

Simvastatin, Its Antimicrobial Activity and Its Prevention of Alzheimer’s Disease



Abstract
:1. Introduction
2. Simvastatin’s Primary Mode of Action—Targeting HMG-CoA Reductase
3. Antimicrobial Effects of Simvastatin
4. Simvastatin Reduces the Incidence of Alzheimer’s Disease
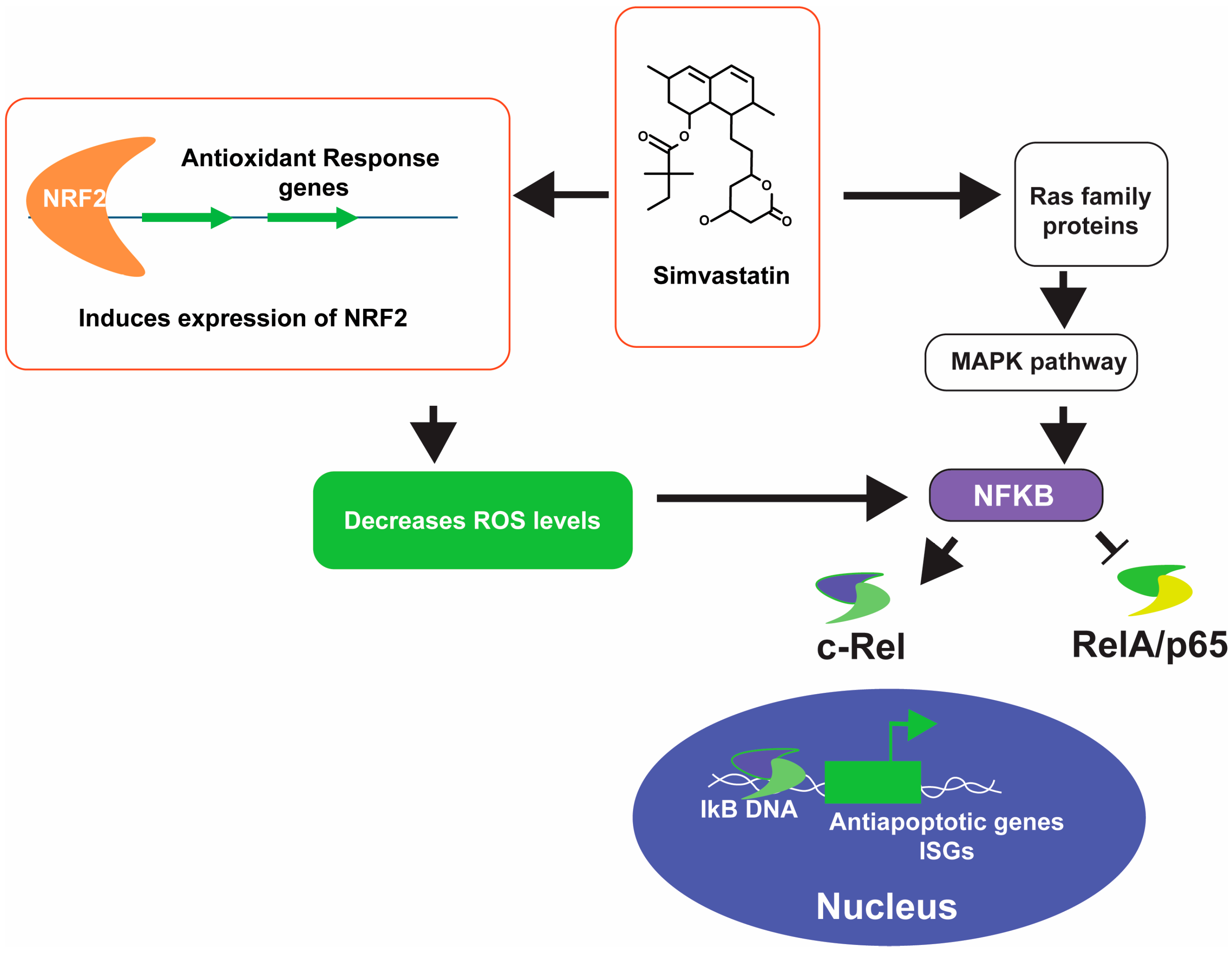
4.1. Anti-Inflammatory Effect
4.2. Reduction of Amyloid Beta and Tau Phosphorylation
4.3. Penetration of Blood Brain Barrier
4.4. Mitochondrial Health
4.5. Improvement of Blood Flow
4.6. Proteostasis
4.7. Controversies and Clinical Trials
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Nelson, R.H. Hyperlipidemia as a risk factor for cardiovascular disease. Prim. Care 2013, 40, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Endo, A. A historical perspective on the discovery of statins. Proc. Jpn. Acad. Ser. B 2010, 86, 484–493. [Google Scholar] [CrossRef] [PubMed]
- Tobert, J.A. Lovastatin and beyond: The history of the HMG-CoA reductase inhibitors. Nat. Rev. Drug Discov. 2003, 2, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Mendes, P.; Robles, P.G.; Mathur, S. Statin-induced rhabdomyolysis: A comprehensive review of case reports. Physiother. Can. 2014, 66, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Furberg, C.D.; Pitt, B. Withdrawal of cerivastatin from the world market. Curr. Control Trials Cardiovasc. Med. 2001, 2, 205–207. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.K.; Laufs, U. Pleiotropic effects of statins. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Mikhailidis, D.P.; Bajraktari, G.; Miserez, A.R.; Cicero, A.F.G.; Bruckert, E.; Serban, M.-C.; Mirrakhimov, E.; Alnouri, F.; Reiner, Ž.; et al. Statin therapy in athletes and patients performing regular intense exercise—Position paper from the International Lipid Expert Panel (ILEP). Pharmacol. Res. 2020, 155, 104719. [Google Scholar] [CrossRef] [PubMed]
- Macreadie, I.G.; Johnson, G.; Schlosser, T.; Macreadie, P.I. Growth inhibition of Candida species and Aspergillus fumigatus by statins. FEMS Microbiol. Lett. 2006, 262, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Westermeyer, C.; Macreadie, I.G. Simvastatin reduces ergosterol levels, inhibits growth and causes loss of mtDNA in Candida glabrata. FEMS Yeast Res. 2007, 7, 436–441. [Google Scholar] [CrossRef]
- Qiao, J.; Kontoyiannis, D.P.; Wan, Z.; Li, R.; Liu, W. Antifungal activity of statins against Aspergillus species. Med. Mycol. 2007, 45, 589–593. [Google Scholar] [CrossRef]
- Kocak, E.; Nemutlu, E.; Kır, S.; Sagıroglu, M.; Özkul, C. Integrative proteomics and metabolomics approach to elucidate the antimicrobial effect of simvastatin on Escherichia coli. Biomed. Chromatogr. 2021, 35, e5180. [Google Scholar] [CrossRef] [PubMed]
- Masadeh, M.; Mhaidat, N.; Alzoubi, K.; Al-azzam, S.; Alnasser, Z. Antibacterial activity of statins: A comparative study of Atorvastatin, Simvastatin, and Rosuvastatin. Ann. Clin. Microbiol. Antimicrob. 2012, 11, 13. [Google Scholar] [CrossRef] [PubMed]
- Thangamani, S.; Mohammad, H.; Abushahba, M.F.N.; Hamed, M.I.; Sobreira, T.J.P.; Hedrick, V.E.; Paul, L.N.; Seleem, M.N. Exploring simvastatin, an antihyperlipidemic drug, as a potential topical antibacterial agent. Sci. Rep. 2015, 5, 16407. [Google Scholar] [CrossRef] [PubMed]
- Graziano, T.S.; Cuzzullin, M.C.; Franco, G.C.; Schwartz-Filho, H.O.; de Andrade, E.D.; Groppo, F.C.; Cogo-Müller, K. Statins and Antimicrobial Effects: Simvastatin as a Potential Drug against Staphylococcus aureus Biofilm. PLoS ONE 2015, 10, e0128098. [Google Scholar] [CrossRef] [PubMed]
- Nyilasi, I.; Kocsubé, S.; Krizsán, K.; Galgóczy, L.; Papp, T.; Pesti, M.; Nagy, K.; Vágvölgyi, C. Susceptibility of clinically important dermatophytes against statins and different statin-antifungal combinations. Med. Mycol. 2014, 52, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Emani, S.; Gunjiganur, G.V.; Mehta, D.S. Determination of the antibacterial activity of simvastatin against periodontal pathogens, Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans: An in vitro study. Contemp. Clin. Dent. 2014, 5, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Kamińska, M.; Aliko, A.; Hellvard, A.; Bielecka, E.; Binder, V.; Marczyk, A.; Potempa, J.; Delaleu, N.; Kantyka, T.; Mydel, P. Effects of statins on multispecies oral biofilm identify simvastatin as a drug candidate targeting Porphyromonas gingivalis. J. Periodontol. 2019, 90, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, J.; Mendes, A.I.; Pacheco, A.R.; Peixoto, M.J.; Pedrosa, J.; Fraga, A.G. Repurposing of statins for Buruli Ulcer treatment: Antimicrobial activity against Mycobacterium ulcerans. Front. Microbiol. 2023, 14, 1266261. [Google Scholar] [CrossRef]
- Haeri, M.R.; White, K.; Qharebeglou, M.; Ansar, M.M. Cholesterol suppresses antimicrobial effect of statins. Iran. J. Basic Med. Sci. 2015, 18, 1253–1256. [Google Scholar]
- Jerwood, S.; Cohen, J. Unexpected antimicrobial effect of statins. J. Antimicrob. Chemother. 2008, 61, 362–364. [Google Scholar] [CrossRef]
- Silva, T.H.S.; Araújo, C.V.; Santos, K.; Alves, N.D.S.; Gomes, T.H.S.; Silva, A.; Silva, N.; Damasceno Júnior, E.C.B.; Carvalho, A.M.A.; Mendes, M.G.A.; et al. Synergic effect of simvastatin in combination with amphotericin B against environmental strains of Cryptococcus neoformans from northeastern Brazil: A prospective experimental study. Sao Paulo Med. J. 2020, 138, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Fan, W.; Duan, M.; Sun, Q.; Fan, B. Simvastatin enhanced antimicrobial effect of Ag(+) against E. faecalis infection of dentine through PLGA co-delivery submicron particles. J. Biomater. Sci. Polym. Ed. 2020, 31, 2331–2346. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, S.; Kushairi, N.; Phan, C.W.; Adhikari, B.; Sabaratnam, V.; Macreadie, I. Dietary Polyphenols: A Multifactorial Strategy to Target Alzheimer’s Disease. Int. J. Mol. Sci. 2019, 20, 5090. [Google Scholar] [CrossRef] [PubMed]
- Goedert, M.; Ghetti, B. Alois Alzheimer: His life and times. Brain Pathol. 2007, 17, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S.; Amieva, H.; Petersen, R.C.; Chételat, G.; Holtzman, D.M.; Hyman, B.T.; Nixon, R.A.; Jones, D.T. Alzheimer disease. Nat. Rev. Dis. Primers 2021, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Zhang, L.; Marshall, I.; Wolfe, C.; Wang, Y. Statin Therapy for Preventing Recurrent Stroke in Patients with Ischemic Stroke: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Observational Cohort Studies. Neuroepidemiology 2022, 56, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, X.; Li, X.; Chen, H.; Hu, Y.; Zhang, X.; Tang, X.; Miao, Y.; Tian, G.; Shang, H. Statins for the Primary Prevention of Coronary Heart Disease. BioMed Res. Int. 2019, 2019, 4870350. [Google Scholar] [CrossRef] [PubMed]
- Wolozin, B.; Wang, S.W.; Li, N.-C.; Lee, A.; Lee, T.A.; Kazis, L.E. Simvastatin is associated with a reduced incidence of dementia and Parkinson’s disease. BMC Med. 2007, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, J.; Steinman, L.; Zamvil, S.S. Statin therapy and autoimmune disease: From protein prenylation to immunomodulation. Nat. Rev. Immunol. 2006, 6, 358–370. [Google Scholar] [CrossRef]
- Taniguchi, K.; Karin, M. NF-κB, inflammation, immunity and cancer: Coming of age. Nat. Rev. Immunol. 2018, 18, 309–324. [Google Scholar] [CrossRef]
- Ghosh, G.; Wang, V.Y.; Huang, D.B.; Fusco, A. NF-κB regulation: Lessons from structures. Immunol. Rev. 2012, 246, 36–58. [Google Scholar] [CrossRef] [PubMed]
- Lietzau, G.; Sienkiewicz, W.; Karwacki, Z.; Dziewiątkowski, J.; Kaleczyc, J.; Kowiański, P. The Effect of Simvastatin on the Dynamics of NF-κB-Regulated Neurodegenerative and Neuroprotective Processes in the Acute Phase of Ischemic Stroke. Mol. Neurobiol. 2023, 60, 4935–4951. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Li, Z.; Zhao, L.; Zhao, W. Simvastatin ameliorate memory deficits and inflammation in clinical and mouse model of Alzheimer’s disease via modulating the expression of miR-106b. Biomed. Pharmacother. 2017, 92, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Xu, N.; Shen, N.; Wang, X.; Jiang, S.; Xue, B.; Li, C. Protein prenylation and human diseases: A balance of protein farnesylation and geranylgeranylation. Sci. China Life Sci. 2015, 58, 328–335. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Trepel, J.; Neckers, L. Ras, ROS and proteotoxic stress: A delicate balance. Cancer Cell 2011, 20, 281–282. [Google Scholar] [CrossRef]
- Kobayashi, K.; Baba, K.; Kambayashi, S.; Okuda, M. Effect of simvastatin on cell proliferation and Ras activation in canine tumour cells. Vet. Comp. Oncol. 2021, 19, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.J.; Liu, Z.-g. Crosstalk of reactive oxygen species and NF-κB signaling. Cell Res. 2011, 21, 103–115. [Google Scholar] [CrossRef]
- Ionescu-Tucker, A.; Cotman, C.W. Emerging roles of oxidative stress in brain aging and Alzheimer’s disease. Neurobiol. Aging 2021, 107, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-C.; Li, C.-Y.; Hsu, C.-H.; Chen, H.-L.; Chen, Y.-H.; Liu, Y.-P.; Liu, Y.-R.; Kuo, H.-F.; Liu, P.-L. Mitochondrial protection by simvastatin against angiotensin II-mediated heart failure. Br. J. Pharmacol. 2019, 176, 3791–3804. [Google Scholar] [CrossRef]
- Fassbender, K.; Simons, M.; Bergmann, C.; Stroick, M.; Lütjohann, D.; Keller, P.; Runz, H.; Kühl, S.; Bertsch, T.; von Bergmann, K.; et al. Simvastatin strongly reduces levels of Alzheimer’s disease β-amyloid peptides Aβ42 and Aβ40 in vitro and in vivo. Proc. Natl. Acad. Sci. USA 2001, 98, 5856–5861. [Google Scholar] [CrossRef]
- Dhakal, S.; Subhan, M.; Fraser, J.M.; Gardiner, K.; Macreadie, I. Simvastatin Efficiently Reduces Levels of Alzheimer’s Amyloid Beta in Yeast. Int. J. Mol. Sci. 2019, 20, 3531. [Google Scholar] [CrossRef] [PubMed]
- Hoglund, K.; Thelen, K.M.; Syversen, S.; Sjogren, M.; von Bergmann, K.; Wallin, A.; Vanmechelen, E.; Vanderstichele, H.; Lutjohann, D.; Blennow, K. The effect of simvastatin treatment on the amyloid precursor protein and brain cholesterol metabolism in patients with Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2005, 19, 256–265. [Google Scholar] [CrossRef]
- Parsons, R.B.; Price, G.C.; Farrant, J.K.; Subramaniam, D.; Adeagbo-Sheikh, J.; Austen, B.M. Statins inhibit the dimerization of beta-secretase via both isoprenoid- and cholesterol-mediated mechanisms. Biochem. J. 2006, 399, 205–214. [Google Scholar] [CrossRef]
- Tuck, B.J.; Miller, L.V.C.; Katsinelos, T.; Smith, A.E.; Wilson, E.L.; Keeling, S.; Cheng, S.; Vaysburd, M.J.; Knox, C.; Tredgett, L.; et al. Cholesterol determines the cytosolic entry and seeded aggregation of tau. Cell Rep. 2022, 39, 110776. [Google Scholar] [CrossRef]
- Riekse, R.G.; Li, G.; Petrie, E.C.; Leverenz, J.B.; Vavrek, D.; Vuletic, S.; Albers, J.J.; Montine, T.J.; Lee, V.M.; Lee, M.; et al. Effect of statins on Alzheimer’s disease biomarkers in cerebrospinal fluid. J. Alzheimer’s Dis. 2006, 10, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Boimel, M.; Grigoriadis, N.; Lourbopoulos, A.; Touloumi, O.; Rosenmann, D.; Abramsky, O.; Rosenmann, H. Statins Reduce the Neurofibrillary Tangle Burden in a Mouse Model of Tauopathy. J. Neuropathol. Exp. Neurol. 2009, 68, 314–325. [Google Scholar] [CrossRef]
- Hamano, T.; Yen, S.H.; Gendron, T.; Ko, L.W.; Kuriyama, M. Pitavastatin decreases tau levels via the inactivation of Rho/ROCK. Neurobiol. Aging 2012, 33, 2306–2320. [Google Scholar] [CrossRef]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef] [PubMed]
- Lütjohann, D.; Papassotiropoulos, A.; Björkhem, I.; Locatelli, S.; Bagli, M.; Oehring, R.D.; Schlegel, U.; Jessen, F.; Rao, M.L.; von Bergmann, K.; et al. Plasma 24S-hydroxycholesterol (cerebrosterol) is increased in Alzheimer and vascular demented patients. J. Lipid Res. 2000, 41, 195–198. [Google Scholar] [CrossRef]
- Vuu, Y.M.; Kadar Shahib, A.; Rastegar, M. The Potential Therapeutic Application of Simvastatin for Brain Complications and Mechanisms of Action. Pharmaceuticals 2023, 16, 914. [Google Scholar] [CrossRef]
- Vuletic, S.; Riekse, R.G.; Marcovina, S.M.; Peskind, E.R.; Hazzard, W.R.; Albers, J.J. Statins of different brain penetrability differentially affect CSF PLTP activity. Dement. Geriatr. Cogn. Disord. 2006, 22, 392–398. [Google Scholar] [CrossRef]
- Csomó, K.; Belik, A.; Hrabák, A.; Kovács, B.; Fábián, O.; Valent, S.; Varga, G.; Kukor, Z. Effect of Pravastatin and Simvastatin on the Reduction of Cytochrome C. J. Pers. Med. 2022, 12, 1121. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Zimbron, L.F.; Luna-Muñoz, J.; Mena, R.; Vazquez-Ramirez, R.; Kubli-Garfias, C.; Cribbs, D.H.; Manoutcharian, K.; Gevorkian, G. Amyloid-β Peptide Binds to Cytochrome C Oxidase Subunit 1. PLoS ONE 2012, 7, e42344. [Google Scholar] [CrossRef]
- Durhuus, J.A.; Hansson, S.; Morville, T.; Kuhlman, A.B.; Dohlmann, T.L.; Larsen, S.; Helge, J.W.; Angleys, M.; Muniesa-Vargas, A.; Bundgaard, J.R.; et al. Simvastatin improves mitochondrial respiration in peripheral blood cells. Sci. Rep. 2020, 10, 17012. [Google Scholar] [CrossRef]
- Xie, J.C.; Ma, X.Y.; Liu, X.H.; Yu, J.; Zhao, Y.C.; Tan, Y.; Liu, X.Y.; Zhao, Y.X. Hypoxia increases amyloid-β level in exosomes by enhancing the interaction between CD147 and Hook1. Am. J. Transl. Res. 2018, 10, 150–163. [Google Scholar]
- Thomas, T.; Thomas, G.; McLendon, C.; Sutton, T.; Mullan, M. β-Amyloid-mediated vasoactivity and vascular endothelial damage. Nature 1996, 380, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Shen, M.; Tan, W.L.W.; Chen, I.Y.; Liu, Y.; Yu, X.; Yang, H.; Zhang, A.; Liu, Y.; Zhao, M.-T.; et al. Statins improve endothelial function via suppression of epigenetic-driven EndMT. Nat. Cardiovasc. Res. 2023, 2, 467–485. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, S.; Macreadie, I. Protein Homeostasis Networks and the Use of Yeast to Guide Interventions in Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 8014. [Google Scholar] [CrossRef]
- Uchiyama, T.; Atsuta, H.; Utsugi, T.; Ohyama, Y.; Nakamura, T.; Nakai, A.; Nakata, M.; Maruyama, I.; Tomura, H.; Okajima, F.; et al. Simvastatin induces heat shock factor 1 in vascular endothelial cells. Atherosclerosis 2006, 188, 265–273. [Google Scholar] [CrossRef]
- Kou, X.; Jiang, X.; Liu, H.; Wang, X.; Sun, F.; Han, J.; Fan, J.; Feng, G.; Lin, Z.; Jiang, L.; et al. Simvastatin functions as a heat shock protein 90 inhibitor against triple-negative breast cancer. Cancer Sci. 2018, 109, 3272–3284. [Google Scholar] [CrossRef]
- Rodrigues, G.; Moreira, A.J.; Bona, S.; Schemitt, E.; Marroni, C.A.; Di Naso, F.C.; Dias, A.S.; Pires, T.R.; Picada, J.N.; Marroni, N.P. Simvastatin Reduces Hepatic Oxidative Stress and Endoplasmic Reticulum Stress in Nonalcoholic Steatohepatitis Experimental Model. Oxidative Med. Cell. Longev. 2019, 2019, 3201873. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.M.; Li, X.; Xu, M.; Abais, J.M.; Chen, Y.; Riebling, C.R.; Boini, K.M.; Li, P.L.; Zhang, Y. Enhancement of autophagy by simvastatin through inhibition of Rac1-mTOR signaling pathway in coronary arterial myocytes. Cell. Physiol. Biochem. 2013, 31, 925–937. [Google Scholar] [CrossRef]
- Dhakal, S. ‘The awesome power of yeast’ in Alzheimer’s disease research. Microbiol. Aust. 2021, 42, 130–133. [Google Scholar] [CrossRef]
- Macreadie, I. Clearing Deleterious Proteins for Healthier Aging. Open J. Soc. Sci. 2019, 7, 128–132. [Google Scholar] [CrossRef]
- Caine, J.; Sankovich, S.; Antony, H.; Waddington, L.; Macreadie, P.; Varghese, J.; Macreadie, I. Alzheimer’s Aβ fused to green fluorescent protein induces growth stress and a heat shock response. FEMS Yeast Res. 2007, 7, 1230–1236. [Google Scholar] [CrossRef] [PubMed]
- Simons, M.; Schwärzler, F.; Lütjohann, D.; von Bergmann, K.; Beyreuther, K.; Dichgans, J.; Wormstall, H.; Hartmann, T.; Schulz, J.B. Treatment with simvastatin in normocholesterolemic patients with Alzheimer’s disease: A 26-week randomized, placebo-controlled, double-blind trial. Ann. Neurol. 2002, 52, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, M.; Gustafsson, K.; Syversen, S.; Olsson, A.; Edman, A.; Davidsson, P.; Wallin, A.; Blennow, K. Treatment with simvastatin in patients with Alzheimer’s disease lowers both alpha- and beta-cleaved amyloid precursor protein. Dement. Geriatr. Cogn. Disord. 2003, 16, 25–30. [Google Scholar] [CrossRef]
- Li, G.; Larson, E.B.; Sonnen, J.A.; Shofer, J.B.; Petrie, E.C.; Schantz, A.; Peskind, E.R.; Raskind, M.A.; Breitner, J.C.; Montine, T.J. Statin therapy is associated with reduced neuropathologic changes of Alzheimer disease. Neurology 2007, 69, 878–885. [Google Scholar] [CrossRef]
- Sano, M.; Bell, K.L.; Galasko, D.; Galvin, J.E.; Thomas, R.G.; van Dyck, C.H.; Aisen, P.S. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology 2011, 77, 556–563. [Google Scholar] [CrossRef]
- McGuinness, B.; Craig, D.; Bullock, R.; Passmore, P. Statins for the prevention of dementia. Cochrane Database Syst. Rev. 2016, 2016, Cd003160. [Google Scholar] [CrossRef]
- Geifman, N.; Brinton, R.D.; Kennedy, R.E.; Schneider, L.S.; Butte, A.J. Evidence for benefit of statins to modify cognitive decline and risk in Alzheimer’s disease. Alzheimer’s Res. Ther. 2017, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Petek, B.; Häbel, H.; Xu, H.; Villa-Lopez, M.; Kalar, I.; Hoang, M.T.; Maioli, S.; Pereira, J.B.; Mostafaei, S.; Winblad, B.; et al. Statins and cognitive decline in patients with Alzheimer’s and mixed dementia: A longitudinal registry-based cohort study. Alzheimer’s Res. Ther. 2023, 15, 220. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Microorganism | Effect | Mechanism of action | Concentration | Reference |
| Candida albicans | Growth inhibition | ND | 100 µM | [8] |
| Aspergillus fumigatus | Growth inhibition | ND | 0.1 µM | [8] |
| Candida glabrata | Growth inhibition | Reduce ergosterol. Causes loss of mitochondrial DNA. | 20 µM | [9] |
| Aspergillus spp. | Growth inhibition | ND | MIC ranging from 16 to 108 µg/mL except for A. niger and A. terreus which were >256 µg/mL. MFC ranging from 32–128 µg/mL for those that are determined. | [10] |
| Escherichia coli | Growth inhibition | Inhibits chaperone protein DnaK (a homologue of mammalian HSP70) Inactivation of AcrAB-TolC efflux pump. Alters amino acid synthesis pathway, ribosomal protein synthesis, TCA cycle and glyoxylate dicarboxylate metabolism. | MIC: 128 µg/mL | [11] |
| Methicillin sensitive Staphylococcus aureus (MSSA) ATTC 25213 | Growth inhibition | Inhibits macromolecular synthesis pathway (DNA replication, RNA synthesis, protein synthesis, lipid synthesis, cell wall synthesis) Enhances protein degradation. Inhibits S. aureus toxin production. Reduces biofilm formation. Reduces inflammatory cytokines induced by bacterial infection in skin. Synergistic activity with other antimicrobials. | MIC: 41.67 ± 18.04 µg/mL | [12,13,14] |
| Methicillin resistant Staphylococcus aureus SA (MRSA) ATTC 43300 | Growth inhibition | MIC: 83.33 ± 36.08 µg/mL | ||
| Vancomycin sensitive Enterococcus ATTC 19433 | Growth inhibition | ND | MIC: 83.33 ± 36.08 µg/mL | |
| Acinetobacter baumannii ATTC 17978 | Growth inhibition | ND | MIC: 15.62 ± 0.00 µg/mL | |
| Enterrobacter aerogenes ATTC 29751 | Growth inhibition | ND | MIC: 15.62 ± 0.00 µg/mL | |
| Trichophyton rubrum ATCC 28188 | Growth inhibition | ND | MIC: 6.25–12.5 µg/mL | [15] |
| Trichophyton mentagrophytes ATCC 9533 | Growth inhibition | ND | MIC: 6.25 µg/mL | |
| Microsporum gypseum (ATCC 24102) | Growth inhibition | ND | MIC: 6.25–12.5 µg/mL | |
| Microsporum canis (ATCC 36299) | Growth inhibition | ND | MIC: 6.25–12.5 µg/mL | |
| Aggregatibacter actinomycetemcomitans | Growth inhibition | ND | MIC: <1 µg/mL | [16,17] |
| Porphyromonas gingivalis | Growth inhibition | ND | MIC: 2 µg/mL | |
| Mycobacterium ulcerans | Growth inhibition (1.7-fold reduction in colony forming unit (CFU)) | ND | IC50: 54.13 μg/mL | [18] |
| Year | Study Design | Findings | Ref | Remarks |
|---|---|---|---|---|
| 2002 | Randomized, placebo-controlled, double-blind study. Research Question: Do statins alter cholesterol metabolites and reduce amyloid beta (Aβ) levels in the cerebrospinal fluid of patients with Alzheimer’s disease? Participants: 44 patients | Simvastatin significantly decreased Aβ40 and 24S-hydroxycholesterol levels in the cerebrospinal fluid of patients with mild AD. These changes were not observed in more severely affected patients. | [66] | The findings suggest benefits of using simvastatin in mild AD, but not in severe AD. |
| 2003 | Clinical and biological effects of cholesterol-lowering treatment with a statin Participants: 19 patients with Alzheimer’s disease. Statin Dosage: Simvastatin 20 mg/day for 12 weeks. Outcome measurement:
| CSF α-sAPP and CSF β-sAPP were significantly reduced, but the CSF levels of tau, phospho-tau, Aβ42, and the plasma levels of Aβ42 were unchanged. The ADAS-cog score was slightly increased (p < 0.05). Simvastatin acts directly on the processing of APP by inhibiting both the α- and the β-secretase pathways. | [67] | Simvastatin reduced APP processing indicating potential in reducing Aβ42 if administered early in life. However, patients of AD may not benefit much as the irreversible damage to the brain persists in AD patients. |
| 2007 | Data from the decision support system of the US Veterans Affairs database, which contain diagnostic, medication, and demographic information on 4.5 million subjects. Participants: 700,000 subjects taking simvastatin for hypercholesterolemia and over 50,000 subjects taking atorvastatin who were aged >64 years. | Simvastatin strongly reduced the incidence of dementia, and atorvastatin showed slight reduction. | [28] | Perhaps this is the only prospective study with data from sufficient subjects at an early age group of ( ≥ 65 years). Simvastatin has a strong potential as preventative by reducing the incidence of AD. |
| 2007 | Cognitively normal subjects: Brain autopsies on 110 subjects, aged 65 to 79 years. Statin Usage: Simvastatin, pravastatin, lovastatin, or atorvastatin user vs nonuser. | The risk for typical AD pathology was reduced in statin users and there was an association between antecedent statin use and neurofibrillary tangle burden at autopsy. | [68] | Simvastatin reduces neurofibrillary tau tangles. |
| 2011 | Randomized, double-blind, placebo-controlled trial. Participants: Mild to moderate AD and normal lipid levels. Statin usage: Simvastatin, 20 mg/day, for 6 weeks then 40 mg per day for the remainder of 18 months or identical placebo. Outcome measurement: Alzheimer’s Disease Assessment Scale-cognitive portion (ADAS-Cog) and clinical global change, cognition, function, and behaviour. | Simvastatin lowered lipid levels but had no effect on change in ADAS-Cog score or the secondary outcome measures. Simvastatin had no benefit on the progression of symptoms in individuals with mild to moderate AD despite significant lowering of cholesterol. | [69] | Simvastatin may not be suitable for treatment of mild and moderate AD. |
| 2016 | Double-blind, randomised, placebo-controlled trials. Statin dosage: Administered for at least 12 months to people at risk of dementia. Participants: All participants had a history of, or risk factors for, vascular disease: 26,340 participants aged 40 to 82 years of whom 11,610 were aged 70 or older. | Statins (pravastatin and simvastatin) given late in life did not prevent dementia. | [70] | Simvastatin may not be beneficial for prospective AD patients after short term usage. |
| 2017 | Analysis of datasets of integrated clinical trials, and prospective observational studies. | The incidence of AD was significantly lower in statin users. ApoE4/ApoE4 AD patients treated with statins showed better cognitive function over the course of 10-year follow-up. | [71] | Long term studies may help understand the benefits of statins in AD patients. |
| 2023 | A longitudinal cohort study using the Swedish Registry for Cognitive/Dementia Disorders: 15,586 patients with mean age of 79.5 years at diagnosis and mostly women (59.2 %). | Taking one defined daily dose of statins on average was associated with more MMSE points after 3 years compared to no use of statins. Simvastatin users showed more MMSE points after 3 years compared to atorvastatin and rosuvastatin users. Younger simvastatin users had more MMSE points compared to younger atorvastatin users after 3 years. | [72] | Simvastatin performed better than other statins; younger simvastatin users benefited more. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhakal, S.; Macreadie, I.G. Simvastatin, Its Antimicrobial Activity and Its Prevention of Alzheimer’s Disease. Microorganisms 2024, 12, 1133. https://doi.org/10.3390/microorganisms12061133
Dhakal S, Macreadie IG. Simvastatin, Its Antimicrobial Activity and Its Prevention of Alzheimer’s Disease. Microorganisms. 2024; 12(6):1133. https://doi.org/10.3390/microorganisms12061133
Chicago/Turabian StyleDhakal, Sudip, and Ian G. Macreadie. 2024. "Simvastatin, Its Antimicrobial Activity and Its Prevention of Alzheimer’s Disease" Microorganisms 12, no. 6: 1133. https://doi.org/10.3390/microorganisms12061133
APA StyleDhakal, S., & Macreadie, I. G. (2024). Simvastatin, Its Antimicrobial Activity and Its Prevention of Alzheimer’s Disease. Microorganisms, 12(6), 1133. https://doi.org/10.3390/microorganisms12061133