Abstract
Pregnant women (PW) are at a higher risk of diseases and hospitalization from viral respiratory infections, particularly influenza and SARS-CoV-2, due to cardiopulmonary and immunological changes. This study assessed the impact of viral respiratory infections on PW hospitalized with severe acute respiratory infection (SARI) prior to the COVID-19 pandemic. It is a cross-sectional study with 42 PW and 85 non-pregnant women (NPW) admitted with SARI to two tertiary hospitals between January 2015 and December 2019. The rates of virus prevalence, SARI hospitalization, length of hospital stay, oxygen supplementation, intensive care unit (ICU) admission, and death were comparable between PW and NPW. A multivariate analysis showed that PW had a higher rate of viral SARI hospitalizations (OR = 2.37; 95% CI = 1.02–5.48) as compared to NPW, with the influenza virus being the most prevalent (aOR = 7.58; 95% CI = 1.53–37.66). The length of hospital stays (aOR = 0.83; 95% CI = 0.73–0.95) and admissions to the ICU (aOR = 0.028; 95% CI = 0.004–0.25) were lower in PW as compared to hospitalized NPW. The influenza virus had a greater impact on the frequency of SARI in the group of PW, and these had a better outcome than NPW due to the earlier antiviral treatment they received.
1. Introduction
Community-acquired pneumonia (CAP) is the leading cause of hospitalization and mortality worldwide [1], with community respiratory viruses (CRVs) being responsible for 15–30% of cases [2]. Many of these cases are associated with severe acute respiratory illness (SARI), an acute respiratory infection that requires hospitalization and can be lethal [3].
Severe acute respiratory illness (SARI) comprises a set of symptoms, such as the following: O2 saturation <95% in room air, shortness of breath or increased respiratory rate assessed according to age, worsening of the clinical picture of the underlying disease, and hypotension in relation to the usual blood pressure of the patient or individual of any age with acute respiratory failure [4]. It is characterized by acute bilateral inflammatory pulmonary infiltrates and severe hypoxia [5]. It may have an infectious or non-infectious cause, including pneumonia, non-pulmonary sepsis, aspiration of gastric and/or oral esophageal contents, and severe trauma. It is a common cause of respiratory failure in critically ill patients and is defined by the acute appearance of non-cardiogenic pulmonary edema, hypoxemia, and the need for mechanical ventilation [6].
Among infectious causes, CRVs identified in SARI include influenza A and B (IF), human adenovirus (hAdV), respiratory syncytial virus (RSV), human rhinovirus (hRV), human metapneumovirus (hMPV), the parainfluenza virus group (PIV 1,2, 3,4), human enterovirus (hEV), human bocavirus (hBoV), and human coronavirus-hCoV (229E, OC43, HKU1, NL-63) [7]. Additionally, SARS-CoV-2 has emerged as a recent threat to public health [8]. CRV infections in pregnant women can result in a spectrum of mild to severe cases of acute respiratory illness [9].
Pregnancy is a serious risk factor for influenza and COVID-19, as physiological changes that occur during pregnancy—including decreased lung capacity, cell-mediated immunity, and increased oxygen consumption—predispose those women to worse outcomes than the general population [10]. Vaccination is an essential element of pre-pregnancy, prenatal, and postpartum care, as it should protect against the risk of complications and progression to SARI during the prenatal or postpartum period [11,12].
In the Brazilian A (H1N1) vaccination campaign in 2010, planned as a national program, the vaccine was mandatory in all public health institutions and especially in those that offered prenatal care [13]. Since 2016, the Brazilian Ministry of Health has extended the recommendation to children <5 years of age, pregnant women, people with chronic non-communicable diseases, and health professionals [14,15].
With the 2020 COVID-19 pandemic, immunization against SARS-CoV-2 has been a priority, and current recommendations from the World Health Organization, the Centers for Disease Control and Prevention, and professional organizations are for pregnant, postpartum, and breastfeeding women receive vaccination against SARS-CoV-2, as these women were designated as a risk group for SARI [11]. In 2021 in Brazil, the estimated case fatality rate of COVID-19 among pregnant and postpartum women was 7.2%, compared to 2.8% in the general population. Furthermore, SARS-CoV-2 has been associated with adverse perinatal events, such as premature birth, fetal loss, and neonatal mortality [16].
Despite the existence of immunization, treatment, and a global surveillance network for influenza viruses and SARS-CoV-2, studies on viral SARI in pregnant women remain limited [17,18]. In addition to these, only research on RSV in pregnant women has gained prominence recently; however, the focus is on the protection of newborns [19].
This study aimed to examine the burden of viral respiratory infections in pregnant women hospitalized with SARI prior to the COVID-19 pandemic.
2. Materials and Methods
A retrospective, cross-sectional study was carried out between January 2015 and December 2019 in two tertiary hospitals in Curitiba, Southern Brazil, using secondary data from medical record reviews.
All information on hospitalizations and deaths related to SARI is recorded in the Epidemiological Surveillance Information Service (SIVEP-Gripe) and forms mandatory notifications. SIVEP-Gripe records several variables, some of which include date of notification, onset of symptoms, hospitalization, clinical sample collection, detection, laboratory results, and case resolution. Access to the identified and non-duplicated data is publicly available (https://opendatasus.saude.gov.br/dataset/bd-srag-2019 accessed on 28 June 2024).
Both hospitals approved the study via their respective Ethics Committees under the identification numbers 15599.8.0000.0096 and 155.99119.8.3001.5225, respectively.
Sampling: The study was carried out with nasopharyngeal swabs collected 3 to 5 days from the onset of symptoms in patients admitted to both hospitals. The genetic material was extracted with the following commercial kits: Invitrogen PureLink, (Invitrogen, Carlsbad, CA, USA), High Pure Viral Nucleic Acid (Roche, Inc., Basel, Switzerland), and Viral RNA, Viral DNA Extraction (Promega, Madison, WI, USA), QIAsymphony automation equipment (Qiagen, Hilden, Germany), and MagNAPure96 equipment (Roche, Mannheim, Germany). Afterwards, the reverse transcription technique was performed, followed by the quantitative polymerase chain reaction (RT-qPCR) following the WHO protocol (2009) [20] as updated in 2017 [21].
Of the 1132 SARI cases reported to SIVEP (Epidemiological Surveillance Information Service) between 2015 and 2019 in both tertiary hospitals, 49 pregnant women (PW) and 159 non-pregnant women (NPW) were eligible. Of these, 42 (85.7%) PW and 85 (53.4%) NPW were included in the study; adhering to the inclusion and exclusion criteria, 42/49 PW and 85/159 NPW with SARS were requested for research on respiratory viruses.
Inclusion criteria: PW aged ≥ 18 years, at any gestational period, hospitalized with SARI, and investigated for the following community respiratory viruses (CRVs): influenza A and B, hAdV, RSV, hRV, hMPV, hPIV group, hEV, hBoV, hCoV HKU1, 229E, OC43, and NL63 via RT-qPCR. NPW aged between 18 and 45 years, without underlying diseases, and hospitalized with SARI with the same CRVs described above.
Exclusion criteria of PW with SARI: Seven were excluded: three due to lack of RT-qPCR, three for being postpartum, and one with a diagnosis of tuberculosis (Figure 1).
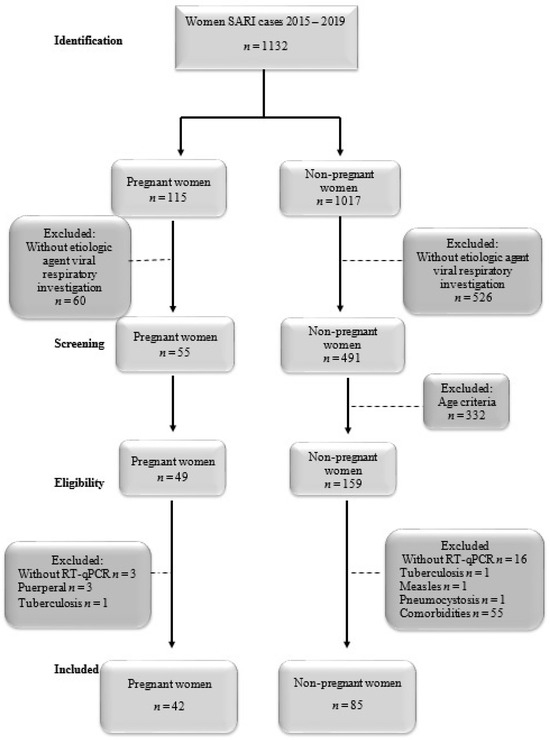
Figure 1.
Flowchart of the study.
NPW with SARI: In total, 74 were excluded (46.5%): 16 due to lack of RT-qPCR, 1 with measles, 1 with pneumonia, 1 with a diagnosis of tuberculosis, and 55 with comorbidities (Figure 1).
Definitions: Primary outcome: ICU admission. Secondary outcomes: length of hospital stay, ventilatory support, and death. Potential confounders: viral co-infection. Effect modifiers: influenza immunization and treatment, underlying diseases, and age group. Bias: etiologic agent unknown in negative RT-qPCRs.
Data analysis: Statistical analyses were performed using IBM SPSS version 23. Univariate analysis used Fisher’s exact and Chi-square tests for categorical variables and the Mann–Whitney and Kruskal–Wallis tests for continuous variables, as appropriate. Multivariate logistic regression analyses evaluated covariates related to outcomes. The adjusted odds ratio (aOR) was calculated using the multivariate model with a stepwise selection of variables, with a cutoff point of p < 0.2, and a Pearson’s analysis to test the model fit. Multivariate linear regression analysis was conducted to assess the impact of viral SARI on length of stay. All statistical tests were two-sided, with significance set at p < 0.05, and a confidence interval (CI) of 95%.
3. Results
Of the 1132 women with SARI cases between 2015 and 2019 in both tertiary hospitals, 60 PW and 526 NPW were excluded for not undergoing investigation for respiratory viruses. A total of 49 PW and 159 NPW were eligible to participate in this study. Of these, 42 (86%) PW and 85 (53%) NPW were included, as shown in Figure 1.
3.1. Clinical–Epidemiological Characteristics
The SARI cases within the study period among PW were concentrated in 2018, while in NPW, they were distributed without much discrepancy, with 2015 having the lowest and 2019 having the highest number of cases, as depicted in Figure 2.
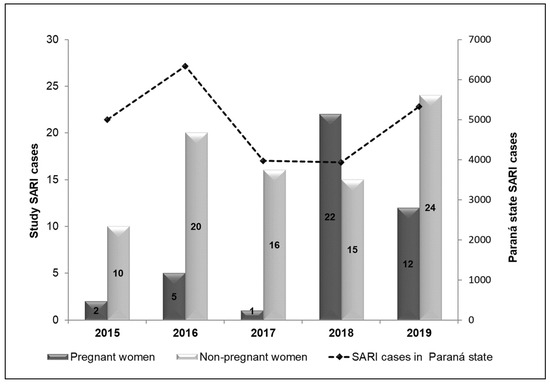
Figure 2.
SARI cases among pregnant and non-pregnant women included in the study (primary axis) and the total number of SARI cases in the state of Paraná (secondary axis); absolute cases of SARI between 2015 and 2019. Legend: SARI, severe acute respiratory syndrome.
The peak of SARI cases in PW occurred during the coldest months (April–September), including viral SARI, which was concentrated in the second trimester of 2018 (April–Jun) (Figure 3A). The NPW showed similar seasonality, with more evenly distributed cases of SARI and viral SARI as compared to PW. However, the highest number of viral infections in NPW occurred in the third quarter (July–September) of 2016 and the fourth quarter (October–December) of 2017 (Figure 3B).
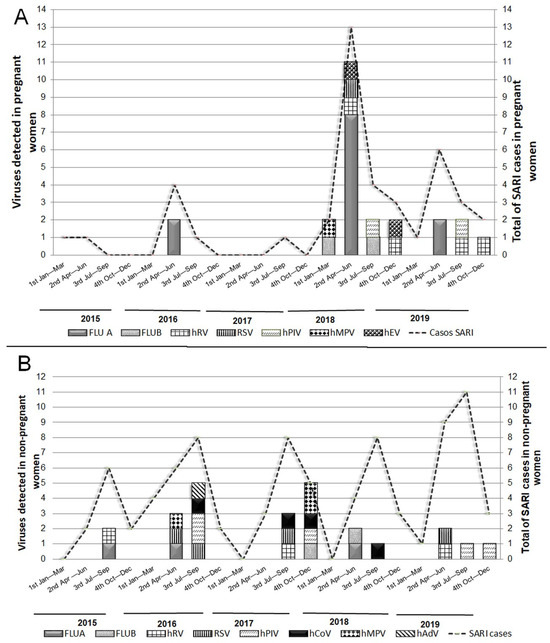
Figure 3.
Viruses identified in pregnant (A) and non-pregnant women (B) between 2015 and 2019. Horizontal axis data were presented in the 4 annual quarters; 1st: January–March; 2nd: April–Jun; 3rd: Jul–September; 4th: October–December. Primary axis—number of viruses identified. Secondary axis—total of SARI cases in the group. FLU A: influenza type A; FLU B: influenza type B; hMPV: human metapneumovirus; hADV: human adenovirus; hPIV: parainfluenza virus; hRV: rhinovirus; RSV: respiratory syncytial virus; hCOV: coronavirus; hEV: enterovirus.
There was no difference in the number of PW hospitalized with SARI based on the gestational period. Only 45% of PW were immunized against influenza. Two-thirds of PW with asthma were infected with hRV, and one HIV-positive patient was infected with influenza. Of the five PW with comorbidities, only the HIV patients had been vaccinated against influenza. Antiviral treatment was prescribed more frequently in PW than in NPW (p < 0.0001). All PW with viral SARI (21/21) and 10/24 of NPW received antiviral therapy. A multivariate analysis showed that hospitalization rates for viral SARI were higher for PW than for NPW (aOR = 2.37; 95% CI = 1.02–5.48; p = 0.044), as shown in Table 1.

Table 1.
Clinical–epidemiological characteristics of pregnant and non-pregnant women groups hospitalized for SARI from 2015 to 2019.
3.2. Impact of Viral SARI on PW and NPW
The median age of PW with viral SARI was similar to that of NPW. Of the 127 (42 PW + 85 NPW) SARI cases, 45 (35%) were positive for viruses. Of these, 50% (21/42) were PW and 28% (24/85) were NPW. Among the 14 viruses investigated via RT-qPCR, hBoV, hCoV, and hAdV were not identified in the PW group, and hEV was recognized only in the PW group.
Out of the 21 PW with viral SARI, 14 (67%) were infected with influenza and 10 (71.4%) did not receive the influenza vaccine. Of the four that received the vaccine, two received the vaccine less than 30 days before the infection, two were infected with influenza B, which was absent in the trivalent vaccine, and only one of the PW diagnosed with influenza SARI had been adequately immunized.
There was no difference in the median time of symptom onset and hospitalization between groups; the medical records of 95% (n = 20/21) of the PW and only 71% (n = 17/24) of the NPW were available. Three PW were co-infected: two with hRV, and only one with SARI had influenza and an RSV co-infection, was admitted to the ICU, had no comorbidities, and was not vaccinated. No cases of hCoV infections (HKU, OC43, and NL63) were detected.
In the NPW group, 24 were positive for viral SARI. The distributions of viral etiological agents were more homogeneous. Influenza was responsible for five (20.8%), and the other CRVs were detected in 15 patients (Table 2). Among these, one PIV + RSV co-infection was identified, and only hEV was not identified in the NPW group.
Table 2.
Impact of viral SARI on pregnant and non-pregnant women groups hospitalized from 2015 to 2019.
The logistic regression showed that the likelihood of viral SARI via influenza was seven times greater in PW than in NPW (aOR = 7.58; 95% IC = 1.53–37.66; p = 0.013).
However, the risk of NPW being admitted to the ICU due to viral SARI was 16 times higher than that of PW (aOR = 0.028; 95% IC = 0.004–0.25; p = 0.001). Nonetheless, there was no difference in median age or co-infection rates in the PW group. Linear regression showed a 16-day increase in the length of hospital stay for viral SARI in the NPW group (β = 16.38; 95% IC = 0.57–32.18; p = 0.043); see Table 2.
4. Discussion
In this study, influenza-associated viral SARI had a more significant impact on the number of hospitalizations among PW than NPW, similar to that found by Creanga et al., 2010, where pregnant women had a higher hospitalization rate and were more likely to have serious illnesses after the first trimester [22].
In Brazil, after the 2009 influenza A(H1N1) pandemic, pregnant women considered part of a risk group received greater attention, as they were susceptible to developing SARI with high morbidity and increased risk of death [13,23,24].
A series of studies in Brazil have highlighted the significant impact of SARI, particularly in the context of the COVID-19 pandemic. Bastos et al. (2020) [25] and Niquini et al. (2020) [26] found an increase in hospitalizations for SARS due to COVID-19 in people with comorbidities, indicating a potential for a more severe progression of the disease. Leal et al. (2021) [27] highlighted the high mortality among pregnant women with SARS due to COVID-19. These findings highlight the importance of continued surveillance and specific interventions to mitigate the impact of viral SARI, especially in vulnerable populations.
Influenza vaccine coverage, the rate of neuraminidase inhibitor prescriptions, and early hospitalization likely explain these findings [18,19].
The distribution of total SARI cases followed influenza seasonality in both groups [28]. The viral SARI rate among PW was higher than NPW, consistent with the findings from the state of Paraná. Influenza was the most frequent among the investigated viruses in PW, followed by hRV, with a similar profile as described previously [9,29]. In accordance with Azziz-Baumgartner et al. (2021) [30], we did not identify any cases of hAdV among PW.
The influenza vaccine coverage in PW was below the target recommended by immunization policies, ranging from 58 to 76% [19] (MS, 2021). The low vaccination coverage observed was consistent with current studies that reported vaccination rates between 5 and 58% among PW [30,31], with an average of 59% for the American continent according to the Pan American Health Organization (PAHO) [32].
Vaccination is the main public health measure used to reduce the frequency of severe influenza cases [14]. As of 2009, the benefits of influenza vaccination were observed not only for pregnant women but also for newborns during the first six months of life [15]. Vaccination with either the seasonal or pandemic vaccine has been shown to be cost-effective in pregnancy. After vaccination, pregnant women had protective concentrations of anti-influenza antibodies, conferring immunogenicity to newborns [33].
The prevalence of comorbidities among PW was lower than previously described (approximately 30%), with asthma being the most frequent, followed by diabetes and hypertension [34]. Although antiviral treatment should be prescribed for all SARI patients [35], prescription was higher for PW than for NPW, especially among those with viral SARI, for which all PW were treated, unlike the other group, which was not attended to in time to institute treatment because it was not a priority [36].
PW were twice as likely to be hospitalized for viral SARI than NPW, with influenza being the main cause of viral SARI, as described previously [37] and confirmed in the present study. However, meta-analysis studies have shown that despite the increase in the need for hospitalization, pregnancy was not associated with more serious flu-associated outcomes, such as ICU admission and death [38,39]. Consistent with our findings, Mertz et al. (2019) found a seven-fold increased risk of influenza SARI among PW compared to NPW. PW with viral SARI also had a decreased length of hospital stay, a finding not previously described.
During the (H1N1)pdm09 pandemic, no differences were found in histopathology between severe cases of PW and NPW women [40]. Although Littauer et al. (2017) demonstrated in a mice model that pregnancy reduces viral clearance in the lungs, they did not observe any difference between the expression of inflammatory cytokines and chemokines in the lungs of PW and NPW mice [41,42].
Prophylaxis, treatment, and clinical management measures may also explain our findings. We observed that 71.4% of PW with influenza did not receive the flu vaccine in the present study. A recent meta-analysis study reported that immunization prevented 50–70% of influenza infections and 45–65% of worse outcomes [43]. However, adherence to vaccination by PW faces obstacles due to a lack of knowledge regarding the risks of influenza or the benefits of vaccination [44]. According to the Centers for Disease Control and Prevention (CDC) (2017), 21% of PW did not receive influenza vaccine recommendations from doctors or medical staff [45].
Antiviral treatment has also been shown to reduce the risk of worse outcomes, including the length of hospital stay, ICU admission, and death in PW [46,47]. In this study, all PW with viral SARI received antiviral treatment. However, our data on the prescription of antivirals suggest that the clinical management of PW is more precise, targeting interventions in the early stages of the infection, unlike what is observed with NPW, who are clinically managed late, with a risk of worse results [18]. Although there are national guidelines for the clinical management of SARI [35], some hospital protocols may differ depending on their participation in the influenza surveillance network or the availability of hospital beds. As NPW are not a risk group for the development of SARI [18], the majority of these patients tend to be hospitalized in more advanced stages of the disease in a tertiary hospital; this is in addition to the lack of clinical–epidemiological data available due to the retrospective collection of data in medical records. All these data reinforce the findings from the present study, emphasizing the importance of investigating factors associated with the clinical evolution and severity of viral SARI in pregnant women, in order to promote public health decisions in health programs and specific clinical management protocols for this group.
This study had some limitations: the small number of participants due to the specificity of the selected group and the large number of SARI notification forms with incomplete data, including substantial under-reporting. Even so, the data presented in this study are extremely relevant and could serve as a basis for expanded studies and for decision-making in public policies to reinforce the recommendation of immunization for pregnant women to prevent SARI due to influenza.
5. Conclusions
The impact of the influenza virus on the number of SARI hospitalizations is usually greater in pregnant women (PW) compared to non-pregnant women (NPW). However, this study highlights an inverse association with disease severity, emphasizing the importance of early antiviral treatment. Additionally, this work underscores the need for new strategies to increase vaccination coverage and ensure accurate clinical management and treatment to reduce the SARI viral burden in pregnant women.
Author Contributions
Conceptualization, M.B.N., S.M.L. and M.d.C.D.; methodology, S.M.L. and M.P.; software, B.A.L., M.E.G. and S.R.; validation, B.A.L. and S.M.L.; formal analysis, M.B.N., S.M.R., J.C.d.O. and N.S.d.C.; investigation, S.M.L., L.A.P., M.P., S.R. and M.E.G.; resources, M.B.N., M.d.C.D., S.R. and M.E.G.; writing—original draft preparation, B.A.L. and S.M.L.; writing—review and editing, M.B.N., S.M.R., J.C.d.O. and N.S.d.C.; visualization, S.M.L., B.A.L., M.E.G., S.R., M.d.C.D., M.P., L.A.P., S.M.R., N.S.d.C., J.C.d.O. and M.B.N.; supervision, M.B.N.; project administration, M.B.N.; funding acquisition, M.B.N., M.d.C.D., S.R. and M.E.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data are contained within the article.
Acknowledgments
We would like to thank the employees of the Virology Laboratory of the Clinical Hospital of the Federal University of Parana, Hospital do Trabalhador, and the Central Laboratory of the State of Parana (LACEN), for their data collection of clinical samples.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Alimi, Y.; Lim, W.; Lansbury, L.; Leonardi-Bee, J.; Nguyen-Van-Tam, J. Systematic review of respiratory viral pathogens identified in adults with community-acquired pneumonia in Europe. J. Clin. Virol. 2017, 95, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, J.; Majumdar, S.R.; Fox, J.D.; Marrie, T.J. Viral infection in adults hospitalized with community-acquired pneumonia. Chest 2008, 134, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Fitzner, J.; Qasmieh, S.; Mounts, A.W.; Alexander, B.; Besselaar, T.; Briand, S.; Brown, C.; Clark, S.; Dueger, E.; Gross, D.; et al. Revision of clinical case definitions: Influenza-like illness and severe acute respiratory infection. Bull. World Health Organ. 2018, 96, 122–128. [Google Scholar] [CrossRef] [PubMed]
- MS—Ministério da Saúde do Brasil. Protocolo de Tratamento de Influenza 2017. Disponível em. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_tratamento_influenza_2017.pdf (accessed on 27 May 2022).
- Przybysz, T.M.; Heffner, A.C. Early Treatment of Severe Acute Respiratory Distress Syndrome. Emerg. Med. Clin. N. Am. 2016, 34, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Prim. 2019, 5, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Pavia, A.T. What is the role of respiratory viruses in community-acquired pneumonia?: What is the best therapy for influenza and other viral causes of community-acquired pneumonia? Infect. Dis. Clin. N. Am. 2013, 27, 157–175. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Hause, A.M.; Avadhanula, V.; Maccato, M.L.; Pinell, P.M.; Bond, N.; Santarcangelo, P.; Ferlic-Stark, L.; Ye, X.; Iwuchukwu, O.; Maurer, L.; et al. Clinical characteristics and outcomes of respiratory syncytial virus infection in pregnant women. Vaccine 2019, 37, 3464–3471. [Google Scholar] [CrossRef]
- Leeper, C.; Lutzkanin, A., 3rd. Infections During Pregnancy. Prim. Care Clin. Off. Pr. 2018, 45, 567–586. [Google Scholar] [CrossRef]
- Badell, M.L.; Dude, C.M.; Rasmussen, S.A.; Jamieson, D. COVID-19 vaccination in pregnancy. BMJ 2022, 378, e069741. [Google Scholar] [CrossRef]
- Silverman, N.S.; Beigi, R. Influenza Vaccination During Pregnancy (Retracted article. See vol. 131, pg. 751, 2018). Obstet. Gynecol. 2018, 131, E109–E114. [Google Scholar] [CrossRef]
- Mendoza-Sassi, R.A.; Cesar, J.A.; Cagol, J.M.; Duarte, I.A.; Friedrich, L.M.; Santos, V.K.; Zhang, L. 2010 A(H1N1) vaccination in pregnant women in Brazil: Identifying coverage and associated factors. Cad Saude Publica 2015, 31, 1247–1256. [Google Scholar] [CrossRef]
- Raboni, S.M.; Moura, F.E.; Caetano, B.C.; Avanzi, V.M.; A Pereira, L.; Nogueira, M.B.; Vidal, L.R.; Tavares, I.C.; Pradel, F.K.; Picot, V.S.; et al. Global Influenza Hospital-based Surveillance Network (GIHSN): Results of surveillance of influenza and other respiratory viruses in hospitalised patients in Brazil, 2015. BMJ Open 2018, 8, e017603. [Google Scholar] [CrossRef]
- Falavina, L.P.; Lentsck, M.H.; Mathias, T.A.d.F. Trend and spatial distribution of infectious diseases in pregnant women in the state of Paraná-Brazil. Rev. Latino-Am. Enferm. 2019, 27, e3160. [Google Scholar] [CrossRef]
- Borges, M.A.S.B.; Florentino, P.T.V.; Cerqueira-Silva, T.; de Carvalho, L.F.; Oliveira, V.d.A.; Aguilar, G.M.O.; Prado, R.d.S.; Soranz, D.; Werneck, G.L.; Pescarini, J.M.; et al. Factors associated with COVID-19 vaccination among pregnant women in Rio De Janeiro City, Brazil. Sci. Rep. 2023, 13, 1–9. [Google Scholar] [CrossRef]
- Sebghati, M.; Khalil, A. Uptake of vaccination in pregnancy. Best Pr. Res. Clin. Obstet. Gynaecol. 2021, 76, 53–65. [Google Scholar] [CrossRef]
- WHO—World Health Organization. Global Influenza Strategy 2019–2030; WHO: Geneva, Switzerland, 2019; Available online: http://apps.who.int/iris (accessed on 17 May 2024).
- Jarvis, J.; Dorey, R.; Warricker, F.; Alwan, N.; Jones, C. The effectiveness of influenza vaccination in pregnancy in relation to child health outcomes: Systematic review and meta-analysis. Vaccine 2020, 38, 1601–1613. [Google Scholar] [CrossRef]
- WHO—World Health Organization. Influenza (Seasonal). CDC Protocol of Realtime RTPCR for Influenza A (H1N1) Characterization of Swine Influenza (Version 2009); General Comments Control; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- WHO—World Health Organization. Influenza (Seasonal), 4th ed.; WHO Information for the Molecular Detection of Influenza Viruses; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Creanga, A.A.; Johnson, T.F.; Graitcer, S.B.; Hartman, L.K.; Al-Samarrai, T.; Schwarz, A.G.; Chu, S.Y.P.; Sackoff, J.E.; Jamieson, D.J.; Fine, A.D.; et al. Severity of 2009 pandemic influenza A (H1N1) virus infection in pregnant women. Obstet. Gynecol. 2010, 115, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Pfitscher, L.C.; Brazilian Network for Surveillance of Severe Maternal Morbidity Group; Cecatti, J.G.; Pacagnella, R.C.; Haddad, S.M.; Parpinelli, M.A.; Souza, J.P.; Quintana, S.M.; Surita, F.G.; Sousa, M.H.; et al. Severe maternal morbidity due to respiratory disease and impact of 2009 H1N1 influenza A pandemic in Brazil: Results from a national multicenter cross-sectional study. BMC Infect. Dis. 2016, 16, 220. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.A.; Ranieri, T.M.S.; Torres, F.D.; Vianna, F.S.L.; Paniz, G.R.; Sanseverino, P.B.; Picon, P.D.; de Azevedo, P.B.; Costa, M.H.; Schuler-Faccini, L.; et al. Impact on pregnancies in South Brazil from the influenza A (H1N1) pandemic: Cohort study. PLoS ONE 2014, 9, e88624. [Google Scholar] [CrossRef]
- Bastos, L.S.; Niquini, R.P.; Lana, R.M.; Villela, D.A.M.; Cruz, O.G.; Coelho, F.C.; Gomes, M.F.C. COVID-19 anda hospitalizations for SARI in Brazil: A comparison up to the 12th epidemiological week of 2020. Cad. Saude Publica 2020, 36, e00070120. [Google Scholar] [CrossRef]
- Niquini, R.P.; Lana, R.M.; Pacheco, A.G.; Cruz, O.G.; Coelho, F.C.; Carvalho, L.M.; Villela, D.A.M.; Gomes, M.F.d.C.; Bastos, L.S. Description and comparison of demographic characteristics and comorbidities in SARI from COVID-19, SARI from influenza, and the Brazilian general population. Cad. Saude Publica 2020, 36, e00149420. [Google Scholar] [CrossRef]
- Leal, L.F.; Merckx, J.; Fell, D.B.; Kuchenbecker, R.; Miranda, A.E.; de Oliveira, W.K.; Platt, R.W.; Antunes, L.; Silveira, M.F.; Barbieri, N.B. Characteristics and outcomes of pregnant women with SARS-CoV-2 infection and other severe acute respiratory infections (SARI) in Brazil from January to November 2020. Braz. J. Infect. Dis. 2021, 25, 101620. [Google Scholar] [CrossRef]
- Li, Y.; Reeves, R.M.; Wang, X.; Bassat, Q.; Brooks, W.A.; Cohen, C.; Moore, D.P.; Nunes, M.; Rath, B.; Campbell, H.; et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis. Lancet Glob. Health 2019, 7, e1031–e1045. [Google Scholar] [CrossRef]
- Paño-Pardo, J.R.; Martínez-Sánchez, N.; Martín-Quirós, A.; Romero-Gómez, M.P.; Muñoz-Muñiz, M.; Sánchez-Pastor, M.; Ruiz, G.; San-José, B.; Prados, M.C.; Mora-Rillo, M.; et al. Influenza-like illness in pregnant women during summertime: Clinical, epidemiological and microbiological features. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 1497–1502. [Google Scholar] [CrossRef]
- Azziz-Baumgartner, E.; Veguilla, V.; Calvo, A.; Franco, D.; Dominguez, R.; Rauda, R.; Armero, J.; Hall, A.J.; Pascale, J.M.; González, R. Incidence of influenza and other respiratory viruses among pregnant women: A multi-country, multiyear cohort. Int. J. Gynecol. Obstet. 2021, 158, 359–367. [Google Scholar] [CrossRef]
- Irving, S.A.; Ball, S.W.; Booth, S.M.; Regan, A.K.; Naleway, A.L.; Buchan, S.A.; Katz, M.A.; Effler, P.V.; Svenson, L.W.; Kwong, J.C.; et al. A multi-country investigation of influenza vaccine coverage in pregnant individuals, 2010–2016. Vaccine 2021, 39, 7598–7605. [Google Scholar] [CrossRef]
- PAHO—Pan American Health Organization. Evaluación multicéntrica de la efectividad de la vacuna de influenza estacional en América Latina y el Caribe. Rede REVELAC-i. 2018. Available online: https://www.paho.org/es/documentos/evaluacion-multicentrica-efectividad-vacuna-influenza-estacional-america-latina-caribe (accessed on 11 February 2021).
- Macias, A.E.; Precioso, A.R.; Falsey, A.R.; the Global Influenza Initiative. The Global Influenza Initiative recommendations for the vaccination of pregnant women against seasonal influenza. Influ. Other Respir. Viruses 2015, 9, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Yan, W.; Du, M.; Tao, L.; Liu, J. The effect of influenza virus infection on pregnancy outcomes: A systematic review and meta-analysis of cohort studies. Int. J. Infect. Dis. 2021, 105, 567–578. [Google Scholar] [CrossRef] [PubMed]
- MS—Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Protocolo de tratamento de Influenza: 2017 Brasília. 2018. Available online: http://bvsms.saude.gov.br/publicacoes/protocolo_tratamento_influenza_2017 (accessed on 11 February 2021).
- Kumari, R.; Sharma, S.D.; Kumar, A.; Ende, Z.; Mishina, M.; Wang, Y.; Falls, Z.; Samudrala, R.; Pohl, J.; Knight, P.R.; et al. Antiviral Approaches against Influenza Virus. Clin. Microbiol. Rev. 2023, 36, e0004022. [Google Scholar] [CrossRef]
- Jamieson, D.J.; A Honein, M.; A Rasmussen, S.; Williams, J.L.; Swerdlow, D.L.; Biggerstaff, M.S.; Lindstrom, S.; Louie, J.K.; Christ, C.M.; Bohm, S.R.; et al. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet 2009, 374, 451–458. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.-P.; Science, M.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; et al. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef]
- Mertz, D.; Lo, C.K.; Lytvyn, L.; Ortiz, J.R.; Loeb, M.; FLURISK-INVESTIGATORS. Pregnancy as a risk factor for severe influenza infection: An individual participant data meta-analysis. BMC Infect. Dis. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- van Riel, D.; Mittrücker, H.-W.; Engels, G.; Klingel, K.; Markert, U.R.; Gabriel, G. Influenza pathogenicity during pregnancy in women and animal models. Semin. Immunopathol. 2016, 38, 719–726. [Google Scholar] [CrossRef]
- Littauer, E.Q.; Esser, E.S.; Antao, O.Q.; Vassilieva, E.V.; Compans, R.W.; Skountzou, I. H1N1 influenza virus infection results in adverse pregnancy outcomes by disrupting tissue-specific hormonal regulation. PLoS Pathog. 2017, 13, e1006757. [Google Scholar] [CrossRef]
- Dawood, F.S.; Garg, S.; Fink, R.V.; Russell, M.L.; Regan, A.K.; A Katz, M.; Booth, S.; Chung, H.; Klein, N.P.; Kwong, J.C.; et al. Epidemiology and Clinical Outcomes of Hospitalizations for Acute Respiratory or Febrile Illness and Laboratory-Confirmed Influenza among Pregnant Women during Six Influenza Seasons, 2010–2016. J. Infect. Dis. 2019, 221, 1703–1712. [Google Scholar] [CrossRef]
- Bansal, A.; Trieu, M.-C.; Mohn, K.G.I.; Cox, R.J. Safety, Immunogenicity, Efficacy and Effectiveness of Inactivated Influenza Vaccines in Healthy Pregnant Women and Children Under 5 Years: An Evidence-Based Clinical Review. Front. Immunol. 2021, 12, 744774. [Google Scholar] [CrossRef]
- Ortiz, J.R.; Perut, M.; Dumolard, L.; Wijesinghe, P.R.; Jorgensen, P.; Ropero, A.M.; Danovaro-Holliday, M.C.; Heffelfinger, J.D.; Tevi-Benissan, C.; Teleb, N.A.; et al. A global review of national influenza immunization policies: Analysis of the 2014 WHO/UNICEF Joint Reporting Form on immunization. Vaccine 2016, 34, 5400–5405. [Google Scholar] [CrossRef]
- Quach, T.H.T.; Mallis, N.A.; Cordero, J.F. Influenza Vaccine Efficacy and Effectiveness in Pregnant Women: Systematic Review and Meta-analysis. Matern. Child Health J. 2020, 24, 229–240. [Google Scholar] [CrossRef]
- Louie, J.K.; Acosta, M.; Jamieson, D.J.; Honein, M.A. Severe 2009 H1N1 influenza in pregnant and postpartum women in California. N. Engl. J. Med. 2010, 362, 27–35. [Google Scholar] [CrossRef]
- Chow, E.J.; Beigi, R.H.; E Riley, L.; Uyeki, T.M. Clinical Effectiveness and Safety of Antivirals for Influenza in Pregnancy. Open Forum Infect. Dis. 2021, 8, ofab138. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).