, 2304–2313. [Google Scholar] [CrossRef]
- Kehinde Aderemi, O.; Dada-Adegbola, H. Epidemiology of Smear—Negative Tuberculosis in Ibadan, Nigeria. Afr. J. Infect. Dis. 2013, 7, 14–17. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Furuta, K.; Ito, A.; Ishida, T.; Ito, Y.; Sone, N.; Takaiwa, T.; Yokoyama, T.; Tachibana, H.; Arita, M.; Hashimoto, T. 18 Cases of Pulmonary Mycobacterium Abscessus: Clinical Difference Depending on the Presence or Absence of Mycobacterium Avium Complex. J. Infect. Chemother. 2016, 22, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Porvaznik, I.; Solovič, I.; Mokrý, J. Non-Tuberculous Mycobacteria: Classification, Diagnostics, and Therapy. Adv. Exp. Med. Biol. 2016, 944, 19–25. [Google Scholar]
- Datta, S.; Shah, L.; Gilman, R.H.; Evans, C.A. Comparison of Sputum Collection Methods for Tuberculosis Diagnosis: A Systematic Review and Pairwise and Network Meta-Analysis. Lancet Glob. Health 2017, 5, e760–e771. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).