
Investigation of Mutations in the crt-o and mdr1 Genes of Plasmodium vivax for the Molecular Surveillance of Chloroquine Resistance in Parasites from Gold Mining Areas in Roraima, Brazil

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2022; World Health Organization: Geneva, Switzerland, 2023; ISBN 978-92-4-008617-3. [Google Scholar]
- Brazil. Ministry of Health. Data for Citizens from the Sivep-Malaria, Sinan and E-SUS-VS Data Sources, for Notifications in Brazil from 2007 to 2023. Available online: https://public.tableau.com/app/profile/mal.ria.brasil/viz/Dadosparacidado_201925_03_2020/Incio (accessed on 10 November 2023).
- Eliminate Malaria Brazil: National Malaria Elimination Plan; Brazil, Ministry of Health, Health Surveillance Secretariat, Department of Immunization and Communicable Diseases: Brasília, Brazil, 2022; 60p.
- Adams, J.H.; Mouller, I. The Biology of Plasmodium vivax. In Malaria: Biology in the Era of Eradication; Cold Spring Harbor: New York, NY, USA, 2017; pp. 43–54. [Google Scholar]
- Commons, R.; Thriemer, K.; Humphreys, G.; Suay, I.; Sibley, C.; Guerin, P.; Price, R.N. The Vivax Surveyor: Online mapping database for Plasmodium vivax clinical trials. International Journal for parasitology. Drugs Drug Resist. 2017, 7, 181–190. [Google Scholar]
- Negreiros, S.; Farias, S.; Viana, G.M.R.; Okoth, S.A.; Chenet, S.M.; de Souza, T.M.H.; Marchesini, P.; Udhayakumar, V.; Povoa, M.M.; e Silva Santelli, A.C.F.; et al. Efficacy of Chloroquine and Primaquine for the Treatment of Uncomplicated Plasmodium vivax Malaria in Cruzeiro do Sul, Brazil. Am. J. Trop. Med. Hyg. 2016, 95, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Rieckmann, K.H.; Davis, D.R.; Hutton, D.C. Plasmodium vivax resistance to chloroquine? Lancet 1989, 18, 1183–1184. [Google Scholar] [CrossRef] [PubMed]
- Price, R.N.; von Seidlein, L.; Valecha, N.; Nosten, F.; Baird, J.K.; White, N.J. Global extent of chloroquine-resistant Plasmodium vivax: A systematic review and meta- analysis. Lancet Infect. Dis. 2014, 14, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Phyo, A.P.; Lwin, K.M.; Price, R.N.; Ashley, E.A.; Russell, B.; Sriprawat, K.; Lindegardh, N.; Singhasivanon, P.; White, N.J.; Nosten, F. Dihydroartemisinin-Piperaquine versus chloroquine in the treatment of Plasmodium vivax malaria in Thailand: A randomized controlled trial. Clin. Infect. Dis. 2011, 53, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Leang, R.; Barrette, A.; Bouth, D.M.; Menard, D.; Abdur, R.; Duong, S.; Ringwald, P. Efficacy of dihydroartemisinin-piperaquine for the treatment of uncomplicated Plasmodium falciparum and Plasmodium vivax in Cambodia, 2008 to 2010. Antimicrob. Agents Chemother. 2013, 57, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Teklehaimanot, A.; Bergqvist, Y.; Ringwald, P. Confirmed vivax resistance to chloroquine and effectiveness of artemether-lumefantrine for the treatment of vivax malaria in Ethiopia. Am. J. Trop. Med. Hyg. 2011, 84, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Ketema, T.; Getahun, K.; Bacha, K. Therapeutic efficacy of chloroquine for treatment of Plasmodium vivax malaria cases in Halaba district, South Ethiopia. Parasites Vectors 2011, 4, 46. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.J.; Keystone, J.S.; Kain, K.C. Failure of combined chloroquine and high-dose primaquine therapy for Plasmodium vivax malaria acquired in Guyana, South America. Clin. Infect. Dis. 1996, 23, 1171–1173. [Google Scholar] [CrossRef]
- Alecrim, M.G.; Alecrim, W.; Macêdo, V. Plasmodium vivax resistance to chloroquine (R2) and mefloquine (R3) in Brazilian Amazon region. Rev. Soc. Bras. Med. Trop. 1999, 32, 67–68. [Google Scholar] [CrossRef] [PubMed]
- de Santana Filho, F.S.; de Lima Arcanjo, A.R.; Chehuan, Y.M.; Costa, M.R.; Martinez-Espinosa, F.E.; Vieira, J.L.; das Graças Vale Barbosa, M.; Alecrim, W.D.; das Graças Costa Alecrim, M. Chloroquine-resistant Plasmodium vivax, Brazilian Amazon. Emerg. Infect. Dis. 2007, 13, 1125–1126. [Google Scholar] [CrossRef] [PubMed]
- Marques, M.M.; Costa, M.R.F.; Filho, F.S.S.; Vieira, J.L.F.; Nascimento, M.T.S.; Brasil, L.W.; Nogueira, F.; Silveira, H.; Reyes-Lecca, R.C.; Monteiro, W.M.; et al. Plasmodium vivax chloroquine resistance and anemia in the western Brazilian Amazon. Antimicrob. Agents Chemother. 2014, 58, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Gomes, L.R.; Lavigne, A.; Brasil, P.; Peterka, C.L.; Ménard, D.; Daniel-Ribeiro, C.T.; Ferreira-da-Cruz, M.F. Lack of quadruple and quintuple mutant alleles associated with sulfadoxine-pyrimethamine resistance in Plasmodium vivax isolates from Brazilian endemic areas. Mem. Inst. Oswaldo Cruz 2019, 114, e180425. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.U.; de Sousa, T.N.; Rangel, G.W.; Johansen, I.C.; Corder, R.M.; Ladeia-Andrade, S.; Gil, J.P. Monitoring Plasmodium vivax resistance to antimalarials: Persisting challenges and future directions. International journal for parasitology. Drugs Drug Resist. 2021, 15, 9–24. [Google Scholar]
- Ibrahim, A.; Manko, E.; Dombrowski, J.G.; Campos, M.; Benavente, E.D.; Nolder, D.; Sutherland, C.J.; Nosten, F.; Fernandez, D.; Vélez-Tobón, G.; et al. Population-based genomic study of Plasmodium vivax malaria in seven Brazilian states and across South America. Lancet Reg. Health Am. 2023, 18, 100420. [Google Scholar] [CrossRef] [PubMed]
- Sánches, P.O. Genetic Diversity in Plasmodium vivax Populations: Analysis of Neutral Genetic Markers and Genes Potentially Associated with Drug Resistance. Ph.D. Thesis, University of São Paulo, São Paulo, Brazil, 2010. [Google Scholar]
- Huang, F.; Li, S.; Tian, P.; Pu, L.J.S.; Cui, Y.; Liu, H.; Yang, L.; Bi, D.Y. Genetic polymorphisms in genes associated with drug resistance in Plasmodium vivax parasites from northeastern Myanmar. Malar. J. 2022, 21, 66. [Google Scholar] [CrossRef] [PubMed]
- Buyon, L.E.; Elsworth, B.; Duraisingh, M.T. The molecular basis of antimalarial drug resistance in Plasmodium vivax. Int. J. Parasitol. Drugs Drug Resist. 2021, 1, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Mharakurwa, S.; Ndiaye, D.; Rathod, P.K.; Rosenthal, P.J. Antimalarial Drug Resistance: Literature Review and Activities and Findings of the ICEMR Network. Am. J. Trop. Med. Hyg. 2015, 93, 57–68. [Google Scholar] [CrossRef]
- Veiga, M.I.; Dhingra, S.K.; Henrich, P.P.; Straimer, J.; Gnädig, N.; Uhlemann, A.-C.; Martin, R.E.; Lehane, A.M.; Fidock, D.A. Globally prevalent PfMDR1 mutations modulate Plasmodium falciparum susceptibility to artemisinin-based combination therapies. Nat. Commun. 2016, 7, 11553. [Google Scholar] [CrossRef] [PubMed]
- Melo, G.C.; Monteiro, W.M.; Siqueira, A.M.; Silva, S.R.; Magalhães, B.M.; Alencar, A.C.; Kuehn, A.; del Portillo, H.A.; Fernandez-Becerra, C.; Lacerda, M.V. Expression levels of pvcrt-o and pvmdr-1 are associated with chloroquine resistance and severe Plasmodium vivax malaria in patients of the Brazilian Amazon. PLoS ONE 2014, 9, e105922. [Google Scholar] [CrossRef] [PubMed]
- Stanley, P.; Rajkumari, N.; Sivaradjy, M. Molecular detection of antimalarial resistance in Plasmodium vivax isolates from a tertiary care setting in Puducherry. Indian J. Med. Microbiol. 2024, 47, 100496. [Google Scholar] [CrossRef] [PubMed]
- Tantiamornkul, K.; Pumpaibool, T.; Piriyapongsa, J.; Culleton, R.; Lek-Uthai, U. The prevalence of molecular markers of drug resistance in Plasmodium vivax from the border regions of Thailand in 2008 and 2014. Int. J. Parasitol. Drugs Drug Resist. 2018, 8, 229–237. [Google Scholar] [CrossRef] [PubMed]
- De-Aguiar-Barros, J.; Granja, F.; Pequeno, P.; Marchesini, P.; Ferreira da Cruz, M.F. Gold miners increase malaria transmission in indigenous territories of Roraima state, Brazil. Malar. J. 2022, 21, 358. [Google Scholar] [CrossRef]
- Baird, J.K. Neglect of Plasmodium vivax malaria. Trends Parasitol. 2007, 23, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Brazil, Ministry of Health, Health Surveillance Secretariat. Guide to Malaria Treatment in Brazil, 2nd ed.; Department of Immunization and Communicable Diseases: Brasília, Brazil, 2020; 75p. [Google Scholar]
- Ministry of Health, Health Surveillance Secretariat. Malaria. In Guia de Vigilância em Saúde; Ministry of Health, Health Surveillance Secretariat: Brasília, Brazil, 2023; pp. 921–953. [Google Scholar]
- Simões, L.R.; Alves, E.R., Jr.; Ribatski-Silva, D.; Gomes, L.T.; Nery, A.F.; Fontes, C.J. Factors associated with recurrent Plasmodium vivax malaria in Porto Velho, Rondônia State, Brazil, 2009. Cad. Saude Publica 2014, 30, 1403–1417. [Google Scholar] [CrossRef] [PubMed]
- Brega, S.; Meslin, B.; de Monbrison, F.; Severini, C.; Gradoni, L.; Udomsangpetch, R.; Sutanto, I.; Peyron, F.; Picot, S. Identification of the Plasmodium vivax Mdr-like Gene (Pvmdr1) and Analysis of Single-Nucleotide Polymorphisms among Isolates from Different Areas of Endemicity. J. Infect. Dis. 2005, 191, 272–277. [Google Scholar] [CrossRef] [PubMed]
- MapBiomas Project—Collection 7.0 of the 2021 Annual Series of Land Use and Coverage Maps of Brazil. Available online: https://brasil.mapbiomas.org/colecoes-mapbiomas/ (accessed on 1 September 2023).
- IBGE—Brazilian Institute of Geography and Statistics. Vectors of geopolitical limits, of Indigenous Lands. Available online: https://www.ibge.gov.br/geociencias/downloads-geociencias.html (accessed on 1 September 2023).
- Barros, J.A.; Granja, F.; Silva, D.S.; Citó, A.C.; Peterka, C.; Ferreira-da-Cruz, M.F. A snapshot of a representative Brazilian state of illegal mining in indigenous areas during the era of malaria elimination. Cad. Saude Publica 2024, 40, e00224023. [Google Scholar] [CrossRef] [PubMed]
- Nyunt, M.H.; Han, J.-H.; Wang, B.; Aye, K.M.; Aye, K.H.; Lee, S.-K.; Htut, Y.; Kyaw, M.P.; Han, K.T.; Han, E.-T. Clinical and molecular surveillance of drug resistant vivax malaria in Myanmar (2009–2016). Malar. J. 2017, 16, 117. [Google Scholar] [CrossRef] [PubMed]
- de Abreu-Fernandes, R.; Almeida-de-Oliveira, N.K.; de Lavigne Mello, A.R.; de Queiroz, L.T.; de Aguiar Barros, J.; de Oliveira Baptista, B.; Oliveira-Ferreira, J.; de Souza, R.M.; Pratt-Riccio, L.R.; Brasil, P.; et al. Are pvcrt-o and pvmdr1 Gene Mutations Associated with Plasmodium vivax Chloroquine-Resistant Parasites? Biomedicines 2024, 12, 141. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.R.; Almeida, A.C.G.; da Silva, G.A.V.; Ramasawmy, R.; Lopes, S.C.P.; Siqueira, A.M.; Costa, G.L.; Sousa, T.N.; Vieira, J.L.F.; Lacerda, M.V.G.; et al. Chloroquine resistance is associated to multi-copy pvcrt-o gene in Plasmodium vivax malaria in the Brazilian Amazon. Malar. J. 2018, 17, 267. [Google Scholar] [CrossRef] [PubMed]
- Musset, L.; Heugas, C.; Naldjinan, R.; Blanchet, D.; Houze, P.; Abboud, P.; Volney, B.; Walter, G.; Lazrek, Y.; Epelboin, L.; et al. Emergence of Plasmodium vivax resistance to chloroquine in French Guiana. Antimicrob. Agents Chemother. 2019, 63, 02116–021118. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wang, L.; Soe, M.T.; Aung, P.L.; Wei, H.; Liu, Z.; Ma, T.; Huang, Y.; Menezes, L.J.; Wang, Q.; et al. Molecular surveillance for drug resistance markers in Plasmodium vivax isolates from symptomatic and asymptomatic infections at the China–Myanmar border. Malar. J. 2020, 19, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rungsihirunrat, K.; Muhamad, P.; Chaijaroenkul, W.; Kuesap, J.; Na-Bangchang, K. Plasmodium vivax drug resistance genes; Pvmdr1 and Pvcrt-o polymorphisms in relation to chloroquine sensitivity from a malaria endemic area of Thailand. Korean J. Parasitol. 2015, 53, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.D.S.M.; Vieira, J.L.F.; Machado, R.L.D.; Nacher, M.; Stefani, A.; Musset, L.; Legrand, E.; Menezes, R.A.O.; Júnior, A.A.P.; Sousa, A.P.M.; et al. Efficacy in the treatment of malaria by Plasmodium vivax in Oiapoque, Brazil, on the border with French Guiana: The importance of control over external factors. Malar. J. 2015, 14, 402. [Google Scholar] [CrossRef] [PubMed]
- Faway, E.; Musset, L.; Pelleau, S.; Volney, B.; Casteras, J.; Caro, V.; Menard, D.; Briolant, S.; Legrand, E. Plasmodium vivax multidrug resistance-1 gene polymorphism in French Guiana. Malar. J. 2016, 15, 540. [Google Scholar] [CrossRef] [PubMed]
- Orjuela-Sánchez, P.; de Santana Filho, F.S.; Machado-Lima, A.; Chehuan, Y.F.; Costa, M.R.F.; das Graças Costa Alecrim, M.; del Portillo Grac, H.A. Analysis of single-nucleotide polymorphisms in the crt-o and mdr1 genes of Plasmodium vivax among chloroquine-resistant isolates from the Brazilian Amazon region. Antimicrob. Agents Chemother. 2009, 53, 3561–3564. [Google Scholar] [CrossRef] [PubMed]
- Schousboe, M.L.; Ranjitkar, S.; Rajakaruna, R.S.; Amerasinghe, P.H.; Morales, F.; Pearce, R.; Ord, R.; Leslie, T.; Rowland, M.; Gadalla, N.B.; et al. Multiple Origins of Mutations in the mdr1 Gene--A Putative Marker of Chloroquine Resistance in P. vivax. PLoS Negl. Trop. Dis. 2015, 9, e0004196. [Google Scholar] [CrossRef] [PubMed]
- Spotin, A.; Mahami-Oskouei, M.; Ahmadpour, E.; Parsaei, M.; Rostami, A.; Emami, S.; Gholipour, S.; Farmani, M. Global assessment of genetic paradigms of Pvmdr1 mutations in chloroquine-resistant Plasmodium vivax isolates. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Nomura, T.; Carlton, J.M.; Baird, J.K.; del Portillo, H.A.; Fryauff, D.J.; Rathore, D.; Fidock, D.A.; Su, X.; Collins, W.E.; McCutchan, T.F.; et al. Evidence for Different Mechanisms of Chloroquine Resistance in 2 Plasmodium Species That Cause Human Malaria. J. Infect. Dis. 2001, 183, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Escalante, A.A.; Cepeda, A.S.; Pacheco, M.A. Why are Plasmodium vivax and Plasmodium falciparum so different? A tale of two clades and their species diversities. Malar. J. 2022, 21, 139. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.A.; Escalante, A.A. Fitness components and natural selection: Why are there different patterns on the emergence of drug resistance in Plasmodium falciparum and Plasmodium vivax? Malar. J. 2013, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Murta, F.L.G.; Marques, L.L.G.; Santos, A.P.C.; Batista, T.S.B.; Mendes, M.O.; Silva, E.D.; Neto, A.V.S.; Fabiano, M.; Rodovalho, S.R.; Monteiro, W.M.; et al. Perceptions about malaria among Brazilian gold miners in an Amazonian border area: Perspectives for malaria elimination strategies. Malar. J. 2021, 20, 286. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, W.M. DHA-PQP vs. Chloroquine and Primaquine for Radical Cure of Vivax Malaria in Brazil (CuraVivax). ID NCT03208907. Available online: https://clinicaltrials.gov/ (accessed on 7 August 2024).
- Lacerda, M.V.; Llanos-Cuentas, A.; Krudsood, S.; Lon, C.; Saunders, D.L.; Mohammed, R.; Yilma, D.; Pereira, D.B.; Espino, F.E.; Mia, R.Z.; et al. Single-dose tafenoquine to prevent relapse of Plasmodium vivax malaria. N. Engl. J. Med. 2019, 380, 215–228. [Google Scholar] [CrossRef]
- Brazil. Ministry of Health. Health Surveillance Secretariat. Malaria Day in the Americas—An overview of malaria in Brazil in 2022 and the first half of 2023, Brasília. Epidemiol. Bull. 2024, 55, 1–12. Available online: www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/edicoes/2024/boletim-epidemiologico-volume-55-no-01/ (accessed on 7 August 2024).
- Pukrittayakamee, S.; Imwong, M.; Looareesuwan, S.; White, N.J. Therapeutic responses to antimalarial and antibacterial drugs in vivax malaria. Acta Trop. 2004, 89, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Bray, P.G.; Martin, R.E.; Tilley, L.; Ward, S.A.; Kirk, K.; Fidock, D.A. Defining the role of PfCRT in Plasmodium falciparum chloroquine resistance. Mol. Microbiol. 2005, 56, 323–333. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Probable Site of Infection | Illegal Mining | Agriculture | Hunting/Fishing | Tourism | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
| Alto Alegre | 120 | 76.4 | 1 | 20 | 1 | 100 | 0 | 0 | 122 | 74.4 |
| Amajari | 1 | 0.6 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0.6 |
| Cantá | 0 | 0.0 | 1 | 20 | 0 | 0 | 0 | 0 | 1 | 0.6 |
| Caroebe | 0 | 0.0 | 1 | 20 | 0 | 0 | 0 | 0 | 1 | 0.6 |
| Mucajaí | 29 | 18.5 | 2 | 40 | 0 | 0 | 1 | 100 | 32 | 19.5 |
| Guyana | 3 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 1.8 |
| Venezuela | 4 | 2.5 | 0 | 0 | 0 | 0 | 0 | 0 | 4 | 2.5 |
| Total | 157 | 100 | 5 | 100 | 1 | 100 | 1 | 100 | 164 | 100 |
| K10 | Agriculture | Illegal Mining | Hunting/ Fishing | Tourism | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | N | % | |
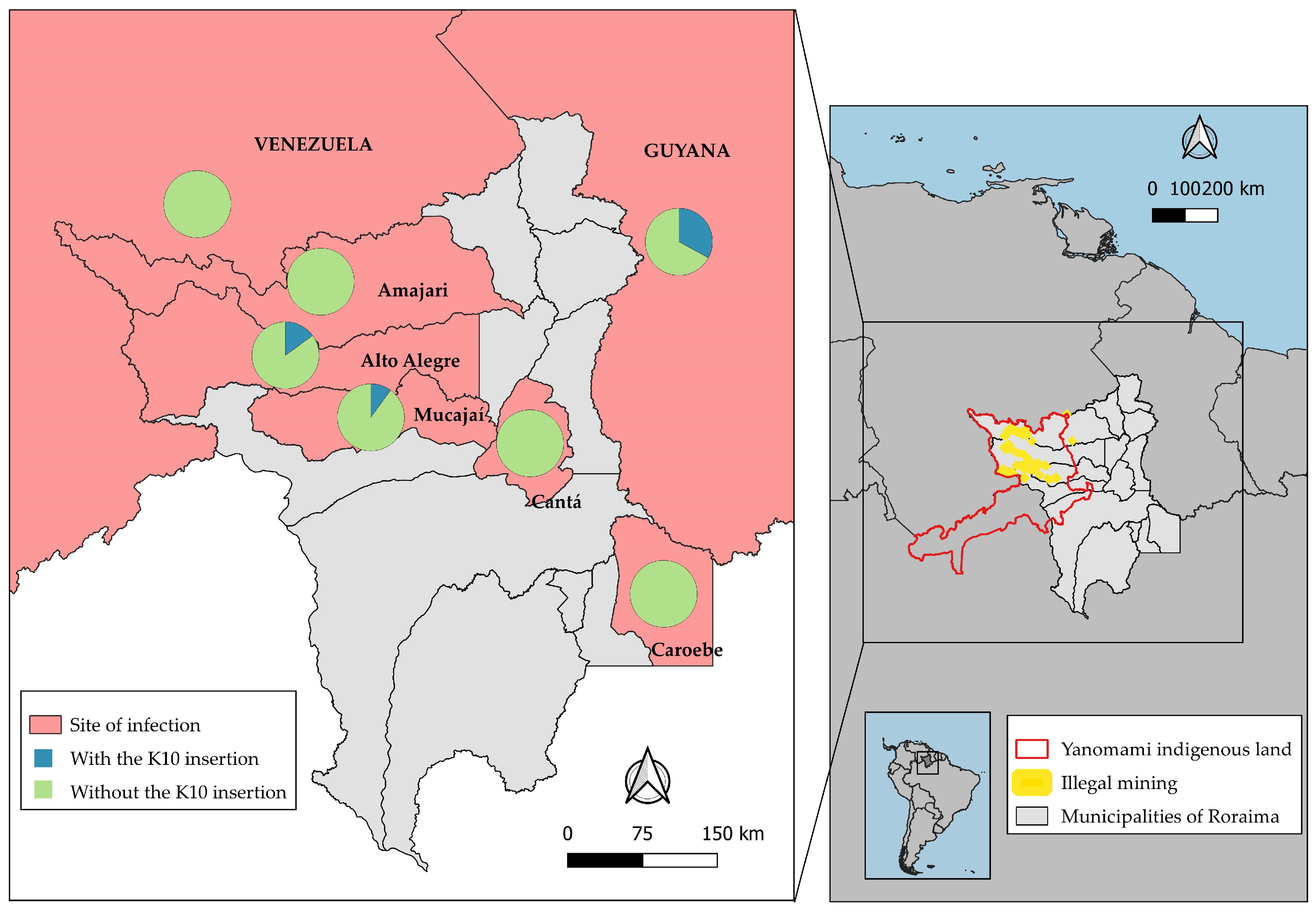
| With | 1 | 25 | 18 | 12.4 | 1 | 100 | 0 | 0 | 20 | 13.2 |
| Without | 3 | 75 | 127 | 87.6 | 0 | 0 | 1 | 100 | 131 | 86.8 |
| Total | 4 | 100 | 145 | 100 | 1 | 100 | 1 | 100 | 151 | 100 |
| Haplotypes | Agriculture | Illegal Mining | Hunting/ Fishing | Total | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | |
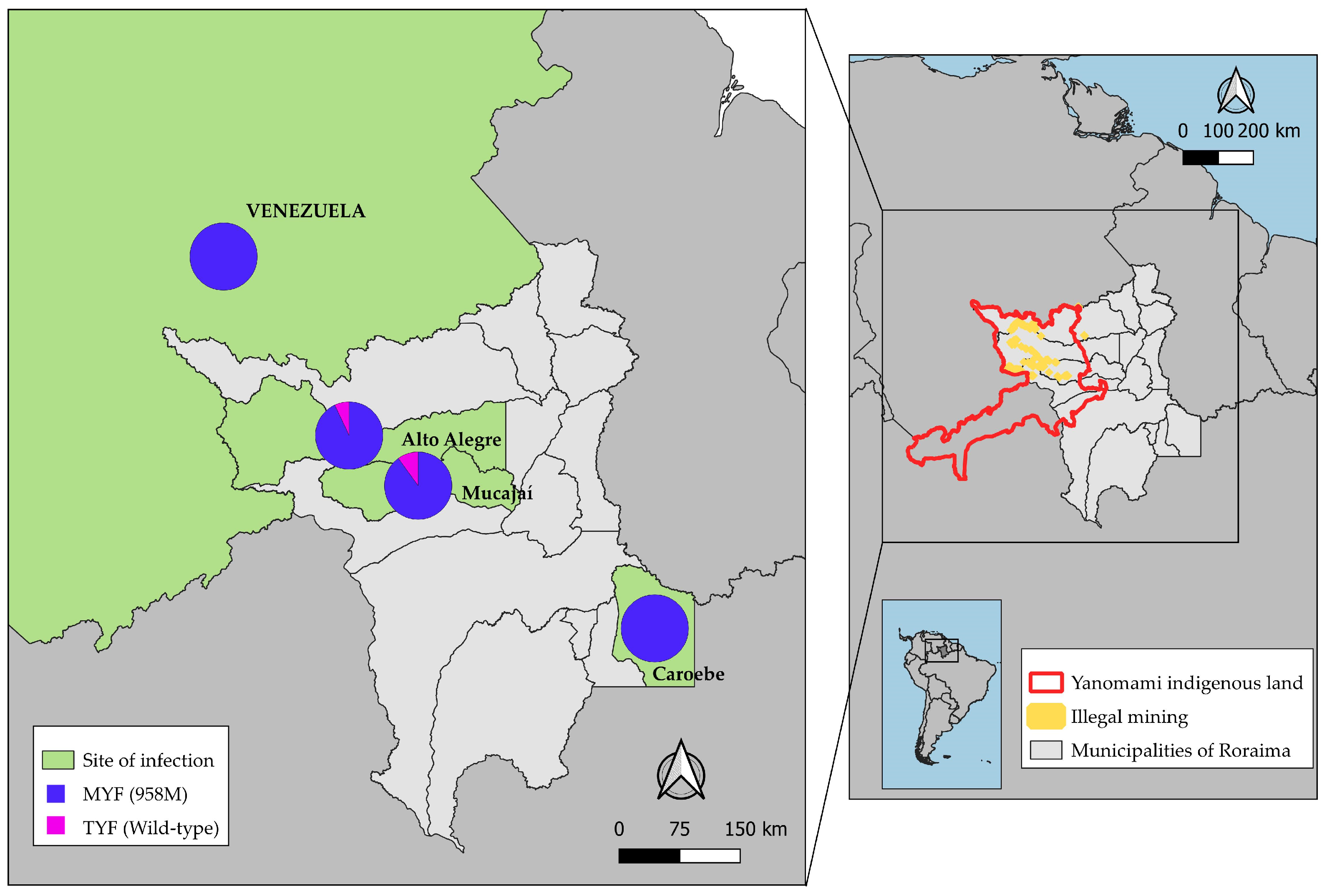
| MYF (958M) | 1 | 100 | 73 | 94 | 0 | 0 | 74 | 92.5 |
| TYF | 0 | 0 | 5 | 6 | 1 | 100 | 6 | 7.5 |
| Total | 1 | 100 | 78 | 100 | 1 | 100 | 80 | 100 |
| Variables | Agriculture (n = 1) | Illegal Mining (n = 18) | Hunting/Fishing (n = 1) | Total (n = 20) | ||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | |
| Sample Collection | 1 | 100 | 9 | 50 | 1 | 100 | 11 | 55 |
| Recrudescence (<28 days) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Probable Relapse (29 to 60 days) | 0 | 0 | 2 | 11 | 0 | 0 | 2 | 10 |
| Probable Reinfection (>60 days) | 0 | 0 | 7 | 39 | 0 | 0 | 7 | 35 |
| Hospitalization | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Death | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Use Antimalarials Prophylaxis | 0 | 0 | 1 | 5.6 | 0 | 0 | 1 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Aguiar Barros, J.; Granja, F.; Abreu-Fernandes, R.d.; de Queiroz, L.T.; e Silva, D.d.S.; Citó, A.C.; Mocelin, N.K.A.-d.-O.; Daniel-Ribeiro, C.T.; Ferreira-da-Cruz, M.d.F. Investigation of Mutations in the crt-o and mdr1 Genes of Plasmodium vivax for the Molecular Surveillance of Chloroquine Resistance in Parasites from Gold Mining Areas in Roraima, Brazil. Microorganisms 2024, 12, 1680. https://doi.org/10.3390/microorganisms12081680
de Aguiar Barros J, Granja F, Abreu-Fernandes Rd, de Queiroz LT, e Silva DdS, Citó AC, Mocelin NKA-d-O, Daniel-Ribeiro CT, Ferreira-da-Cruz MdF. Investigation of Mutations in the crt-o and mdr1 Genes of Plasmodium vivax for the Molecular Surveillance of Chloroquine Resistance in Parasites from Gold Mining Areas in Roraima, Brazil. Microorganisms. 2024; 12(8):1680. https://doi.org/10.3390/microorganisms12081680
Chicago/Turabian Stylede Aguiar Barros, Jacqueline, Fabiana Granja, Rebecca de Abreu-Fernandes, Lucas Tavares de Queiroz, Daniel da Silva e Silva, Arthur Camurça Citó, Natália Ketrin Almeida-de-Oliveira Mocelin, Cláudio Tadeu Daniel-Ribeiro, and Maria de Fátima Ferreira-da-Cruz. 2024. "Investigation of Mutations in the crt-o and mdr1 Genes of Plasmodium vivax for the Molecular Surveillance of Chloroquine Resistance in Parasites from Gold Mining Areas in Roraima, Brazil" Microorganisms 12, no. 8: 1680. https://doi.org/10.3390/microorganisms12081680