
Influence of the Incubator as Direct Patient Environment on Bacterial Colonization of Neonates

 ,
,  ,
,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
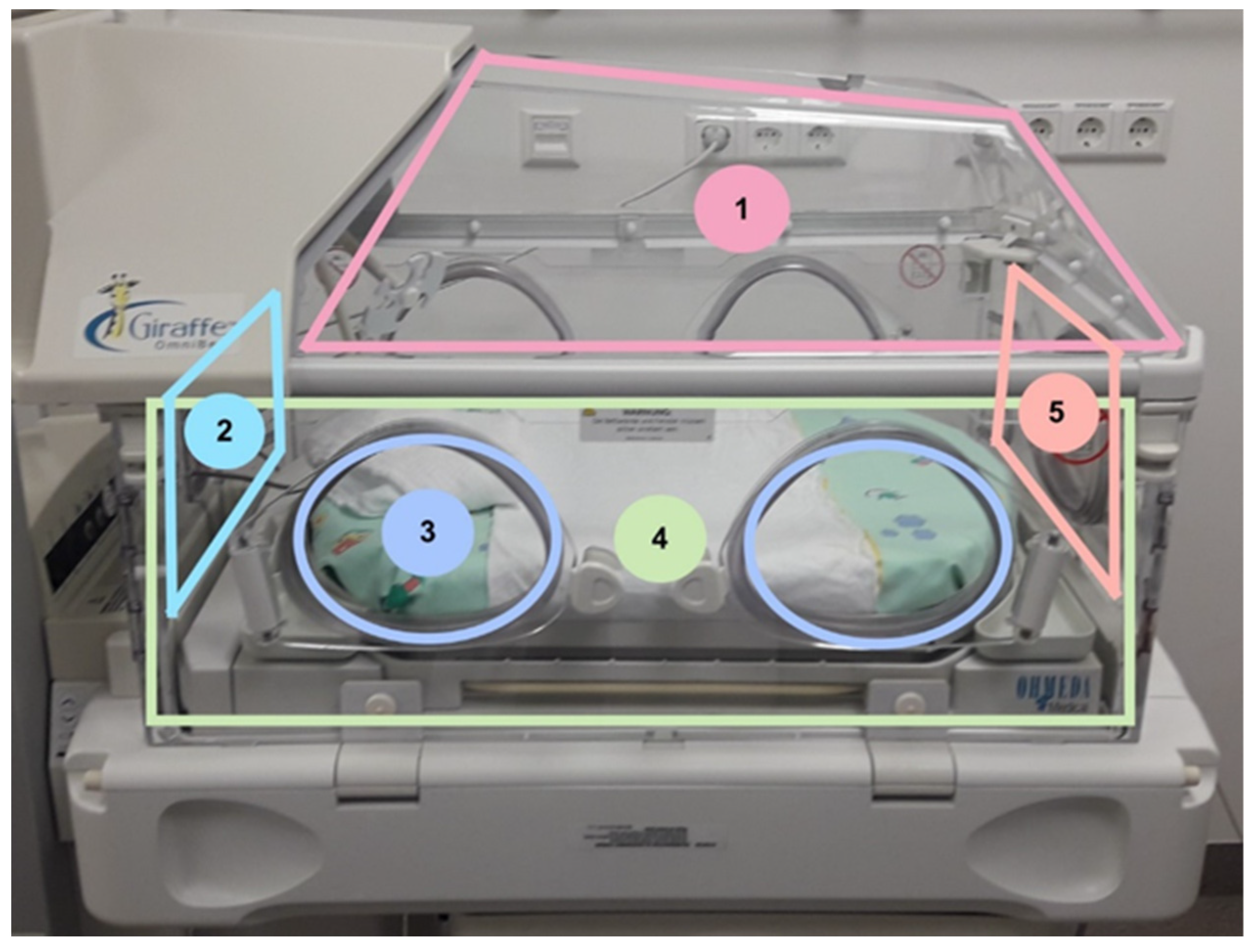
2.1. Incubator Disinfection and Sampling
2.2. Neonatal Screening and Match Process
2.3. Enrichment and Incubation of the Incubator and the Patient Samples
2.4. DNA Isolation and Whole Genome Sequencing
3. Results
3.1. Patient Population and Microbial Colonization
3.2. Microbial Findings of Neonatal Incubators
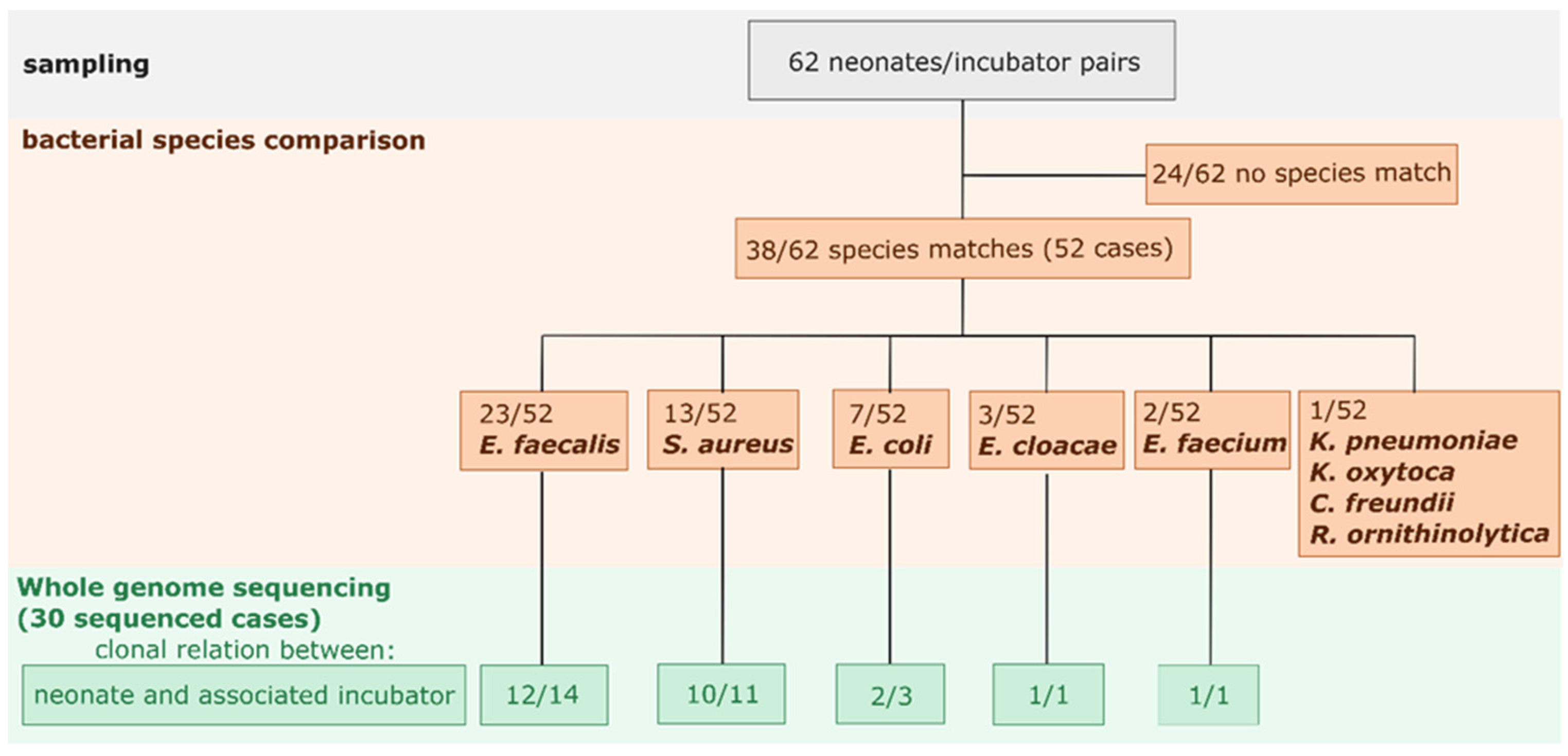
3.3. Bacterial Species Comparison between Neonatal and Their Associated Incubator
3.4. Clonality and Cluster Analysis
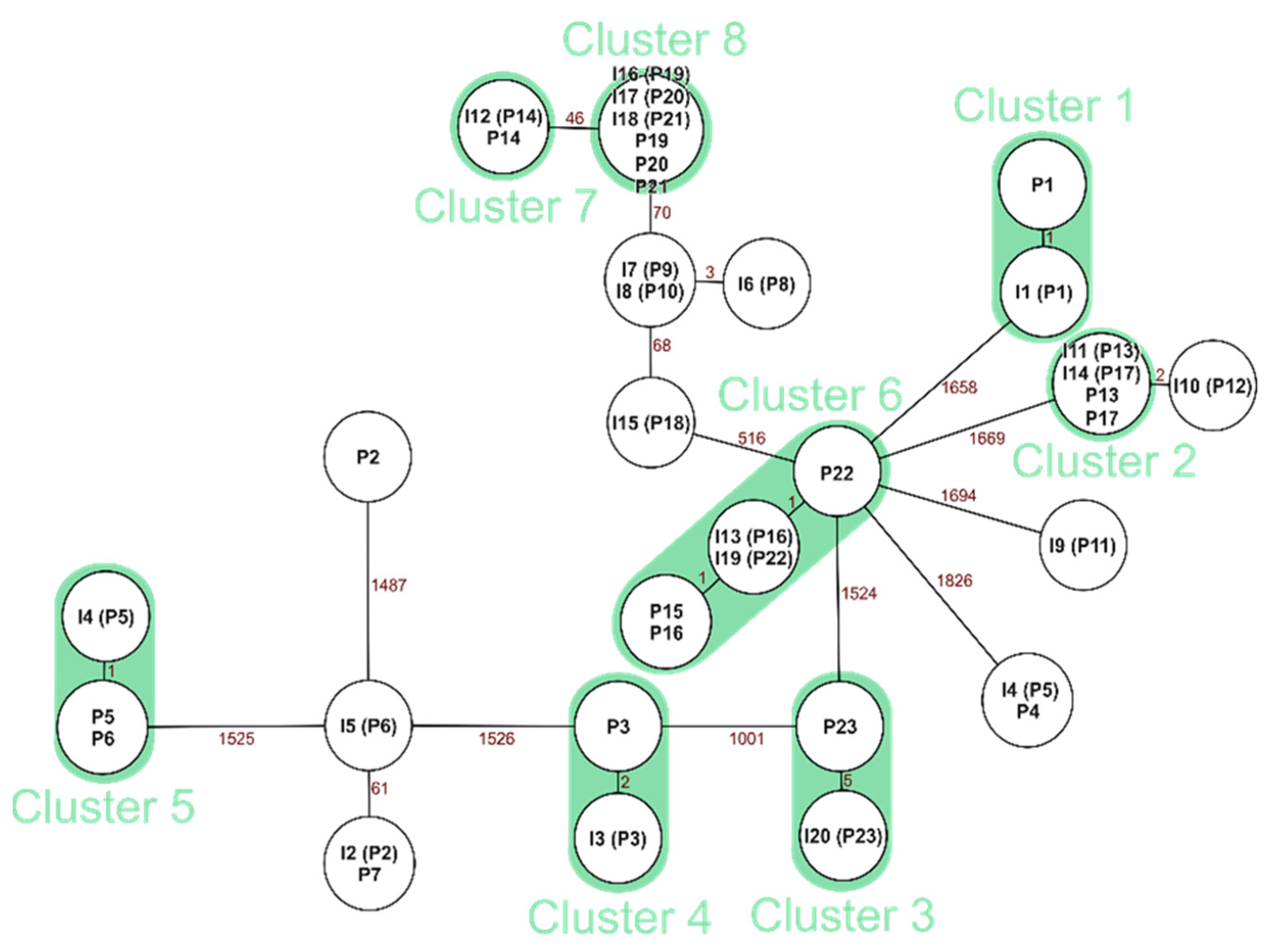
3.4.1. Clonal Comparison: Neonate and the Corresponding Incubator for E. faecalis
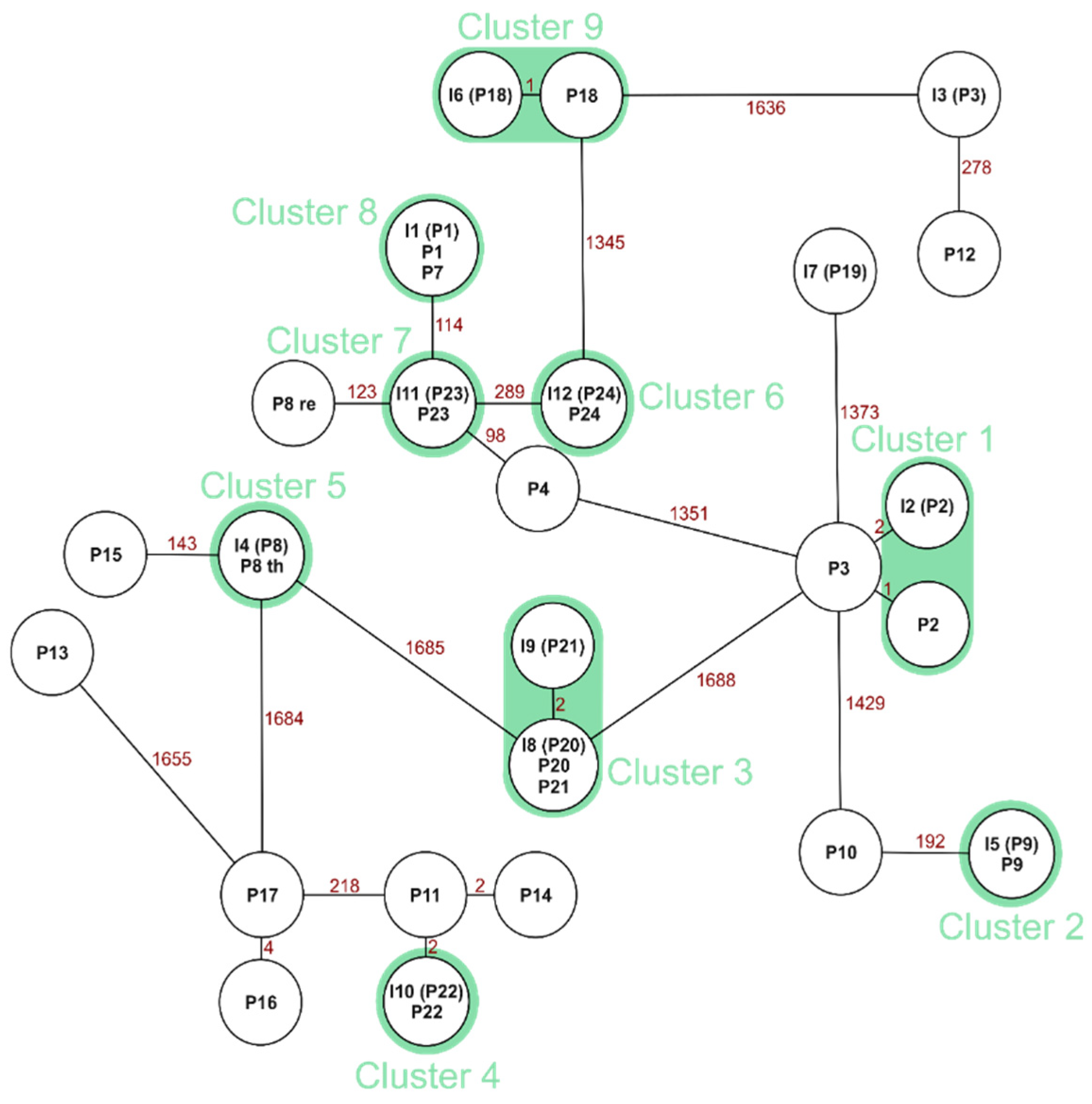
3.4.2. Clonal Comparison: Neonate and the Corresponding Incubator for S. aureus
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shao, Y.; Forster, S.C.; Tsaliki, E.; Vervier, K.; Strang, A.; Simpson, N.; Kumar, N.; Stares, M.D.; Rodger, A.; Brocklehurst, P.; et al. Stunted microbiota and opportunistic pathogen colonization in caesarean-section birth. Nature 2019, 574, 117–121. [Google Scholar] [CrossRef]
- Maqsood, R.; Rodgers, R.; Rodriguez, C.; Handley, S.A.; Ndao, I.M.; Tarr, P.I.; Warner, B.B.; Lim, E.S.; Holtz, L.R. Discordant transmission of bacteria and viruses from mothers to babies at birth. Microbiome 2019, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Bello, M.G.; Costello, E.K.; Contreras, M.; Magris, M.; Hidalgo, G.; Fierer, N.; Knight, R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns. Proc. Natl. Acad. Sci. USA 2010, 107, 11971–11975. [Google Scholar] [CrossRef] [Green Version]
- Butel, M.; Waligora-Dupriet, A.; Wydau-Dematteis, S. The developing gut microbiota and its consequences for health. J. Dev. Orig. Health Dis. 2018, 9, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Hornik, C.P.; Fort, P.; Clark, R.H.; Watt, K.; Benjamin, D.K., Jr.; Smith, P.B.; Manzoni, P.; Jacqz-Aigrain, E.; Kaguelidou, F.; Cohen-Wolkowiez, M. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum. Dev. 2012, 88 (Suppl. S2), S69–S74. [Google Scholar] [CrossRef] [Green Version]
- Legeay, C.; Bourigault, C.; Lepelletier, D.; Zahar, J.R. Prevention of healthcare-associated infections in neonates: Room for improvement. J. Hosp. Infect. 2015, 89, 319–323. [Google Scholar] [CrossRef]
- Christoph, J.; Dame, C.; Eckmanns, T. Praktische Umsetzung sowie krankenhaushygienische und infektionspräventive Konsequenzen des mikrobiellen Kolonisationsscreenings bei intensivmedizinisch behandelten Früh-und Neugeborenen. Epidemiol. Bull. 2013, 42, 421–431. [Google Scholar] [CrossRef]
- Empfehlung, R.I.Z. Ergänzende Empfehlung (2011) zur Prävention nosokomialer Infektionen bei neonatologischen Intensivpflegepatienten mit einem Geburtsgewicht unter 1.500 g (2007). Epidemiol. Bull. 2011, 2012, 13–15. [Google Scholar] [CrossRef]
- Lavage, B.B.; oder Tubus, M. Empfehlung zur Prävention nosokomialer Infektionen bei neonatologischen Intensivpflegepatienten mit einem Geburtsgewicht unter 1500 g. Bundesgesundheitsblatt-Gesundh.-Gesundh. 2007, 50, 1265–1303. [Google Scholar] [CrossRef]
- Fleischmann-Struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Samuels, N.; van de Graaf, R.A.; de Jonge, R.C.J.; Reiss, I.K.M.; Vermeulen, M.J. Risk factors for necrotizing enterocolitis in neonates: A systematic review of prognostic studies. BMC Pediatr. 2017, 17, 105. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.; Olm, M.R.; Firek, B.A.; Baker, R.; Geller-McGrath, D.; Reimer, S.R.; Soenjoyo, K.R.; Yip, J.S.; Dahan, D.; Thomas, B.C.; et al. The developing premature infant gut microbiome is a major factor shaping the microbiome of neonatal intensive care unit rooms. Microbiome 2018, 6, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimentel de Araujo, F.; Tinelli, M.; Battisti, A.; Ercoli, A.; Anesi, A.; Pantosti, A.; Monaco, M. An outbreak of skin infections in neonates due to a Staphylococcus aureus strain producing the exfoliative toxin A. Infection 2018, 46, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Fortunov, R.M.; Hulten, K.G.; Hammerman, W.A.; Mason, E.O., Jr.; Kaplan, S.L. Community-acquired Staphylococcus aureus infections in term and near-term previously healthy neonates. Pediatrics 2006, 118, 874–881. [Google Scholar] [CrossRef]
- Zingg, W.; Posfay-Barbe, K.M.; Pittet, D. Healthcare-associated infections in neonates. Curr. Opin. Infect. Dis. 2008, 21, 228–234. [Google Scholar] [CrossRef]
- Kotsanas, D.; Tan, K.; Scott, C.; Baade, B.; Cheng, M.H.L.; Tan, Z.V.; Taylor, J.E.; Kwong, J.C.; Seemann, T.; Coombs, G.W.; et al. A nonclonal outbreak of vancomycin-sensitive Enterococcus faecalis bacteremia in a neonatal intensive care unit. Infect. Control Hosp. Epidemiol. 2019, 40, 1116–1122. [Google Scholar] [CrossRef]
- Mariani, M.; Bandettini, R.; La Masa, D.; Minghetti, D.; Baldelli, I.; Serveli, S.; Mesini, A.; Saffioti, C.; Ramenghi, L.A.; Castagnola, E. Bacterial invasive infections in a neonatal intensive care unit: A 13 years microbiological report from an Italian tertiary care centre. J. Prev. Med. Hyg. 2020, 61, E162–E166. [Google Scholar] [CrossRef] [PubMed]
- Akinboyo, I.C.; Voskertchian, A.; Gorfu, G.; Betz, J.F.; Ross, T.L.; Carroll, K.C.; Milstone, A.M. Epidemiology and risk factors for recurrent Staphylococcus aureus colonization following active surveillance and decolonization in the NICU. Infect. Control Hosp. Epidemiol. 2018, 39, 1334–1339. [Google Scholar] [CrossRef]
- Robert-Koch-Institut. KISS Krankenhaus-Infektions-Surveillance-System. Modul NEO-KISS. Referenzdaten. 2019. Available online: https://www.nrz-hygiene.de/fileadmin/nrz/module/neo/201701_201912_NEORef.pdf (accessed on 28 June 2021).
- Mellmann, A.; Bletz, S.; Boking, T.; Kipp, F.; Becker, K.; Schultes, A.; Prior, K.; Harmsen, D. Real-Time Genome Sequencing of Resistant Bacteria Provides Precision Infection Control in an Institutional Setting. J. Clin. Microbiol. 2016, 54, 2874–2881. [Google Scholar] [CrossRef] [Green Version]
- Leopold, S.R.; Goering, R.V.; Witten, A.; Harmsen, D.; Mellmann, A. Bacterial whole-genome sequencing revisited: Portable, scalable, and standardized analysis for typing and detection of virulence and antibiotic resistance genes. J. Clin. Microbiol. 2014, 52, 2365–2370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neumann, B.; Prior, K.; Bender, J.K.; Harmsen, D.; Klare, I.; Fuchs, S.; Bethe, A.; Zuhlke, D.; Gohler, A.; Schwarz, S.; et al. A Core Genome Multilocus Sequence Typing Scheme for Enterococcus faecalis. J. Clin. Microbiol. 2019, 57, 3. [Google Scholar] [CrossRef] [Green Version]
- Brooks, B.; Olm, M.R.; Firek, B.A.; Baker, R.; Thomas, B.C.; Morowitz, M.J.; Banfield, J.F. Strain-resolved analysis of hospital rooms and infants reveals overlap between the human and room microbiome. Nat. Commun. 2017, 8, 1814. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.Y.L.; Bloomfield, F.H.; O’Sullivan, J.M. Factors Affecting Gastrointestinal Microbiome Development in Neonates. Nutrients 2018, 10, 274. [Google Scholar] [CrossRef] [Green Version]
- Adeghate, J.O.; Juhasz, E.; Ivan, M.A.; Pongracz, J.; Kristof, K. Similar Strains of Coagulase-Negative Staphylococci Found in the Gastrointestinal Tract and Bloodstream of Bacteremic Neonates. Can. J. Infect. Dis. Med. Microbiol. 2020, 2020, 3509676. [Google Scholar] [CrossRef] [PubMed]
- Chavignon, M.; Reboux, M.; Tasse, J.; Tristan, A.; Claris, O.; Laurent, F.; Butin, M. Persistent microbial contamination of incubators despite disinfection. Pediatr. Res. 2021. [Google Scholar] [CrossRef]
- Stein, C.; Lange, I.; Rodel, J.; Pletz, M.W.; Kipp, F. Targeted Molecular Detection of Nosocomial Carbapenemase-Producing Gram-Negative Bacteria-On Near- and Distant-Patient Surfaces. Microorganisms 2021, 9, 1190. [Google Scholar] [CrossRef] [PubMed]
- Hartz, L.E.; Bradshaw, W.; Brandon, D.H. Potential NICU Environmental Influences on the Neonate’s Microbiome: A Systematic Review. Adv. Neonatal. Care 2015, 15, 324–335. [Google Scholar] [CrossRef] [Green Version]
- Andersen, B.M.; Banrud, H.; Boe, E.; Bjordal, O.; Drangsholt, F. Comparison of UV C light and chemicals for disinfection of surfaces in hospital isolation units. Infect. Control Hosp. Epidemiol. 2006, 27, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Katara, G.; Hemvani, N.; Chitnis, S.; Chitnis, V.; Chitnis, D.S. Surface disinfection by exposure to germicidal UV light. Indian J. Med. Microbiol. 2008, 26, 241–242. [Google Scholar] [CrossRef]
- Cipolla, D.; Giuffre, M.; Mammina, C.; Corsello, G. Prevention of nosocomial infections and surveillance of emerging resistances in NICU. J. Matern.-Fet. Neonatal Med. 2011, 24 (Suppl. S1), 23–26. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Lin, C.F.; Rehn, Y.F.; Chen, J.C.; Chen, P.Y.; Chen, C.H.; Wang, T.M.; Huang, F.L. Reduced nosocomial infection rate in a neonatal intensive care unit during a 4-year surveillance period. J. Chin. Med. Assoc. 2017, 80, 427–431. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, I.; Edel, B.; Dawczynski, K.; Proquitté, H.; Pletz, M.W.; Kipp, F.; Stein, C. Influence of the Incubator as Direct Patient Environment on Bacterial Colonization of Neonates. Microorganisms 2021, 9, 2533. https://doi.org/10.3390/microorganisms9122533
Lange I, Edel B, Dawczynski K, Proquitté H, Pletz MW, Kipp F, Stein C. Influence of the Incubator as Direct Patient Environment on Bacterial Colonization of Neonates. Microorganisms. 2021; 9(12):2533. https://doi.org/10.3390/microorganisms9122533
Chicago/Turabian StyleLange, Isabel, Birgit Edel, Kristin Dawczynski, Hans Proquitté, Mathias W. Pletz, Frank Kipp, and Claudia Stein. 2021. "Influence of the Incubator as Direct Patient Environment on Bacterial Colonization of Neonates" Microorganisms 9, no. 12: 2533. https://doi.org/10.3390/microorganisms9122533
APA StyleLange, I., Edel, B., Dawczynski, K., Proquitté, H., Pletz, M. W., Kipp, F., & Stein, C. (2021). Influence of the Incubator as Direct Patient Environment on Bacterial Colonization of Neonates. Microorganisms, 9(12), 2533. https://doi.org/10.3390/microorganisms9122533