
Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
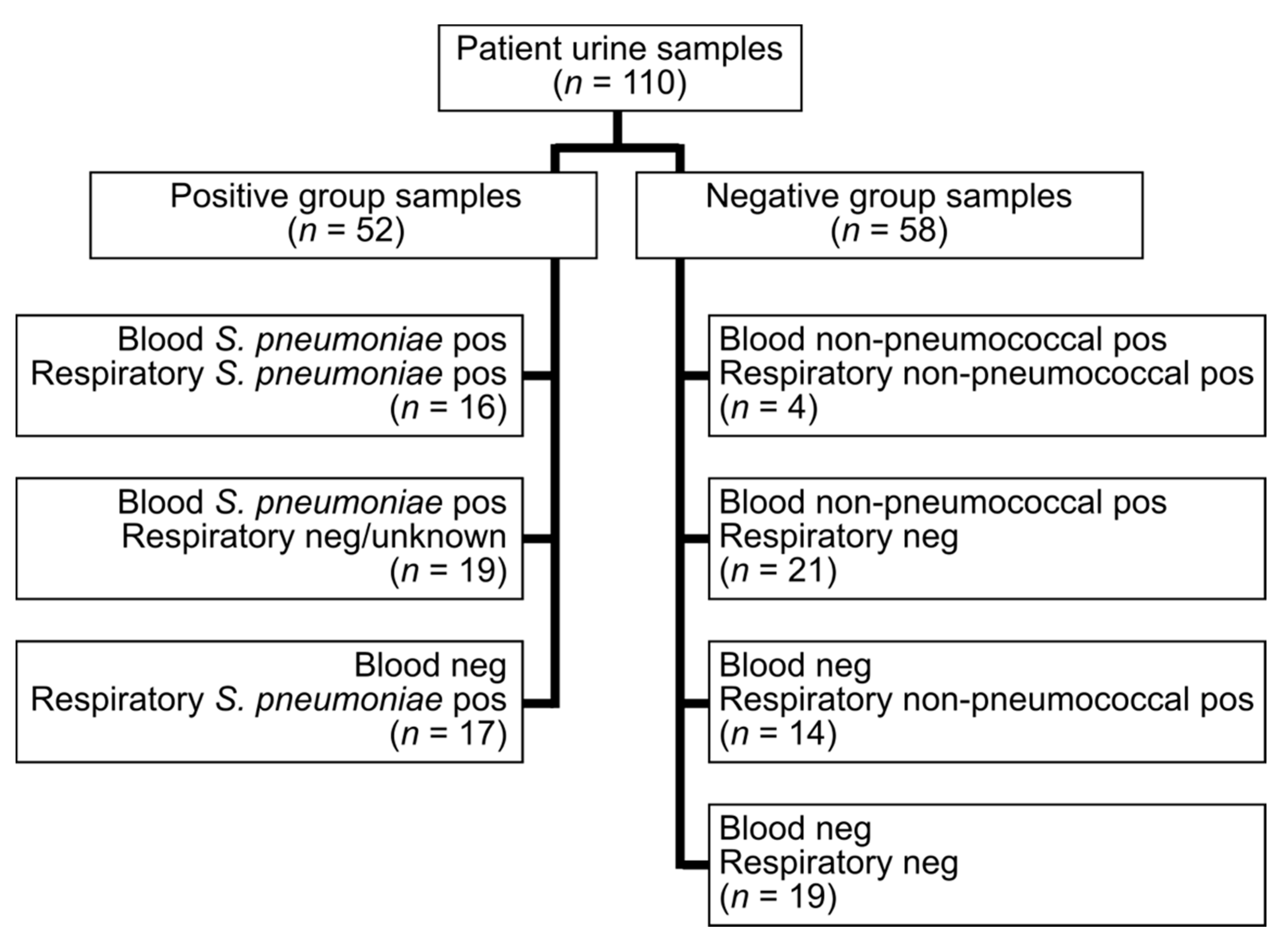
2.1. Samples
2.2. Urinary Antigen Tests (UATs)
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Sensitivity of S. pneumoniae UATs
3.3. Specificity of S. pneumoniae UATs
3.4. Agreement of Results between UATs
3.5. Agreement between Visual and Automatic Reading of UATs
3.6. Assay Performance after Long-Time Storage
3.7. Time to Result and User Friendliness
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Weiser, J.N.; Ferreira, D.M.; Paton, J.C. Streptococcus pneumoniae: Transmission, colonization and invasion. Nat. Rev. Microbiol. 2018, 16, 355–367. [Google Scholar] [CrossRef] [PubMed]
- WHO. W.H.O. Pneumococcal Disease. Available online: https://www.who.int/ith/diseases/pneumococcal/en/ (accessed on 14 July 2020).
- Athlin, S.; Iversen, A.; Özenci, V. Comparison of the ImmuView and the BinaxNOW antigen tests in detection of Streptococcus pneumoniae and Legionella pneumophila in urine. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Euser, S.M.; Badoux, P.; Kracht-Kosten, L.; Yzerman, E.P.F. Evaluation of the Sofia Streptococcus pneumoniae FIA test for the detection of S. pneumoniae antigen in urine. J. Med. Microbiol. 2018, 67, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Burgos, J.; Garcia-Pérez, J.N.; di Lauro, S.G.; Falcó, V.; Pumarola, T.; Almirante, B.; Teresa Martín Gomez, M. Usefulness of Sofia Pneumococcal FIA® test in comparison with BinaxNOW® Pneumococcal test in urine samples for the diagnosis of pneumococcal pneumonia. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Vicente, D.; López-Olaizola, M.; de la Caba, I.; Cilla, G. Evaluation of Sofia Fluorescent immunoassay analyzer for pneumococcal urinary antigen detection in hospitalized patients with community-acquired pneumonia. J. Microbiol. Methods 2017, 141, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, F.; Masiá, M.; Rodríguez, J.C.; Ayelo, A.; Soldán, B.; Cebrián, L.; Mirete, C.; Royo, G.; Hidalgo, A.M. Evaluation of the immunochromatographic Binax NOW assay for detection of Streptococcus pneumoniae urinary antigen in a prospective study of community-acquired pneumonia in Spain. Clin. Infect. Dis. 2003, 36, 286–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olofsson, E.; Özenci, V.; Athlin, S. Evaluation of the Sofia, S. pneumoniae FIA for Detection of Pneumococcal Antigen in Patients with Bloodstream Infection. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Badoux, P.; Kracht-Kosten, L.; Herpers, B.; Euser, S. Method Comparison of the ImmuView, L. pneumophila and L. longbeachae Urinary Antigen Test with the BinaxNOW Legionella Urinary Antigen Card for Detection of Legionella pneumophila Serogroup 1 Antigen in Urine. J. Clin. Microbiol. 2020, 58, e01429-19. [Google Scholar] [CrossRef] [PubMed]
- Zaiontz, C. Real Statistics Using Excel. Available online: http://www.real-statistics.com/ (accessed on 16 September 2020).
- Congestri, F.; Morotti, M.; Vicari, R.; Pedna, M.F.; Sparacino, M.; Torri, A.; Bertini, S.; Fantini, M.; Sambri, V. Comparative evaluation of the novel IMMUNOCATCH™ Streptococcus pneumoniae (EIKEN CHEMICAL CO., LTD) test with the Uni-Gold™ Streptococcus pneumoniae assay and the BinaxNOW® Streptococcus pneumoniae antigen card for the detection of pneumococcal capsular antigen in urine samples. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 749–751. [Google Scholar] [PubMed]
- Sinclair, A.; Xie, X.; Teltscher, M.; Dendukuri, N. Systematic review and meta-analysis of a urine-based pneumococcal antigen test for diagnosis of community-acquired pneumonia caused by Streptococcus pneumoniae. J. Clin. Microbiol. 2013, 51, 2303–2310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.D.; Derrington, P.; Evans, R.; Creek, M.; Morris, R.; Dance, D.A.; Cartwright, K. Rapid diagnosis of bacteremic pneumococcal infections in adults by using the Binax NOW Streptococcus pneumoniae urinary antigen test: A prospective, controlled clinical evaluation. J. Clin. Microbiol. 2003, 41, 2810–2813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athlin, S.; Altun, O.; Eriksen, H.B.; Özenci, V.; Strålin, K. The Uni-Gold Streptococcus pneumoniae urinary antigen test: An interassay comparison with the BinaxNOW® Streptococcus pneumoniae test on consecutive urine samples and evaluation on patients with bacteremia. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Slotved, H.C.; Jørgensen, C.S.; Jørgensen, K.M.; Fuursted, K. A case of false-positive pneumococcal urinary antigen test in a bacteremic Streptococcus agalactiae infection. APMIS 2020, 128, 511–512. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.Y.W.; Johnsson, A.T.A.; Iversen, A.; Athlin, S.; Özenci, V. Evaluation of Four Lateral Flow Assays for the Detection of Legionella Urinary Antigen. Microorganisms 2021, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, D.R.; Laing, R.T.; Mills, G.D.; Karalus, N.C.; Town, G.I.; Mirrett, S.; Reller, L.B. Evaluation of a rapid immunochromatographic test for detection of Streptococcus pneumoniae antigen in urine samples from adults with community-acquired pneumonia. J. Clin. Microbiol. 2001, 39, 3495–3498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jørgensen, C.S.; Uldum, S.A.; Sørensen, J.F.; Skovsted, I.C.; Otte, S.; Elverdal, P.L. Evaluation of a new lateral flow test for detection of Streptococcus pneumoniae and Legionella pneumophila urinary antigen. J. Microbiol. Methods 2015, 116, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Saukkoriipi, A.; Pascal, T.; Palmu, A.A. Evaluation of the BinaxNOW® Streptococcus pneumoniae antigen test on fresh, frozen and concentrated urine samples in elderly patients with and without community-acquired pneumonia. J. Microbiol. Methods 2016, 121, 24–26. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Assay | Commercial Name | Reader | Manufacturer |
|---|---|---|---|
| BinaxNOW | BinaxNOW S. pneumoniae Antigen Card | DIGIVAL instrument | Abbott (Chicago, IL, USA) |
| ImmuView | ImmuView S. pneumoniae and Legionella | ImmuView Reader | SSI Diagnostica (Hillerød, Denmark) |
| Sofia | Sofia S. pneumoniae FIA | Sofia FIA Analyzer | Quidel Corporation (San Diego, CA, USA) |
| STANDARD F | STANDARD F S. pneumoniae Ag FIA | STANDARD F200 Analyzer | SD Biosensor (Gyeonggi, South Korea) |
| Assay | UAT Positive | UAT Negative | Sensitivity (95% CI) |
|---|---|---|---|
| BinaxNOW | 43 | 9 | 82.7 (70.2–90.6) |
| ImmuView | 40 | 12 | 76.9 (63.9–86.3) |
| Sofia | 45 | 7 | 86.5 (74.7–93.3) |
| STANDARD F | 42 | 10 | 80.8 (68.1–89.2) |
| χ2 (3) | Q = 5.57 (p = 0.13) |
| Sample | Blood Culture Result | Respiratory Culture Result | BinaxNOW | ImmuView | Sofia | STANDARD F |
|---|---|---|---|---|---|---|
| P15 | Streptococcus pneumoniae | Streptococcus pneumoniae | Negative | Negative | Negative | Negative |
| P28 | Streptococcus pneumoniae | Negative (normal flora) | Negative | Negative | Negative | Negative |
| P23 | Streptococcus pneumoniae | Negative (normal flora) | Negative | Negative | Negative | Negative |
| P51 | Negative | Streptococcus pneumoniae | Negative | Negative | Negative | Negative |
| P36 | Escherichia coli | Streptococcus pneumoniae | Negative | Negative | Negative | Negative |
| P3 | Streptococcus pneumoniae | Streptococcus pneumoniae, Staphylococcus aureus | Negative | Positive | Negative | Negative |
| P24 | Streptococcus pneumoniae | Negative (normal flora) | Negative | Negative | Positive | Negative |
| P27 | Streptococcus pneumoniae | Negative (normal flora) | Negative | Negative | Positive | Negative |
| P35 | Streptococcus pneumoniae | Not determined | Positive | Negative | Negative | Negative |
| P38 | Negative | Streptococcus pneumoniae | Negative | Positive | Positive | Negative |
| P5 | Streptococcus pneumoniae | Streptococcus pneumoniae | Positive | Negative | Positive | Positive |
| P19 | Streptococcus pneumoniae | Staphylococcus aureus | Positive | Negative | Positive | Positive |
| P34 | Streptococcus pneumoniae | Not determined | Positive | Negative | Positive | Positive |
| P42 | Negative | Streptococcus pneumoniae | Positive | Negative | Positive | Positive |
| Assay | UAT Negative | UAT Positive | Invalid/Error | Sensitivity (95% CI) |
|---|---|---|---|---|
| BinaxNOW | 52 | 6 | 0 | 89.7 (79.2–95.2) |
| ImmuView | 49 | 9 | 0 | 84.5 (73.1–91.6) |
| Sofia | 48 | 9 | 1 | 84.2 (72.6–91.5) |
| STANDARD F | 52 | 6 | 0 | 89.7 (79.2–95.2) |
| χ2 (3) | Q = 4.50 (p = 0.70) |
| Sample | Blood Culture Result | Respiratory Culture Result | BinaxNOW | ImmuView | Sofia | STANDARD F |
|---|---|---|---|---|---|---|
| N5 | Bacteroides fragilis | Negative (normal flora) | Positive | Positive | Positive | Positive |
| N32 | Negative | Klebsiella pneumoniae | Positive | Positive | Positive | Positive |
| N38 | Negative | Moraxella catarrhalis | Positive | Positive | Positive | Positive |
| N31 | Negative | Hemophilus influenzae | Positive | Positive | Positive | Positive |
| N47 | Negative | Negative (normal flora) | Positive | Positive | Positive | Positive |
| N27 | Negative | Hemophilus influenzae | Negative | Positive | Positive | Negative |
| N43 | Negative | Negative (normal flora) | Negative | Positive | Positive | Negative |
| N56 | Negative | Negative (normal flora) | Negative | Negative | Invalid | Positive |
| N23 | Staphylococcus epidermidis | Negative (normal flora) | Negative | Positive | Negative | Negative |
| N11 | Escherichia coli | Negative (normal flora) | Negative | Negative | Positive | Negative |
| N17 | Proteus mirabilis | Negative (normal flora) | Positive | Negative | Negative | Negative |
| N6 | Escherichia coli | Negative (normal flora) | Negative | Negative | Positive | Negative |
| N33 | Negative | Moraxella catarrhalis | Negative | Positive | Negative | Negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, A.Y.W.; Johnsson, A.T.A.; Ininbergs, K.; Athlin, S.; Özenci, V. Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers. Microorganisms 2021, 9, 827. https://doi.org/10.3390/microorganisms9040827
Wong AYW, Johnsson ATA, Ininbergs K, Athlin S, Özenci V. Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers. Microorganisms. 2021; 9(4):827. https://doi.org/10.3390/microorganisms9040827
Chicago/Turabian StyleWong, Alicia Yoke Wei, Alexander Tony Arvind Johnsson, Karolina Ininbergs, Simon Athlin, and Volkan Özenci. 2021. "Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers" Microorganisms 9, no. 4: 827. https://doi.org/10.3390/microorganisms9040827
APA StyleWong, A. Y. W., Johnsson, A. T. A., Ininbergs, K., Athlin, S., & Özenci, V. (2021). Comparison of Four Streptococcus pneumoniae Urinary Antigen Tests Using Automated Readers. Microorganisms, 9(4), 827. https://doi.org/10.3390/microorganisms9040827