1. Introduction
Despite being known of since the Mesopotamian era, about 3000 BCE, and despite the significant progress in novel medical technologies and the implementation of various control programs, rabies continues to pose a serious threat to human and animal health, remaining one of the most significant veterinary and public health concerns in the 21st century [
1,
2,
3]. Based on global estimates, there are more than 59,000 rabies-related deaths annually in 150 countries across all continents (excluding Antarctica). Most of these cases, about 95%, occur in African and Asian countries [
4], with 99% of cases being dog-mediated through bite exposures [
1,
5].
This disease, caused by a single-stranded RNA neurotropic virus of the family Rhabdoviridae and the genus Lyssavirus, is one of the most fatal worldwide, as almost all individuals who develop symptoms of rabies succumb to an acute progressive encephalitis [
6,
7]. However, mortality can be prevented through prompt and early post-exposure prophylaxis (PEP), which includes wound washing with water and soap, administration of rabies immunoglobulin, and vaccines following animal bites [
8,
9].
It is evident that mass vaccination of domestic dog populations is the key strategy to preventing human rabies [
9,
10,
11]. This strategy helped to eliminate dog rabies and reduce human cases in multiple countries in Europe and in North and Latin America [
6]. These results were attained thanks to one health approach that involves the collaboration of professionals in human, animal, and environmental health [
6].
Based on these experiences, a collaborative plan was established by the World Health Organization (WHO), the Food and Agriculture Organization (FAO), the World Organization for Animal Health (WOAH), and the Global Alliance for Rabies Control (GARC) to achieve “zero human deaths from dog-mediated rabies by 2030” [
4].
Algeria has also adopted this strategy. In fact, a legislative panel was put in place to ensure mass vaccination of dog populations and the fight against free-roaming dogs [
12]. However, despite these measures, this neglected zoonosis is still spreading, resulting in approximately 15 deaths annually. In addition, approximately 120,000 animal bites are recorded every year, with dogs being the primary culprits [
13]. In 2019, 382 rabies cases were reported among dogs in the country [
14]. Interestingly, all these cases were concentrated in the northern region, with no reported cases (neither in animals nor humans) in the Sahara, located in the southern region of Algeria [
12]. These data highlight the necessity of reassessing the rabies prevention strategy in Algeria. One crucial aspect that seems to be lacking is public education about this disease. Enhancing the level of knowledge is likely to positively impact attitudes and practices, ultimately aiding in the fight against rabies [
15]. Similar findings have been reported in various public health studies focusing on knowledge, attitudes, and practices (KAP) in endemic countries [
8,
9,
10,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26]. However, there is limited information available on this topic in Algeria. Therefore, the present study was conducted to assess the KAP of Algerian students regarding this disease.
4. Discussion
The study evaluated rabies-related knowledge, attitudes, and practices among university students in the endemic region of Algeria, where rabies continues to persist and cause fatalities [
3,
29] despite being recognized as a major disease since 1984 and having legal measures in place in regard to its prevention since 1996 [
12,
30]. This area of study has often been overlooked, with no prior research having been conducted in the country. Therefore, the findings of this study are anticipated to offer fundamental insights into students’ knowledge in the endemic region which can be utilized in awareness initiatives to combat this lethal disease.
Overall, a medium level (63%) of knowledge was obtained in this study. This level appears to be higher than the knowledge levels reported among various communities in certain African and South Asian countries [
16,
26,
31,
32,
33,
34]. Higher rates were also documented among other cohorts such as dog owners in Ghana [
19], scholar students in Thailand [
35], and the population of the Amhara region in Ethiopia [
20]. Nevertheless, these results should be interpreted with caution considering the variations in the items and scales utilized.
Looking in more detail, if the respondents were highly aware of the endemicity of the disease in Algeria, its deadly nature, and the role of dogs as the main source for human cases, they were less knowledgeable regarding the other methods of its transmission, its clinical signs, and its prevention. The link between dogs and rabies is a common finding in almost all previous studies [
20,
24,
33]. This result is not surprising, knowing that 99% of human cases originated from a dog bite according to the World Health Organization (WHO) [
4]. The same observation was also reported in Algeria [
12]. Note that the name of rabies in the Arabic language (
Alkalab الكَلَبْ) is derived from dog (
Alkalb الكَلْبْ), which could explain the link between dogs and rabies among the respondents. However, the importance of other animals was overlooked in our study. A similar observation was also previously reported in Morocco [
24] and in Nepal [
21]. These findings suggest the need to sensitize the population about the risk that other animals could pose in the persistence of rabies, especially when considering that this disease is also common among cattle (bovine, ovine/caprine, equine), and cases were also reported among wild animals in Algeria [
12,
14].
Another missing aspect of the respondents regarding rabies is related to clinical signs. Indeed, while 72.9% of the respondents were aware that rabies could be transmitted by saliva, a considerable portion of 34% and 39.4% were unaware that a sudden change in attitude, excessive salivation, and the tendency to bite anything are a potential signs of rabies, respectively. In addition, 55.3% of them only knew that the disease is associated with nervous signs. These rates are far lower than the results previously reported in different African (Rwanda, Ethiopia, Senegal) and Asian (Nepal) countries [
8,
15,
20,
33,
36]. Contrarily, Awuni et al. [
19] reported a low level of knowledge of clinical signs in humans among dog owners in Ghana, while excessive salivation was known as a sign of rabies by only 38% of school children of South Bhutan in Thailand [
35] and 37% of the younger population in Pakistan [
16]. These results showed the fragmented information of the participants regarding clinical signs of rabies, suggesting the need to raise the level of knowledge by focusing on the items with the lowest level of correct responses.
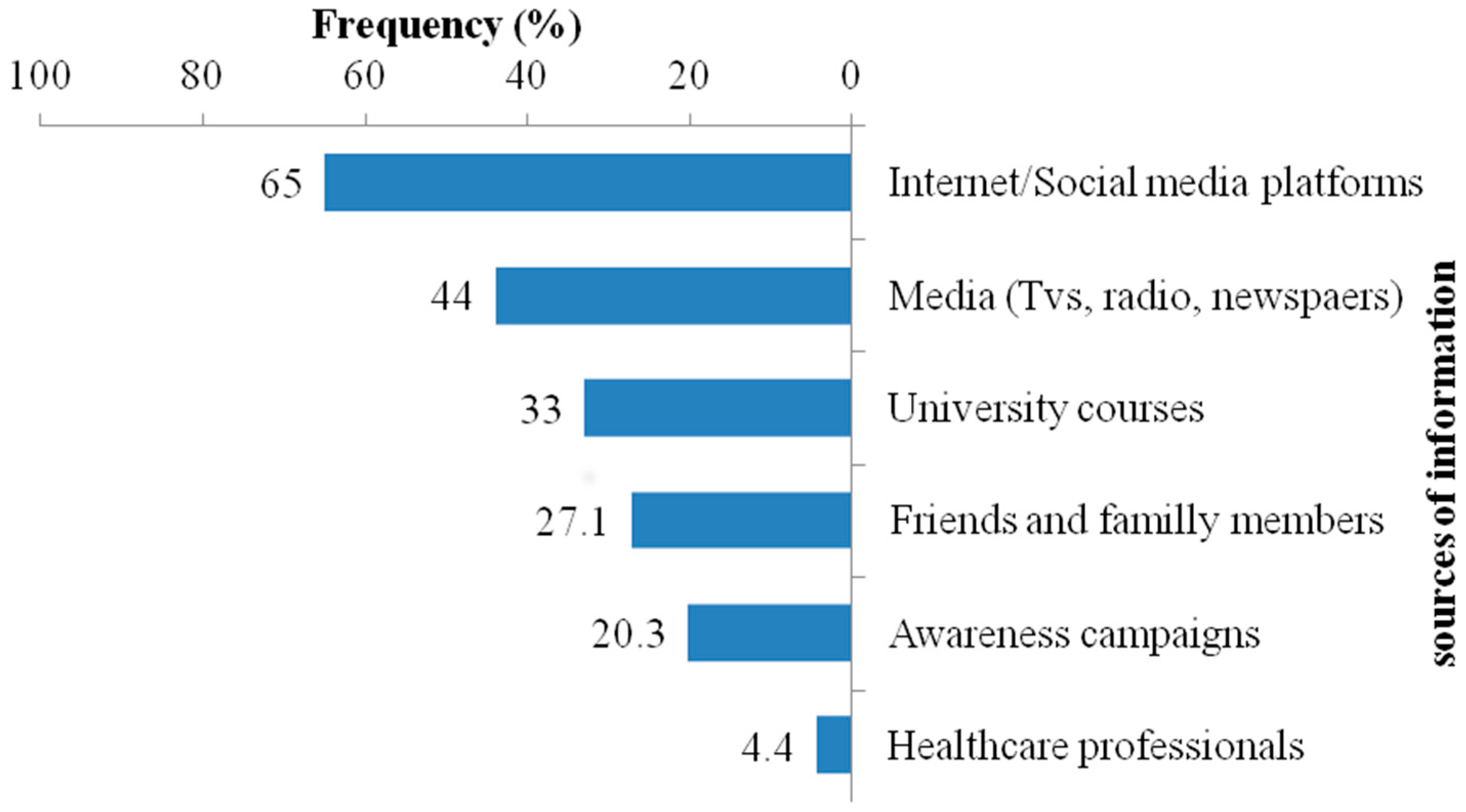
Contrary to findings in Ethiopia and Tanzania, where almost all household heads obtained information about rabies from informal sources [
23,
26], students in our study primarily mentioned the Internet/social media and traditional media as their sources of information. This variance could be attributed to age differences, as younger individuals are typically more engaged with social networking platforms compared to older individuals. However, a significant concern arises from the limited involvement of healthcare providers and awareness campaigns in disseminating information about the disease in our study. This result underscores the necessity of intensifying efforts to inform and educate the population in order to eradicate this disease.
The significant finding regarding attitude is that 59.2% of respondents believed that a dog that bites someone should be caught and killed regardless of its vaccination status. Similar views have been reported in various countries such as Rwanda [
8], Ethiopia [
20,
23], Morocco [
24], Nepal [
21], and Pakistan [
16,
37]. It is important to note that the appropriate measure in such situations is to place the dog in quarantine for 10 days to monitor any potential changes that could indicate or rule out rabies infection [
38].
Regarding students’ practices, it is apparent that only 35.5% were in favor of washing the wound with soap after a dog bite. While this practice was reported by 86% of school children and 60% among the rural community in Bangladesh, it was overlooked by the majority of the population in different countries. For instance, rates of 3.2% in Pakistan [
16], 8–30.7% in Ethiopia [
20,
23,
36], 20% in Zimbabwe [
34], and 30% in Uganda [
31] have been cited. More importantly, Tiwari et al. [
9], found that individuals with higher knowledge about rabies control practices were oppositely unaware of the importance of wound washing.
Of note, immediate wound washing with soap and water for a minimum of 15 min is the first step recommended by the World Health Organization (WHO) and national health authorities [
39] in post-exposure prophylaxis. This practice is associated with a 50% increase in the survival of affected animals and can reduce the development of rabies by one-third [
40]. Therefore, improving awareness about the importance of this basic and simplistic method could significantly reduce the risk of developing the disease. The subsequent essential step is the timely administration of rabies immunoglobulin and vaccines, both of which are available in Algeria (where two types of vaccines are available: a cell culture vaccine for immune-compromised individuals and a tissue vaccine produced from mice brains by the Pasteur Institute of Algeria, which is the most commonly used one) [
41].
The positive aspect of this study is that only a small percentage of the surveyed students indicated a preference for traditional healers in the event of a dog bite. Despite the lack of scientific evidence supporting their effectiveness, the use of these remedies is widespread in various countries [
16,
20,
21,
23,
36,
37]. Considering that this practice is accountable for a significant number of fatal rabies cases, increasing awareness about the risks associated with traditional healers is crucial for safeguarding people’s lives.
In this study, Medical (AOR: 2.723, CI 95%: 1.317–5.634) and Natural and Life (AOR:1.95, CI 95%: 1.205–3.155) Sciences education and male sex (AOR: 0.533, CI 95%: 0.336–0.845) were the only determinants that increased the level of knowledge. While the role of the field of study is understandable, as this subject may be included in the curriculum of medical and life sciences programs, the impact of sex requires further investigation. Although similar findings were reported by Bahiru et al. [
20] and Bihon et al. [
23] in Ethiopia and Sambo et al. [
17] in Tanzania, most studies have not identified a significant difference between males and females [
8,
19,
34,
37]. One possible explanation could be that females are less likely to experience dog bites [
41], leading them to place less importance on understanding this disease.
Furthermore, students in the medical sciences exhibited a higher likelihood of having a positive attitude (AOR: 2.306, CI 95%: 1.113–4.779) and good practice (AOR: 3.560, CI 95%: 1.632–7.769). These findings are significant given the crucial role these students play as future healthcare providers and sources of public information. In contrast, there should be increased focus on students from other disciplines, considering them a priority group in awareness initiatives aimed at enhancing rabies knowledge.
In contrast, students who had a history of dog bites and those involved in dog raising were surprisingly not associated with any of the levels of knowledge, attitude, and practice. For example, the positive impact of pet ownership on knowledge levels is a consistent finding in previous studies [
17,
20,
26,
34,
37]. A similar trend was also noted for attitude [
10] and practice [
17,
21] regarding this disease.
Regarding the history of dog bites, while the same result was shared by Dhakal et al. [
22], Bihon et al. [
23], and Hagos et al. [
26], Subedi et al. [
33] found that, even though a history of family exposure to dog bites was not associated with the level of knowledge, it could positively affect attitudes and practices in regard to rabies. Surprisingly, a study from China revealed that exposure to animals two or more times was associated with negative practices regarding rabies control [
18].
Another intriguing finding is the correlation between rural students (AOR: 1.842, CI 95%: 1.017–3.334), individuals involved in livestock breeding (AOR: 1.591, CI 95%: 1.040–2.434), and those exhibiting a high level of knowledge (AOR: 1.607, CI 95%: 1.052–2.456) with a positive attitude. Previous research has already established a link between rabies knowledge, attitude, and rural residency [
23], although conflicting results have also been reported [
20].
Taken together, while the results of Hagos et al. [
26] were surprisingly in favor of the association between knowledge, attitude, and practice, other researchers have also confirmed that the level of knowledge positively influences attitude, which in turn affects practice regarding rabies [
15,
25,
32]. These findings underscore the significance of educational programs aimed at enhancing knowledge levels, attitudes, and practices, which can be instrumental in the prevention strategy against this disease.
As with any KAP study, our study has its strengths and limitations. The most significant strength is related to the timing and exclusivity of this study. It is the first of its kind in Algeria to address rabies KAP. Additionally, it focused on university students, who are key in disseminating information to the general population. Moreover, this study was conducted just a few years before the WHO’s deadline to eliminate rabies by 2030. Therefore, its findings could assist in assessing preventive strategies and implementing any needed adjustments.
Regarding the limitations, the sampling method represents the most significant one. In fact, this study is conducted among students and cannot be generalized to the general population. It may also marginalize the most susceptible populations (habitant of rural communities, dog owners) that could provide more pertinent and detailed information regarding this disease. In addition, conducted through an online questionnaire, this study may have marginalized certain categories, particularly students with limited Internet access, especially those residing in rural areas. Another limitation is the influence of social desirability in this type of study. Respondents might have sought information online before answering to provide what they perceived as the ‘correct’ response. Additionally, they may have been inclined to report positive attitudes and good practices, a factor that is challenging to control in such studies.


 ,
, 

{kind=link}
{kind=link}