_Di_Marco.png)

Comparative Analysis of Microbial Species and Multidrug Resistance Patterns Associated with Lower Urinary Tract Infections in Preterm and Full-Term Births

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Framework and Ethical Considerations
2.2. Participant Selection and Definitions
2.3. Study Variables
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Literature Findings
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mitrogiannis, I.; Evangelou, E.; Efthymiou, A.; Kanavos, T.; Birbas, E.; Makrydimas, G.; Papatheodorou, S. Risk factors for preterm birth: An umbrella review of meta-analyses of observational studies. BMC Med. 2023, 21, 494. [Google Scholar] [CrossRef] [PubMed]
- Kurian, N.K.; Modi, D. Mechanisms of group B Streptococcus-mediated preterm birth: Lessons learnt from animal models. Reprod. Fertil. 2022, 3, R109–R120. [Google Scholar] [CrossRef]
- Bianchi-Jassir, F.; Seale, A.C.; Kohli-Lynch, M.; Lawn, J.E.; Baker, C.J.; Bartlett, L.; Cutland, C.; Gravett, M.G.; Heath, P.T.; Ip, M.; et al. Preterm Birth Associated With Group B Streptococcus Maternal Colonization Worldwide: Systematic Review and Meta-analyses. Clin. Infect. Dis. 2017, 65, S133–S142. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.J.; Nidey, N.; Bandoli, G.; Chambers, B.D.; Chambers, C.D.; Feuer, S.; Karasek, D.; Oltman, S.P.; Rand, L.; Ryckman, K.K.; et al. Risk of Early Birth among Women with a Urinary Tract Infection: A Retrospective Cohort Study. AJP Rep. 2021, 11, e5–e14. [Google Scholar] [CrossRef] [PubMed]
- Werter, D.E.; Kazemier, B.M.; Schneeberger, C.; Mol, B.W.J.; de Groot, C.J.M.; Geerlings, S.E.; Pajkrt, E. Risk Indicators for Urinary Tract Infections in Low Risk Pregnancy and the Subsequent Risk of Preterm Birth. Antibiotics 2021, 10, 1055. [Google Scholar] [CrossRef]
- Urinary Tract Infections in Pregnant Individuals. Obstet. Gynecol. 2023, 142, 435–445. [CrossRef] [PubMed]
- Mancuso, G.; Midiri, A.; Gerace, E.; Marra, M.; Zummo, S.; Biondo, C. Urinary Tract Infections: The Current Scenario and Future Prospects. Pathogens 2023, 12, 623. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.D.; Hultgren, S.J. Urinary tract infections: Microbial pathogenesis, host-pathogen interactions and new treatment strategies. Nat. Rev. Microbiol. 2020, 18, 211–226. [Google Scholar] [CrossRef]
- Tabibian, J.H.; Gornbein, J.; Heidari, A.; Dien, S.L.; Lau, V.H.; Chahal, P.; Churchill, B.M.; Haake, D.A. Uropathogens and host characteristics. J. Clin. Microbiol. 2008, 46, 3980–3986. [Google Scholar] [CrossRef]
- Storme, O.; Tirán Saucedo, J.; Garcia-Mora, A.; Dehesa-Dávila, M.; Naber, K.G. Risk factors and predisposing conditions for urinary tract infection. Ther. Adv. Urol. 2019, 11, 1756287218814382. [Google Scholar] [CrossRef]
- Meštrović, T.; Matijašić, M.; Perić, M.; Čipčić Paljetak, H.; Barešić, A.; Verbanac, D. The Role of Gut, Vaginal, and Urinary Microbiome in Urinary Tract Infections: From Bench to Bedside. Diagnostics 2020, 11, 7. [Google Scholar] [CrossRef]
- Xu, R.; Deebel, N.; Casals, R.; Dutta, R.; Mirzazadeh, M. A New Gold Rush: A Review of Current and Developing Diagnostic Tools for Urinary Tract Infections. Diagnostics 2021, 11, 479. [Google Scholar] [CrossRef] [PubMed]
- Xie, R.; Li, X.; Li, G.; Fu, R. Diagnostic value of different urine tests for urinary tract infection: A systematic review and meta-analysis. Transl. Androl. Urol. 2022, 11, 325–335. [Google Scholar] [CrossRef]
- Werneburg, G.T.; Rhoads, D.D. Diagnostic stewardship for urinary tract infection: A snapshot of the expert guidance. Clevel. Clin. J. Med. 2022, 89, 581–587. [Google Scholar] [CrossRef]
- Wensel, C.R.; Pluznick, J.L.; Salzberg, S.L.; Sears, C.L. Next-generation sequencing: Insights to advance clinical investigations of the microbiome. J. Clin. Investig. 2022, 132, e154944. [Google Scholar] [CrossRef] [PubMed]
- Khawcharoenporn, T.; Vasoo, S.; Singh, K. Urinary Tract Infections due to Multidrug-Resistant Enterobacteriaceae: Prevalence and Risk Factors in a Chicago Emergency Department. Emerg. Med. Int. 2013, 2013, 258517. [Google Scholar] [CrossRef] [PubMed]
- Muteeb, G. Network meta-analysis of antibiotic resistance patterns in gram-negative bacterial infections: A comparative study of carbapenems, fluoroquinolones, and aminoglycosides. Front. Microbiol. 2023, 14, 1304011. [Google Scholar] [CrossRef] [PubMed]
- Ligozzi, M.; Bernini, C.; Bonora, M.G.; De Fatima, M.; Zuliani, J.; Fontana, R. Evaluation of the VITEK 2 system for identification and antimicrobial susceptibility testing of medically relevant gram-positive cocci. J. Clin. Microbiol. 2002, 40, 1681–1686. [Google Scholar] [CrossRef]
- M100-S22; Performance Standards for Antimicrobial Susceptibility; Twenty-Second Informational Supplement. CLSI: Wayne, PA, USA, 2023.
- Mazor-Dray, E.; Levy, A.; Schlaeffer, F.; Sheiner, E. Maternal urinary tract infection: Is it independently associated with adverse pregnancy outcome? J. Matern. Fetal Neonatal Med. 2009, 22, 124–128. [Google Scholar] [CrossRef]
- Schieve, L.A.; Handler, A.; Hershow, R.; Persky, V.; Davis, F. Urinary tract infection during pregnancy: Its association with maternal morbidity and perinatal outcome. Am. J. Public Health 1994, 84, 405–410. [Google Scholar] [CrossRef]
- Farkash, E.; Weintraub, A.Y.; Sergienko, R.; Wiznitzer, A.; Zlotnik, A.; Sheiner, E. Acute antepartum pyelonephritis in pregnancy: A critical analysis of risk factors and outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Bánhidy, F.; Acs, N.; Puhó, E.H.; Czeizel, A.E. Pregnancy complications and birth outcomes of pregnant women with urinary tract infections and related drug treatments. Scand. J. Infect. Dis. 2007, 39, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.K.; Chen, S.F.; Li, H.C.; Lin, H.C. No increased risk of adverse pregnancy outcomes in women with urinary tract infections: A nationwide population-based study. Acta Obstet. Gynecol. Scand. 2010, 89, 882–888. [Google Scholar] [CrossRef] [PubMed]
- Morken, N.H.; Gunnes, N.; Magnus, P.; Jacobsson, B. Risk of spontaneous preterm delivery in a low-risk population: The impact of maternal febrile episodes, urinary tract infection, pneumonia and ear-nose-throat infections. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 310–314. [Google Scholar] [CrossRef]
- Dube, R.; Al-Zuheiri, S.T.S.; Syed, M.; Harilal, L.; Zuhaira, D.A.L.; Kar, S.S. Prevalence, Clinico-Bacteriological Profile, and Antibiotic Resistance of Symptomatic Urinary Tract Infections in Pregnant Women. Antibiotics 2022, 12, 33. [Google Scholar] [CrossRef]
- Naber, K.; Schito, G.; Botto, H.; Palou, J.; Mazzei, T. Surveillance study in Europe and Brazil on clinical aspects and microbial resistance epidemiology in females with cystitis (ARESC): Implications for empiric therapy. Eur. Urol. 2008, 54, 1164–1178. [Google Scholar] [CrossRef]
- Lee, A.C.; Mullany, L.C.; Koffi, A.K.; Rafiqullah, I.; Khanam, R.; Folger, L.V.; Rahman, M.; Mitra, D.K.; Labrique, A.; Christian, P.; et al. Urinary tract infections in pregnancy in a rural population of Bangladesh: Population-based prevalence, risk factors, etiology, and antibiotic resistance. BMC Pregnancy Childbirth 2020, 20, 1. [Google Scholar] [CrossRef]
- Oli, A.N.; Akabueze, V.B.; Ezeudu, C.E.; Eleje, G.U.; Ejiofor, O.S.; Ezebialu, I.U.; Oguejiofor, C.B.; Ekejindu, I.M.; Emechebe, G.O.; Okeke, K.N. Bacteriology and Antibiogram of Urinary Tract Infection Among Female Patients in a Tertiary Health Facility in South Eastern Nigeria. Open Microbiol. J. 2017, 11, 292–300. [Google Scholar] [CrossRef]
- Glaser, A.P.; Schaeffer, A.J. Urinary tract infection and bacteriuria in pregnancy. Urol. Clin. N. Am. 2015, 42, 547–560. [Google Scholar] [CrossRef]
- Balachandran, L.; Jacob, L.; Al Awadhi, R.; Yahya, L.O.; Catroon, K.M.; Soundararajan, L.P.; Wani, S.; Alabadla, S.; Hussein, Y.A. Urinary Tract Infection in Pregnancy and Its Effects on Maternal and Perinatal Outcome: A Retrospective Study. Cureus 2022, 14, e21500. [Google Scholar] [CrossRef]
- AlZuheiri, S.T.; Dube, R.; Menezes, G.; Qasem, S. Clinical profile and outcome of Group B streptococcal colonization in mothers and neonates in Ras Al Khaimah, United Arab Emirates: A prospective observational study. Saudi Med. J. 2021, 9, 235–240. [Google Scholar] [CrossRef]
- Rosana, Y.; Ocviyanti, D.; Halim, M.; Harlinda, F.Y.; Amran, R.; Akbar, W.; Billy, M.; Akhmad, S.R.P. Urinary tract infections among Indonesian pregnant women and its susceptibility pattern. Infect. Dis. Obstet. Gynecol. 2020, 2020, 9681632. [Google Scholar] [CrossRef] [PubMed]
- Corrales, M.; Corrales-Acosta, E.; Corrales-Riveros, J.G. Which Antibiotic for Urinary Tract Infections in Pregnancy? A Literature Review of International Guidelines. J. Clin. Med. 2022, 11, 7226. [Google Scholar] [CrossRef] [PubMed]
- Committee on Obstetric Practice. Committee Opinion No. 717: Sulfonamides, Nitrofurantoin, and Risk of Birth Defects. Obstet. Gynecol. 2017, 130, e150–e152. [Google Scholar] [CrossRef]
- Hamdan, H.Z.; Ziad, A.H.; Ali, S.K.; Adam, I. Epidemiology of urinary tract infections and antibiotics sensitivity among pregnant women at Khartoum North Hospital. Ann. Clin. Microbiol. Antimicrob. 2011, 10, 2. [Google Scholar] [CrossRef]
- Correia, M.C.; Fontes, M.C.; Lima, N.S.; Marques, K.M.G.; Santos, A.T.; Santos, L.C.B.; Gomes, M.C.T.; de Souza Júnior, V.R.; da Mota Sousa, C.F.; de Barros Correia Fontes, L. Subclinical hypothyroidism and recurrent infection of the urinary tract: A case report. J. Urol. Ren. Dis. 2019, 11, 1151–1152. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Preterm (n = 126) | Full Term (n = 182) | p-Value |
|---|---|---|---|
| Age (mean ± SD) | 27.5 ± 4.2 | 28.3 ± 4.9 | 0.136 |
| Age category | 0.929 | ||
| 18–24 years | 35 (27.8%) | 48 (26.4%) | |
| 25–29 years | 42 (33.3%) | 64 (35.2%) | |
| 30–34 years | 29 (23.0%) | 45 (24.7%) | |
| ≥35 years | 20 (15.9%) | 25 (13.7%) | |
| BMI * | 0.483 | ||
| <25 kg/m2 | 34 (27.0%) | 54 (29.7%) | |
| 25–29.9 kg/m2 | 76 (60.3%) | 98 (53.8%) | |
| ≥30 kg/m2 | 16 (12.7%) | 30 (16.5%) | |
| Lifestyle | |||
| Smoking during pregnancy | 12 (9.5%) | 22 (12.1%) | 0.480 |
| Alcohol use during pregnancy | 8 (6.3%) | 15 (8.2%) | 0.544 |
| Professional status | 0.655 | ||
| Employed | 68 (54.0%) | 104 (57.1%) | |
| Unemployed | 20 (15.9%) | 33 (18.1%) | |
| Student | 15 (11.9%) | 21 (11.5%) | |
| Housewife | 23 (18.3%) | 24 (13.2%) | |
| Parity | 0.865 | ||
| Primigravida | 58 (46.0%) | 82 (45.1%) | |
| Multigravida | 68 (54.0%) | 100 (54.9%) | |
| Trimester of infection | 0.932 | ||
| 1st Trimester | 40 (31.7%) | 55 (30.2%) | |
| 2nd Trimester | 48 (38.1%) | 73 (40.1%) | |
| 3rd Trimester | 38 (30.2%) | 54 (29.7%) | |
| Medical history | |||
| Previous UTI | 56 (44.4%) | 70 (38.5%) | 0.293 |
| Hypertension | 20 (15.9%) | 31 (17.0%) | 0.787 |
| Diabetes | 18 (14.3%) | 22 (12.1%) | 0.572 |
| Anemia | 23 (18.3%) | 29 (15.9%) | 0.593 |
| Asthma | 10 (7.9%) | 16 (8.8%) | 0.790 |
| Others | 12 (9.5%) | 20 (11.0%) | 0.678 |
| UTI symptoms | |||
| Increased urinary frequency | 67 (53.2%) | 92 (50.5%) | 0.650 |
| Dysuria | 58 (46.0%) | 80 (44.0%) | 0.718 |
| Urgency | 51 (40.5%) | 71 (39.0%) | 0.796 |
| Hematuria | 20 (15.9%) | 26 (14.3%) | 0.701 |
| Cloudy/dark/strong-smelling urine | 45 (35.7%) | 61 (33.5%) | 0.689 |
| Suprapubic pain | 18 (14.3%) | 40 (22.0%) | 0.089 |
| Fever and chills | 21 (16.7%) | 19 (10.4%) | 0.109 |
| Back pain | 23 (18.3%) | 30 (16.5%) | 0.685 |
| Variables | Preterm (n = 126) | Full Term (n = 182) | p-Value |
|---|---|---|---|
| Blood tests (median, IQR) | |||
| WBC (4.5–11.0 × 103/mm3) | 12.3 (10.5–14.7) | 9.1 (7.4–11.2) | 0.032 |
| Lymphocytes (1.0–4.0 × 103/mm3) | 1.9 (1.4–2.5) | 2.3 (1.8–2.9) | 0.227 |
| Neutrophils (1.5–8.0 × 103/mm3) | 7.8 (6.8–8.3) | 6.1 (4.9–6.7) | <0.001 |
| PLT (150–450 thousands/mm3) | 283 (189–352) | 326 (241–390) | 0.055 |
| RBC (3.9–5.5 × 106/mm3) | 4.2 (3.5–4.7) | 4.6 (4.1–5.0) | 0.308 |
| Hemoglobin (12–16 g/L) | 12.2 (10.5–13.0) | 13.8 (12.9–14.2) | 0.092 |
| CRP (0–10 mg/L) | 18 (14–26) | 7 (4–10) | <0.001 |
| Creatinine (0.6–1.1 mg/dL) | 0.9 (0.7–1.3) | 0.8 (0.6–1.0) | 0.526 |
| Urea (7–20 mg/dL) | 17 (14–21) | 12 (9–15) | 0.060 |
| Urine cultures (n = 308) | 0.009 | ||
| 1 bacterium | 73 (57.9%) | 132 (72.5%) | |
| 2 bacteria | 33 (26.2%) | 38 (20.9%) | |
| ≥3 bacteria | 20 (15.9%) | 12 (6.6%) |
| Microbial Identification | Preterm (n = 126) | Full Term (n = 182) | p-Value |
|---|---|---|---|
| Gram-negative | |||
| Escherichia coli = 190/308 (61.7%) | 83 (65.9%) | 107 (58.8%) | 0.208 |
| Klebsiella spp. = 53/308 (17.2%) | 14 (11.1%) | 39 (21.4%) | 0.018 |
| Pseudomonas spp. = 38/308 (12.3%) | 16 (12.7%) | 22 (12.1%) | 0.872 |
| Enterobacter spp. = 45/308 (14.6%) | 27 (21.4%) | 18 (9.9%) | 0.004 |
| Proteus spp. = 23/308 (7.5%) | 9 (7.1%) | 14 (7.7%) | 0.856 |
| Bacteroides spp. = 18/308 (5.8%) | 6 (4.8%) | 12 (6.6%) | 0.501 |
| Gram-positive | |||
| Enterococcus spp. = 23/308 (7.5%) | 7 (5.6%) | 16 (8.8%) | 0.289 |
| Streptococcus spp. = 22/308 (7.1%) | 11 (8.7%) | 11 (6.0%) | 0.368 |
| Group B Streptococcus = 25/308 (8.1%) | 22 (17.5%) | 3 (1.6%) | <0.001 |
| Staphylococcus spp. = 11/308 (3.6%) | 4 (3.2%) | 7 (3.8%) | 0.754 |
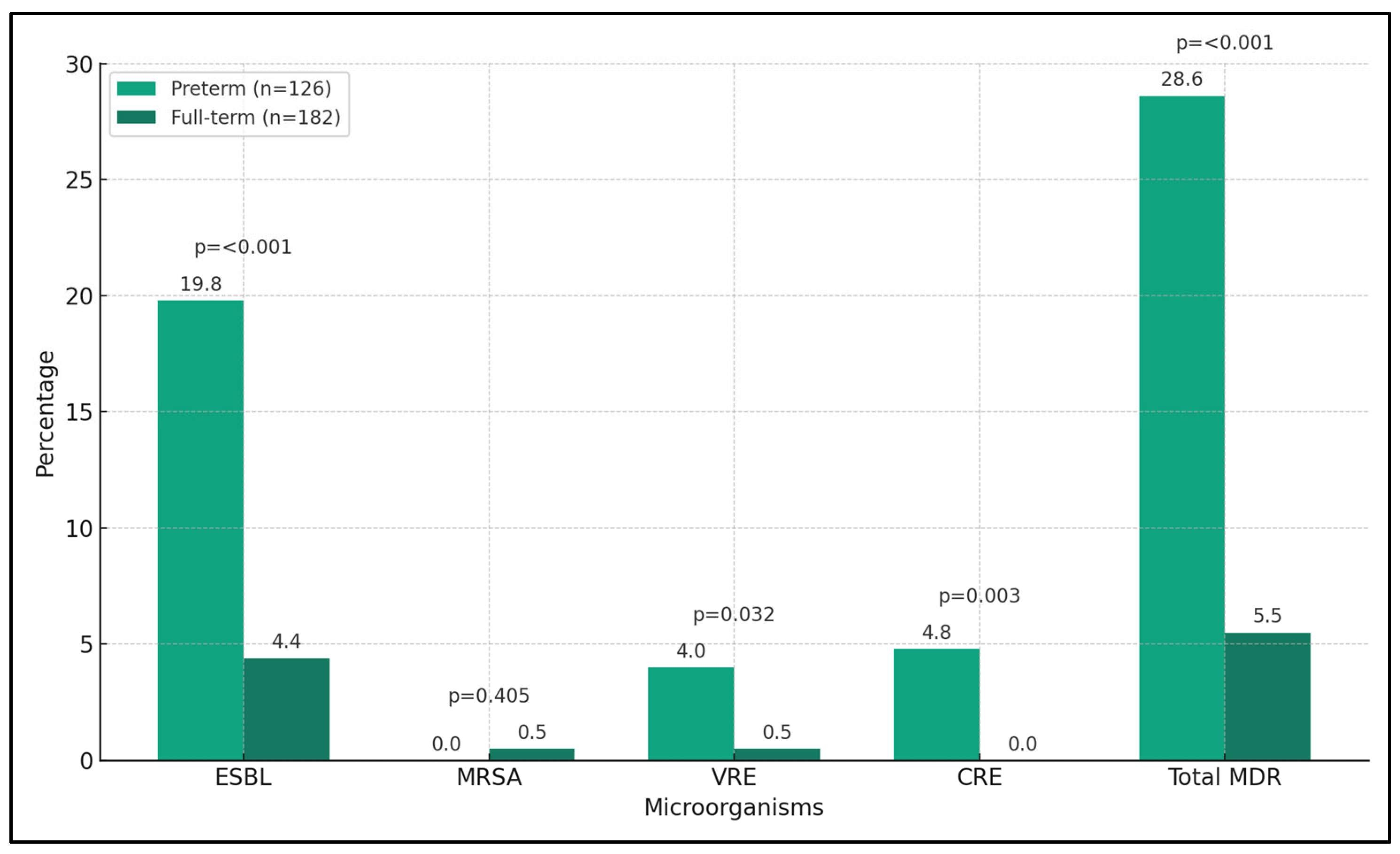
| Urine Samples (n = 308) | Preterm (n = 126) | Full Term (n = 182) | p-Value |
|---|---|---|---|
| ESBL = 33 (10.7%) | 25 (19.8%) | 8 (4.4%) | <0.001 |
| MRSA = 1 (0.3%) | 0 (0%) | 1 (0.5%) | 0.405 |
| VRE = 6 (1.9%) | 5 (4.0%) | 1 (0.5%) | 0.032 |
| CRE = 6 (1.9%) | 6 (4.8%) | 0 (0.0%) | 0.003 |
| Total MDR = 46 (14.9%) | 36 (28.6%) | 10 (5.5%) | <0.001 |
| Antibiotic Resistance * | Preterm (n = 126) | Full Term (n = 182) | p-Value |
|---|---|---|---|
| Amoxicillin = 36/294 (12.2%) | 26 (20.6%) | 12 (6.6%) | <0.001 |
| Nitrofurantoin = 43/289 (14.9%) | 15 (11.9%) | 28 (15.4%) | 0.386 |
| Ampicillin/sulbactam = 25/206 (12.1%) | 13 (10.3%) | 12 (6.6%) | 0.239 |
| Macrolides = 20/148 (13.5%) | 10 (7.9%) | 10 (5.5%) | 0.393 |
| Fosfomycin = 27/145 (18.6%) | 18 (14.3%) | 9 (4.9%) | 0.004 |
| Piperacillin/tazobactam = 15/139 (10.8%) | 8 (6.3%) | 7 (3.8%) | 0.315 |
| Penems (meropenem/imipenem) = 19/166 (11.4%) | 8 (6.3%) | 11 (6.0%) | 0.912 |
| Glycopeptides = 18/201 (8.9%) | 11 (8.7%) | 7 (3.8%) | 0.072 |
| 2nd Gen. cephalosporin = 32/265 (12.1%) | 22 (17.4%) | 10 (5.5%) | <0.001 |
| 3rd Gen. cephalosporin = 37/277 (13.4%) | 25 (19.8%) | 12 (6.6%) | <0.001 |
| 4th Gen. cephalosporin = 25/201 (12.4%) | 5 (4.0%) | 10 (5.5%) | 0.540 |
| Ticarcillin/clavulanic = 29/139 (20.9%) | 7 (5.5%) | 12 (6.6%) | 0.709 |
| Piperacillin = 11/108 (10.2%) | 4 (3.2%) | 7 (3.8%) | 0.754 |
| Significant Risk Factors | Coefficient (β) | SE | OR | 95% CI | p-Value |
|---|---|---|---|---|---|
| GBS infection | 0.92 | 0.30 | 2.5 | 1.5–4.1 | 0.001 |
| Enterobacter spp. infection | 0.59 | 0.26 | 1.8 | 1.1–2.9 | 0.022 |
| MDR presence | 1.16 | 0.32 | 3.2 | 2.0–5.2 | <0.001 |
| ESBL production | 0.99 | 0.35 | 2.7 | 1.6–4.5 | 0.003 |
| Anemia during pregnancy | 0.47 | 0.21 | 1.6 | 1.1–2.3 | 0.015 |
| Elevated CRP levels | 0.69 | 0.24 | 2.0 | 1.3–3.1 | 0.002 |
| Elevated neutrophils | 0.64 | 0.28 | 1.9 | 1.2–3.0 | 0.007 |
| Amoxicillin resistance | 0.79 | 0.33 | 2.2 | 1.4–3.4 | 0.001 |
| 2nd Gen. cephalosporin resistance | 0.41 | 0.20 | 1.5 | 1.0–2.2 | 0.048 |
| 3rd Gen. cephalosporin resistance | 1.03 | 0.37 | 2.8 | 1.7–4.6 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bratosin, F.; Folescu, R.; Krupyshev, P.; Popa, Z.L.; Citu, C.; Ratiu, A.; Rosca, O.; Ilie, A.C. Comparative Analysis of Microbial Species and Multidrug Resistance Patterns Associated with Lower Urinary Tract Infections in Preterm and Full-Term Births. Microorganisms 2024, 12, 139. https://doi.org/10.3390/microorganisms12010139
Bratosin F, Folescu R, Krupyshev P, Popa ZL, Citu C, Ratiu A, Rosca O, Ilie AC. Comparative Analysis of Microbial Species and Multidrug Resistance Patterns Associated with Lower Urinary Tract Infections in Preterm and Full-Term Births. Microorganisms. 2024; 12(1):139. https://doi.org/10.3390/microorganisms12010139
Chicago/Turabian StyleBratosin, Felix, Roxana Folescu, Pavel Krupyshev, Zoran Laurentiu Popa, Cosmin Citu, Adrian Ratiu, Ovidiu Rosca, and Adrian Cosmin Ilie. 2024. "Comparative Analysis of Microbial Species and Multidrug Resistance Patterns Associated with Lower Urinary Tract Infections in Preterm and Full-Term Births" Microorganisms 12, no. 1: 139. https://doi.org/10.3390/microorganisms12010139
APA StyleBratosin, F., Folescu, R., Krupyshev, P., Popa, Z. L., Citu, C., Ratiu, A., Rosca, O., & Ilie, A. C. (2024). Comparative Analysis of Microbial Species and Multidrug Resistance Patterns Associated with Lower Urinary Tract Infections in Preterm and Full-Term Births. Microorganisms, 12(1), 139. https://doi.org/10.3390/microorganisms12010139