1. Introduction
The presence of high concentrations of ketone bodies in the blood—namely beta-hydroxybutyrate (BHB), acetoacetate, and acetone—is called hyperketonemia or ketosis and is one of the most harmful and damaging metabolic diseases in dairy cows, resulting from negative energy balance (NEB), especially during early lactation [
1]. In Europe, a prevalence of subclinical ketosis has been reported (serum BHB ≥ 1.2 mmol/L) between 11.2 and 36.6% from 2nd to 15th days in milk (DIM) [
2], similar to that observed in other continents, and where the prevalence of cows developing serum BHB ≥ 3.0 mmol/L, and related to clinical ketosis, was 3.4% on average [
3].
Clinical ketosis, displacement of the abomasum (DA), metritis, and lameness are more likely to occur in dairy cows with hyperketonemia levels [
2]. It is reasonable to expect that metabolic (oxidative) stress NEB at the beginning of lactation associated with hyperketonemia, will have a depressive effect on the immune system of the affected animals, increasing their susceptibility to the occurrence of pathologies such as metritis and laminitis, in this initial phase [
2,
4]. Moreover, Holstein cows, as other breeds such as Jerseys, Brown Swiss, Guernseys, Ayrshires, and Simmental-Red Holsteins commonly present DA [
5]. Left side DA (LDA), with heritability estimated at 0.30 on Holstein cows [
5], is more frequent than right side DA with implications for animal health and welfare, representing significant financial losses for dairy farmers.
LDA is common in high-producing dairy cows, mainly during the first month of lactation [
6]. A surgical approach is usually required to treat this condition. A one-step laparoscopy-guided abomasopexy (Christiansen modified technique) treatment of LDA is a minimally invasive technique that allows the confirmation of the LDA and the evaluation of eventual adhesions between the abomasum and the left abdominal wall or rumen. More importantly, it can be performed completely in a standing cow, without the need to put it in recumbency, and is easier and faster than two-step laparoscopy [
7,
8,
9]. According to Wapenaar and Roberts (2017), the survival rate ranges from 73 to 88% in six months [
10].
The determination, by spectrophotometry, of the BHB concentration has been considered the gold standard method [
1]. However, in recent years, due to the high correlation between the concentration of BHB in blood and milk (about 10 times less concentration), this latter fluid has served as a viable sample to determine this metabolite [
11,
12], being of common use in dairy farms. Another indirect method of assessing the energy balance is the fat to protein content (F:P) ratio [
13]. An increase in the F:P ratio coincides with periods of NEB associated with increased mobilization of lipid reserves, which stimulates hyperketonemia and the fat content of milk [
14]. According to Heuer et al. F:P ratio threshold between 1.35 and 1.50 can predict cows in energy deficit [
13], but these values are not consensual [
15]. Moreover, the F:P ratio of milk reflects the health status of the cow if the cow has already suffered or is suffering from the effects of a disease, so it can potentially serve as an indicator of energy deficit, including estimating hyperketonemia [
16] and for monitoring energy balance during the first few months after delivery. Furthermore, van Knegsel et al. [
17] and Denis-Robichaud et al. [
18] suggested a F:P ratio threshold of ≥1.5 and ≥1.3 [
18], respectively, to predict cows with hyperketonemia. The serum BHB concentration was used in these last studies.
Although numerous studies on the association between hyperketonemia and postpartum diseases, such as some of the above, have been carried out, we have not found relevant studies investigating the metabolic pattern of BHB measured by milk, or that of the F:P ratio preceding and following its treatment. The present study’s main objective is to determine the profiles of BHB in milk and the F:P ratio, during the first five months of lactation, in laparoscopic-treated LDA Holstein dairy cows. Other general postpartum diseases were also assessed.
4. Discussion
Cows with LDA (group B) were found to have higher BHB concentrations in milk (0.18 ± 0.02 mmol/L) than the control group (0.07 ± 0.02 mmol/L; p < 0.001) in DIM1, decreasing rapidly in the following month, even though the proportion of LDA and clinical ketosis was similar in DIM1 and DIM2. The results also show that the animals recover quickly after treatment, with no significant differences in BHB between groups from DIM3.
The control group kept BHB levels (0.7 mmol/ L) in DIM1 and DIM2 stable, which halved in DIM3, when the peak dry matter intake was reached, indicating that the energy management of the farms in question was adequate to the different groups. The higher concentrations of BHB at DIM1 and DIM2 of group A (control) follow the same trend found by Belay et al. [
19]; these authors observed that milk BHB concentrations (obtained by FTIR technique) were higher between 11–61 DIM [
19]. Previously, Koeck et al. had already verified the same trend [
20]. This is probably due to the increase in dry matter intake and the gradual return to the positive energy balance as the days in milk progress [
21]. It is known that the manifestation of clinical ketosis is not necessarily associated with higher serum concentrations of BHB [
2] and that the lower capacity of dry matter intake, and as a consequence, lower supply of energy, as well as the process of adaptation of the papillae and rumen microbiome, may have influenced the greater degree of energy deficit in this phase (DIM1).
Although group C did not show any significant difference with the control group in DIM1, a similar profile of decrease in BHB was observed, with significant differences in DIM3. Unlike group B, whose distribution of LDA as well as their concomitant pathologies, were homogeneous (
p > 0.05) in DIM1 and DIM2, in group C, 60% of the pathologies occurred in DIM1 (
p < 0.001), with no significant differences to group A or group B. This suggests that although there may be an additive effect of disease association, this effect is largely dependent on the time that has elapsed since the beginning of lactation. The relation of pathologies associated with the beginning of lactation, and the position they occupy in a cause-effect relationship, are complex issues and not yet fully clarified [
1]. Most authors believe that cows with ketosis have an increased risk of developing other pathologies at the beginning of lactation [
1]. Effectively, Raboisson et al. summarized from multiple studies that the OR of hyperketonemic animals develop different pathologies: 5.4 (3.3–8.8) for clinical ketosis; 3.3 (2.6–4.3) for abomasum displacement; 1.8 (1.5–2.0) for metritis; 1.5 (1.2–1.9) for placental retention; 1.6 (1.2–2.1) for mastitis; 1.4 (1.3–1.6) for somatic cells count duplication; 2.0 (1.6–2.4) for laminitis, and 1.9 (1.6–2.3) for early culling [
22]. This same risk, according to McArt et al. [
23] and Suthar et al. [
2], increases with increasing blood BHB concentration. McArt et al. [
23] observed that cows diagnosed with ketosis from the third to the fifth day of lactation were 6.1 (95% CI = 2.3 to 16.0) times more likely to develop displacement of the abomasum than cows diagnosed after the first week. Ketosis probably induces hypoglycemia in multiparous cows [
24] and decreased time and rumination activity [
25]. Duffield et al. [
26] observed that some cows developed pathologies, such as DA, before being diagnosed with ketosis, reinforcing the hypothesis that the pathologies associated with ketosis may be more than the effects of this, the cause. The interaction between ketosis and the DA has been stated as bidirectional, proposing that they can both be a risk factor or a consequence of each other. Inclusively they are both multifactorial diseases and there are already described some risk factors that are common to both pathologies, mostly related to housing, management, and feeding adopted systems [
27]. Suthar et al. [
2] recorded both diseases at the same time and verified that they were both related to high levels of BHB, proving that they are both directly correlated with NEB. Duffield et al. [
26] hypothesized the explanation: the presence of common factors of hyperketonemia and DA with a similar causal etiologic is also related to a poor adaptive response at the onset of lactation conducting to NEB. This same theory has already been addressed regarding other postpartum diseases like mastitis and metritis [
28].
In our study, only 11 of the 25 cows with LDA had clinical ketosis in the same month that the pathology was diagnosed, which shows the complexity of demonstrating cause and effect. An interesting finding is the observed decrease of the BHB concentration from DIM1 to DIM2, DIM2 as the period with the higher number of LDA (14 LDA). Duffield et al. [
26], McArt et al. [
23] and Suthar et al. [
2] suggested that ketosis is a risk factor for LDA; It would be expected that the month with the higher number of diagnosed LDA (DIM2 in our study) presents high concentration of BHB, and the OR increases with increasing BHB concentration. In the present study, similar BHB concentrations of the animals that suffered from LDA on DIM2 were observed between DIM1 and DIM2 suggesting that, in these cases, ketosis contributed to LDA etio-pathophysiology. Nevertheless, BHB concentrations remained high in DIM2 for cows suffering LDA in DIM1 suggesting that hyperketonemia could be a consequence of LDA. These findings are in agreement with the bidirectional association between ketosis and LDA referred to in the Stengärde et al. study [
27].
We observed that the fat content in milk in the different groups was maximum at the first milk control, a control that mirrors the repercussions of the NEB that can be installed up to three weeks postpartum. Furthermore, and in agreement with Zhang et al. [
14], in our study, the maximum percentages of fat content in milk also correspond to the maximum concentrations of BHB in milk for most groups, as we can see through the higher fat content in group B than in group A. Additionally, moderate and higher correlations between fat content in milk and BHB in group B were observed in DIM1 and DM2, respectively. From the second or third milk control, after the NEB, we saw a less abrupt decrease in the fat content in milk in all groups.
During phases of energy deficit, such as the beginning of lactation, there are increased levels of fat content in milk [
15] and decreased levels of protein [
29]. The high concentrations of fat content in milk in periods of NEB correspond in more than 95% to triglycerides (TG) [
14] and are mainly due to the increased mobilization of lipid reserves [
15] that lead to the production of a large amount of BHB [
30] that induces increased synthesis of TG by mammary epithelial cells [
14].
The essential fatty acids to the synthesis of these TG come from the diet or the activity of the ruminal microbiota [
31]. In the mammary gland, there is also the “de novo” synthesis in the mammary epithelial cells. It is in the “de novo” synthesis that BHB, mainly from the butyric acid metabolization, gains special importance; in this way, in ruminants, BHB is one of the main precursors (originating about 50%) of the “de novo” synthesized fat in mammary epithelial cells [
14].
Regarding the protein content in milk, we observed that there was a decrease between DIM1 and DIM2 for groups A and E, contrary to what was observed in groups B, C, and D in which diseases occur in the first three months of lactation. The decrease in protein content in milk is a normal situation, since NEB worsens by that time, reducing milk protein synthesis. These data are in agreement with the conclusions of Gross et al. [
15] that protein evolves inversely to milk productivity and hence it is expected that, at the beginning of lactation when productivity is low, the maximum levels of protein in milk can be verified. In fact, a healthy animal reflects the expected start of lactation and therefore relatively low productivity that increases until the peak of lactation.
The non-decreasing in milk protein in groups B, C, and D, between DIM1 and DIM2, may be related to the lower protein supply in DIM1 due to the potential lower DMI that normally occurs during the manifestation of diseases (anorexia). A significant part of these groups developed some form of the disease during the first month. In some of these cases, there may still be less protein production in milk due to the worsening of NEB, since the increase in circulating non-esterified fatty acids may inhibit the production of somatotropin (growth hormone; Akers) [
32]. It should be noted that the amount of milk was not significantly reduced in these groups (except between groups B and E at DIM2) at the time of sample collection, which due to the normal lag between the occurrence of the disease and that the moment of milk sample collection indicates that this production is quickly resumed after treatment.
The amount of fat and protein reflects a cow’s energy status/condition [
15]. Toni et al. [
33] observed that cows with high F:P ratios at the beginning of lactation showed a higher incidence of various pathologies and were, as a result, more often early culled. Similar to the results found by Toni et al. [
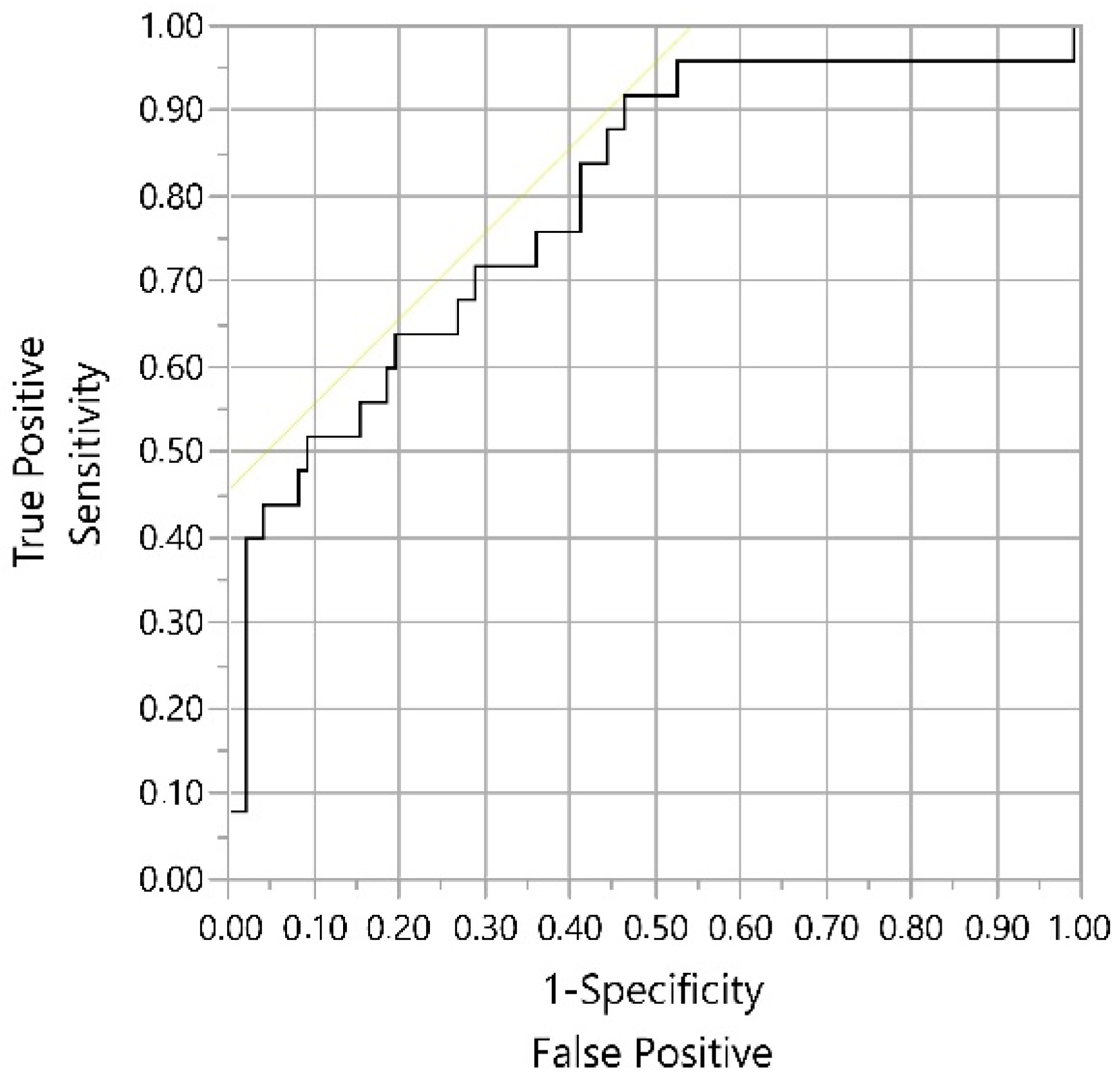
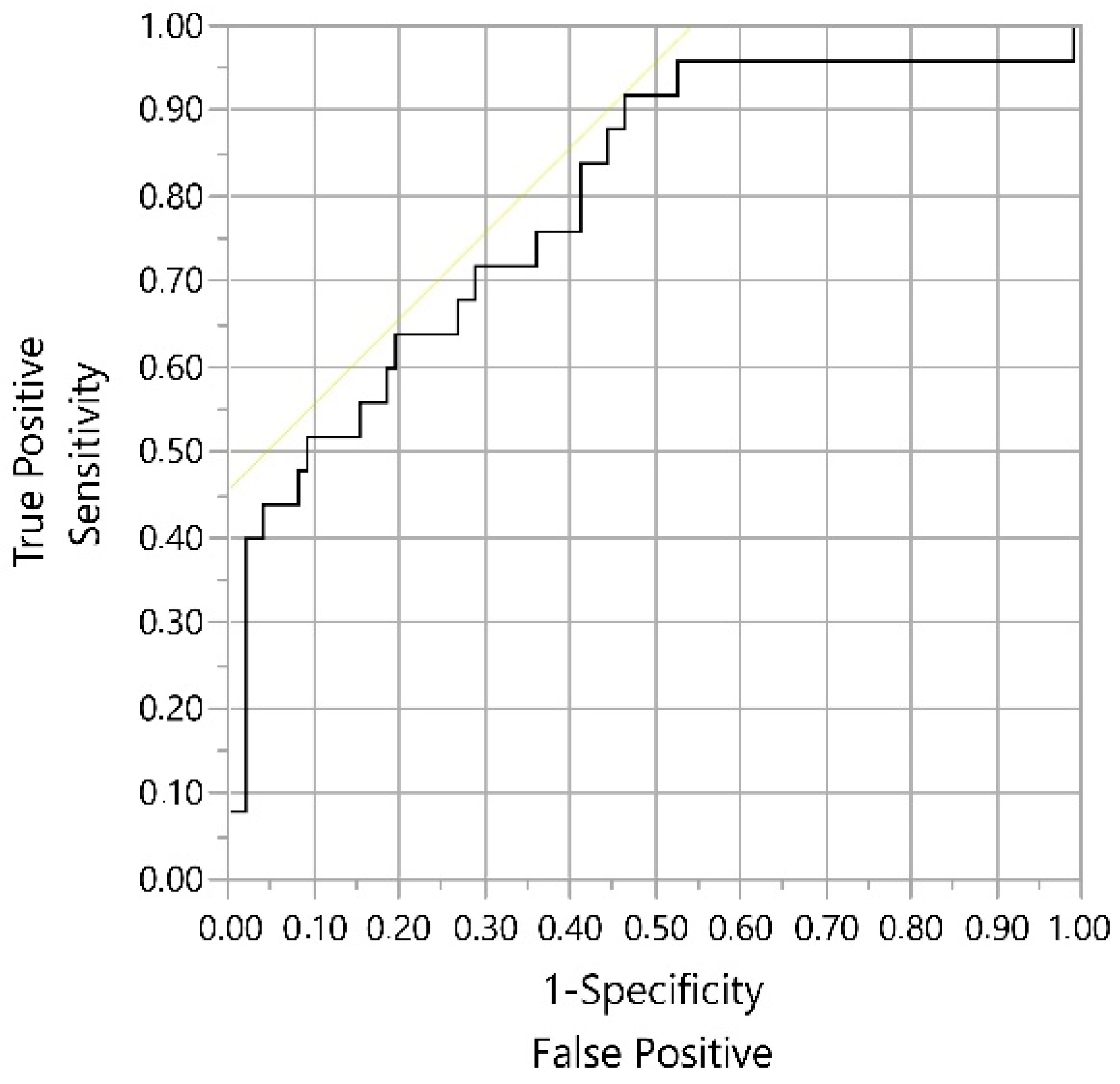
33], we observed that animals affected by LDA (group B) and various pathologies other than LDA (group C), presented higher F:P ratios in DIM1 than cows in the control group. Furthermore, we found that animals in group B with a F:P ratio ≥1.29 are about four to six times more likely to have BHB concentrations ≥0.14 mmol/L, that is, of having subclinical ketosis. These observations are accompanied by moderate and high correlations between the F:P ratio and the BHB for DIM1, in this same group. Zhang et al. [
14] observed, in vitro, that animals with high circulating concentrations of BHB had higher TG content, indicating that high concentrations of BHB increase TG synthesis by mammary epithelial cells, justifying why animals with ketosis generally have milk with higher fat content. The increase in the F:P ratio, therefore, coincides evidently with periods of NEB associated with increased mobilization of lipid reserves and consequently with the increase in circulating levels of BHB.
Our results indicate that the determination of the F:P ratio, starting at 1.29, is a useful tool in the management of dairy cattle health, allowing the estimation of subclinical ketosis associated with LDA and other postpartum pathologies with high sensitivity and reasonable specificity. This F:P ratio threshold agrees with the ≥1.3 threshold obtained by Denis-Robichaud et al. [
18] to predict hyperketonemia (serum BHB ≥ 1.4 mmol/L). Equally important, the present study emphasizes that in farms that offer, to their animals, diets with correctly balanced energy, cows with health problems (mainly LDA) are the ones most associated with the development of ketosis and most exposed to greater negative energy balance during the first two months of lactation, especially during the first month. Therefore, cows with high BHB and F:P ratio in milk in DIM1 should be preventively monitored for the diagnosis of the pathologies in question (groups B and C) in the first two months. This strategy allows a timely (earlier) diagnosis and respective treatment. Cows with diseases on the third, fourth, and fifth months of lactation do not have such a significant impact on the evaluated milk parameters (subclinical ketosis and NEB).





{kind=link}