
Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Statistical Analysis
3. Results
3.1. Demographics and Baseline Characteristics
3.2. Community- and Hospital-Acquired Infections
3.3. Positive Blood Cultures
3.4. Clinical Outcomes
4. Discussion
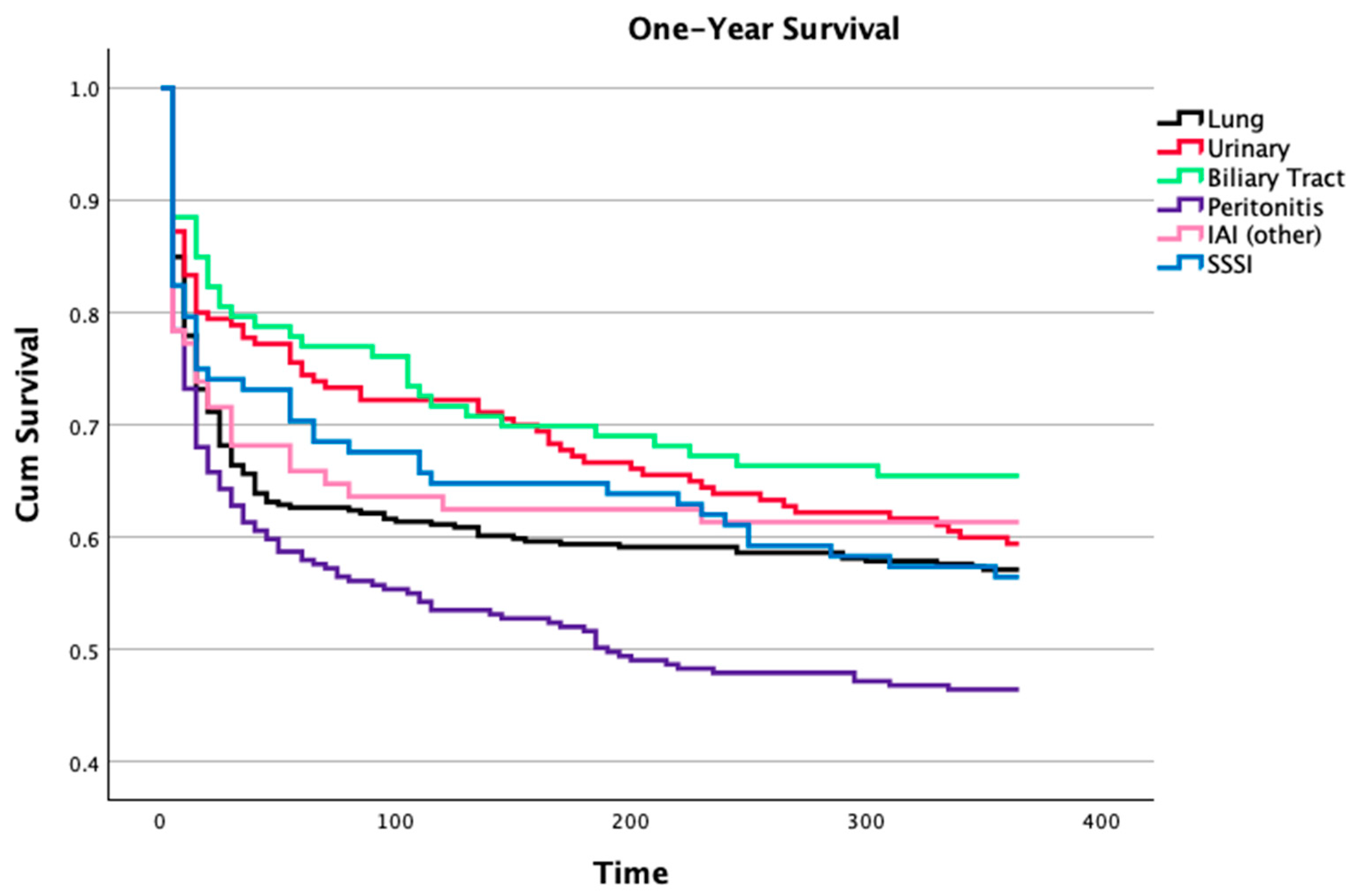
4.1. Infection Foci
4.2. Community and Hospital-Acquired Infections
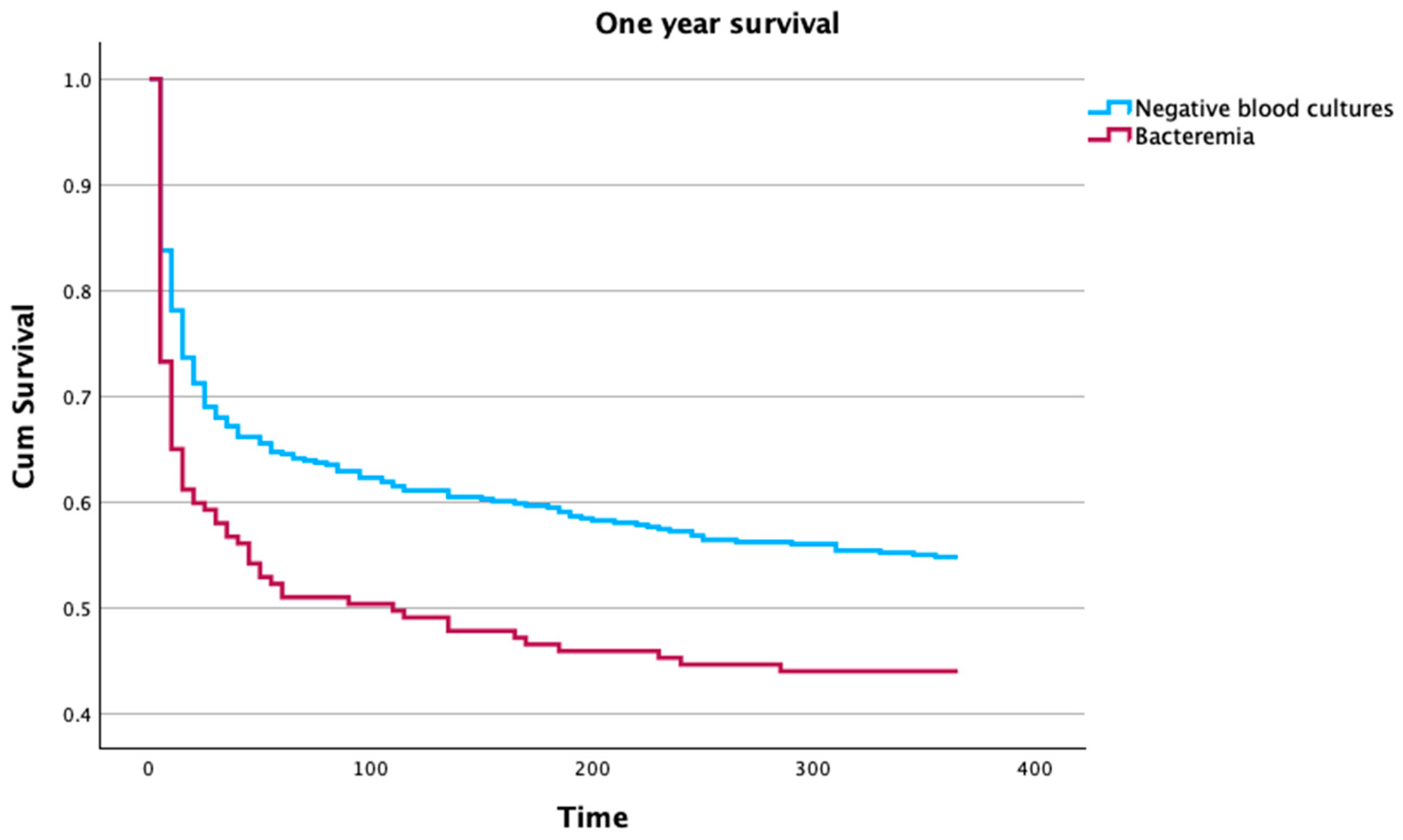
4.3. Bacteremia
4.4. Septic Shock
4.5. Mortality
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Pereira, J.M.; Ribeiro, O.; Baptista, J.P.; Froes, F.; Paiva, J.-A. Impact of Infection on Admission and of the Process of Care on Mortality of Patients Admitted to the Intensive Care Unit: The INFAUCI Study. Clin. Microbiol. Infect. 2014, 20, 1308–1315. [Google Scholar] [CrossRef]
- Almansa, R.; Wain, J.; Tamayo, E.; Andaluz-Ojeda, D.; Martin-Loeches, I.; Ramirez, P.; Bermejo-Martin, J.F. Immunological Monitoring to Prevent and Treat Sepsis. Crit. Care 2013, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit Care Med. 2018, 46, 997–1000. [Google Scholar] [CrossRef]
- Vincent, J.L.; Jones, G.; David, S.; Olariu, E.; Cadwell, K.K. Frequency and Mortality of Septic Shock in Europe and North America: A Systematic Review and Meta-Analysis. Crit. Care 2019, 23, 196. [Google Scholar] [CrossRef]
- Vincent, J.L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; MacHado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478–1487. [Google Scholar] [CrossRef]
- Stortz, J.A.; Cox, M.C.; Hawkins, R.B.; Ghita, G.L.; Brumback, B.A.; Mohr, A.M.; Moldawer, L.L.; Efron, P.A.; Brakenridge, S.C.; Moore, F.A. Phenotypic Heterogeneity by Site of Infection in Surgical Sepsis: A Prospective Longitudinal Study. Crit. Care 2020, 24, 203. [Google Scholar] [CrossRef]
- Schertz, A.R.; Eisner, A.E.; Smith, S.A.; Lenoir, K.M.; Thomas, K.W. Clinical Phenotypes of Sepsis in a Cohort of Hospitalized Patients According to Infection Site. Crit. Care Explor. 2023, 5, e0955. [Google Scholar] [CrossRef] [PubMed]
- Bin Ghaffar, W.; Nazir, S.; Siddiqui, S.; Abdul Ghaffar, M.B.; Khan, M.F.; Latif, A.; Cheema, Z.; Hanif, S.; Sohaib, M. Association Between the Site of Infection and Mortality Analysis in Critically Ill Surgical Patients. Cureus 2023, 15, e50033. [Google Scholar] [CrossRef]
- Moreira, S.B.; Baptista, J.P.; Gonçalves-Pereira, J.; Pereira, J.M.; Ribeiro, O.; Dias, C.C.; Froes, F.; Paiva, J.A. Impact of Age in Critically Ill Infected Patients: A Post-Hoc Analysis of the INFAUCI Study. Eur. Geriatr. Med. 2021, 12, 1057–1064. [Google Scholar] [CrossRef] [PubMed]
- Mewes, C.; Runzheimer, J.; Böhnke, C.; Büttner, B.; Nemeth, M.; Hinz, J.; Quintel, M.; Mansur, A. Differences in Mortality and Sepsis-Associated Organ Dysfunction between Surgical and Non-Surgical Sepsis Patients. Biomedicines 2023, 11, 2233. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, J.; Povoa, P.R.; Lobo, C.; Carneiro, A.H. Bloodstream Infections as a Marker of Community-Acquired Sepsis Severity. Results from the Portuguese Community-Acquired Sepsis Study (SACiUCI Study). Clin. Microbiol. Infect. 2013, 19, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Rodrigues, A.R.; Oliveira, A.; Vieira, T.; Assis, R.; Lume, C.; Gonçalves-Pereira, J.; Fernandes, S.M. A Prolonged Intensive Care Unit Stay Defines a Worse Long-Term Prognosis–Insights from the Critically Ill Mortality by Age (Cimba) Study. Aust. Crit. Care 2024, 37, 734–739. [Google Scholar] [CrossRef]
- Motzkus, C.A.; Luckmann, R. Does Infection Site Matter? A Systematic Review of Infection Site Mortality in Sepsis. J. Intensive Care Med. 2017, 32, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.K.; Dhasmana, N.; Dubey, N.; Kumar, N.; Gangwal, A.; Gupta, M.; Singh, Y. Bacterial Virulence Factors: Secreted for Survival. Indian J. Microbiol. 2017, 57, 1–10. [Google Scholar] [CrossRef]
- Minasyan, H. Sepsis: Mechanisms of Bacterial Injury to the Patient. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 19. [Google Scholar] [CrossRef]
- Burgos, J.; Luján, M.; Larrosa, M.N.; Fontanals, D.; Bermudo, G.; Planes, A.M.; Puig, M.; Rello, J.; Falco, V.; Pahissa, A. Risk Factors for Respiratory Failure in Pneumococcal Pneumonia: The Importance of Pneumococcal Serotypes. Eur. Respir. J. 2014, 43, 545–553. [Google Scholar] [CrossRef]
- Caraballo, C.; Jaimes, F. Organ Dysfunction in Sepsis: An Ominous Trajectory From Infection To Death. Yale J. Biol. Med. 2019, 92, 629–640. [Google Scholar]
- Soni, J.; Sinha, S.; Pandey, R. Understanding Bacterial Pathogenicity: A Closer Look at the Journey of Harmful Microbes. Front. Microbiol. 2024, 15, 1370818. [Google Scholar] [CrossRef]
- De Waele, J.; Lipman, J.; Sakr, Y.; Marshall, J.C.; Vanhems, P.; Barrera Groba, C.; Leone, M.; Vincent, J.L. Abdominal Infections in the Intensive Care Unit: Characteristics, Treatment and Determinants of Outcome. BMC Infect. Dis. 2014, 14, 420. [Google Scholar] [CrossRef] [PubMed]
- Mačiulienė, A.; Maleckas, A.; Kriščiukaitis, A.; Mačiulis, V.; Vencius, J.; Macas, A. Predictors of 30-Day in-Hospital Mortality in Patients Undergoing Urgent Abdominal Surgery Due to Acute Peritonitis Complicated with Sepsis. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 6331–6340. [Google Scholar] [CrossRef]
- Diaz-Tang, G.; Marin Meneses, E.; Patel, K.; Mirkin, S.; García-Diéguez, L.; Pajon, C.; Barraza, I.; Patel, V.; Ghali, H.; Tracey, A.P.; et al. Growth Productivity as a Determinant of the Inoculum Effect for Bactericidal Antibiotics. Sci. Adv. 2022, 8, eadd0924. [Google Scholar] [CrossRef] [PubMed]
- Shankar-Hari, M.; Harrison, D.A.; Rubenfeld, G.D.; Rowan, K. Epidemiology of Sepsis and Septic Shock in Critical Care Units: Comparison between Sepsis-2 and Sepsis-3 Populations Using a National Critical Care Database. Br. J. Anaesth. 2017, 119, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Azuhata, T.; Kinoshita, K.; Kawano, D.; Komatsu, T.; Sakurai, A.; Chiba, Y.; Tanjho, K. Time from Admission to Initiation of Surgery for Source Control Is a Critical Determinant of Survival in Patients with Gastrointestinal Perforation with Associated Septic Shock. Crit. Care 2014, 18, R87. [Google Scholar] [CrossRef] [PubMed]
- Reitz, K.M.; Kennedy, J.; Li, S.R.; Handzel, R.; Tonetti, D.A.; Neal, M.D.; Zuckerbraun, B.S.; Hall, D.E.; Sperry, J.L.; Angus, D.C.; et al. Association between Time to Source Control in Sepsis and 90-Day Mortality. JAMA Surg. 2022, 157, 817–826. [Google Scholar] [CrossRef]
- Kumar, A.; Haery, C.; Paladugu, B.; Kumar, A.; Symeoneides, S.; Taiberg, L.; Osman, J.; Trenholme, G.; Opal, S.M.; Goldfarb, R.; et al. The Duration of Hypotension before the Initiation of Antibiotic Treatment Is a Critical Determinant of Survival in a Murine Model of Escherichia Coli Septic Shock: Association with Serum Lactate and Inflammatory Cytokine Levels. J. Infect. Dis. 2006, 193, 251–258. [Google Scholar] [CrossRef]
- Abe, T.; Tokuda, Y.; Shiraishi, A.; Fujishima, S.; Mayumi, T.; Sugiyama, T.; Deshpande, G.A.; Shiino, Y.; Hifumi, T.; Otomo, Y.; et al. In-Hospital Mortality Associated with the Misdiagnosis or Unidentified Site of Infection at Admission. Crit. Care 2019, 23, 202. [Google Scholar] [CrossRef]
- Pereira, J.M.; Gonçalves-Pereira, J.; Ribeiro, O.; Baptista, J.P.; Froes, F.; Paiva, J.A. Impact of Antibiotic Therapy in Severe Community-Acquired Pneumonia: Data from the Infauci Study. J. Crit. Care 2018, 43, 183–189. [Google Scholar] [CrossRef]
- Otero, M.L.; Menezes, R.C.; Ferreira, I.B.B.; Issa, F.L.; Agareno, G.; Carmo, T.A.; Arriaga, M.B.; Fukutani, K.F.; Neto, L.P.; Agareno, S.; et al. Factors Associated with Mortality in Critically Ill Patients Diagnosed with Hospital Acquired Infections. Infect. Drug Resist. 2020, 13, 2811–2817. [Google Scholar] [CrossRef] [PubMed]
- Timsit, J.F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream Infections in Critically Ill Patients: An Expert Statement. Intensive Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef]
- Abe, T.; Ogura, H.; Kushimoto, S.; Shiraishi, A.; Sugiyama, T.; Deshpande, G.A.; Uchida, M.; Nagata, I.; Saitoh, D.; Fujishima, S.; et al. Variations in Infection Sites and Mortality Rates among Patients in Intensive Care Units with Severe Sepsis and Septic Shock in Japan. J. Intensive Care 2019, 7, 28. [Google Scholar] [CrossRef]
- Yang, L.; Lin, Y.; Wang, J.; Song, J.; Wei, B.; Zhang, X.; Yang, J.; Liu, B. Comparison of Clinical Characteristics and Outcomes between Positive and Negative Blood Culture Septic Patients: A Retrospective Cohort Study. Infect. Drug Resist. 2021, 14, 4191–4205. [Google Scholar] [CrossRef]
- Corona, A.; Bertolini, G.; Lipman, J.; Wilson, A.P.; Singer, M. Antibiotic Use and Impact on Outcome from Bacteraemic Critical Illness: The Bacteraemia Study in Intensive Care (BASIC). J. Antimicrob. Chemother. 2010, 65, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Gerlach, H.; Vogelmann, T.; Preissing, F.; Stiefel, J.; Adam, D. Mortality in Sepsis and Septic Shock in Europe, North America and Australia between 2009 and 2019-Results from a Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 239. [Google Scholar] [CrossRef]
- Quenot, J.P.; Binquet, C.; Kara, F.; Martinet, O.; Ganster, F.; Navellou, J.C.; Castelain, V.; Barraud, D.; Cousson, J.; Louis, G.; et al. The Epidemiology of Septic Shock in French Intensive Care Units: The Prospective Multicenter Cohort EPISS Study. Crit. Care 2013, 17, R65. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Thompson, B.T.; Barie, P.S.; Dhainaut, J.-F.; Douglas, I.S.; Finfer, S.; Gårdlund, B.; Marshall, J.C.; Rhodes, A.; Artigas, A.; et al. Drotrecogin Alfa (Activated) in Adults with Septic Shock. N. Engl. J. Med. 2012, 366, 2055–2064. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.C.; Chen, H.L.; Lin, S.Y.; Chen, T.C.; Lu, P.L. Short Time to Positivity of Blood Culture Predicts Mortality and Septic Shock in Bacteremic Patients: A Systematic Review and Meta-Analysis. BMC Infect. Dis. 2022, 22, 142. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves-Pereira, J.; Fernandes, J.; Duarte, A.R.; Fernandes, S.M. β-Lactam Dosing in Critical Patients: A Narrative Review of Optimal Efficacy and the Prevention of Resistance and Toxicity. Antibiotics 2022, 11, 1839. [Google Scholar] [CrossRef]
- Prescott, H.C.; Osterholzer, J.J.; Langa, K.M.; Angus, D.C.; Iwashyna, T.J. Late Mortality after Sepsis: Propensity Matched Cohort Study. BMJ 2016, 353, i2375. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Sakr, Y.; Sprung, C.L.; Ranieri, V.M.; Reinhart, K.; Gerlach, H.; Moreno, R.; Carlet, J.; Le Gall, J.-R.; Payen, D. Sepsis in European Intensive Care Units: Results of the SOAP Study. Crit. Care Med. 2006, 34, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Vieira, T.; Rodrigues, A.; Jorge, N.; Tavares, L.; Costa, L.; Paiva, J.A.; Gonçalves Pereira, J. Critically Ill Patients with High Predicted Mortality: Incidence and Outcome. Med. Intensiv. 2024, 48, 85–91. [Google Scholar] [CrossRef]
- Pieroni, M.; Olier, I.; Ortega-Martorell, S.; Johnston, B.W.; Welters, I.D. In-Hospital Mortality of Sepsis Differs Depending on the Origin of Infection: An Investigation of Predisposing Factors. Front. Med. 2022, 9, 915224. [Google Scholar] [CrossRef] [PubMed]
- Klastrup, V.; Hvass, A.M.; Mackenhauer, J.; Fuursted, K.; Schønheyder, H.C.; Kirkegaard, H. Site of Infection and Mortality in Patients with Severe Sepsis or Septic Shock. A Cohort Study of Patients Admitted to a Danish General Intensive Care Unit. Infect. Dis. 2016, 48, 726–731. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lung (N = 400) | Urinary (N = 182) | Biliary Tract Infection (N = 115) | Peritonitis (N = 270) | Other IAI (N = 88) | Endocarditis (N = 21) | SSSI (N = 108) | CNS (N = 28) | Other (N = 84) | Total (N = 1296) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Male sex | 66.5% | 50% | 52.2% | 58.1% | 43.2% | 61.9% | 62% | 50.0% | 59.5% | 58.1% |
| Age (years) * | 66.3 ± 16.3 | 70.1 ± 11.8 | 71.3 ± 14.3 | 67.8 ± 15.4 | 67.0 ± 15.5 | 68.9 ± 15.1 | 66.6 ± 15.1 | 60.5 ± 15.6 | 65.0 ± 14.6 | 67.5 ± 15.3 |
| Comorbidities | ||||||||||
| Dementia | 2.5% | 2.2% | 7.8% | 1.1% | 0.0% | 0.0% | 1.9% | 0.0% | 0.0% | 28 (2.2%) |
| Diabetes | 29.5% | 30.2% | 28.7% | 26.3% | 23.9% | 42.9% | 40.7% | 39.3% | 25.0% | 383 (29.6%) |
| Arterial Hypertension | 40.5% | 47.8% | 57.4% | 44.4% | 53.4% | 47.6% | 39.8% | 42.9% | 32.1% | 574 (44.3%) |
| HF | 18.3% | 15.4% | 9.6% | 8.1% | 13.6% | 23.8% | 22.2% | 7.1% | 10.7% | 186 (14.4%) |
| Obesity | 9% | 14.8% | 13.9% | 13.3% | 12.5% | 4.8% | 13.0% | 7.1% | 7.1% | 149 (11.5%) |
| Cancer | 9.3% | 13.2% | 11.3% | 30% | 13.6% | 4.8% | 5.6% | 0.0% | 9.5% | 182 (14.0%) |
| Hematologic cancer | 4.5% | 3.3% | 1.7% | 3.0% | 5.7% | 4.8% | 9.3% | 3.6% | 8.3% | 58 (4.5%) |
| COPD | 22.5% | 13.2% | 11.3% | 9.3% | 11.4% | 14.3% | 11.1% | 3.6% | 11.1% | 189 (14.6%) |
| CKD | 14.0% | 24.2% | 12.2% | 13.0% | 18.2% | 33.3% | 16.7% | 7.1% | 20.2% | 209 (16.1%) |
| CHD | 4.5% | 2.2% | 7.0% | 7.8% | 3.4% | 0.0% | 4.6% | 0.0% | 4.8% | 63 (4.9%) |
| Community-acquired | 73.0% | 61.0% | 35.7% | 28.9% | 55.7% | 38.1% | 51.9% | 85.7% | 64.3% | 713 (55.0%) |
| Hospital | Community | p | ||
|---|---|---|---|---|
| Focus of Infection | Lung | 108 (27%) | 292 (73%) | <0.001 |
| Urinary | 71 (39%) | 111 (61%) | ||
| Biliary tract | 74 (64.3%) | 41 (35.7%) | ||
| Peritonitis | 192 (71.1%) | 78 (28.9%) | ||
| Other IAI | 39 (44.3%) | 49 (55.7%) | ||
| Endocarditis | 13 (61.9%) | 8 (38.1%) | ||
| SSSI | 52 (48.1%) | 56 (51.9%) | ||
| CNS | 4 (14.3%) | 24 (85.7%) | ||
| Other | 30 (35.7%) | 54 (64.3%) | ||
| Bacteremia | 28.0% | 21.4% | 0.055 | |
| Age | 68.6 ± 15.4 | 66.6 ± 15.1 | 0.018 * | |
| SAPS II | 43.9 ± 19.2 | 44.3 ± 19.5 | 0.46 * | |
| ICU LOS | 5 [3–9] | 5 [3–8] | 0.99 ** | |
| Hospital LOS | 14 [7–32] | 11 [6–22.5] | <0.001 ** | |
| RRT | 21.3% | 23.1% | 0.461 | |
| Vasopressors | 56.3% | 51.8% | 0.117 | |
| IMV | 41.7% | 30.2% | <0.001 | |
| ICU Mortality | 25.9% | 22.2% | 0.117 | |
| Hosp Mortality | 36.4% | 30.3% | 0.024 |
| Bacteremia | Negative Blood Cultures | p | ||
|---|---|---|---|---|
| N | 160 | 495 | ||
| RRT | 28.1% | 24.8% | 0.407 | |
| IMV | 32.5% | 39.2% | 0.134 | |
| Vasopressors | 61.3% | 56.4% | 0.312 | |
| ICU LOS | 5 [3–9] | 5 [3–9] | 0.46 ** | |
| Hospital LOS | 13 [7–24] | 11 [5–25.75] | 0.47 ** | |
| ICU Mortality | 37.5% | 25.9% | 0.006 | |
| Hospital Mortality | 33.9% | 45.0% | 0.014 | |
| 1-Year Mortality | 56.1% | 45.2% | 0.022 | |
| Age | 69.4 ± 13.6 | 68.0 ± 14.2 | 0.263 * | |
| SAPS II | 49.7 ± 19.9 | 45.6 ± 18.1 | 0.028 * | |
| Focus of Infection | <0.001 | |||
| Lung | 17 (7.6%) | |||
| Urinary | 31 (34.8%) | |||
| Biliary tract | 26 (44.8%) | |||
| Peritonitis | 30 (27.0%) | |||
| Other IAI | 12 (29.3%) | |||
| Endocarditis | 6 (40.0%) | |||
| SSSI | 16 (25.8%) | |||
| CNS | 0 (0.0%) | |||
| Other | 22 (47.8%) |
| N | Hospital Mortality | ||
|---|---|---|---|
| Gram positive | 47 | 46.8% | |
| Staphylococcus spp. | 14 | 46.7% | |
| Streptococcus spp | 5 | 41.7% | |
| Enterococcus spp. | 2 | 100% | |
| Other Gram Positive | 1 | 33% | |
| Gram Negative | 99 | 41.4% | |
| Klebsiella spp | 33 | 45.5% | |
| Escherichia spp. | 42 | 35.7% | |
| Proteus spp. | 2 | 50% | |
| Citrobacter spp. | 6 | 50% | |
| Enterobacter spp. | 6 | 66.7% | |
| Serratia spp. | 6 | 50% | |
| Other Gram Negative | 5 | 20% | |
| Non-fermenting Gram-negative | 14 | 60% | |
| Pseudomonas spp. | 14 | 60% |
| Gram Positive | Gram Negative | Non Fermenting Gram Negative | p | ||
|---|---|---|---|---|---|
| N | 47 | 99 | 14 | ||
| Age | 67.9 ± 15.2 | 70.4 ± 13.4 | 68.1 ± 16.5 | 0.547 * | |
| SAPS II | 46.2 ± 20.2 | 51.13 ± 19.7 | 49.9 ± 21.8 | 0.473 * | |
| Focus of Infection | |||||
| Lung | 70.6% | 17.6% | 11.8% | <0.001 | |
| Urinary | 6.5% | 93.5% | 0.0% | ||
| Biliary tract | 3.8% | 96.2% | 0.0% | ||
| Peritonitis | 13.3% | 76.7% | 10% | ||
| Other IAI | 33.3% | 41.7% | 25% | ||
| Endocarditis | 100% | 0.0% | 0.0% | ||
| SSSI | 37.5% | 31.3% | 31.3% | ||
| Other | 54.5% | 36.4% | 9.1% | ||
| RRT | 29.8% | 29.6% | 13.3% | 0.408 | |
| IMV | 31.9% | 32.7% | 33.3% | 0.993 | |
| Vasopressors | 55.3% | 61.2% | 80% | 0.232 | |
| ICU LOS | 6 [3–9] | 5 [3–8] | 4 [1–9] | 0.24 ** | |
| Hospital LOS | 16 [5–31] | 11.5 [5–23.2] | 8 [1–23] | 0.47 ** | |
| ICU Mortality | 36.2% | 36.7% | 46.7% | 0.742 | |
| Hospital Mortality | 46.8% | 41.8% | 60% | 0.402 | |
| 1-Year Mortality | 31.8% | 55.7% | 71.4% | 0.022 |
| Hospital Mortality | Standard Mortality | One-Year Mortality | OR if Septic Shock* | 95% CI | |
|---|---|---|---|---|---|
| Lung | 34.5% | 0.88 | 42.8% | 6.8 | 3.9–11.8 |
| Urinary | 22.5% | 0.53 | 40.1% | 4.8 | 2.2–10.7 |
| Biliary | 20.9% | 0.46 | 33.9% | 2.0 | 0.8–05.1 |
| Peritonitis | 40.4% | 0.90 | 53.3% | 6.4 | 3.7–11.0 |
| Other IAI | 31.8% | 0.66 | 38.6% | 11.3 | 3.1–41.9 |
| Endocarditis | 57.1% | 1.49 | 66.7% | 0.9 | 0.2–05.1 |
| SSSI | 29.6% | 0.74 | 43.5% | 4.4 | 1.8–10.6 |
| CNS | 42.9% | 0.94 | 46.4% | 1.4 | 0.2–11.7 |
| Other | 38.1% | 0.92 | 47.6% | 3.8 | 1.5–09.8 |
| Septic Shock | Sepsis | p | |
|---|---|---|---|
| RRT | 37.7% | 12.9% | <0.001 |
| IMV | 52.1% | 25.1% | <0.001 |
| ICU LOS | 5 [2–10] | 5 [3–8] | 0.741 ** |
| Hospital LOS | 11 [3–25] | 7 [13–26] | <0.001 ** |
| ICU Mortality | 42.0% | 12.8% | <0.001 |
| Hospital Mortality | 51.1% | 22.0% | <0.001 |
| 1-Year Mortality | 60.5% | 35.0% | <0.001 |
| Age | 70.2 ± 14.1 | 65.9 ± 21.3 | <0.001 * |
| SAPS II | 51.8 ± 16.6 | 39.5 ± 16.6 | <0.001 * |
| Bacteremia | 35.6% | 16.6% | <0.001 |
| Community-acquired infection | 34.1% | 65.9% | 0.002 |
| Hospital-acquired infection | 42.5% | 57.5% |
| OR | 95% CI | p | |
|---|---|---|---|
| SAPS II | 1.03 | 1.02–1.04 | p < 0.001 |
| Age | 1.03 | 1.02–1.04 | p < 0.001 |
| Chronic hypertension | 0.56 | 0.42–0.73 | p < 0.001 |
| Solid neoplasia | 1.76 | 1.20–2.56 | p = 0.004 |
| Hematological neoplasia | 1.83 | 1.00–3.33 | p = 0.049 |
| Chronic kidney disease | 1.63 | 1.15–2.30 | p = 0.006 |
| Chronic hepatic disease | 2.63 | 1.50–4.62 | p < 0.001 |
| Community-acquired infection | 0.72 | 0.54–0.97 | p = 0.029 |
| Infection focus * | p < 0.001 | ||
| Lung | 0.93 | 0.54–1.60 | p = 0.792 |
| Urinary tract | 0.41 | 0.22–0.76 | p = 0.005 |
| Biliary tract | 0.33 | 0.16–0.67 | p = 0.002 |
| Peritonitis | 0.80 | 0.45–1.43 | p = 0.450 |
| Other Intra-abdominal | 0.63 | 0.31–1.31 | p = 0.217 |
| Endocarditis | 2.64 | 0.90–7.72 | p = 0.076 |
| Skin and Skin structures | 0.64 | 0.33–1.26 | p = 0.201 |
| Central nervous system | 1.60 | 0.59–4.35 | p = 0.359 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveira, A.M.; Oliveira, A.; Vidal, R.; Gonçalves-Pereira, J. Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients. Microorganisms 2024, 12, 1705. https://doi.org/10.3390/microorganisms12081705
Oliveira AM, Oliveira A, Vidal R, Gonçalves-Pereira J. Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients. Microorganisms. 2024; 12(8):1705. https://doi.org/10.3390/microorganisms12081705
Chicago/Turabian StyleOliveira, Ana Maria, André Oliveira, Raquel Vidal, and João Gonçalves-Pereira. 2024. "Infectious Foci, Comorbidities and Its Influence on the Outcomes of Septic Critically Ill Patients" Microorganisms 12, no. 8: 1705. https://doi.org/10.3390/microorganisms12081705