Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches

 ,
, 
{kind=link}
{kind=link}
Abstract
:1. Introduction
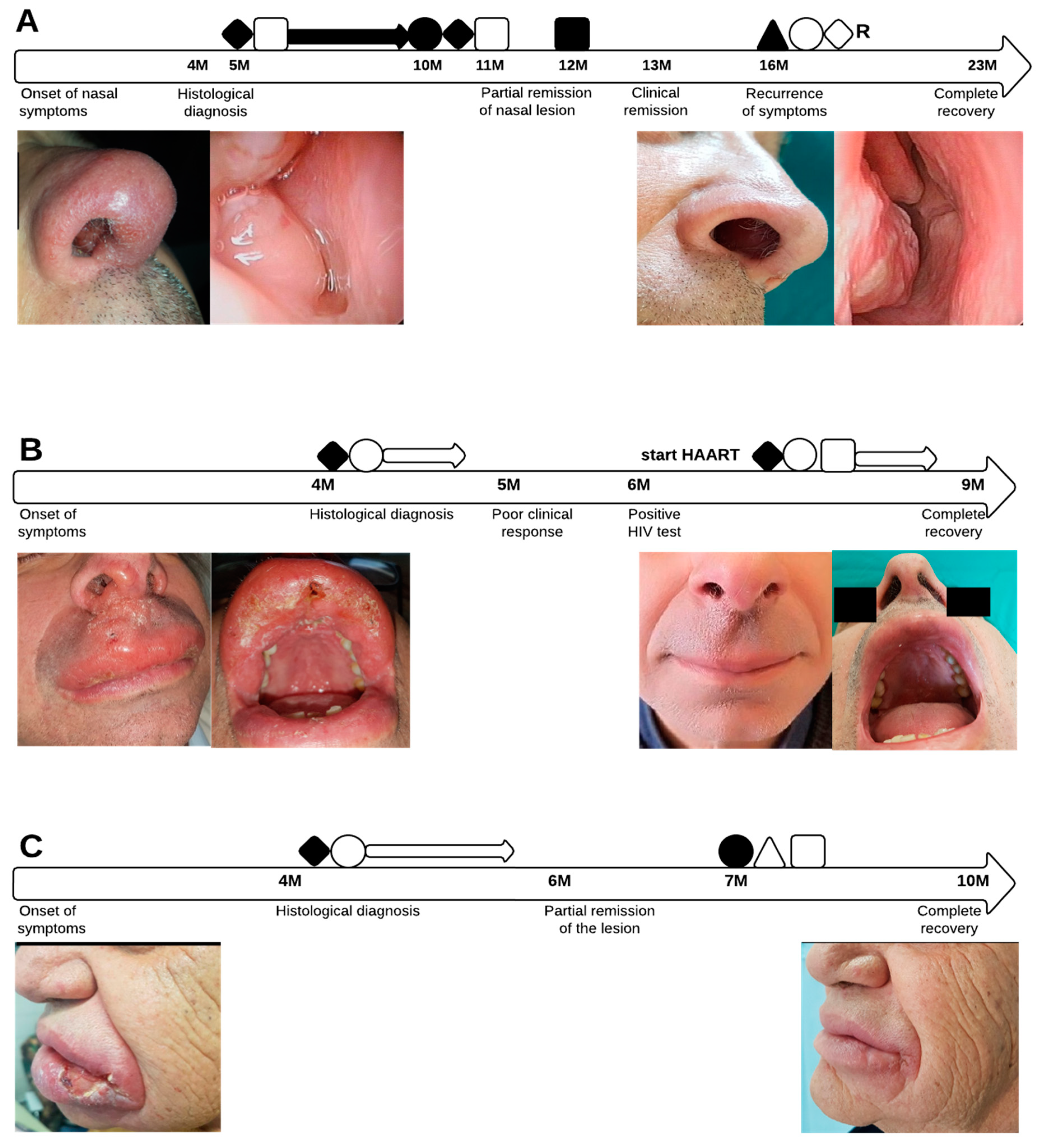
2. Description of Cases
2.1. Case 1
2.2. Case 2
2.3. Case 3
2.4. Ethics
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gradoni, L.; López-Vélez, R.; Mokni, M. Manual on Case Management and Surveillance of the Leishmaniases in the WHO European Region; World Health Organization: Copenhagen, Denmark, 2017. [Google Scholar]
- Faucher, B.; Pomares, C.; Fourcade, S.; Benyamine, A.; Marty, P.; Pratlong, L.; Faraut, F.; Mary, C.; Piarroux, R.; Dedet, J.-P.; et al. Mucosal Leishmania infantum leishmaniasis: Specific pattern in a multicentre survey and historical cases. J. Infect. 2011, 63, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Blum, J.; Buffet, P.; Visser, L.; Harms, G.; Bailey, M.S.; Caumes, E.; Clerinx, J.; van Thiel, P.P.A.M.; Morizot, G.; Hata, C.; et al. LeishMan recommendations for treatment of cutaneous and mucosal leishmaniasis in travelers, 2014. J. Travel. Med. 2014, 21, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Aliaga, L.; Cobo, F.; Mediavilla, J.D.; Bravo, J.; Osuna, A.; Amador, J.M.; Martín-Sánchez, J.; Cordero, E.; Navarro, J.M. Localized mucosal leishmaniasis due to Leishmania (Leishmania) infantum: Clinical and microbiologic findings in 31 patients. Medicine 2003, 82, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Richter, J.; Hanus, I.; Häussinger, D.; Löscher, T.; Harms, G. Mucosal Leishmania infantum infection. Parasitol Res. 2011, 109, 959–962. [Google Scholar] [CrossRef] [PubMed]
- Mignogna, M.D.; Celentano, A.; Leuci, S.; Cascone, M.; Adamo, D.; Ruoppo, E.; Favia, G. Mucosal leishmaniasis with primary oral involvement: A case series and a review of the literature. Oral. Dis. 2015, 21, e70–e78. [Google Scholar] [CrossRef] [PubMed]
- Mosimann, V.; Blazek, C.; Grob, H.; Chaney, M.; Neumayr, A.; Blum, J. Miltefosine for Mucosal and Complicated Cutaneous Old World Leishmaniasis: A Case Series and Review of the Literature. Open Forum. Infect. Dis. 2016, 3, ofw008. [Google Scholar] [CrossRef] [Green Version]
- Bafica, A.; Oliveira, F.; Freitas, L.A.; Nascimento, E.G.; Barral, A. American cutaneous leishmaniasis unresponsive to antimonial drugs: Successful treatment using combination of Nmethilglucamine antimoniate plus pentoxifylline. Int. J. Dermatol. 2003, 42, 203–207. [Google Scholar] [CrossRef]
- Lessa, H.A.; Machado, P.; Lima, F.; Cruz, A.A.; Bacellar, O.; Guerreiro, J.; Carvalho, E.M. Successful treatment of refractory mucosal leishmaniasis with pentoxifylline plus antimony. Am. J. Trop. Med. Hyg. 2001, 65, 87–89. [Google Scholar] [CrossRef]
- Machado, P.R.; Lessa, H.; Lessa, M.; Guimaraes, L.H.; Bang, H.; Ho, J.L.; Carvalho, E.M. Oral pentoxifylline combined with pentavalent antimony: A randomized trial for mucosal leishmaniasis. Clin. Infect. Dis. 2007, 44, 788–793. [Google Scholar] [CrossRef] [Green Version]
- Varani, S.; Cagarelli, R.; Melchionda, F.; Attard, L.; Salvadori, C.; Finarelli, A.C.; Gentilomi, G.A.; Tigani, R.; Rangoni, R.; Todeschini, R.; et al. Ongoing outbreak of visceral leishmaniasis in Bologna Province, Italy, November 2012 to May 2013. Eurosurveillance 2013, 18, 20530. [Google Scholar] [CrossRef] [Green Version]
- Gaspari, V.; Ortalli, M.; Foschini, M.P.; Baldovini, C.; Lanzoni, A.; Cagarelli, R.; Gaibani, P.; Rossini, G.; Vocale, C.; Tigani, R.; et al. New evidence of cutaneous leishmaniasis in north-eastern Italy. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Wortmann, G.; Sweeney, C.; Houng, H.S.; Aronson, N.; Stiteler, J.; Jackson, J.; Ockenhouse, C. Rapid diagnosis of leishmaniasis by fluorogenic polymerase chain reaction. Am. J. Trop. Med. Hyg. 2001, 65, 583–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mary, C.; Faraut, F.; Lascombe, L.; Dumon, H. Quantification of Leishmania infantum DNA by a real-time PCR assay with high sensitivity. J. Clin. Microbiol. 2004, 42, 5249–5255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Tai, N.O.; El Fari, M.; Mauricio, I.; Miles, M.A.; Oskam, L.; El Safi, S.H.; Presber, W.H.; Schonian, G. Leishmania donovani: Intraspecific polymorphisms of Sudanese isolates revealed by PCR-based analyses and DNA sequencing. Exp. Parasitol. 2001, 97, 35–44. [Google Scholar] [CrossRef] [Green Version]
- Rugna, G.; Carra, E.; Corpus, F.; Calzolari, M.; Salvatore, D.; Bellini, R.; Di Francesco, A.; Franceschini, E.; Bruno, A.; Poglayen, G.; et al. Distinct Leishmania infantum Strains Circulate in Humans and Dogs in the Emilia-Romagna Region, Northeastern Italy. Vector Borne Zoonotic Dis. 2017, 17, 409–415. [Google Scholar] [CrossRef]
- Kirigi, G.; Mbuchi, M.W.; Mbui, J.K.; Rashid, J.R.; Kinoti, D.M.; Njoroge, S.N.; Basiye, F.; Magiri, C.; Wasunna, M.K. A successful treatment of a Kenyan case of unresponsive cutaneous leishmaniasis with a combination of pentostam and oral allopurinol: Case report. East Afr. Med. J. 2010, 87, 521–524. [Google Scholar]
- Yaich, S.; Charfeddine, K.; Masmoudi, A.; Masmoudi, M.; Zaghdhane, S.; Turki, H.; Hachicha, J. Atypical presentation of cutaneous leishmaniasis in a renal transplant recipient successfully treated with allopurinol and fluconazole. Ann. Saudi. Med. 2013, 33, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Boecken, G.; Sunderkötter, C.; Bogdan, C.; Weitzel, T.; Fischer, M.; Müller, A.; Löbermann, M.; Anders, G.; von Stebut, E.; Schunk, M.; et al. Diagnosis and therapy of cutaneous and mucocutaneous Leishmaniasis in Germany. J. Dtsch. Dermatol. Ges. 2011, 9, 1–51. [Google Scholar] [CrossRef]
- Di Muccio, T.; Scalone, A.; Bruno, A.; Marangi, M.; Grande, R.; Armignacco, O.; Gradoni, L.; Gramiccia, M. Epidemiology of Imported Leishmaniasis in Italy: Implications for a European Endemic Country. PLoS ONE 2015, 26, e0129418. [Google Scholar]
- Diniz, J.L.C.P.; Costa MO da, R.; Gonçalves, D.U. Mucocutaneous Leishmaniasis: Clinical markers in presumptive diagnosis. Braz. J. Otorhinolaryngol. 2011, 77, 380–384. [Google Scholar] [CrossRef] [Green Version]
- da Costa, D.C.S.; Palmeiro, M.R.; Moreira, J.S.; Martins, A.C.d.C.; da Silva, A.F.; Madeira, M.d.F.; Quintella, L.P.; Confort, E.M.; Schubach, A.d.O.; da Conceicao Silva, F.; et al. Oral manifestations in the American tegumentary leishmaniasis. PLoS ONE 2014, 9, e109790. [Google Scholar]
- Fernandez-Flores, A.; Rodriguez-Peralto, J.L. Morphological and immunohistochemical clues for the diagnosis of cutaneous leishmaniasis and the interpretation of CD1a status. J. Am. Acad. Dermatol. 2016, 74, 536–543. [Google Scholar] [CrossRef]
- Dias-Polak, D.; Geffen, Y.; Ben-Izhak, O.; Bergman, R. The Role of Histopathology and Immunohistochemistry in the Diagnosis of Cutaneous Leishmaniasis Without “Discernible” Leishman–Donovan Bodies. Am. J. Dermatopathol. 2017, 39, 890. [Google Scholar] [CrossRef] [PubMed]
- Strazzulla, A.; Cocuzza, S.; Pinzone, M.R.; Postorino, M.C.; Cosentino, S.; Serra, A.; Cacopardo, B.; Munnari, G. Mucosal leishmaniasis: An underestimated presentation of a neglected disease. Biomed. Res. Int. 2013, 2013, 805108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobo, F.; Rodríguez-Granger, J.; Gómez-Camarasa, C.; Sampedro, A.; Aliaga-Martínez, L.; Navarro, J.M.; Fernández, J.G. Localized mucosal leishmaniasis caused by Leishmania infantum mimicking cancer in the rhinolaryngeal region. Int. J. Infect. Dis. 2016, 50, 54–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, O.P.; Sundar, S. Immunotherapy and targeted therapies in treatment of visceral leishmaniasis: Current status and future prospects. Front Immunol. 2014, 5, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boaventura, V.S.; de Oliveira, J.G.S.; Costa, J.M.L.; Novais, F.O.; de Oliveira, C.I.; Barral-Netto, M.; Barral, A. The value of the otorhinolaryngologic exam in correct mucocutaneous leishmaniasis diagnosis. Am. J. Trop Med. Hyg. 2009, 81, 384–386. [Google Scholar] [CrossRef]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspari, V.; Zaghi, I.; Macrì, G.; Patrizi, A.; Salfi, N.; Locatelli, F.; Carra, E.; Re, M.C.; Varani, S. Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches. Microorganisms 2020, 8, 588. https://doi.org/10.3390/microorganisms8040588
Gaspari V, Zaghi I, Macrì G, Patrizi A, Salfi N, Locatelli F, Carra E, Re MC, Varani S. Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches. Microorganisms. 2020; 8(4):588. https://doi.org/10.3390/microorganisms8040588
Chicago/Turabian StyleGaspari, Valeria, Irene Zaghi, Giovanni Macrì, Annalisa Patrizi, Nunzio Salfi, Francesca Locatelli, Elena Carra, Maria Carla Re, and Stefania Varani. 2020. "Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches" Microorganisms 8, no. 4: 588. https://doi.org/10.3390/microorganisms8040588
APA StyleGaspari, V., Zaghi, I., Macrì, G., Patrizi, A., Salfi, N., Locatelli, F., Carra, E., Re, M. C., & Varani, S. (2020). Autochthonous Cases of Mucosal Leishmaniasis in Northeastern Italy: Clinical Management and Novel Treatment Approaches. Microorganisms, 8(4), 588. https://doi.org/10.3390/microorganisms8040588