
Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
3.1. Demographics and Baseline Characteristics
3.2. Community- and Hospital-Acquired Infections
3.3. Positive Blood Cultures
3.4. Clinical Outcomes
4. Discussion
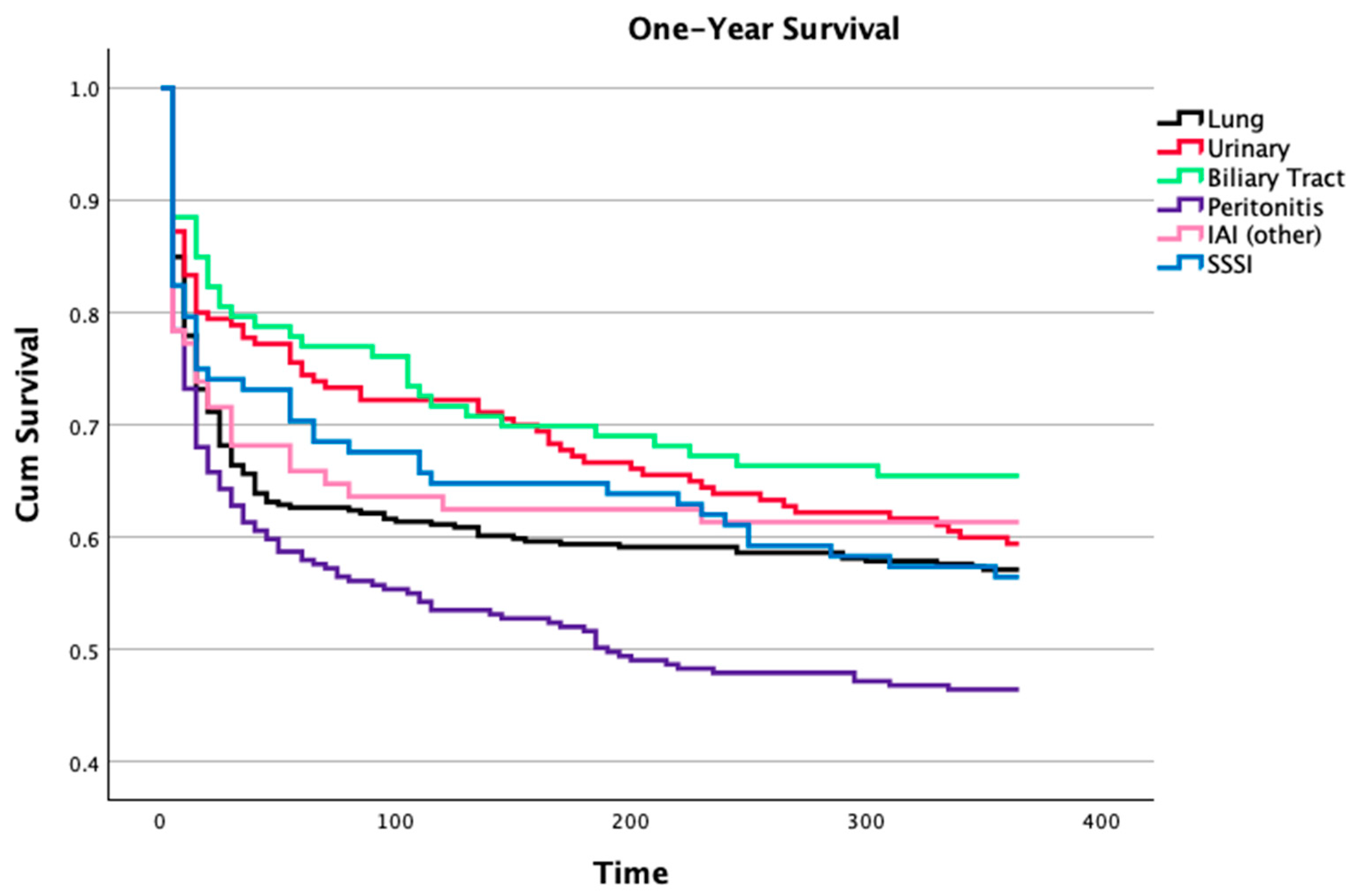
4.1. Infection Foci
4.2. Community and Hospital-Acquired Infections
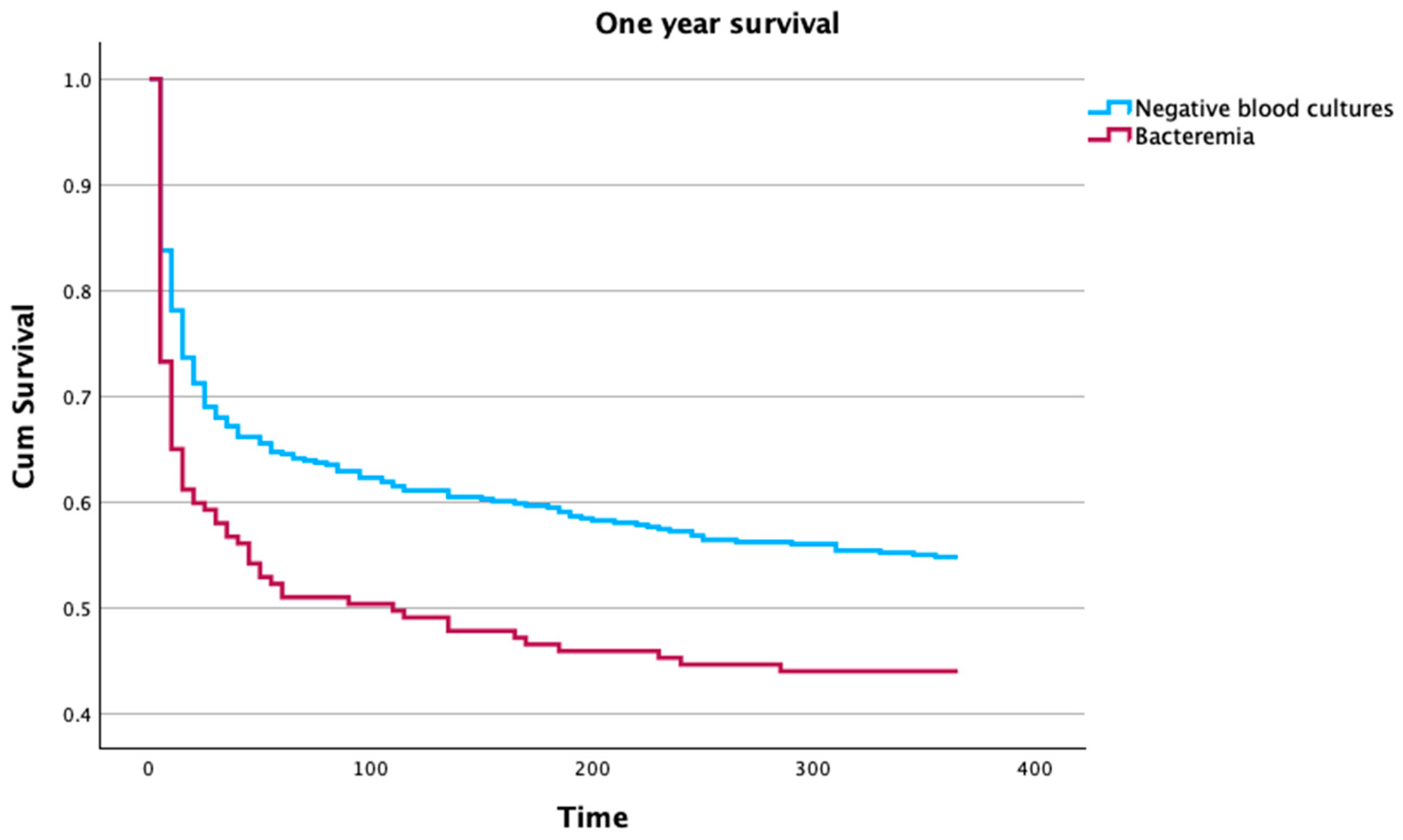
4.3. Bacteremia
4.4. Septic Shock
4.5. Mortality
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Pereira, J.M.; Ribeiro, O.; Baptista, J.P.; Froes, F.; Paiva, J.-A. Impact of Infection on Admission and of the Process of Care on Mortality of Patients Admitted to the Intensive Care Unit: The INFAUCI Study. Clin. Microbiol. Infect. 2014, 20, 1308–1315. [Google Scholar] [CrossRef]
- Almansa, R.; Wain, J.; Tamayo, E.; Andaluz-Ojeda, D.; Martin-Loeches, I.; Ramirez, P.; Bermejo-Martin, J.F. Immunological Monitoring to Prevent and Treat Sepsis. Crit. Care 2013, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit Care Med. 2018, 46, 997–1000. [Google Scholar] [CrossRef]
- Vincent, J.L.; Jones, G.; David, S.; Olariu, E.; Cadwell, K.K. Frequency and Mortality of Septic Shock in Europe and North America: A Systematic Review and Meta-Analysis. Crit. Care 2019, 23, 196. [Google Scholar] [CrossRef]
- Vincent, J.L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; MacHado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef]
- Stortz, J.A.; Cox, M.C.; Hawkins, R.B.; Ghita, G.L.; Brumback, B.A.; Mohr, A.M.; Moldawer, L.L.; Efron, P.A.; Brakenridge, S.C.; Moore, F.A. Phenotypic Heterogeneity by Site of Infection in Surgical Sepsis: A Prospective Longitudinal Study. Crit. Care 2020, 24, 203. [Google Scholar] [CrossRef]
- Schertz, A.R.; Eisner, A.E.; Smith, S.A.; Lenoir, K.M.; Thomas, K.W. Clinical Phenotypes of Sepsis in a Cohort of Hospitalized Patients According to Infection Site. Crit. Care Explor. 2023, 5, e0955. [Google Scholar] [CrossRef] [PubMed]
- Bin Ghaffar, W.; Nazir, S.; Siddiqui, S.; Abdul Ghaffar, M.B.; Khan, M.F.; Latif, A.; Cheema, Z.; Hanif, S.; Sohaib, M. Association Between the Site of Infection and Mortality Analysis in Critically Ill Surgical Patients. Cureus 2023, 15, e50033. [Google Scholar] [CrossRef]
- Moreira, S.B.; Baptista, J.P.; Gonçalves-Pereira, J.; Pereira, J.M.; Ribeiro, O.; Dias, C.C.; Froes, F.; Paiva, J.A. Impact of Age in Critically Ill Infected Patients: A Post-Hoc Analysis of the INFAUCI Study. Eur. Geriatr. Med. 2021, 12, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Mewes, C.; Runzheimer, J.; Böhnke, C.; Büttner, B.; Nemeth, M.; Hinz, J.; Quintel, M.; Mansur, A. Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients. Biomedicines 2023, 11, 2233. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, J.; Povoa, P.R.; Lobo, C.; Carneiro, A.H. Bloodstream Infections as a Marker of Community-Acquired Sepsis Severity. Results from the Portuguese Community-Acquired Sepsis Study (SACiUCI Study). Clin. Microbiol. Infect. 2013, 19, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Rodrigues, A.R.; Oliveira, A.; Vieira, T.; Assis, R.; Lume, C.; Gonçalves-Pereira, J.; Fernandes, S.M. A Prolonged Intensive Care Unit Stay Defines a Worse Long-Term Prognosis–Insights from the Critically Ill Mortality by Age (Cimba) Study. Aust. Crit. Care 2024, 37, 734–739. [Google Scholar] [CrossRef]
- Motzkus, C.A.; Luckmann, R. Does Infection Site Matter? A Systematic Review of Infection Site Mortality in Sepsis. J. Intensive Care Med. 2017, 32, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Dhasmana, N.; Dubey, N.; Kumar, N.; Gangwal, A.; Gupta, M.; Singh, Y. Bacterial Virulence Factors: Secreted for Survival. Indian J. Microbiol. 2017, 57, 1–10. [Google Scholar] [CrossRef]
- Minasyan, H. Sepsis: Mechanisms of Bacterial Injury to the Patient. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 19. [Google Scholar] [CrossRef]
- Burgos, J.; Luján, M.; Larrosa, M.N.; Fontanals, D.; Bermudo, G.; Planes, A.M.; Puig, M.; Rello, J.; Falco, V.; Pahissa, A. Risk Factors for Respiratory Failure in Pneumococcal Pneumonia: The Importance of Pneumococcal Serotypes. Eur. Respir. J. 2014, 43, 545–553. [Google Scholar] [CrossRef]
- Caraballo, C.; Jaimes, F. Organ Dysfunction in Sepsis: An Ominous Trajectory From Infection To Death. Yale J. Biol. Med. 2019, 92, 629–640. [Google Scholar]
- Soni, J.; Sinha, S.; Pandey, R. Understanding Bacterial Pathogenicity: A Closer Look at the Journey of Harmful Microbes. Front. Microbiol. 2024, 15, 1370818. [Google Scholar] [CrossRef]
- De Waele, J.; Lipman, J.; Sakr, Y.; Marshall, J.C.; Vanhems, P.; Barrera Groba, C.; Leone, M.; Vincent, J.L. Abdominal Infections in the Intensive Care Unit: Characteristics, Treatment and Determinants of Outcome. BMC Infect. Dis. 2014, 14, 420. [Google Scholar] [CrossRef] [PubMed]
- Mačiulienė, A.; Maleckas, A.; Kriščiukaitis, A.; Mačiulis, V.; Vencius, J.; Macas, A. Predictors of 30-Day in-Hospital Mortality in Patients Undergoing Urgent Abdominal Surgery Due to Acute Peritonitis Complicated with Sepsis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 6331–6340. [Google Scholar] [CrossRef]
- Diaz-Tang, G.; Marin Meneses, E.; Patel, K.; Mirkin, S.; García-Diéguez, L.; Pajon, C.; Barraza, I.; Patel, V.; Ghali, H.; Tracey, A.P.; et al. Growth Productivity as a Determinant of the Inoculum Effect for Bactericidal Antibiotics. Sci. Adv. 2022, 8, eadd0924. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Harrison, D.A.; Rubenfeld, G.D.; Rowan, K. Epidemiology of Sepsis and Septic Shock in Critical Care Units: Comparison between Sepsis-2 and Sepsis-3 Populations Using a National Critical Care Database. Br. J. Anaesth. 2017, 119, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Azuhata, T.; Kinoshita, K.; Kawano, D.; Komatsu, T.; Sakurai, A.; Chiba, Y.; Tanjho, K. Time from Admission to Initiation of Surgery for Source Control Is a Critical Determinant of Survival in Patients with Gastrointestinal Perforation with Associated Septic Shock. Crit. Care 2014, 18, R87. [Google Scholar] [CrossRef] [PubMed]
- Reitz, K.M.; Kennedy, J.; Li, S.R.; Handzel, R.; Tonetti, D.A.; Neal, M.D.; Zuckerbraun, B.S.; Hall, D.E.; Sperry, J.L.; Angus, D.C.; et al. Association between Time to Source Control in Sepsis and 90-Day Mortality. JAMA Surg. 2022, 157, 817–826. [Google Scholar] [CrossRef]
- Kumar, A.; Haery, C.; Paladugu, B.; Kumar, A.; Symeoneides, S.; Taiberg, L.; Osman, J.; Trenholme, G.; Opal, S.M.; Goldfarb, R.; et al. The Duration of Hypotension before the Initiation of Antibiotic Treatment Is a Critical Determinant of Survival in a Murine Model of Escherichia Coli Septic Shock: Association with Serum Lactate and Inflammatory Cytokine Levels. J. Infect. Dis. 2006, 193, 251–258. [Google Scholar] [CrossRef]
- Abe, T.; Tokuda, Y.; Shiraishi, A.; Fujishima, S.; Mayumi, T.; Sugiyama, T.; Deshpande, G.A.; Shiino, Y.; Hifumi, T.; Otomo, Y.; et al. In-Hospital Mortality Associated with the Misdiagnosis or Unidentified Site of Infection at Admission. Crit. Care 2019, 23, 202. [Google Scholar] [CrossRef]
- Pereira, J.M.; Gonçalves-Pereira, J.; Ribeiro, O.; Baptista, J.P.; Froes, F.; Paiva, J.A. Impact of Antibiotic Therapy in Severe Community-Acquired Pneumonia: Data from the Infauci Study. J. Crit. Care 2018, 43, 183–189. [Google Scholar] [CrossRef]
- Otero, M.L.; Menezes, R.C.; Ferreira, I.B.B.; Issa, F.L.; Agareno, G.; Carmo, T.A.; Arriaga, M.B.; Fukutani, K.F.; Neto, L.P.; Agareno, S.; et al. Factors Associated with Mortality in Critically Ill Patients Diagnosed with Hospital Acquired Infections. Infect. Drug Resist. 2020, 13, 2811–2817. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream Infections in Critically Ill Patients: An Expert Statement. Intensive Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef]
- Abe, T.; Ogura, H.; Kushimoto, S.; Shiraishi, A.; Sugiyama, T.; Deshpande, G.A.; Uchida, M.; Nagata, I.; Saitoh, D.; Fujishima, S.; et al. Variations in Infection Sites and Mortality Rates among Patients in Intensive Care Units with Severe Sepsis and Septic Shock in Japan. J. Intensive Care 2019, 7, 28. [Google Scholar] [CrossRef]
- Yang, L.; Lin, Y.; Wang, J.; Song, J.; Wei, B.; Zhang, X.; Yang, J.; Liu, B. Comparison of Clinical Characteristics and Outcomes between Positive and Negative Blood Culture Septic Patients: A Retrospective Cohort Study. Infect. Drug Resist. 2021, 14, 4191–4205. [Google Scholar] [CrossRef]
- Corona, A.; Bertolini, G.; Lipman, J.; Wilson, A.P.; Singer, M. Antibiotic Use and Impact on Outcome from Bacteraemic Critical Illness: The Bacteraemia Study in Intensive Care (BASIC). J. Antimicrob. Chemother. 2010, 65, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in Sepsis and Septic Shock in Europe, North America and Australia between 2009 and 2019-Results from a Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef]
- Quenot, J.P.; Binquet, C.; Kara, F.; Martinet, O.; Ganster, F.; Navellou, J.C.; Castelain, V.; Barraud, D.; Cousson, J.; Louis, G.; et al. The Epidemiology of Septic Shock in French Intensive Care Units: The Prospective Multicenter Cohort EPISS Study. Crit. Care 2013, 17, R65. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.-F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin Alfa (Activated) in Adults with Septic Shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.C.; Chen, H.L.; Lin, S.Y.; Chen, T.C.; Lu, P.L. Short Time to Positivity of Blood Culture Predicts Mortality and Septic Shock in Bacteremic Patients: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2022, 22, 142. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, J.; Fernandes, J.; Duarte, A.R.; Fernandes, S.M. β-Lactam Dosing in Critical Patients: A Narrative Review of Optimal Efficacy and the Prevention of Resistance and Toxicity. Antibiotics 2022, 11, 1839. [Google Scholar] [CrossRef]
- Prescott, H.C.; Osterholzer, J.J.; Langa, K.M.; Angus, D.C.; Iwashyna, T.J. Late Mortality after Sepsis: Propensity Matched Cohort Study. BMJ 2016, 353, i2375. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Sakr, Y.; Sprung, C.L.; Ranieri, V.M.; Reinhart, K.; Gerlach, H.; Moreno, R.; Carlet, J.; Le Gall, J.-R.; Payen, D. Sepsis in European Intensive Care Units: Results of the SOAP Study. Crit. Care Med. 2006, 34, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Vieira, T.; Rodrigues, A.; Jorge, N.; Tavares, L.; Costa, L.; Paiva, J.A.; Gonçalves Pereira, J. Critically Ill Patients with High Predicted Mortality: Incidence and Outcome. Med. Intensiv. 2024, 48, 85–91. [Google Scholar] [CrossRef]
- Pieroni, M.; Olier, I.; Ortega-Martorell, S.; Johnston, B.W.; Welters, I.D. In-Hospital Mortality of Sepsis Differs Depending on the Origin of Infection: An Investigation of Predisposing Factors. Front. Med. 2022, 9, 915224. [Google Scholar] [CrossRef] [PubMed]
- Klastrup, V.; Hvass, A.M.; Mackenhauer, J.; Fuursted, K.; Schønheyder, H.C.; Kirkegaard, H. Site of Infection and Mortality in Patients with Severe Sepsis or Septic Shock. A Cohort Study of Patients Admitted to a Danish General Intensive Care Unit. Infect. Dis. 2016, 48, 726–731. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lung (N = 400) | Urinary (N = 182) | Biliary Tract Infection (N = 115) | Peritonitis (N = 270) | Other IAI (N = 88) | Endocarditis (N = 21) | SSSI (N = 108) | CNS (N = 28) | Other (N = 84) | Total (N = 1296) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Male sex | 66.5% | 50% | 52.2% | 58.1% | 43.2% | 61.9% | 62% | 50.0% | 59.5% | 58.1% |
| Age (years) * | 66.3 ± 16.3 | 70.1 ± 11.8 | 71.3 ± 14.3 | 67.8 ± 15.4 | 67.0 ± 15.5 | 68.9 ± 15.1 | 66.6 ± 15.1 | 60.5 ± 15.6 | 65.0 ± 14.6 | 67.5 ± 15.3 |
| Comorbidities | ||||||||||
| Dementia | 2.5% | 2.2% | 7.8% | 1.1% | 0.0% | 0.0% | 1.9% | 0.0% | 0.0% | 28 (2.2%) |
| Diabetes | 29.5% | 30.2% | 28.7% | 26.3% | 23.9% | 42.9% | 40.7% | 39.3% | 25.0% | 383 (29.6%) |
| Arterial Hypertension | 40.5% | 47.8% | 57.4% | 44.4% | 53.4% | 47.6% | 39.8% | 42.9% | 32.1% | 574 (44.3%) |
| HF | 18.3% | 15.4% | 9.6% | 8.1% | 13.6% | 23.8% | 22.2% | 7.1% | 10.7% | 186 (14.4%) |
| Obesity | 9% | 14.8% | 13.9% | 13.3% | 12.5% | 4.8% | 13.0% | 7.1% | 7.1% | 149 (11.5%) |
| Cancer | 9.3% | 13.2% | 11.3% | 30% | 13.6% | 4.8% | 5.6% | 0.0% | 9.5% | 182 (14.0%) |
| Hematologic cancer | 4.5% | 3.3% | 1.7% | 3.0% | 5.7% | 4.8% | 9.3% | 3.6% | 8.3% | 58 (4.5%) |
| COPD | 22.5% | 13.2% | 11.3% | 9.3% | 11.4% | 14.3% | 11.1% | 3.6% | 11.1% | 189 (14.6%) |
| CKD | 14.0% | 24.2% | 12.2% | 13.0% | 18.2% | 33.3% | 16.7% | 7.1% | 20.2% | 209 (16.1%) |
| CHD | 4.5% | 2.2% | 7.0% | 7.8% | 3.4% | 0.0% | 4.6% | 0.0% | 4.8% | 63 (4.9%) |
| Community-acquired | 73.0% | 61.0% | 35.7% | 28.9% | 55.7% | 38.1% | 51.9% | 85.7% | 64.3% | 713 (55.0%) |
| Hospital | Community | p | ||
|---|---|---|---|---|
| Focus of Infection | Lung | 108 (27%) | 292 (73%) | <0.001 |
| Urinary | 71 (39%) | 111 (61%) | ||
| Biliary tract | 74 (64.3%) | 41 (35.7%) | ||
| Peritonitis | 192 (71.1%) | 78 (28.9%) | ||
| Other IAI | 39 (44.3%) | 49 (55.7%) | ||
| Endocarditis | 13 (61.9%) | 8 (38.1%) | ||
| SSSI | 52 (48.1%) | 56 (51.9%) | ||
| CNS | 4 (14.3%) | 24 (85.7%) | ||
| Other | 30 (35.7%) | 54 (64.3%) | ||
| Bacteremia | 28.0% | 21.4% | 0.055 | |
| Age | 68.6 ± 15.4 | 66.6 ± 15.1 | 0.018 * | |
| SAPS II | 43.9 ± 19.2 | 44.3 ± 19.5 | 0.46 * | |
| ICU LOS | 5 [3–9] | 5 [3–8] | 0.99 ** | |
| Hospital LOS | 14 [7–32] | 11 [6–22.5] | <0.001 ** | |
| RRT | 21.3% | 23.1% | 0.461 | |
| Vasopressors | 56.3% | 51.8% | 0.117 | |
| IMV | 41.7% | 30.2% | <0.001 | |
| ICU Mortality | 25.9% | 22.2% | 0.117 | |
| Hosp Mortality | 36.4% | 30.3% | 0.024 |
| Bacteremia | Negative Blood Cultures | p | ||
|---|---|---|---|---|
| N | 160 | 495 | ||
| RRT | 28.1% | 24.8% | 0.407 | |
| IMV | 32.5% | 39.2% | 0.134 | |
| Vasopressors | 61.3% | 56.4% | 0.312 | |
| ICU LOS | 5 [3–9] | 5 [3–9] | 0.46 ** | |
| Hospital LOS | 13 [7–24] | 11 [5–25.75] | 0.47 ** | |
| ICU Mortality | 37.5% | 25.9% | 0.006 | |
| Hospital Mortality | 33.9% | 45.0% | 0.014 | |
| 1-Year Mortality | 56.1% | 45.2% | 0.022 | |
| Age | 69.4 ± 13.6 | 68.0 ± 14.2 | 0.263 * | |
| SAPS II | 49.7 ± 19.9 | 45.6 ± 18.1 | 0.028 * | |
| Focus of Infection | <0.001 | |||
| Lung | 17 (7.6%) | |||
| Urinary | 31 (34.8%) | |||
| Biliary tract | 26 (44.8%) | |||
| Peritonitis | 30 (27.0%) | |||
| Other IAI | 12 (29.3%) | |||
| Endocarditis | 6 (40.0%) | |||
| SSSI | 16 (25.8%) | |||
| CNS | 0 (0.0%) | |||
| Other | 22 (47.8%) |
| N | Hospital Mortality | ||
|---|---|---|---|
| Gram positive | 47 | 46.8% | |
| Staphylococcus spp. | 14 | 46.7% | |
| Streptococcus spp | 5 | 41.7% | |
| Enterococcus spp. | 2 | 100% | |
| Other Gram Positive | 1 | 33% | |
| Gram Negative | 99 | 41.4% | |
| Klebsiella spp | 33 | 45.5% | |
| Escherichia spp. | 42 | 35.7% | |
| Proteus spp. | 2 | 50% | |
| Citrobacter spp. | 6 | 50% | |
| Enterobacter spp. | 6 | 66.7% | |
| Serratia spp. | 6 | 50% | |
| Other Gram Negative | 5 | 20% | |
| Non-fermenting Gram-negative | 14 | 60% | |
| Pseudomonas spp. | 14 | 60% |
| Gram Positive | Gram Negative | Non Fermenting Gram Negative | p | ||
|---|---|---|---|---|---|
| N | 47 | 99 | 14 | ||
| Age | 67.9 ± 15.2 | 70.4 ± 13.4 | 68.1 ± 16.5 | 0.547 * | |
| SAPS II | 46.2 ± 20.2 | 51.13 ± 19.7 | 49.9 ± 21.8 | 0.473 * | |
| Focus of Infection | |||||
| Lung | 70.6% | 17.6% | 11.8% | <0.001 | |
| Urinary | 6.5% | 93.5% | 0.0% | ||
| Biliary tract | 3.8% | 96.2% | 0.0% | ||
| Peritonitis | 13.3% | 76.7% | 10% | ||
| Other IAI | 33.3% | 41.7% | 25% | ||
| Endocarditis | 100% | 0.0% | 0.0% | ||
| SSSI | 37.5% | 31.3% | 31.3% | ||
| Other | 54.5% | 36.4% | 9.1% | ||
| RRT | 29.8% | 29.6% | 13.3% | 0.408 | |
| IMV | 31.9% | 32.7% | 33.3% | 0.993 | |
| Vasopressors | 55.3% | 61.2% | 80% | 0.232 | |
| ICU LOS | 6 [3–9] | 5 [3–8] | 4 [1–9] | 0.24 ** | |
| Hospital LOS | 16 [5–31] | 11.5 [5–23.2] | 8 [1–23] | 0.47 ** | |
| ICU Mortality | 36.2% | 36.7% | 46.7% | 0.742 | |
| Hospital Mortality | 46.8% | 41.8% | 60% | 0.402 | |
| 1-Year Mortality | 31.8% | 55.7% | 71.4% | 0.022 |
| Hospital Mortality | Standard Mortality | One-Year Mortality | OR if Septic Shock* | 95% CI | |
|---|---|---|---|---|---|
| Lung | 34.5% | 0.88 | 42.8% | 6.8 | 3.9–11.8 |
| Urinary | 22.5% | 0.53 | 40.1% | 4.8 | 2.2–10.7 |
| Biliary | 20.9% | 0.46 | 33.9% | 2.0 | 0.8–05.1 |
| Peritonitis | 40.4% | 0.90 | 53.3% | 6.4 | 3.7–11.0 |
| Other IAI | 31.8% | 0.66 | 38.6% | 11.3 | 3.1–41.9 |
| Endocarditis | 57.1% | 1.49 | 66.7% | 0.9 | 0.2–05.1 |
| SSSI | 29.6% | 0.74 | 43.5% | 4.4 | 1.8–10.6 |
| CNS | 42.9% | 0.94 | 46.4% | 1.4 | 0.2–11.7 |
| Other | 38.1% | 0.92 | 47.6% | 3.8 | 1.5–09.8 |
| Septic Shock | Sepsis | p | |
|---|---|---|---|
| RRT | 37.7% | 12.9% | <0.001 |
| IMV | 52.1% | 25.1% | <0.001 |
| ICU LOS | 5 [2–10] | 5 [3–8] | 0.741 ** |
| Hospital LOS | 11 [3–25] | 7 [13–26] | <0.001 ** |
| ICU Mortality | 42.0% | 12.8% | <0.001 |
| Hospital Mortality | 51.1% | 22.0% | <0.001 |
| 1-Year Mortality | 60.5% | 35.0% | <0.001 |
| Age | 70.2 ± 14.1 | 65.9 ± 21.3 | <0.001 * |
| SAPS II | 51.8 ± 16.6 | 39.5 ± 16.6 | <0.001 * |
| Bacteremia | 35.6% | 16.6% | <0.001 |
| Community-acquired infection | 34.1% | 65.9% | 0.002 |
| Hospital-acquired infection | 42.5% | 57.5% |
| OR | 95% CI | p | |
|---|---|---|---|
| SAPS II | 1.03 | 1.02–1.04 | p < 0.001 |
| Age | 1.03 | 1.02–1.04 | p < 0.001 |
| Chronic hypertension | 0.56 | 0.42–0.73 | p < 0.001 |
| Solid neoplasia | 1.76 | 1.20–2.56 | p = 0.004 |
| Hematological neoplasia | 1.83 | 1.00–3.33 | p = 0.049 |
| Chronic kidney disease | 1.63 | 1.15–2.30 | p = 0.006 |
| Chronic hepatic disease | 2.63 | 1.50–4.62 | p < 0.001 |
| Community-acquired infection | 0.72 | 0.54–0.97 | p = 0.029 |
| Infection focus * | p < 0.001 | ||
| Lung | 0.93 | 0.54–1.60 | p = 0.792 |
| Urinary tract | 0.41 | 0.22–0.76 | p = 0.005 |
| Biliary tract | 0.33 | 0.16–0.67 | p = 0.002 |
| Peritonitis | 0.80 | 0.45–1.43 | p = 0.450 |
| Other Intra-abdominal | 0.63 | 0.31–1.31 | p = 0.217 |
| Endocarditis | 2.64 | 0.90–7.72 | p = 0.076 |
| Skin and Skin structures | 0.64 | 0.33–1.26 | p = 0.201 |
| Central nervous system | 1.60 | 0.59–4.35 | p = 0.359 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, A.M.; Oliveira, A.; Vidal, R.; Gonçalves-Pereira, J. Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients. Microorganisms 2024, 12, 1705. https://doi.org/10.3390/microorganisms12081705
Oliveira AM, Oliveira A, Vidal R, Gonçalves-Pereira J. Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients. Microorganisms. 2024; 12(8):1705. https://doi.org/10.3390/microorganisms12081705
Chicago/Turabian StyleOliveira, Ana Maria, André Oliveira, Raquel Vidal, and João Gonçalves-Pereira. 2024. "Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients" Microorganisms 12, no. 8: 1705. https://doi.org/10.3390/microorganisms12081705
APA StyleOliveira, A. M., Oliveira, A., Vidal, R., & Gonçalves-Pereira, J. (2024). Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients. Microorganisms, 12(8), 1705. https://doi.org/10.3390/microorganisms12081705