

Comparison of Amoxicillin Administered Twice versus Four Times a Day in First-Line Helicobacter pylori Eradication Using Tegoprazan, Clarithromycin, and Bismuth: A Propensity Score Matching Analysis


Abstract
1. Introduction
2. Materials and Methods
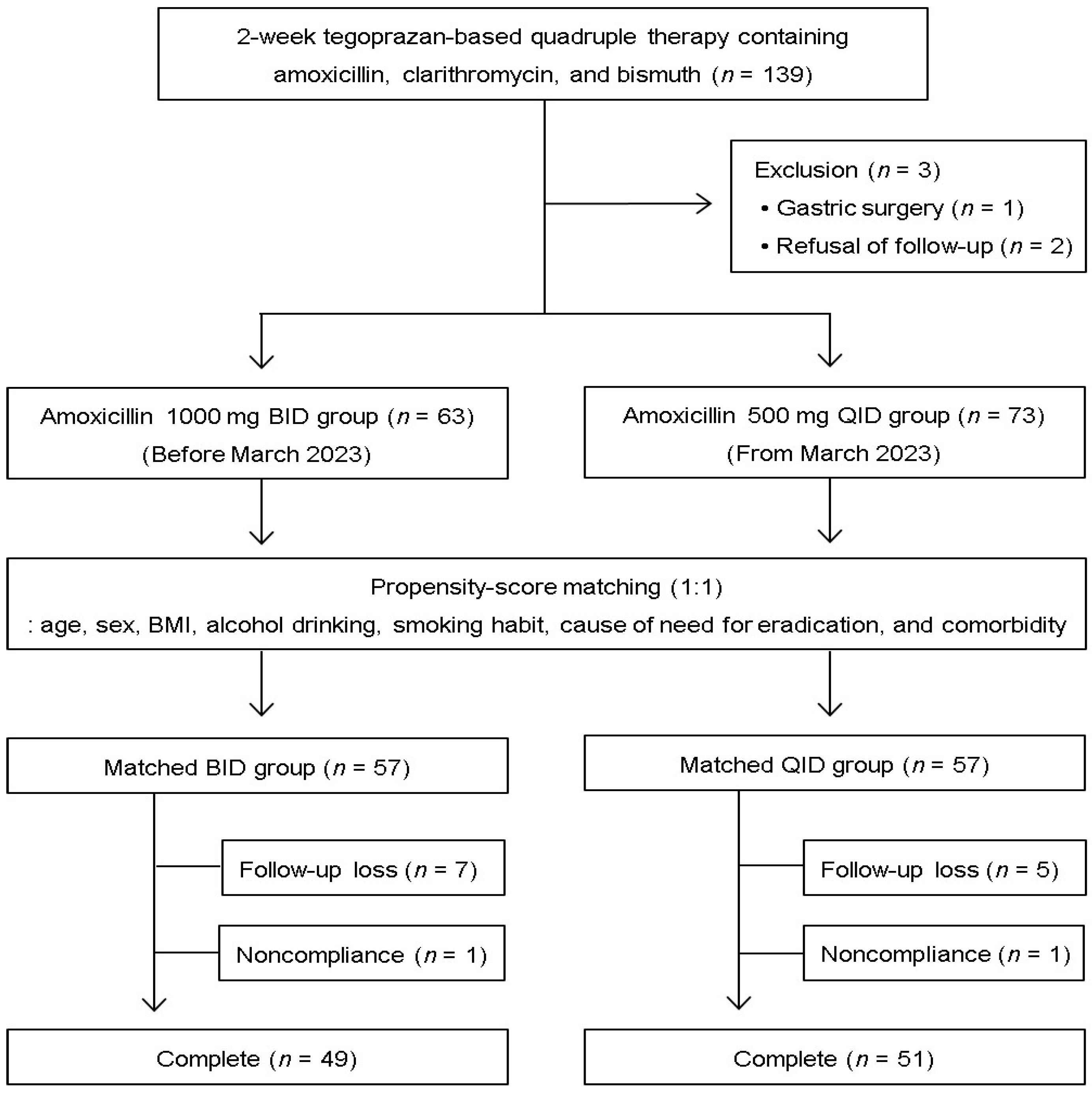
2.1. Patients and Study Design
2.2. Helicobacter pylori Eradication Therapy
2.3. Study Outcomes
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Eradication Rate
3.3. Compliance and Adverse Events
3.4. Analysis of Clinical Factors Affecting H. pylori Eradication
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Malfertheiner, P.; Camargo, M.C.; El-Omar, E.; Liou, J.-M.; Peek, R.; Schulz, C.; Smith, S.I.; Suerbaum, S. Helicobacter pylori infection. Nat. Rev. Dis. Primers 2023, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y. Best Practices for Helicobacter pylori Management. Gastroenterol. Hepatol. 2024, 20, 159–168. [Google Scholar]
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto Consensus for the Treatment of Helicobacter pylori Infection in Adults. Gastroenterology 2016, 151, 51–69.e14. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Xue, J.; Lin, F.; Liu, D.; Zhang, W.; Ru, S.; Jiang, F. Global Primary Antibiotic Resistance Rate of Helicobacter pylori in Recent 10 years: A Systematic Review and Meta-Analysis. Helicobacter 2024, 29, e13103. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Graham, D.Y. Pharmacologic aspects of eradication therapy for Helicobacter pylori Infection. Gastroenterol. Clin. N. Am. 2010, 39, 465–480. [Google Scholar] [CrossRef]
- Mégraud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [Google Scholar] [CrossRef]
- Klotz, U. Pharmacokinetic considerations in the eradication of Helicobacter pylori. Clin. Pharmacokinet. 2000, 38, 243–270. [Google Scholar] [CrossRef]
- Jung, Y.S.; Kim, S.; Kim, H.Y.; Noh, S.J.; Park, J.H.; Sohn, C.I.; Park, C.H. Efficacy and Tolerability of 14-Day Tegoprazan- versus Rabeprazole-Based Triple Therapy for Eradication of Helicobacter pylori: A Real-World Evidence Study. Gut Liver 2023, 17, 711–721. [Google Scholar] [CrossRef]
- Shin, D.W.; Cheung, D.Y.; Song, J.H.; Choi, K.; Lim, J.; Lee, H.H.; Kim, J.I.; Park, S.-H. The benefit of the bismuth add-on to the 2-week clarithromycin-based triple regimen for Helicobacter pylori eradication: A propensity score-matched retrospective study. Gut Pathog. 2023, 15, 13. [Google Scholar] [CrossRef]
- Cho, J.H. Bismuth add-on improves the efficacy of 2-week tegoprazan-based triple therapy for first-line Helicobacter pylori eradication: A real-world evidence study. Expert Rev. Anti Infect. Ther. 2024. Epub ahead of print. [Google Scholar] [CrossRef]
- Hong, T.C.; El-Omar, E.M.; Kuo, Y.T.; Wu, J.-Y.; Chen, M.-J.; Chen, C.-C.; Fang, Y.-J.; Leow, A.H.R.; Lu, H.; Lin, J.-T.; et al. Primary antibiotic resistance of Helicobacter pylori in the Asia-Pacific region between 1990 and 2022: An updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2024, 9, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.-M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Jeon, S.R.; Kim, H.G.; Jin, S.; Park, S. Cost-effectiveness of a tailored Helicobacter pylori eradication strategy based on the presence of a 23S ribosomal RNA point mutations that causes clarithromycin resistance in Korean patients. J. Gastroenterol. Hepatol. 2019, 34, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Nyssen, O.P.; Perez-Aisa, A.; Tepes, B.; Castro-Fernandez, M.; Kupcinskas, J.; Jonaitis, L.; Bujanda, L.; Lucendo, A.; Jurecic, N.B.; Perez-Lasala, J.; et al. Adverse event profile during the treatment of Helicobacter pylori: A real-world experience of 22,000 patients from the European Registry on H. pylori management (Hp-EuReg). Am. J. Gastroenterol. 2021, 116, 1220–1229. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Chung, J.W.; Woo, H.S.; Kim, S.Y.; Kim, J.H.; Kim, Y.J.; Kim, K.O.; Kwon, K.A.; Park, D.K. Two-week bismuth-containing quadruple therapy and concomitant therapy are effective first-line treatments for Helicobacter pylori eradication: A prospective open-label randomized trial. World J. Gastroenterol. 2019, 25, 6790–6798. [Google Scholar] [CrossRef]
- Jung, H.K.; Kang, S.J.; Lee, Y.C.; Yang, H.-J.; Park, S.-Y.; Shin, C.M.; Kim, S.E.; Lim, H.C.; Kim, J.-H.; Nam, S.Y.; et al. Evidence-based guidelines for the treatment of Helicobacter pylori infection in Korea 2020. Gut Liver 2021, 15, 168–195. [Google Scholar] [CrossRef]
- Kim, B.J.; Yang, C.H.; Song, H.J.; Jeon, S.W.; Kim, G.H.; Kim, H.; Kim, T.H.; Shim, K.; Chung, I.; Park, M.I.; et al. Online registry for nationwide database of Helicobacter pylori eradication in Korea: Correlation of antibiotic use density with eradication success. Helicobacter 2019, 24, e12646. [Google Scholar] [CrossRef]
- Mouton, J.W.; Vinks, A.A. Is continuous infusion of beta-lactam antibiotics worthwhile?--efficacy and pharmacokinetic considerations. J. Antimicrob. Chemother. 1996, 38, 5–15. [Google Scholar] [CrossRef]
- Arancibia, A.; Guttmann, J.; González, G.; González, C. Absorption and disposition kinetics of amoxicillin in normal human subjects. Antimicrob. Agents Chemother. 1980, 17, 199–202. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, S.W.; Jung, S.W.; Koo, J.S.; Yim, H.J.; Park, J.J.; Chun, H.J.; Lee, H.S.; Choi, J.H.; Kim, C.D.; et al. Comparative study of Helicobacter pylori eradication rates of twice-versus four-times-daily amoxicillin administered with proton pump inhibitor and clarithromycin: A randomized study. Helicobacter 2008, 13, 282–287. [Google Scholar] [CrossRef]
- Furuta, T.; Sugimoto, M.; Yamade, M.; Uotani, T.; Sahara, S.; Ichikawa, H.; Yamada, T.; Osawa, S.; Sugimoto, K.; Watanabe, H.; et al. Effect of dosing schemes of amoxicillin on eradication rates of Helicobacter pylori with amoxicillin-based triple therapy. J. Clin. Pharmacol. 2014, 54, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Miwa, H. Potent Potassium-competitive Acid Blockers: A New Era for the Treatment of Acid-related Diseases. J. Neurogastroenterol. Motil. 2018, 24, 334–344. [Google Scholar] [CrossRef] [PubMed]
- Miftahussurur, M.; Pratama Putra, B.; Yamaoka, Y. The Potential Benefits of Vonoprazan as Helicobacter pylori Infection Therapy. Pharmaceuticals 2020, 13, 276. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.R.; Midolo, P. The actions of bismuth in the treatment of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 1997, 11 (Suppl. 1), 27–33. [Google Scholar] [CrossRef] [PubMed]
- Dore, M.P.; Lu, H.; Graham, D.Y. Role of bismuth in improving Helicobacter pylori eradication with triple therapy. Gut 2016, 65, 870–878. [Google Scholar] [CrossRef]
- Yun, J.; Wu, Z.; Qi, G.; Han, T.; Zhang, D. The high-dose amoxicillin-proton pump inhibitor dual therapy in eradication of Helicobacter pylori infection. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 149–157. [Google Scholar] [CrossRef]
- Du, R.C.; Hu, Y.X.; Ouyang, Y.; Ling, L.; Xu, J.; Sa, R.; Liu, X.; Hong, J.; Zhu, Y.; Lu, N.; et al. Vonoprazan and amoxicillin dual therapy as the first-line treatment of Helicobacter pylori infection: A systematic review and meta-analysis. Helicobacter 2024, 29, e13039. [Google Scholar] [CrossRef]
- Ju, K.P.; Kong, Q.Z.; Li, Y.Y.; Li, Y.Q. Low-dose or high-dose amoxicillin in vonoprazan-based dual therapy for Helicobacter pylori eradication? A systematic review and meta-analysis. Helicobacter 2024, 29, e13054. [Google Scholar] [CrossRef]
- Hu, Y.; Xu, X.; Ouyang, Y.B.; He, C.; Li, N.; Xie, C.; Peng, C.; Zhu, Z.; Xie, Y.; Shu, X.; et al. Optimization of vonoprazan-amoxicillin dual therapy for eradicating Helicobacter pylori infection in China: A prospective, randomized clinical pilot study. Helicobacter 2022, 27, e12896. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Before Matching | After Matching | ||||
|---|---|---|---|---|---|---|
| BID Group (n = 63) | QID Group (n = 73) | p-Value | BID Group (n = 57) | QID Group (n = 57) | p-Value | |
| Age (years) | 53.3 ± 12.2 | 55.5 ± 11.5 | 0.286 | 53.4 ± 12.6 | 54.8 ± 11.9 | 0.538 |
| Male (%) | 35 (55.6) | 35 (47.9) | 0.376 | 31 (54.4) | 31 (54.4) | 1.000 |
| Alcohol drinking (%) | 28 (44.4) | 32 (43.8) | 0.943 | 26 (45.6) | 23 (40.4) | 0.570 |
| Current smoker (%) | 18 (28.6) | 11 (15.1) | 0.055 | 13 (22.8) | 11 (19.3) | 0.646 |
| Body mass index (kg/m2) | 24.2 ± 3.7 | 24.0 ± 3.3 | 0.712 | 24.4 ± 3.7 | 24.1 ± 3.4 | 0.611 |
| Cause of need for eradication (%) | 0.344 | 0.404 | ||||
| Chronic active gastritis | 41 (65.1) | 53 (72.6) | 39 (68.4) | 43 (75.4) | ||
| Peptic ulcer/neoplasia | 22 (34.9) | 20 (27.4) | 18 (31.6) | 14 (24.6) | ||
| Laboratory finding, mean (SD) | ||||||
| Hemoglobin (g/dL) | 13.9 ± 1.8 | 13.7 ± 1.3 | 0.529 | 14.0 ± 1.8 | 13.9 ± 1.4 | 0.814 |
| AST (U/L) | 23.1 ± 8.7 | 23.8 ± 7.3 | 0.600 | 23.5 ± 9.0 | 23.7 ± 7.2 | 0.887 |
| ALT (U/L) | 24.4 ± 16.3 | 22.9 ± 9.8 | 0.539 | 24.6 ± 16.9 | 22.8 ± 9.3 | 0.495 |
| Creatinine (mg/dL) | 0.83 ± 0.17 | 0.83 ± 0.16 | 0.944 | 0.84 ± 0.17 | 0.85 ± 0.17 | 0.682 |
| Underlying disease (%) | ||||||
| Cardiovascular disease | 20 (31.7) | 24 (32.9) | 0.888 | 18 (31.6) | 20 (35.1) | 0.691 |
| Respiratory disease | 0 (0) | 0 (0) | 1.000 | 0 (0) | 0 (0) | 1.000 |
| Liver dysfunction | 0 (0) | 2 (2.7) | 0.499 | 0 (0) | 2 (3.5) | 0.496 |
| Renal dysfunction | 1 (1.6) | 0 (0) | 0.463 | 1 (1.8) | 0 (0) | 1.000 |
| Diabetes | 7 (11.1) | 5 (6.8) | 0.382 | 5 (8.8) | 3 (5.3) | 0.716 |
| BID Group | QID Group | Adjusted 95% CI for Difference | p-Value | |
|---|---|---|---|---|
| Intention-to-treat analysis | ||||
| Eradication rate | 82.5% (47/57) | 87.7% (50/57) | 5.2% (−7.8 to 18.3%) | 0.429 |
| Per-protocol analysis | ||||
| Eradication rate | 95.9% (47/49) | 98.0% (50/51) | 2.1% (−4.6 to 8.8%) | 0.536 |
| BID Group (n = 50) | QID Group (n = 52) | p-Value | |
|---|---|---|---|
| Compliance | 49 (98.0%) | 51 (98.1%) | 1.000 |
| Patients with adverse events | 20 (40.0%) | 12 (23.1%) | 0.066 |
| Bitter taste | 13 (26.0%) | 9 (17.3%) | 0.286 |
| Abdominal pain | 1 (2%) | 0 (0%) | 0.490 |
| Nausea or vomiting | 7 (14.0%) | 2 (3.8%) | 0.089 |
| Diarrhea | 3 (6.0%) | 0 (0%) | 0.114 |
| Bloating | 1 (2.0%) | 1 (1.9%) | 1.000 |
| Others | 3 (6.0%) | 0 (0%) | 0.114 |
| Variable | Eradication Rate | p-Value |
|---|---|---|
| Sex | 0.245 | |
| Male (n = 53) | 50 (94.3%) | |
| Female (n = 47) | 47 (100%) | |
| Age, years | 0.294 | |
| <50 (n = 36) | 34 (94.4%) | |
| ≥50 (n = 64) | 63 (98.4%) | |
| Body mass index, kg/m2 | 0.559 | |
| <25 (n = 61) | 60 (98.4%) | |
| ≥25 (n = 39) | 37 (94.9%) | |
| Alcohol drinking | 0.076 | |
| No (n = 57) | 57 (100%) | |
| Yes (n = 43) | 40 (93.0%) | |
| Current smoker | 1.000 | |
| No (n = 81) | 78 (96.3%) | |
| Yes (n = 19) | 19 (100%) | |
| Cause of need for eradication | 1.000 | |
| Chronic active gastritis (n = 73) | 71 (97.3%) | |
| Peptic ulcer/neoplasia (n = 27) | 26 (96.3%) | |
| Comorbidity | 0.562 | |
| Absent (n = 60) | 59 (98.3%) | |
| Present (n = 40) | 38 (95.0%) | |
| Adverse drug event | 0.550 | |
| Absent (n = 69) | 66 (95.7%) | |
| Present (n = 31) | 31 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.-H.; Jin, S.-Y. Comparison of Amoxicillin Administered Twice versus Four Times a Day in First-Line Helicobacter pylori Eradication Using Tegoprazan, Clarithromycin, and Bismuth: A Propensity Score Matching Analysis. Microorganisms 2024, 12, 1952. https://doi.org/10.3390/microorganisms12101952
Cho J-H, Jin S-Y. Comparison of Amoxicillin Administered Twice versus Four Times a Day in First-Line Helicobacter pylori Eradication Using Tegoprazan, Clarithromycin, and Bismuth: A Propensity Score Matching Analysis. Microorganisms. 2024; 12(10):1952. https://doi.org/10.3390/microorganisms12101952
Chicago/Turabian StyleCho, Jun-Hyung, and So-Young Jin. 2024. "Comparison of Amoxicillin Administered Twice versus Four Times a Day in First-Line Helicobacter pylori Eradication Using Tegoprazan, Clarithromycin, and Bismuth: A Propensity Score Matching Analysis" Microorganisms 12, no. 10: 1952. https://doi.org/10.3390/microorganisms12101952
APA StyleCho, J.-H., & Jin, S.-Y. (2024). Comparison of Amoxicillin Administered Twice versus Four Times a Day in First-Line Helicobacter pylori Eradication Using Tegoprazan, Clarithromycin, and Bismuth: A Propensity Score Matching Analysis. Microorganisms, 12(10), 1952. https://doi.org/10.3390/microorganisms12101952