4.1. Literature Findings
The current study found significant differences in microbial species and multidrug resistance patterns between urinary tract infections (UTIs) in preterm and full-term births. Notably, the prevalence of Group B Streptococcus (GBS) and Enterobacter spp. was significantly higher in the preterm group, indicating a distinct bacterial profile associated with preterm births, in turn suggesting that these pathogens might contribute to the induction of inflammatory responses, potentially leading to preterm labor.
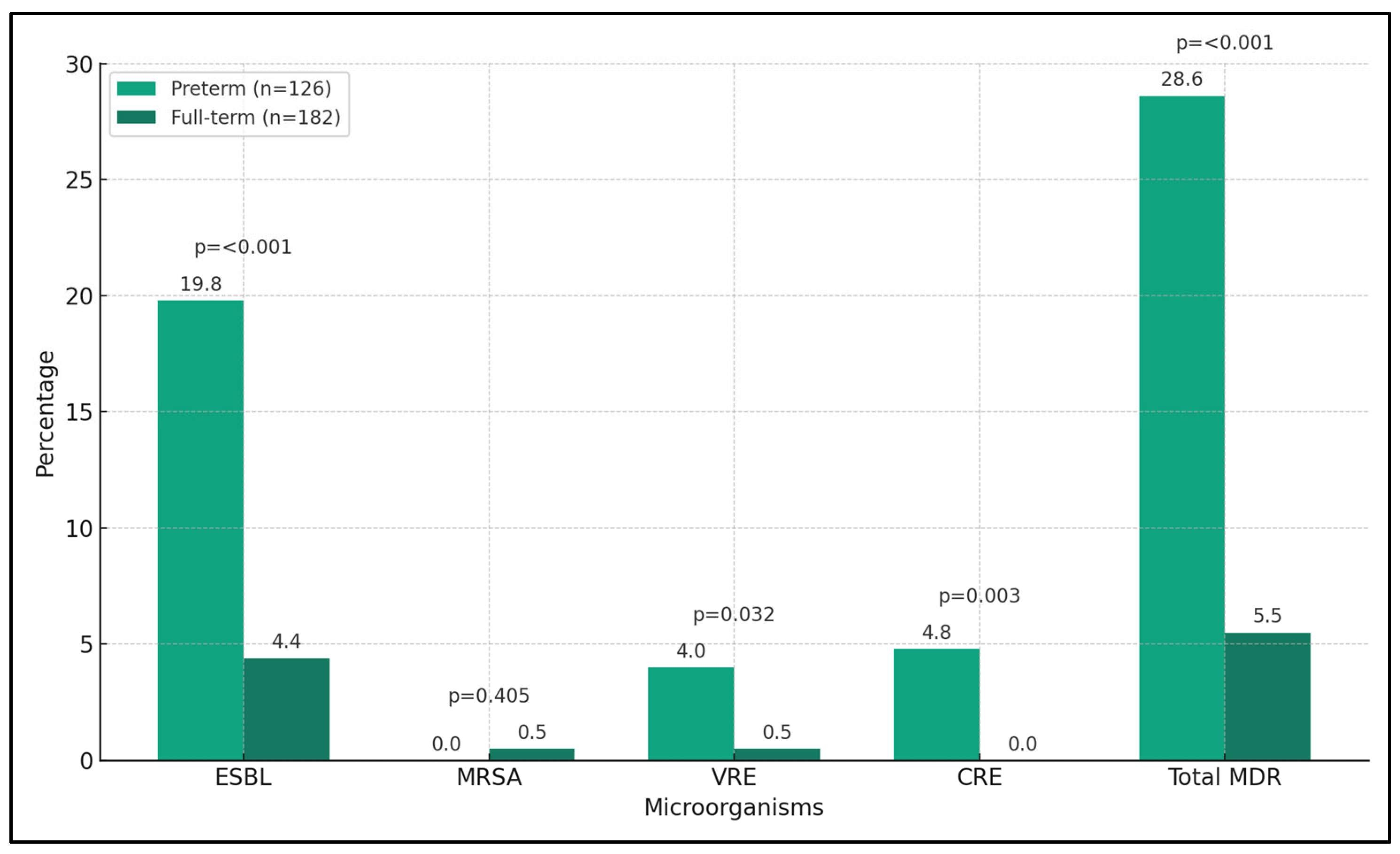
Furthermore, the study revealed a notable rise in multidrug-resistant organisms, particularly extended-spectrum beta-lactamases (ESBL) producing organisms and carbapenem-resistant Enterobacteriaceae (CRE) in the preterm birth group, highlighting the complex challenge of managing UTIs in pregnant women due to evolving resistance patterns. The increased resistance to antibiotics such as amoxicillin and cephalosporins in the preterm group underscored the urgency for personalized antimicrobial therapies informed by robust microbial identification and sensitivity testing.
These findings demonstrate a clear divergence in the microbial landscape and resistance patterns between the two groups. The significant differences observed emphasize the need for a nuanced understanding of the interplay between microbial pathogenesis, antibiotic resistance, and pregnancy outcomes, pointing to the importance of integrating detailed microbial analysis into clinical practice to better inform treatment choices for UTIs in pregnant women, particularly those at risk of preterm birth.
In an important study from California, it was demonstrated that urinary tract infections significantly increase the risk of preterm birth, particularly spontaneous preterm birth, with an adjusted risk score that is 1.4 times higher than the normal population [
4]. This risk has been reported to persist across all trimesters; however, notably, women hospitalized with UTIs during their second trimester faced a threefold increased risk of delivering before 32 weeks. This finding is in line with previous studies [
20,
21] that have reported a two-fold increase in the odds of preterm birth for women with UTIs during pregnancy.
Contrasting findings have emerged regarding the association between pyelonephritis and preterm birth. While studies by Farkash et al. [
22] and Bánhidy et al. [
23] show an increased odds of preterm birth with pyelonephritis, Chen et al. did not find a significant association [
24]. Another study confirmed an association between pyelonephritis and preterm birth, but the risk was not markedly higher than that associated with acute cystitis. This highlights in particular that hospitalization for UTIs during the second trimester significantly elevates the risk of preterm birth, in turn suggesting that severe infections during this period are particularly detrimental [
25].
Considering that the current study used a monocentric database, it is important to acknowledge geographical and population-based differences in terms of UTIs. For example, one study from UAE found around 37% of pregnant symptomatic patients with UTI not exhibiting any growth of uropathogens in their urine [
26], a proportion exceeding that reported in some other research [
27]. However, in our study we excluded the negative samples to better determine antibiotic resistance patterns and MDR.
Similar to our study,
E. coli is the most commonly isolated pathogen in different studies, but with relatively different prevalences, as low as 27% in Dube’s et al. study [
26], compared with other studies [
28,
29], while the prevalence of GBS and
K. pneumoniae is reported in higher prevalence in other research [
28,
30]. Even though we identified only 3.6% of
Staphylococcus isolates, in the UAE study, no cultures identified
Staphylococcus spp. [
26,
31]. Therefore, it can be assumed that the local microbial profile, including the predominance of
E. coli in recurrent UTIs, likely reflects geographical and sociocultural influences.
In our study, the observed higher prevalence of ESBL resistance compared with other resistance types, such as MRSA, may be attributable to several factors. Primarily, the distribution and nature of the infecting organisms are crucial determinants. ESBL production is predominantly associated with Enterobacteriaceae, especially Escherichia coli and Klebsiella spp., which were significantly more prevalent in our cohort. Considering the global rise in ESBL-producing E. coli infections, our findings align with the broader trend of increasing ESBL resistance rates, potentially reflecting local or regional antibiotic prescribing patterns and subsequent selection pressures. In contrast, MRSA, which is associated with Staphylococcus aureus, had a very low incidence in our study population. This discrepancy could be due to several factors, including the natural prevalence of these bacteria in pregnant women, the specific susceptibility of these organisms to the antibiotics used in this population, and the overall lower rate of S. aureus as a causative agent of urinary tract infections compared with E. coli. Additionally, the zero incidence of MRSA in the preterm group versus the full-term group might not necessarily indicate a trend but could be a result of the smaller sample size or lower exposure to risk factors for MRSA in the preterm group.
Interestingly, antimicrobial resistance for
E. coli was lower in other studies, compared with our findings of 10.7% ESBL organisms, while GBS showed higher sensitivity to common antibiotics [
32,
33]. Regarding antibiotic use, most studies favor nitrofurantoin as the first-line treatment for UTIs in pregnant women, except for specific conditions and late pregnancy [
34]. High organism sensitivity to penicillins, erythromycin, and cephalosporins is noted in the literature, with moderate sensitivity to cefuroxime, commonly used in empirical therapy for culture-negative cases, comparable to an overall resistance percentage of 12.1% for second-generation cephalosporines in our study, although it was significantly higher among mothers who gave birth preterm [
35].
Regarding the background data of participants, the association of demographic factors like age, BMI, and parity with UTI remains unclear due to conflicting evidence from various studies [
36], the majority of pregnant women with UTI were in their second trimester, differing from another study where symptoms were more common in the first trimester [
31]. Notably, diabetes and a previous history of UTI were identified as risk factors for UTI, in line with broader research [
5]; however, the expected association with hypothyroidism was only observed in two symptomatic women [
37], suggesting a need for further research to establish more definitive associations. When comparing culture-negative and culture-positive groups, the latter had significantly more known risk factors although individual comparisons were limited by small group sizes [
26].
This study illuminates the critical need for personalized management of UTIs in pregnant women, particularly against a backdrop of increasing multidrug resistance. Our findings reveal distinct microbial profiles and resistance patterns in preterm versus full-term births, underscoring the importance of precise microbial identification and tailored antimicrobial therapies. The significant prevalence of multidrug-resistant organisms in preterm births further emphasizes the necessity for vigilant, adaptive treatment strategies and ongoing surveillance. These insights are pivotal for informing future clinical guidelines and research, aiming to enhance maternal and neonatal outcomes by effectively combating UTIs in pregnancy.
Furthermore, while this study posits a global applicability given the widespread prevalence of urinary tract infections, it is imperative to acknowledge the specific demographic nuances of the Romanian population from which the sample was drawn. Predominantly composed of white, middle-class Caucasian women, this homogeneity presents unique characteristics that may influence the generalization of the findings.
_Di_Marco.png)


 ,
, 


{kind=link}
{kind=link}