Simple Summary
Despite advances in puppy and kitten neonatology in recent years, mortality rates for these patients are still high, making the neonatal period a challenge for veterinarians and owners. Early recognition of newborns at risk allows for rapid intervention, increasing the chance of neonatal survival. To this end, an adequate clinical assessment is essential, which demands knowing the particularities of these patients and the reference parameters for age.
Abstract
Neonatal puppies and kittens have physiological and anatomical characteristics that differ from those of adult animals, which impacts the interpretation of physical examination and complementary tests. The veterinarian must be familiar with the clinical, laboratory, and imaging aspects observed in neonates. It is necessary to thoroughly evaluate the litter and the mother to notice the most subtle signs of illness and advise the owner to constantly monitor the newborns, quickly sending them to specialized care. This review describes how to perform clinical assessments of newborns systematically and recognize clinical signs of neonatal changes or affections in puppies and kittens.
1. Introduction
Neonatology is a medical area dedicated to newborn care, physiological particularities, and neonatal diseases. Currently, in dogs and cats, this period can be considered between 21 and 30 days of age, when organic systems undergo anatomophysiological maturation that gradually allows neonatal survival without maternal care [1,2]. The characteristics of neonates are completely different from adult animals, which can make the clinical evaluation of these patients challenging.
Newborn care involves multiple aspects (detailed clinical examination of the puppy together with the mother and litter), difficult management, handling, and diagnostic exploration, such as laboratory analyses (sample collection), radiographic, ultrasound, and electrocardiographic examinations, among others, as a consequence of patient size/weight. Therefore, recognizing clinical signs and distinguishing between healthy neonates and sick neonates is often challenging.
Failure in clinical assessment, diagnosis, and puppy and kitten early care is still common, contributing to high mortality rates globally [3,4,5,6,7,8,9]. For a long time, there was a perception that newborns demonstrated nonspecific clinical signs for different diseases with frequent sudden death, leading to thinking that immediate assistance was impossible. Currently, it is known that the clinical signs of a newborn at risk can be noticeable early and that sudden death is preceded by clinical signs (often suggestive/specific of some conditions) that were not identified before, mainly because of the absence of litter monitoring. To perceive clinical signs in newborns, it is necessary to carry out a thorough clinical assessment, knowledge of neonatal particularities, and constant examination of the litter, enabling early diagnosis and treatment that increases the chances of newborn survival.
In addition to the veterinary clinical assessment, the owner also plays an important role in observing clinical signs and identifying puppies at risk. They must be instructed on constant monitoring of the litter, which assessments should be carried out, and when to seek veterinary care.
Despite the importance of neonatology for veterinary medicine, few studies have been published on the physical examination of newborns, and physiological parameters during the neonatal period are incomplete, especially in kittens. The literature on neonatal hematological and biochemical parameters is scarce and mostly outdated or provides limited and insufficient data.
Therefore, knowledge of the neonatal clinical assessment of dogs and cats still has gaps. Understanding the particularities of physiological evolution and changes in clinical parameters during the neonatal period is crucial for the adequate clinical management of these patients. This review addresses how to perform clinical assessments and perceive clinical signs of neonatal disorders in puppies and kittens, as well as providing guidance for the development of future research.
2. Methods
The scientific articles used to support this review were selected from the following databases: PubMed/Medline, Scopus, Science Direct, and Google Scholar, based on the search for keywords: Puppy, kitten, physiology, neonatal health, clinical evaluation, vitality scores, neonatal diseases and malformations, neonatal sepsis, neonatal triad, weight, mortality, neonatal hematology and biochemistry, neonatal imaging, neonatal care. The average number of article occurrences for search terms related to the main themes of this manuscript was 400 for neonatal puppies and 300 for neonatal kittens. The selection of articles to be used in the review mainly followed the criteria of describing neonatal parameters during the first weeks of life, related to physiology, development, and the diagnosis of disorders.
3. Relevant Sections
3.1. Anamnesis
The clinical history of neonatal patients should be obtained by investigating several reproductive aspects related to the parents, pregnancy, parturition, environment, litter, and individual information about each newborn. It is important to highlight that the health of the parents, pregnancy development, and parturition directly influence fetal and neonatal health [2,10]. This means that if we look at the newborn’s diagnostic investigation from a broad point of view, it begins with information acquired “before conception.” The newborn’s health is not defined by circumstances that occur only during the neonatal period, being a continuation of parental genetics, maternal health, pregnancy, and the birth process itself, in addition to all other events that may occur during the neonatal period [11].
Table 1 demonstrates the first stage of the clinical approach and key points to be addressed during neonatal appointments. However, whenever newborns arrive for emergency care, the first step will be to evaluate vital parameters and carry out other procedures to stabilize the patient, followed by a complete medical history and anamnesis.

Table 1.
Key points about the clinical history and anamnesis of the neonatal patient.
3.2. Newborn Identification
The identification of neonates is essential to proceed with clinical appointments since newborns may have similar colored coats and confuse those evaluators. It is necessary to know which newborn the data from the physical examinations and complementary exams belong to or which newborn has already been examined and treated. For identification, colored ribbons (Figure 1), numbered cords around the newborn’s neck, or even bracelets on the limbs can be used.

Figure 1.
Identification of newborns with colored ribbons around their necks.
3.3. Physical Examination
After identifying and obtaining the clinical history of each newborn in the litter, a systematic physical examination must be conducted. It is essential to know neonatal physiology to correctly interpret the parameters, whose majority differ from those in adults and vary according to the week of age during the neonatal period. The basic materials and equipment needed for neonatal assessment are described in Table 2 and depicted in Figure 2.
Table 2.
Basic materials used in neonatal clinical assessment.
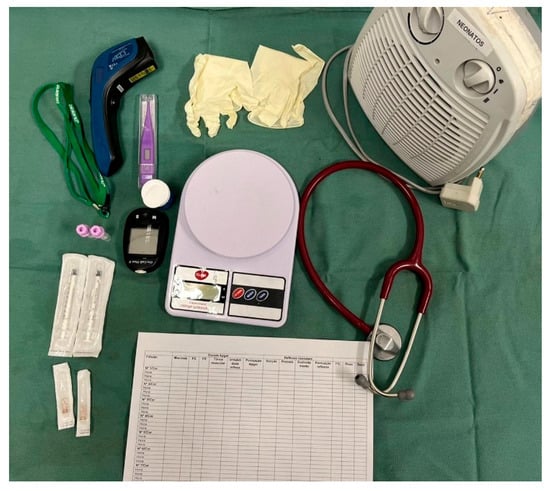
Figure 2.
Basic materials and equipment for neonatal clinical assessment.
During the neonatal period, it is necessary to examine not only the sick newborn but the entire litter and the mother. Although only the affected newborn is often taken for an appointment, the entire litter may be affected. It is also important to observe neonatal changes by comparing the sick sibling with a healthy sibling.
As neonatal affection can be a consequence of maternal disorder, it is essential to carry out a maternal clinical assessment and complementary exams if necessary, due to the possibility of nutritional imbalance, agalactia or hypogalactia, mastitis, abnormal maternal behavior, and changes in uterine status and vaginal secretion [5,6].
The neonatal physical examination must begin by inspecting the level of consciousness, posture, locomotion, and breathing pattern before manipulation since these parameters can change after touch. Next, the patient’s vital parameters must be assessed, but it must be noted that if the assessment occurs at the birth time, a modified Apgar score should be used. Following, the main neonatal reflexes, muscle tone, neonatal triad, and general physical examination must be performed, evaluating each region of the newborn’s body (Figure 3).
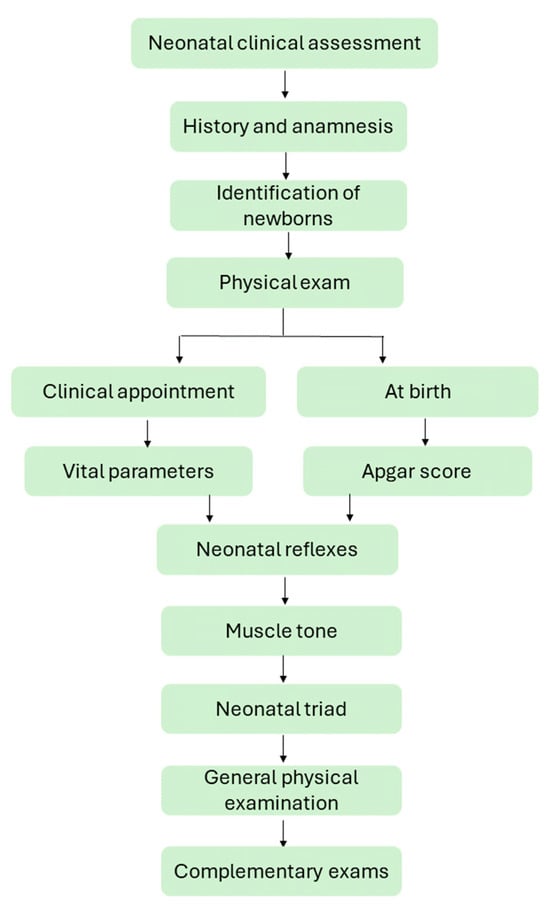
Figure 3.
Flowchart of neonatal clinical assessment.
3.3.1. Vital Parameters
Upon clinical appointment, the first step of the physical examination is to evaluate the newborn’s vital parameters, which include heart rate, respiratory rate, body temperature, and blood pressure. However, studies that describe vital parameters in newborns, for the most part, are focused on initial parameters after birth [12,13,14,15,16], with data on the evolution of these parameters over the weeks during the neonatal period being scarce.
Canine and feline neonates have immature cardiovascular systems, with low blood pressure (average of 50–70 mmHg) and low peripheral vascular resistance. To compensate for these aspects and maintain adequate blood perfusion, neonates have a higher heart rate (>200 bpm) and greater cardiac output, plasma volume, and central venous pressure than adults do (5.2 mmHg in neonatal puppies; there are no studies in neonatal kittens) [1,17,18,19,20]. The heart rate gradually decreases, from approximately 260 bpm at birth to 200 bpm in the fourth week of age in puppies (varying with animal size) [14,21] and from 280 bpm at birth to 200 bpm in kittens [16], approaching that of an adult around the seventh to eighth week. On the other hand, there is an increase in systolic blood pressure throughout the neonatal period, from 61 to 70 mmHg at birth to 139 mmHg in the fourth week of life in puppies, and from 50 mmHg at birth to 120 mmHg in the sixth week of life in kittens [1,18,19,20].
Heart rate can be assessed with the aid of a neonatal stethoscope (Figure 4) or vascular Doppler (Video S1) on the left side of the thorax or by visualizing the beats in the left thoracic region (visualization of precordial shock). Sometimes, neonates are vocalizing at the time of assessment, which interferes with auscultation; stimulating the sucking reflex by inserting a finger into the newborn’s mouth stops vocalizing, and the heartbeat becomes more audible (Figure 4). The canine and feline neonatal heart rates are described in Table 3. Measuring blood pressure in neonatal puppies (Figure 5) and kittens can be challenging in clinical practice because of the small size of the patients and restricted cuff size options. Therefore, this assessment is often limited to older neonates or those with a larger thoracic limb. For adequate blood pressure assessment, the cuff width must be 40% of the size of the thoracic limb [22,23]. However, in the first week of life, the thoracic limb of a feline or canine newborn (from a small breed) measures an average of 4 cm in diameter; on the other hand, the smallest veterinary cuff (n°1) is 2.5 cm wide. Therefore, there is a need for smaller veterinary cuffs for adequate neonatal assessment.
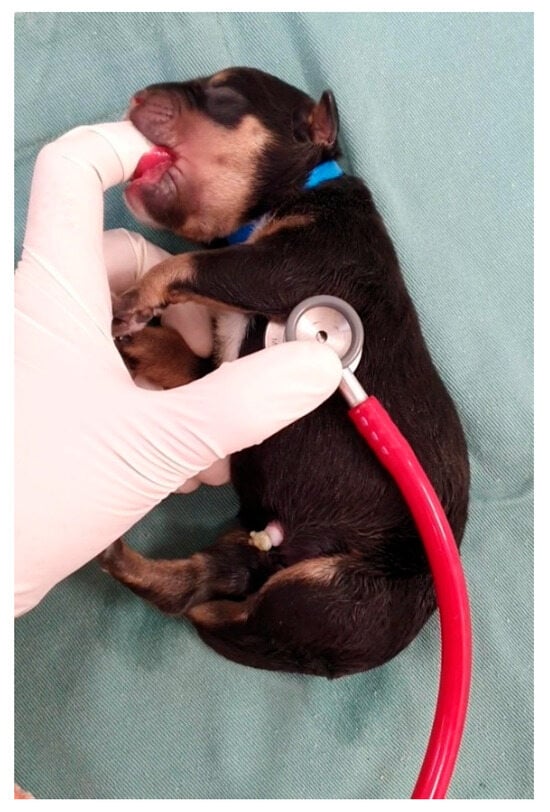
Figure 4.
Cardiac auscultation in a puppy.
Table 3.
Vital parameters of puppies and kittens during the neonatal period.

Figure 5.
Measurement of blood pressure in a neonatal puppy.
The control of the newborn’s respiratory function develops before birth, maturing during the postnatal period. Canine and feline neonates have structurally immature lungs, less expansion capacity of the thorax wall, immature carotid chemoreceptors, and high metabolism, which is why they are more predisposed to hypoxia. Volume and minute ventilation are lower, but the respiratory rate (Table 3) is greater than in adults [1,16,24,25]. Neonatal kittens have greater heart and respiratory rates than puppies. It is possible that the feline species present greater maturity of the cardiorespiratory system [16,26]. However, additional studies are needed to examine cardiorespiratory maturity in newborn cats compared to dogs. The respiratory rate is assessed by observing chest expansion movements, leaving the newborn on the assessment table (Video S2).
Due to hypothalamic immaturity, the temperature of neonatal puppies and kittens is lower than that of adult animals (Table 3), gradually increasing over time and approaching adult parameters in the fourth and sixth weeks of life in puppies and kittens, respectively, when complete maturity of the thermoregulatory system occurs [1]. The neonate’s temperature can be assessed rectally (using a digital thermometer with a soft tip) (Figure 6) or using an infrared thermometer pointed to the neonate’s abdomen (Figure 7).
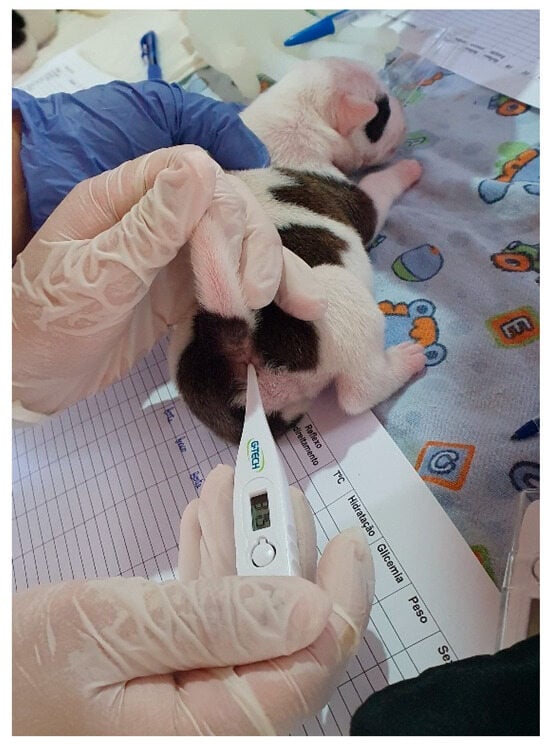
Figure 6.
Assessment of rectal temperature in a puppy.

Figure 7.
Assessment of temperature with an infrared thermometer.
3.3.2. At Birth: Modified Apgar Score
The Apgar score is a simple and reliable method of systematic assessment of vitality, neurological clinical depression, and viability at the time of birth. The principle of this score is to evaluate the immediate health of the newborn and provide quick assistance to critical patients or even evaluate the effectiveness of the provided assistance. The method was developed by Doctor Virginia Apgar after three years of observing newborn babies at the Sloane Hospital for Women, New York [14,27,28]. In veterinary medicine, the score has been described with modifications for several species, including dogs and cats [14,16,21].
Despite the evolution of studies with puppies and neonatal kittens, there is a discrepancy in published studies between these species, with fewer data available on kittens. For example, the modified Apgar score for dogs and its ability to predict survival was first proposed and described in the 2000s [14], after which several studies have been published over the years [13,15,29,30,31,32]. However, in kittens, the first proposed modified Apgar score was published in the 2020s [16], with a delay of almost 20 years of studies and important parameters for feline species. This resulted in dog parameters being used for cats in clinical practice for years, erroneously, since there are clear differences in parameters between these species [16]. Therefore, regarding the use of the Apgar score, differences between breeds and assessment of survival prognosis, more studies should be carried out in kittens.
The modified Apgar score for puppies and kittens (Table 4 and Table 5, respectively) is based on the evaluation of mucous membrane color, heart rate, respiratory rate, muscle tone, and reflex irritability (Videos S3 and S4), which are assigned grades of 0, 1 or 2, according to what was presented by the newborn, with the sum of the grades ranging from 0 to 10 [14,16,21].
Table 4.
Modified Apgar score for neonatal puppies (adapted from [14,21]).
Table 5.
Modified Apgar score for neonatal kittens (adapted from [16]).
Mucous color is assessed by visualizing the oral mucosa. Heart rate and respiratory rate can be measured with the aid of a stethoscope on the left side of the chest and by observing the expansion of the chest wall, respectively, as previously described. Muscle tone is determined with the newborn in the supine position on the palm of the hand, observing active movements of the limbs and body. The irritability reflex is assessed after a painful stimulus caused by pressing the interdigital space [14,16,21,33].
The interpretation of the score is evaluated according to the species and differences related to the body size characteristics of the breed (Table 6) [34]. Normal viability scores/without respiratory distress are considered ideal, with newborns being healthy and in clinical conditions favorable for survival. Moderate viability/moderate respiratory distress scores may indicate a possible need for resuscitation and neonatal monitoring, whereas neonates with poor viability/severe respiratory distress scores indicate a risk of imminent death. The vast majority of these patients experience prolonged asphyxia in the uterus and consequent prominent hypoxia at birth, indicating an emergency need for resuscitation [6,14,16,21,34].
Table 6.
Modified Apgar score and classification of neonatal viability of puppies (according to size) and kittens.
Neonates are susceptible to hypoxemia because of the need for high oxygen metabolism, lung immaturity, and the immaturity of carotid chemoreceptors [1]. Although they may present physiological hypoxemia shortly after birth, resulting in hypercapnia and mixed acidosis, this is transient [13,21]. However, prolonged and dystocic births can lead to pronounced asphyxia and severe hypoxia in newborns, leading to failure in respiratory adaptation and the need for intervention, with the Apgar score being an essential tool in the diagnosis and monitoring of these hypoxemic patients [14,21,33].
The modified Apgar score is a predictor of mortality; scores below 5 in small dogs and below 6 in medium and large dogs are strongly associated with the risk of death in the first 24 h, especially if these patients do not receive adequate assistance [34].
The modified Apgar score must be determined within the first five minutes after birth and repeated after 10 and 60 min to evaluate the clinical evolution of the newborn. It is important to remember that the score should not replace the complete physical examination of the patient in the first hours of life but rather assist in the quick classification of the newborn’s condition at birth [35].
3.3.3. Neonatal Reflexes
The main neurological reflexes (sucking, rooting response, and vestibular righting) (Videos S5 and S6) are present at birth and can be used to assess neonatal vitality. Healthy newborns must have strong reflexes, which allow breastfeeding and adequate development. On the other hand, any neonatal condition/disease that induces apathy and clinical depression culminates in reduced reflexes (weak vitality), failure to breastfeed, and progression to the neonatal triad (hypoglycemia, hypothermia, dehydration). In this way, the neonatal reflex score can be evaluated in cases where a neonatal alteration is suspected, favoring either early diagnosis and intervention or monitoring the clinical improvement of the newborn after the institution of treatment.
The sucking reflex must be assessed by inserting the tip of the examiner’s finger into the newborn’s mouth and observing the strength of the suction, which must be strong, presenting a vacuum during the evaluation. The rooting response reflex can be performed by placing the examiner’s hand close to the newborn’s face, who must immediately search for the mammary glands. The righting reflex is stimulated by placing the newborn in the supine position under a soft, heated surface. The expected response of this reflex corresponds to the straightening of the newborn’s body, with a quick return to the prone position. Each reflex receives a score of 0, 1, or 2 (absent, weak, or strong response, respectively) (Table 7), and the sum is used to indicate neonatal vitality. The score is evaluated as follows: 0–2, weak vitality; 3–4, moderate vitality; and 5–6, normal vitality [21,36].
Table 7.
Neonatal reflex scores for puppies and kittens (adapted from [21,33]).
In conjunction with the rooting response reflex, the newborn’s march reflex can be assessed (Video S7); however, due to its immaturity, the newborn moves by dragging its thorax and abdomen through swimming movements with its limbs. The objective of this reflex is to observe neonatal vigor in moving (crawling) in search of the mammary glands, determining its vitality. This reflex is present from birth, but the ability to support the body with the pelvic limbs occurs later, approximately 14 to 16 days of age, when the newborn begins to walk. Other neurological assessment reflexes included the magnum and landau. The magnum reflex is characterized by the rotation of the newborn’s neck to the side, with an expected extension of the ipsilateral thoracic and pelvic limbs, rotation of the head, and flexion of the contralateral limbs. The response is usually most evident in the thoracic limbs. The landau reflex (seal posture) is assessed by supporting the newborn in the prone position on the palm of the hand. The expected response is opisthotonus and extension of the pelvic limbs and tail. The magnum and landau reflexes are present until the third week of age [2,36], and the persistence of these reflexes denotes delayed neonatal neurological development.
3.3.4. Muscle Tone
Muscle tone, as previously described in the Apgar score, can be assessed with the newborn in the supine position on the palm of the hand, observing the movements of the limbs and body contortion (Video S8). The objective is to determine the vitality of the newborn, which may be absent, weak, or strong (see Table 4) [16,21]. A strong tone is essential for adequate movement and breastfeeding of the newborn. However, the movements of newborns are uncoordinated, demonstrating cerebellar immaturity. Tone can also be used for neurological assessment: by elevating the neonate by the mastoid region, a flexor posture of the body or pelvic limbs is observed until four to five days of age, which is later replaced by an extensor posture of the body or pelvic limbs, which lasts until the third or fourth week of age, followed by normotonia [36].
3.3.5. Assessment of the Neonatal Triad
During the neonatal period, puppies and kittens present immaturity in several organic systems, possessing unique characteristics that completely differ from those of adult animals. One of the main consequences of physiological immaturity is the greater risk of manifestation of the neonatal triad (hypothermia, hypoglycemia, and dehydration).
The neonatal triad is the most common clinical manifestation of any condition or change in the newborn. It is important to highlight that any neonatal disease can cause depression, apathy, a reduced sucking reflex, and a consequent reduction in milk intake, which can lead to the manifestation of this condition. Furthermore, the triad can occur due to management errors and maternal changes, such as agalactia, hypogalactia, or failure of maternal instinct. Assessment of the triad is essential at any neonatal appointment for puppies and kittens.
Hypothermia
Several physiological aspects are related to the predisposition of newborns to develop hypothermia, such as hypothalamic immaturity, reduced adipose tissue, poorly vasoconstriction mechanisms, inability of the tremor reflex in the first days of life, and a large surface/body mass ratio [1,2,37]. Therefore, newborns are considered ectothermic animals, requiring maternal or environmental heating to maintain a stable body temperature and active metabolism.
Moderate hypothermia can reduce metabolism, leading to lethargy, inappetence, and decreased neonatal reflexes. The newborn still tries to breastfeed, but the milk may not be properly digested due to reduced motility of the gastrointestinal tract (paralytic ileus), which can cause regurgitation, aspiration pneumonia, gas production, and gastrointestinal dilation [1,38]. For these reasons, hypothermic neonates should not be fed.
In severe hypothermia, neonatal clinical depression occurs, and newborns become extremely lethargic, interrupting attempts to breastfeed. There is a decrease in cardiorespiratory function (bradycardia and bradypnea), resulting in a risk of tissue hypoxia, acidosis, and death [38].
Hypoglycemia
Some physiological characteristics make neonates particularly susceptible to hypoglycemia. Due to liver immaturity, puppies and kittens are born with limited glycogen reserves and minimal capacity for gluconeogenesis. In puppies and kittens that are not breastfeeding, blood glucose levels can decline quickly as the ability to maintain normoglycemia during fasting is reduced. Liver reserves are completely depleted within 24 h; however, a rapid decline in glycemia may occur before this period in fragile, sick, premature, or low-birth-weight neonates [1,39].
Hypoglycemic newborns may manifest crying, weakness, apathy, decreased or absent sucking reflex, and interruption of breastfeeding, worsening their condition. Severe hypoglycemia can lead to bradycardia, seizures, coma, and death. Bradycardia occurs due to reduced metabolism and glucose supply to the myocardium. As the treatment is carried out and the blood glucose increases, the heart rate increases concomitantly [39].
Blood glucose should be measured with a portable glucometer, using a 24 or 26-gauge needle to collect a blood sample from the newborn’s digital pad (Figure 8), from the inside of the ear, or by collecting blood from the jugular vein.

Figure 8.
Blood collection from the neonatal puppy digital pad and blood glucose measurement.
The glycemic reference value in puppies and neonatal kittens is still controversial. In dogs, an old study demonstrated that concentrations such as 40 mg/dL [40] shortly after birth were considered normal. A more recent study reported an average concentration of 66 mg/dL in the umbilical cord [41]. However, another recent study demonstrated that at birth, the glycemia of neonatal dogs is related to maternal glycemia (approximately 90%) [42], and this cannot be considered a standard of normality for the species. Another study demonstrated that a glucose concentration <92 mg/dL during the first 24 hours of life is correlated with a greater risk of death during the first 21 days of life [43], indicating that concentrations lower than these are not considered normal. For example, a study demonstrated that the average blood glucose levels in newborn puppies aged one, four, and seven days were 106, 114, and 129 mg/dL, respectively [12]. With respect to glycemia during the first four weeks of age, one study reported a mean glycemic level of 125 mg/dL (range 106–182 mg/dL) in 349 healthy neonatal dogs [44]. Thus, neonatal normoglycemia in dogs can be considered to be between 90 and 200 mg/dL [39]. A glucose concentration <90 mg/dL indicates hypoglycemia [39,43]. Neonatal hypoglycemia can be characterized as mild (<90 to 70 mg/dL), moderate (<70 mg/dL to 40 mg/dL), or severe (<40 mg/dL) [39].
In neonatal kittens, one study demonstrated that the mean blood glucose at birth (eutocic parturition) was 68 mg/dL (ranging from 26 to 151 mg/dL) [16], but possibly, in the same way as in puppies, glycemia at birth may be related to maternal glycemia. Authors suggest that a blood glucose concentration <50 mg/dL in kittens up to two weeks after birth is abnormal, especially when accompanied by clinical signs [37,45]. In the literature, a range of 75 to 154 mg/dL on the second day after birth is considered normal [45]. More studies are needed to evaluate the average blood glucose levels of kittens over time during the neonatal period.
Dehydration
Newborn puppies and kittens are more susceptible to dehydration than adult animals, mainly due to renal immaturity, with a lower water conservation capacity. The puppy neonatal kidney is functionally characterized by a low glomerular filtration rate, renal plasma flow, filtration fraction, depressed reabsorption of aminoacids and phosphate, and low concentrating ability [46,47,48]. In the literature, information concerning the renal physiology of neonatal kittens is lacking. Furthermore, other physiological characteristics, such as a higher concentration of body water, a large surface area/body mass ratio, and greater loss of fluids due to skin immaturity or a thin layer of keratin, increase the predisposition of newborns to dehydration [1,2]. Dehydrated puppies can progress to hypovolemia, hypotension, shock, and death.
It can be challenging to assess hydration status in canine and feline neonates. Due to the physiological immaturity of the skin, lower subcutaneous fat, and higher concentration of body water, skin turgor is not developed as in adults and is not a reliable assessment in neonates. The color of mucous membranes can be used to assess hydration; the dark red color is indicative of dehydration in newborns [49,50]. Neonatal dehydration can be assessed subjectively by the urine color, which in newborns is very diluted with no visible color [6,10,50]. Shades of yellow suggest dehydration; the darker the urine is, the more dehydrated the newborn is. A gentle manipulation of the genitalia with a damp cotton pad stimulates urination and evaluation of urine color (Figure 9). Furthermore, urinary density can be evaluated using a refractometer, where a value > 1.017 is considered an indication of dehydration. As the kidney is not able to concentrate urine effectively, the specific gravity of urine gives results when there is already possible severe dehydration [1,2,50].

Figure 9.
Differences in urine color. (A) Normohydrated neonate whose urine color was close to transparent. (B) Dehydration of the neonate (dark yellow urine).
Other subjective methods of assessing dehydration include laboratory parameters such as hematocrit and total protein. The hemoconcentration is an indication of dehydration. Hemograms must be evaluated according to the normal parameters of the neonatal period.
After evaluation of temperature, blood glucose, and hydration, a physical examination should proceed. However, if the neonate is diagnosed with a triad, it is essential first to stabilize the newborn and then continue the diagnostic investigation.
3.3.6. General Physical Examination
To identify puppies and kitten neonates at risk, each part of the newborn’s body must be carefully analyzed, such as the head, chest, abdomen, limbs, tail, skin, anus, and genitals (Figure 10), in search of possible changes.

Figure 10.
Regions to be evaluated in the systematic physical examination of the newborn.
Head
In the head region, we must evaluate the shape, size, symmetry, and presence of the fontanelle, ears, eyelids, eyes, oral and nasal cavity, and lymph nodes since each region can demonstrate neonatal changes that often go unnoticed.
- Shape/size/symmetry: changes such as macrocephaly can be a clinical sign of hydrocephalus (Figure 11), a common malformation in neonatal puppies and kittens, especially in brachycephalic breeds. Hydrocephalus can cause neurological dysfunction, such as seizures, which in newborns can be identified by generalized muscle rigidity (most commonly observed) (Video S9) or pedaling movements (Video S10). Cranioschisis and exencephaly (Figure 12) are also frequently observed malformations;
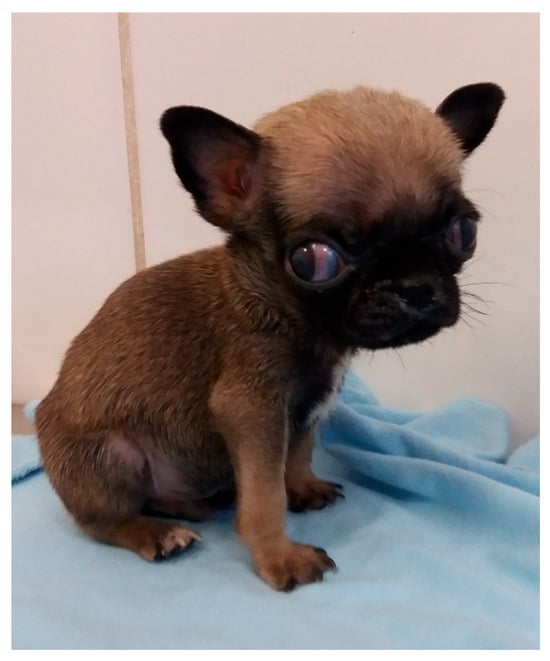 Figure 11. Macrocephaly and strabismus in a neonatal puppy with hydrocephalus.
Figure 11. Macrocephaly and strabismus in a neonatal puppy with hydrocephalus. Figure 12. Cranioschisis, exencephaly, and eyelid coloboma in a neonatal puppy.
Figure 12. Cranioschisis, exencephaly, and eyelid coloboma in a neonatal puppy. - Fontanelle: the skull of the newborn must be palpated to assess the presence of a fontanelle (nonclosure of bone fissures) (Figure 13). Some newborns may have an open fontanel at birth; however, this should close within the first few days of birth. A persistent fontanelle may also be a clinical sign of hydrocephalus and should be investigated;
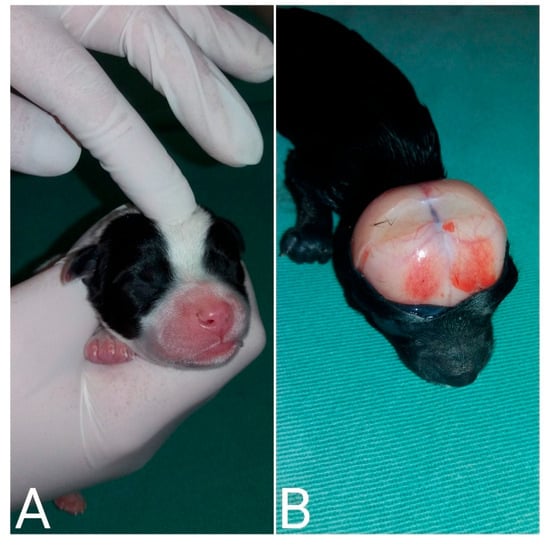 Figure 13. (A) Palpation of the skull to identify an open fontanelle. (B) Neonatal necropsy demonstrating the presence of a fontanelle (nonclosing of the bone fissures) in a puppy with hydrocephalus.
Figure 13. (A) Palpation of the skull to identify an open fontanelle. (B) Neonatal necropsy demonstrating the presence of a fontanelle (nonclosing of the bone fissures) in a puppy with hydrocephalus. - Ear and ear canal: neonates are born with a closed ear canal, which should open on average between 12 and 17 days of age [2]. One should always evaluate the shape, insertion, size, and presence of changes in the ear canal and ear, such as otitis and anotia (absence of one or both ears);
- Eyelids and eyes: neonates are born with their eyelids closed, beginning opening on average between eight to 12 days in kittens and 12 to 15 days in puppies [2,10]. The size and symmetry of the eyelids and eyeballs must be observed. A common condition in newborns is neonatal ophthalmia, characterized by infection of the conjunctiva and cornea before opening the eyelids, where there is an increase in volume in the ocular region due to the accumulation of purulent secretions (Figure 14). In some cases, this increase in volume may be subtle; therefore, it is important to carefully evaluate each newborn. Other frequent disorders in neonates are ventrolateral strabismus (common in hydrocephalus) (Figure 11), conjunctivitis, corneal ulcers, and malformations, such as palpebral coloboma (absence of eyelids) (Figure 12), microphthalmia and anophthalmia [51]. The pupillary light reflex begins between 10 and 16 days of age in puppies and between 5 and 14 days of age in kittens. The eyelid reflex begins between two and four days of age in puppies and between one and three days in kittens. The threat response starts between 10 days and 4 weeks in puppies and between 7 days and 4 weeks in kittens [2].
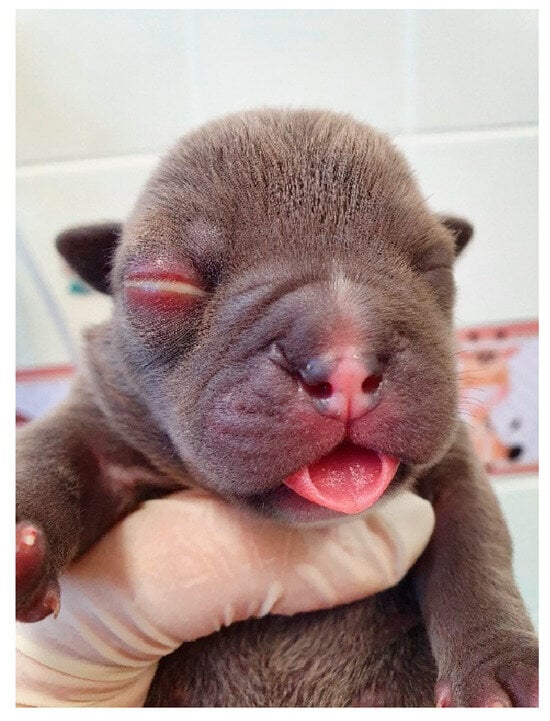 Figure 14. Neonatal ophthalmia in a puppy.
Figure 14. Neonatal ophthalmia in a puppy. - Oral cavity: abnormalities in the lip (cleft lip) (Figure 15), position and size of the tongue (such as macroglossia) (Figure 16), and changes in the hard and/or soft palate (cleft palate) (Figure 17) can be diagnosed [51,52]. Additionally, the color of the muzzle or mucous membranes must be evaluated, which in healthy newborns must be intense pink; other colors may indicate changes, such as cyanotic (e.g., perinatal asphyxia/hypoxia, heart disease, neonatal triad, sepsis), pale (e.g., anemia, hypotension, heart disease, septic shock, feline neonatal isoerythrolysis) (Figure 18), hyperemic (e.g., systemic bacterial infections/sepsis, dehydration), and jaundice (e.g., hemolytic anemia, feline neonatal isoerythrolysis, infections, liver changes). It is also important to evaluate neonatal dentition. Puppies and kittens are born edentulous, with tooth eruption starting from the third week of age. The dentition can be used to estimate the age of newborns.
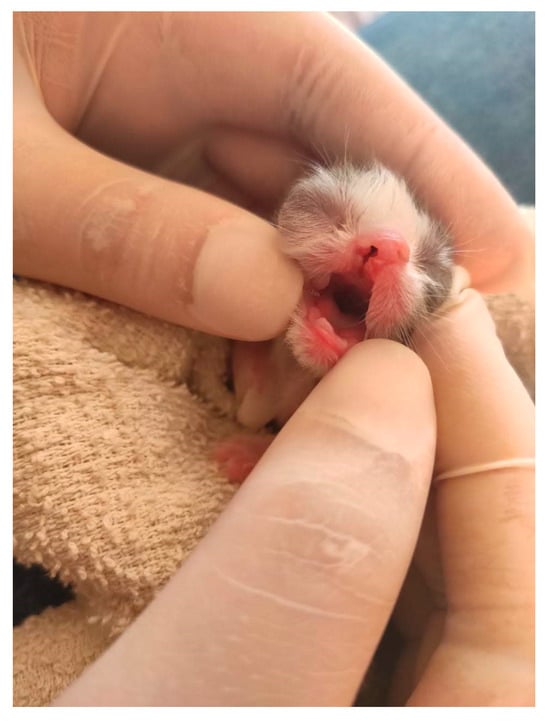 Figure 15. The cleft lip in a neonatal kitten.
Figure 15. The cleft lip in a neonatal kitten.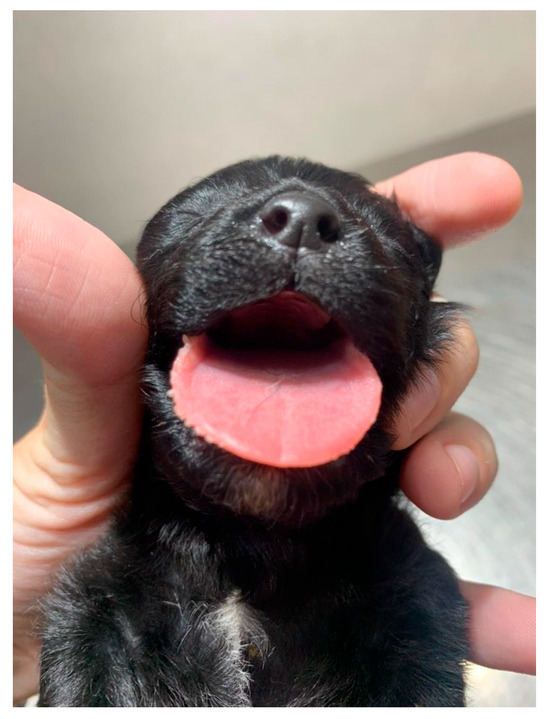 Figure 16. Macroglossia in a neonatal puppy.
Figure 16. Macroglossia in a neonatal puppy.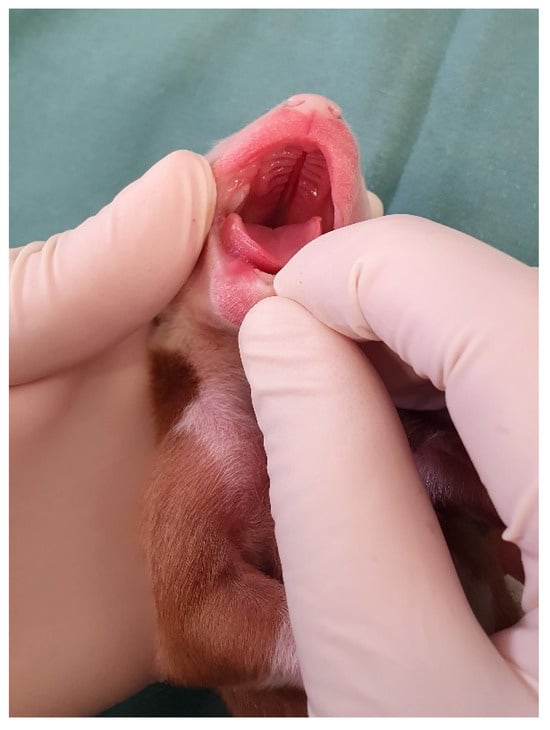 Figure 17. Cleft palate in a neonatal puppy.
Figure 17. Cleft palate in a neonatal puppy. Figure 18. Coloration of mucous membranes in newborn puppies. (A) Intense pink color; (B) cyanotic; and (C) pale.
Figure 18. Coloration of mucous membranes in newborn puppies. (A) Intense pink color; (B) cyanotic; and (C) pale. - Nasal cavity: observe the presence of nasal secretions, epistaxis, nostril stenosis (brachycephalic syndrome), obstructions, and cleft lip, which can extend to the nostril unilaterally or bilaterally.
- Lymph nodes: depending on the size/port of the newborn, the submandibular and popliteal lymph nodes are palpable. Enlargement of submandibular lymph nodes is common in juvenile cellulitis and submandibular abscesses. Occasionally, the inguinal lymph nodes can be visualized when they are enlarged.
Thorax
Thoracic evaluation is based on inspection of the breathing pattern, observation of asymmetries and malformations of the spine and rib cage, assessment of heart and respiratory rates, and cardiopulmonary auscultation to detect cardiac, pulmonary, esophageal, and tracheal disorders.
- Heart rate: As previously described, the heart rate of neonatal puppies should be between 200 and 260 bpm and that of kittens should be between 200 and 280 bpm. Bradycardia can be observed in several neonatal changes and conditions, including perinatal asphyxia/hypoxia, hypothermia, hypoglycemia, heart disease, systemic bacterial infections/sepsis, and septic shock [10,13,21].
- Respiratory rate and pattern: the presence of eupnea with a respiratory rate between 15 and 40 mpm in puppies and 40 and 180 mpm in kittens should be assessed. Neonates always breathe with their oral cavity closed; observing movements of the mouth opening to breathe indicates respiratory distress. Changes in respiratory patterns, such as dyspnea (Video S11), tachypnea, and bradypnea, occur in newborns with cardiorespiratory abnormalities, such as perinatal asphyxia/hypoxia, congenital cardiac anomalies, pulmonary edema, pneumonia, brachycephalic syndrome, prematurity, hypothermia, pectus excavatum, and septic shock [2,13,16].
- Cardiopulmonary auscultation: the presence of abnormal sounds, such as wheezing, crackles, stridor, cardiac arrhythmias, and murmurs, should be assessed.
- Asymmetries and malformations: abnormalities in the spine (e.g., scoliosis), cardiomegaly, tracheal hypoplasia, megaesophagus (Figure 19), lung changes, rib cage deformities (e.g., pectus excavatum (Figure 20), thoracoschisis), diaphragmatic hernia, among others [2,51].
 Figure 19. Contrast thorax X-ray demonstrating congenital megaesophagus secondary to the persistence of the right aortic arch in a neonatal puppy.
Figure 19. Contrast thorax X-ray demonstrating congenital megaesophagus secondary to the persistence of the right aortic arch in a neonatal puppy. Figure 20. Pectus excavatum in a neonatal puppy. Ventrodorsal narrowing is observed in the sternal region (arrow).
Figure 20. Pectus excavatum in a neonatal puppy. Ventrodorsal narrowing is observed in the sternal region (arrow).
Abdomen
Color changes, omphalitis, distension, hematomas, pustules, eviscerations, and malformations must be evaluated in the abdominal region.
- Color changes: the abdomen of a healthy newborn has a light pink color. The observation of a reddish (erythematous) color (Figure 21) strongly indicates systemic bacterial infection or neonatal sepsis, which must be investigated immediately with a complete blood count and microbiological culture. Bacterial infections are common in the neonatal period, with sepsis being the main cause of mortality in the first three weeks of life. Abdominal erythema occurs mainly due to vasodilation caused by systemic inflammatory response syndrome [44,53]. Other color changes commonly observed in the abdominal region are cyanotic, pale, and jaundiced, where the possible causes were previously described (see evaluation of the oral cavity);
 Figure 21. (A) Light pink abdominal color in a healthy neonate. (B) Abdominal/body erythema in a neonate with systemic bacterial infection.
Figure 21. (A) Light pink abdominal color in a healthy neonate. (B) Abdominal/body erythema in a neonate with systemic bacterial infection. - Omphalitis is an inflammation of the umbilical region, often caused by infection [2]. It is essential to know that at the time of birth, the umbilical stump has a whitish color that dries out over time and falls off between two and three days of age. Omphalitis can be observed as a hyperemic halo around the umbilical stump (Figure 22), violet coloration of the stump, edema in the region, and the presence of abscess or free purulent secretion. Commonly, the hyperemic halo can present subtly and often go unnoticed, reinforcing the importance of a thorough newborn evaluation in search of this sign. For the most part, a hyperemic halo is a sign of systemic bacterial infection/neonatal sepsis and should be investigated early [44].
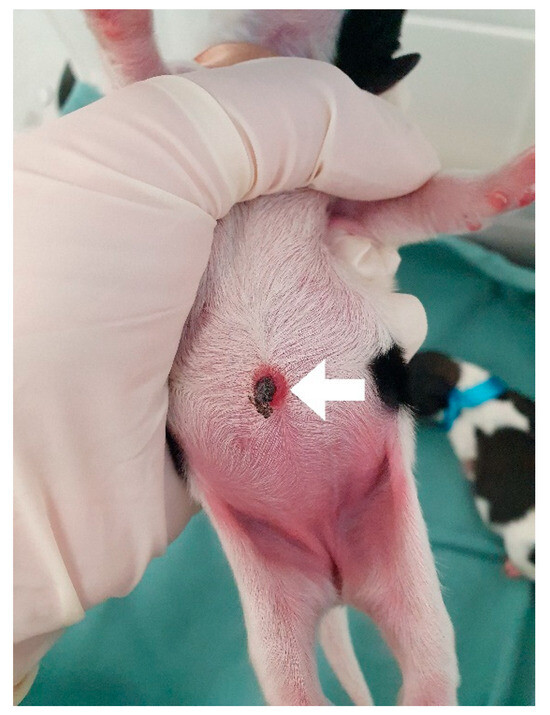 Figure 22. Omphalitis in a neonatal puppy with systemic bacterial infection. A hyperemic halo can be seen in the umbilical stump (arrow).
Figure 22. Omphalitis in a neonatal puppy with systemic bacterial infection. A hyperemic halo can be seen in the umbilical stump (arrow). - Abdominal distension: increased abdominal volume can be observed in some cases of neonatal changes and diseases, such as the presence of gas in the stomach or intestine, ascites, constipation/obstipation and consequent accumulation of feces, verminosis, and visceromegaly, among others. Abdominal palpation and imaging tests, such as ultrasound and abdominal radiography, can help to determine the underlying cause.
- Hematomas: the presence of abdominal hematomas often indicates hemostatic disorders, which can occur in neonatal sepsis and other infectious processes, liver diseases, neonatal hemorrhagic syndrome, toxic processes, and congenital changes, such as hemophilia and von Willebrand disease.
- Pustules: the presence of abdominal pustules (Figure 23) is commonly observed in infectious processes, mainly in bacterial skin infections (impetigo). In newborns, pustular dermatitis is often associated with immunodeficiency, especially in puppies and kittens that have not ingested colostrum, being often associated with systemic infection.
 Figure 23. Abdominal pustules in a neonatal puppy that did not ingest colostrum, presenting failure in passive immunity transfer and systemic bacterial infection.
Figure 23. Abdominal pustules in a neonatal puppy that did not ingest colostrum, presenting failure in passive immunity transfer and systemic bacterial infection. - Eviscerations and malformations: eviscerations can be observed in trauma (umbilical cord avulsion by the mother) and congenital defects, such as gastroschisis and omphalocele (Figure 24), which require immediate correction surgery. Other malformations may include segmental aplasia of the intestine, hernias, urinary system defects, and portosystemic shunts [51].
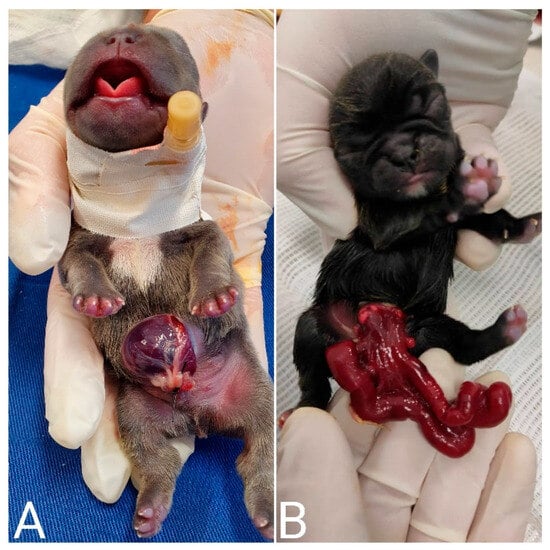 Figure 24. Omphalocele (A) and gastroschisis (B) in neonatal puppies. Both congenital defects are eviscerations; however, in omphalocele, the viscera are contained within a thin membrane, usually the peritoneum. In gastroschisis, the viscera are exposed.
Figure 24. Omphalocele (A) and gastroschisis (B) in neonatal puppies. Both congenital defects are eviscerations; however, in omphalocele, the viscera are contained within a thin membrane, usually the peritoneum. In gastroschisis, the viscera are exposed.
Genitalia and Anus
The evaluation of the genitalia and anus is based on the observation of urine and feces (color, appearance, volume, consistency) and the presence of malformations.
- Genital and urine assessment: to observe urine, urination stimulation must be carried out with gentle massage of the genitalia with the help of moistened cotton. At the time of urination, the color should be observed (important in the assessment of dehydration), as previously described (see assessment of the neonatal triad–dehydration), as well as the presence of hematuria, which is common in neonatal sepsis and feline neonatal isoerythrolysis. The neonatal urine output is 0.1 mL per 100 g of weight per hour, and oliguria and anuria are common in severe dehydration, septic shock, and malformations [2,10,54].
- Assessment of the anus and feces: to observe the feces, stimulation of defecation must be performed with gentle massage of the anus with the help of moistened cotton. The first feces expelled by the newborn are called meconium and are brownish. After starting breastfeeding, the newborn’s feces become yellowish. Color changes, such as a greenish or whitish color or the presence of live or digested blood, should be observed. Furthermore, the meconium and feces of a healthy newborn must be consistent and must not be pasty or diarrheal (Figure 25 and Figure 26). These changes are frequently associated with gastrointestinal disorders, such as bacterial, parasitic, or viral infections and nutritional or management errors. Diarrhea is the main clinical sign of parasitic and bacterial infection, occurring in approximately 93% of cases of neonatal sepsis in puppies. Meconium diarrhea is associated with neonatal systemic infection arising from intrauterine/maternal infection [44]. Constant diarrhea can also cause proctitis, resulting in perianal hyperemia. Another common change in the neonatal period is dry feces, culminating in constipation. This condition occurs mainly due to dehydration and is common in management errors of orphaned newborns when water is not administered between breastfeeding. For monitoring, it is important to know that newborns should defecate at least twice a day [2].
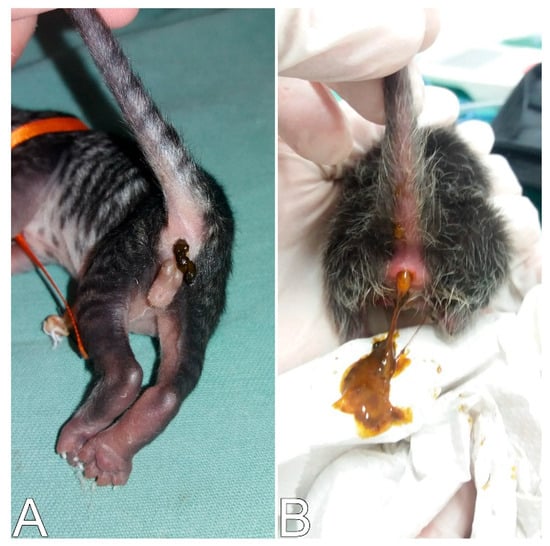 Figure 25. (A) Meconium consistent in a healthy neonatal kitten. (B) Meconium diarrhea in a neonatal kitten shortly after birth resulting from neonatal sepsis acquired in utero.
Figure 25. (A) Meconium consistent in a healthy neonatal kitten. (B) Meconium diarrhea in a neonatal kitten shortly after birth resulting from neonatal sepsis acquired in utero. Figure 26. (A) Consistent feces in a healthy neonatal puppy. (B) Diarrhea in a puppy resulting from neonatal sepsis.
Figure 26. (A) Consistent feces in a healthy neonatal puppy. (B) Diarrhea in a puppy resulting from neonatal sepsis. - Malformations: Anal atresia, rectovaginal fistula, vaginal atresia, hypospadias, among others, can commonly be observed. Atresias require immediate surgical correction.
Limbs and Tail
To evaluate the limbs and tail, the presence of trauma, injuries, and malformations must be observed.
- Traumas and lesions: traumas due to failure in maternal instinct, such as lesions and amputation of the limbs and tail, can occur in neonatal routine. Another observed change is cyanosis of the limb, digit, or tail extremities (Figure 27), which frequently occurs in neonatal sepsis and feline neonatal isoerythrolysis, which can progress to necrosis of the extremities (Figure 28) if not diagnosed and treated early. Cyanosis occurs as a result of hypoxia due to reduced blood supply to the extremities (due to systemic vasodilation and hypotension) associated with vasculitis caused by the infectious agent [44,53]. Another change observed in the limbs is an increase in volume, as in cases of abscesses and osteomyelitis.
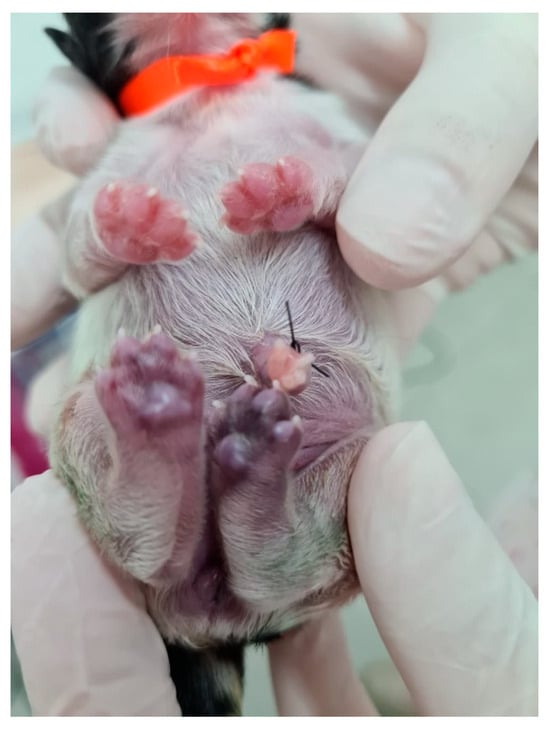 Figure 27. Cyanosis in the pelvic limbs in a neonatal puppy with sepsis.
Figure 27. Cyanosis in the pelvic limbs in a neonatal puppy with sepsis.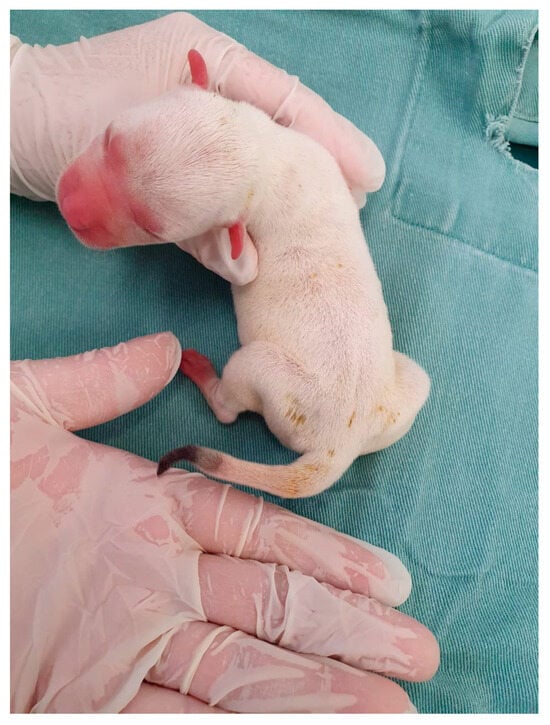 Figure 28. Tail tip necrosis in a neonatal puppy with sepsis.
Figure 28. Tail tip necrosis in a neonatal puppy with sepsis. - Malformations: in the limbs and tail, we can diagnose congenital defects, such as amelia (absence of limb), pygomyelia (increased number of limbs), meromyelia (absence of the end of limbs), swimmer cub syndrome (abduction of limbs) (Figure 29), equinovarus (twisted limb), polydactyly (larger number of digits), sidactyly (absence of digits), a twisted tail, and absence of the tail, among others.
 Figure 29. Swimming puppy syndrome in pelvic limbs.
Figure 29. Swimming puppy syndrome in pelvic limbs.
Skin
Skin evaluation is based on the observation of lesions that may indicate dermatopathies, the presence of ectoparasites, and congenital changes.
- Skin lesions: signs of bacterial, parasitic, fungal, and other skin diseases can be observed, such as alopecia, crusts, papules, pustules, abscesses, vesicles, erythema, erosion, scaling, dry, moist, or oily skin.
- Ectoparasites: assess the presence of fleas, ticks, lice, and larvae (myiasis) and carry out complementary tests to diagnose scabies.
- Congenital or genetic changes included aplasia cutis (absence of the formation of regions of skin/fur) (Figure 30), which is frequently observed in the head region; skin asthenia (hyperextensibility and skin fragility); juvenile cellulitis; alopecia due to color dilution; and ichthyosis, among others. In premature newborns, we can observe the absence of fur on the ends of the limbs, face, and tail (Figure 31) due to the shorter time of intrauterine development.
 Figure 30. Aplasia cutis in a neonatal puppy.
Figure 30. Aplasia cutis in a neonatal puppy. Figure 31. Absence of fur on the extremities of a premature neonatal kitten.
Figure 31. Absence of fur on the extremities of a premature neonatal kitten.
3.3.7. Neonatal Weighing
Neonatal weighing is one of the main newborn management strategies, essential for identifying newborns at risk. Steady weight gain is an indication of neonatal health and well-being. Healthy newborns who are breastfeeding adequately should gain weight every day, expecting a minimum weight gain of 5 to 10% daily [2,11,55], which doubles their weight in seven to 10 days. In puppies, the daily growth rate can vary according to the size of the breed: 5 to 7% for small breeds, 8 to 10% for medium breeds, and 5 to 9% for large/giant breeds [unpublished data].
Weight loss, or insufficient gain (<5%), is related to a breastfeeding problem (maternal agalactia/hypogalactia, failure in maternal care, absent or weak neonatal sucking, large litter, among others), management errors, or some neonatal disease, since any affection can lead to neonatal clinical depression, apathy, reduced sucking reflex and consequent reduction in milk intake, which will culminate in weight loss. Often, failure to gain weight occurs before the development of clinical signs of disease; thus, a newborn who is at risk can be identified early, and diagnosis and intervention can be carried out, which is essential for a greater chance of survival [11,55].
Although a weight loss of up to 10% within 24 h after birth is commonly described in the literature as physiological and tolerable in puppies, studies attempt to dispel this myth [4,41,43]. In fact, in healthy newborns, this weight loss is not observed in the neonatal routine. When this occurs, it is related to some change or disease, as described previously. According to Mila et al. (2017), negative growth rates during the first two days of life are linked to a greater risk of mortality in the first 21 days of life. The initial growth rate cutoff value that defines puppies at risk is −4%. Approximately 40% of puppies with retarded growth die during the neonatal period, whereas only 5% of puppies with adequate growth die. The absence of weight gain may suggest insufficient colostrum intake, which is essential for newborn puppies, both for maintaining caloric requirements and for the transfer of passive immunity [4,43]. Furthermore, a study demonstrated that the colostrum microbiota can vary according to the type of parturition, impacting the growth rate of the puppies. The colostrum of bitches and the meconium of puppies from vaginal birth and elective cesarean section demonstrated a significantly higher abundance of bacteria compared to emergency cesarean section. Consequently, puppies with greater microbiota presented greater weight gain in the first days of life [56].
The daily weight gain of newborns must be assessed using a small digital scale in grams (Figure 32). The weight must be recorded on evaluation sheets and can be easily carried out by tutors or breeders.
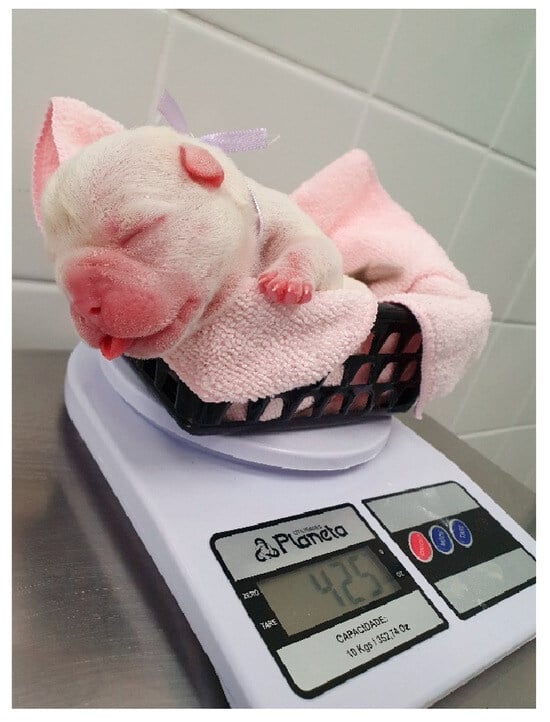
Figure 32.
Neonatal weighing on a small digital scale in grams.
A risk group for mortality is low-birth-weight newborns (Figure 33). These newborns suffered intrauterine growth restriction due to deprivation of adequate oxygenation and nutrition resulting from placental changes. They are characterized by being born at least 25% lighter than the average weight of their littermates or their breed. Consequently, they are physiologically more immature and susceptible to lower viability at birth, lower vitality scores, weak sucking reflex, immune deficits, lower hepatic glycogen stores, greater deficiency of the thermoregulatory system, and a higher risk of developing neonatal triad, fading syndrome, and infections [5,8,43].

Figure 33.
Low-birth-weight puppy (right) compared to his littermate (left).
For these reasons, weight is of great relevance in predicting neonatal mortality; more than 80% of puppies who die in the first 48 h of life (early mortality) are low-birth-weight newborns [43], and approximately 60% of low-birth-weight kittens do not survive weaning [2], especially if they do not have adequate assistance. Therefore, the identification of low-birth-weight newborns and the appropriate management of these patients are crucial for their survival. Birth weight can be analyzed according to each size due to the wide variation in body weight (Table 8). However, studies have shown that there are size variations between breeds [5,8] (Table 9).
Table 8.
Mean weight at birth of dogs and cats (adapted from [2]).
Table 9.
Mean birth weight by breed of dogs and cats (adapted from [5,8]).
Furthermore, weight limits were established for these at-risk newborns, namely, low birth weight (LBW) and very low birth weight (VLBW), where their classification depends on the species and race (Table 10 and Table 11). These two thresholds distinguish newborns at slightly higher risk and those at very high risk of death compared with normal birth weight (NBW) pups. Puppies with NBW have neonatal mortality of 4% (during the first 21 days of life); for LBW puppies, it is 9%; and for VLBW puppies, it is up to 55% [57]. Kittens with NBW present 4.5% mortality during the first two months of life, whereas those with LBW are 16.5%, and those with MLB are 50.9% [8].
Table 10.
Classification of newborn puppies according to birth weight [57].
Table 11.
Classification of newborn kittens according to birth weight [8].
These practical guidelines for measuring weight provide an easy tool for detecting and nursing puppies at increased risk of mortality. They may be relevant for breeders and veterinarians to objectively identify precocious puppies that require special attention, reducing the mortality rate [8].
Low birth weight in canines and felines still has a poorly understood and insufficiently investigated etiology. Due to the current scarcity of studies on risk factors and how to prevent them, measures to date have been limited to providing breastfeeding care and monitoring to improve the survival rates of these puppies and kittens [8]. More research is essential to study the etiology and medium- and long-term consequences of low birth weight.
3.3.8. Facts and Periods of Neonatal Development
For an appropriate clinical approach, veterinarians must be aware of the maturation time or development of the newborn’s systems or organs to identify the possible age of the newborn when this information is not available and to guide or resolve the doubts of tutors and breeders on monitoring the development of the litter. Table 12 shows the main facts of puppy and kitten neonatal development and the period in which they occur.
Table 12.
Neonatal development according to age (adapted from [2]).
3.3.9. The Role of the Owner in Identifying Newborns at Risk
It is important to instruct the owner to constantly evaluate their litters and when to consult a veterinarian if any abnormalities are observed. They must be instructed to monitor weight gain, stimulate urination and defecation to observe the color and consistency of excreta, observe the behavior of the litter and the mother, whether the puppies are suckling, milk the breasts to observe production and the appearance of the milk, assess the neonatal temperature with a digital or infrared thermometer, observe the respiratory pattern, and observe the color of the oral region, abdomen, umbilical region, and limb extremities.
Litter daily monitoring can ensure early identification of clinical signs of changes or affections. Table 13 shows the main risk signs that owners can observe, and based on these findings, the litter and mother can be referred for a veterinary clinical appointment.
Table 13.
What signs should owners observe to identify newborns at risk?
3.4. Complementary Exams
After the neonatal physical examination, additional tests, such as complete blood count, biochemistry, urine, coproparasitology, radiography, ultrasound, echocardiogram, electrocardiogram, blood gas analysis, and lactate, may be requested to aid in the diagnosis. Complementary exam results must be interpreted according to the newborn dogs’ and cats’ physiological characteristics and reference parameters. However, studies on the laboratory parameters of newborn puppies and kittens are limited; some of them are old, and updating is always necessary.
3.4.1. Laboratory Analyses
To perform exams, the newborn must be positioned under a heated surface to prevent hypothermia. Long periods of fasting are not possible in neonatal patients due to the risk of hypoglycemia.
Blood samples can be obtained from the jugular vein using 24- or 26-gauge needles coupled with 1 to 3 mL syringes. The blood volume of newborns is approximately 5 to 8 mL/100 g of body weight. The blood sample collected must be less than 1 mL/100 g of weight in 24 h. The minimum recommended laboratory parameters include blood glucose, hematocrit, total protein, and leukocyte count [2,55,58]. Physical restraint for collection can be carried out with the newborn in lateral or dorsal decubitus, with the front limbs close to the chest and abdomen and the neck and head extended. For collection, the authors prefer to insert the needle into the jugular vein in a cranio-caudal direction (Video S12).
Neonates have physiological particularities that reflect the interpretation of red blood cell count results. Considering the body’s compensatory response to physiological hypoxemia during the birth process, at birth, they have a higher hematocrit, polycythemia, macrocytosis, a higher concentration of reticulocytes, and polychromasia. However, the number of red blood cells begins to decrease from the third day of age due to the replacement of fetal red blood cells by neonatal red blood cells, culminating with a decrease in hematocrit, known as physiological anemia of the newborn [1,58]. It is important to note that the reference values for red blood cells and leukocytes differ among adult animals and change according to neonatal age, as well as according to species (Table 14 and Table 15).
In the biochemical profile, physiological particularities are also observed during the neonatal period (Table 16). The alanine aminotransferase (ALT) and total protein (mainly albumin) levels are reduced compared to adults due to liver immaturity. The levels of alkaline phosphatase (ALP) and gamma-glutamyl transpeptidase (GGTP) are 30 to 100 times greater than those in adults during the first 10 days of life. This elevation occurs after the ingestion of colostrum, which is rich in these enzymes, which allows them to be used as an indirect assessment of failure in the transfer of passive immunity. Urea, on the other hand, varies rapidly with food intake during the weeks of life but is still a more accurate indicator of kidney abnormalities than creatinine, which is reduced in newborns (compared to adults) due to its lower muscle mass [1,59]. Other tests commonly used to evaluate the clinical condition of the newborn at birth, such as blood gas analysis, oxygen saturation, troponin I, and lactate, are mainly performed in cases of perinatal asphyxia/hypoxia resulting from cases of dystocia, prolonged births, and cesarean sections (Table 17) [21,33].
Urine samples can be collected by stimulating the micturition reflex. The minimum urinalysis assessment includes the determination of specific density and urinary sediment. Normal urinary density is 1.006 to 1.017 until the eighth week of age. Physiological proteinuria and glycosuria may be present in the first few days of life due to renal immaturity and low glomerular filtration rate. Stool samples for coproparasitology can be obtained by stimulating the defecation reflex [1,2,33].
Table 14.
Mean, minimum, and maximum blood cell count parameters of neonatal puppies according to age (adapted from [58]).
Table 14.
Mean, minimum, and maximum blood cell count parameters of neonatal puppies according to age (adapted from [58]).
| Age (Weeks) | |||||
|---|---|---|---|---|---|
| Parameter | At Birth | 1 | 2 | 3 | 4 |
| Red blood cells (×106/µL) | 5.1 (4.7–5.6) | 4.6 (3.6–5.9) | 3.9 (3.4–4.4) | 3.8 (3.5–4.3) | 4.1 (3.6–4.9) |
| Hemoglobin (g/dL) | 15.2 (14.0–17.0) | 12.9 (10.4–17.5) | 10.0 (9.0–11.0) | 9.7 (8.6–11.6) | 9.5 (8.5–10.3) |
| Hematocrit (%) | 47.5 (45.0–52.5) | 40.5 (33.0–52.0) | 31.8 (29.0–34.0) | 31.7 (27.0–37.0) | 29.9 (27.0–33.5) |
| MCV (µ3) | 93.0 | 89.0 | 81.5 | 83.0 | 73.0 |
| MCHC (%) | 32.0 | 32.0 | 31.5 | 31.0 | 32.0 |
| Reticulocytes (%) | 6.5 (4.5–9.2) | 6.9 (3.8 a 15.2) | 6.7 (4.0–8.4) | 6.9 (5.0–9.0) | 5.8 (4.6–6.6) |
| Leukocytes (×103/µL) | 12.0 (6.8–18.4) | 14.1 (9.0–23.0) | 11.7 (8.1–15.1) | 11.2 (6.7–15.1) | 12.9 (8.5–16.4) |
| Neutrophils | 8.6 (4.4–15.8) | 7.4 (3.8–15.2) | 5.2 (3.2–10.4) | 5.1 (1.4–9.4) | 7.2 (3.7–12.8) |
| Lymphocytes | 1.9 (0.5–4.2) | 4.3 (1.3–9.4) | 3.8 (1.5–7.4) | 5.0 (2.1–10.1) | 4.5 (1.0–8.4) |
| Monocytes | 0.9 (0.2–2.2) | 1.1 (0.3–2.5) | 0.7 (0.2–1.4) | 0.7 (0.1–1.4) | 0.8 (0.3–1.5) |
| Eosinophils | 0.4 (0.0–1.3) | 0.8 (0.2–2.8) | 0.6 (0.08–1.8) | 0.3 (0.07–0.9) | 0.25 (0.0–0.7) |
| Basophils | 0.0 | 0.01 (0.0–0.2) | 0.0 | 0.0 | 0.01 (0.0–0.15) |
| Platelets (×103/µL) | 178–465 | 282–560 | 210–352 | 203–370 | 130–360 |
MCV = mean corpuscular volume; MCHC = mean corpuscular hemoglobin concentration.
Table 15.
Mean blood cell count parameters of neonatal kittens according to age (adapted from [60]).
Table 15.
Mean blood cell count parameters of neonatal kittens according to age (adapted from [60]).
| Age (Weeks) | |||
|---|---|---|---|
| Parameter | 0 to 2 | 2 to 4 | 4 to 6 |
| Red blood cells (×106/µL) | 5.29 ± 0.24 | 4.67 ± 0.10 | 5.89 ± 0.23 |
| Hemoglobin (g/dL) | 12.1 ± 0.6 | 8.7 ± 0.2 | 8.6 ± 0.3 |
| Hematocrit (%) | 35.3 ± 1.7 | 26.5 ± 0.8 | 27.1 ± 0.8 |
| MCV (µ3) | 67.4 ± 1.9 | 53.9 ± 1.2 | 45.6 ± 1.3 |
| MCHC (%) | 34.5 ± 0.8 | 33.0 ± 0.5 | 31.9 ± 0.6 |
| Reticulocytes (%) | 9.67 ± 0.57 | 15.31 ± 1.21 | 17.45± 1.37 |
| Leukocytes (×103/µL) | 5.96 ± 0.68 | 6.92 ± 0.77 | 9.57 ± 1.65 |
| Neutrophils | 3.73 ± 0.52 | 6.56 ± 0.59 | 6.41 ± 0.77 |
| Lymphocytes | 0.01 ± 0.01 | 0.02 ± 0.02 | 0.00 |
| Monocytes | 0.96 ± 0.43 | 1.40 ± 0.16 | 1.47 ± 0.25 |
| Eosinophils | 0.02 ± 0.01 | 0.00 | 0.00 |
MCV= mean corpuscular volume; MCHC= mean corpuscular hemoglobin concentration.
Table 16.
Minimum and maximum biochemical parameters of neonatal puppies and kittens according to age (adapted from [59,61]).
Table 16.
Minimum and maximum biochemical parameters of neonatal puppies and kittens according to age (adapted from [59,61]).
| Puppies | Kittens | |||||
|---|---|---|---|---|---|---|
| Parameter | 1–3 Days | 2 Weeks | 4 Weeks | 1 Day | 2 Weeks | 4 Weeks |
| Total bilirubin (mg/L) | 0.2–1.0 | 0.1–0.5 | 0.0–0.1 | 0.1–1.6 | 0.1–1.0 | 0.1–0.2 |
| ALT (IU/L) | 17–337 | 10–21 | 20–22 | 7–42 | 11–24 | 14–26 |
| AST (IU/L) | 45–194 | 10–40 | 14–23 | 75–263 | 8–48 | 12–24 |
| ALP (IU/L) | 618–8.760 | 176–541 | 135–201 | 1348–3715 | 68–269 | 90 -135 |
| GGTP (IU/L) | 163–3.558 | 4–77 | 2–7 | 0–9 | 0–3 | 0–3 |
| Urea | 23–37 | 15–23 | 10 -21 | 34–94 | 22–54 | 17–30 |
| Creatinine | 0.4–0.6 | 0.3–0.5 | 0.3–0.5 | 0.6–1.2 | 0.2–0.6 | 0.3–0.5 |
| Total protein (g/dL) | 3.4–5.2 | 3.6–4.4 | 3.9–4.2 | 3.9–5.8 | 4.0–5.2 | 4.6–5.2 |
| Albumin (g/dL) | 1.5–2.8 | 1.7–2.0 | 1.0–2.0 | 1.9–2.7 | 2.0–4.0 | 2.2–2.4 |
| Cholesterol (mg/dL) | 112–204 | 223–344 | 266–352 | 48–212 | 164–443 | 222–434 |
| Calcium (mg/dL) | 10.4–13.6 | 11.2–13.2 | 10.4–13.2 | 9.6–12.2 | 10.0–13.7 | 10.0–12.2 |
| Phosphorus (mg/dL) | 5.26–10.83 | 8.35–11.14 | 8.66–11.45 | 4.90–8.90 | 6.70–11.00 | 6.70–9.00 |
ALP = alkaline phosphatase; ALT = alanine aminotransferase; AST = aspartate aminotransferase; GGTP = gamma-glutamyl transpeptidase.
Table 17.
Mean, minimum, and maximum values of the parameters troponin I, venous blood gas analysis, lactate, and oxygen saturation of neonatal puppies at birth and 60 min later (adapted from [33]).
Table 17.
Mean, minimum, and maximum values of the parameters troponin I, venous blood gas analysis, lactate, and oxygen saturation of neonatal puppies at birth and 60 min later (adapted from [33]).
| Parameter | Time Point | Type of Parturition/Clinical Condition | ||
|---|---|---|---|---|
| Eutocia | Cesarean Section | Perinatal Asphyxia | ||
| Troponina I (ng/mL) | At birth 60 min after | 0.02 (<0.01–0.04) 0.01 (<0.01–0.03) | 0.05 (0.03–0.07) 0.05 (0.02–0.08) | 0.15 (0.11–0.25) 0.11 (0.07–0.20) |
| pH | At birth 60 min after | 7.1 (7.0–7.3) 7.2 (7.1–7.3) | 7.2 (7.1–7.3) 7.3 (7.2–7.3) | 7.1 (6.9–7.2) 7.3 (7.2–7.3) |
| pCO2 (mmHg) | At birth 60 min after | 43.2 (29.2–58.2) 46.8 (33.2–60.8) | 49.3 (39.0–59.9) 48.9 (45.7–52.5) | 64.4 (55.9–71.7) 52.8 (47.8–60.2) |
| pO2 (mmHg) | At birth 60 min after | 21.7 (13.0–36.0) 21.4 (17.0–35.0) | 13.7 (8.0–19.0) 14.7 (12.0–17.0) | 7.0 (5.0–9.0) 11.0 (10.0–12.0) |
| HCO3 (mmol/L) | At birth 60 min after | 16.5 (8.5–22.0) 21.7 (16.5–26.9) | 23.2 (19.8–27.1) 25.1 (23.0–26.5) | 25.7 (19.9–32.5) 27.5 (23.8–31.4) |
| TCO2 (mM) | At birth 60 min after | 18.0 (10.0–24.0) 23.4 (18.0–29.0) | 25.1 (21.0–29.0) 26.9 (25.0–28.0) | 28.2 (22.0–35.0) 29.4 (26.0–33.0) |
| Beecf (mmol/L) | At birth 60 min after | −12.5 (−23.0 to −6.0) −5.8 (−10.0 to −1.0) | −5.1 (−8.0 to −1.0) −1.7 (−4.0 to 0.0) | −4.2 (−13.0 to 4.0) 0.4 (−4.0 to 4.0) |
| Lactate (mg/dL) | At birth 60 min after | 2.3 (1.7–2.7) 1.8 (1.5–2.2) | 3.9 (2.3–5.5) 2.3 (1.8–3.2) | 4.8 (2.2–9.0) 2.1 (1.4–2.9) |
| SO2 (%) | At birth 60 min after | 31.4 (11.0–57.0) 33.2 (20.0–48.0) | 19.6 (6.0–36.0) 19.9 (15.0–30.0) | 8.6 (4.0–12.0) 14.0 (10.0–18.0) |
| Peripheral SO2 (%) | At birth 60 min after | 91.6 (65.0–99.0) 99.0 | 97.9 (94.0–96.0) 99.0 | 57.6 (48.0–74.0) 98.0 |
3.4.2. Imaging Exams
Radiographic Examination
Radiographic interpretation also has particularities in neonatal patients. Little bone mineralization and the small thickness of soft tissues interfere with the quality of ray penetration. A decrease in kilovoltage (kV) to half that used in adult animals has been described. The absence of costochondral mineralization, open growth plates in long bones, loss of abdominal details (due to lack of body fat), and a more opaque lung interstitium due to increased water content in the parenchyma, and often, the heart may appear relatively large in proportion to the thorax [10,25]. Therefore, when the veterinarian is not familiar with the physiological aspects of neonatal radiographs, we suggest that radiographs be taken of a healthy littermate, together with the affected neonate, as a way of comparing the physiological pattern and possible changes (Figure 34). Radiographic examination is commonly requested to identify congenital alterations, cardiopulmonary alterations, foreign bodies, traumas, and orthopedic alterations, among others.
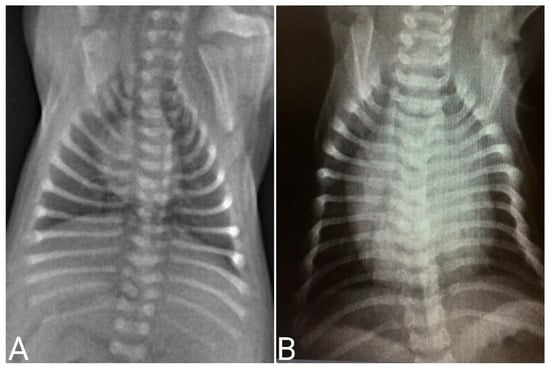
Figure 34.
Thorax radiographs in neonatal puppies. (A) Healthy neonate. (B) Neonate presenting cardiomegaly on radiographic examination due to congenital heart disease.
Ultrasound Examination
Ultrasonography of the abdominal cavity of neonatal patients is performed using 6- to 8-MHz transducers (Figure 35). The most frequently found artifacts are acoustic shadows due to the greater amount of food and gases in the digestive system, which can increase the difficulty of adequately visualizing organs such as the liver and other viscera. In newborns, a lack of a full urinary bladder and a greater occurrence of abdominal fluid are common. Oppositely to radiographic examination, the smaller amount of abdominal fat provides better image quality [2,24]. Ultrasound examination is often requested to identify congenital anomalies, foreign bodies, constipations, parasitic infections, and signs of infectious diseases.
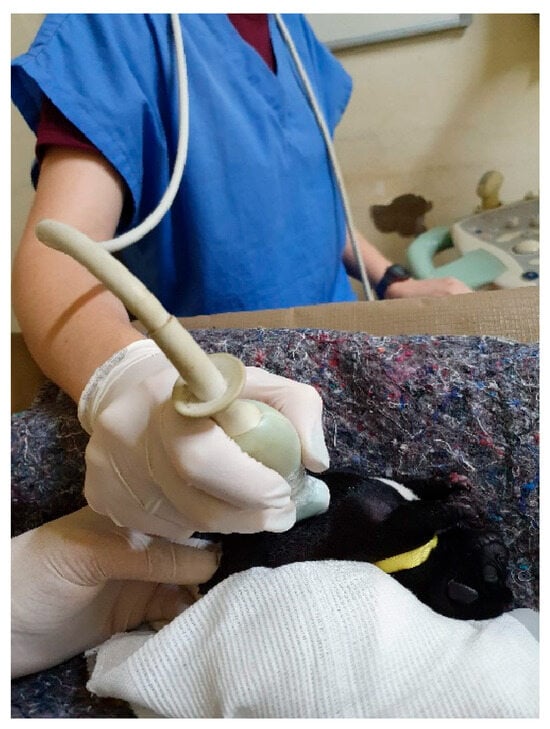
Figure 35.
Abdominal ultrasound in a neonatal puppy.
Echocardiographic Examination
For the echocardiographic examination (Figure 36), the newborn must be positioned in the lateral decubitus on a heated surface, and the ultrasound gel must also be previously heated to provide a more comfortable environment. The transducer is positioned on the left chest wall, and depending on its dimensions, images are obtained through several intercostal spaces simultaneously. Using pulsed Doppler, peak blood flow speeds are measured through the mitral, tricuspid, aortic, and pulmonary valves. Color flow Doppler imaging is of great value for observing and identifying flows and helps to position the cursor to measure peak flow velocity. The flow direction is identified based on their coding in red or blue, which is crucial for understanding the hemodynamics of the newborn’s small heart. With echocardiography, it is possible to diagnose several congenital heart diseases that affect canine and feline newborns.
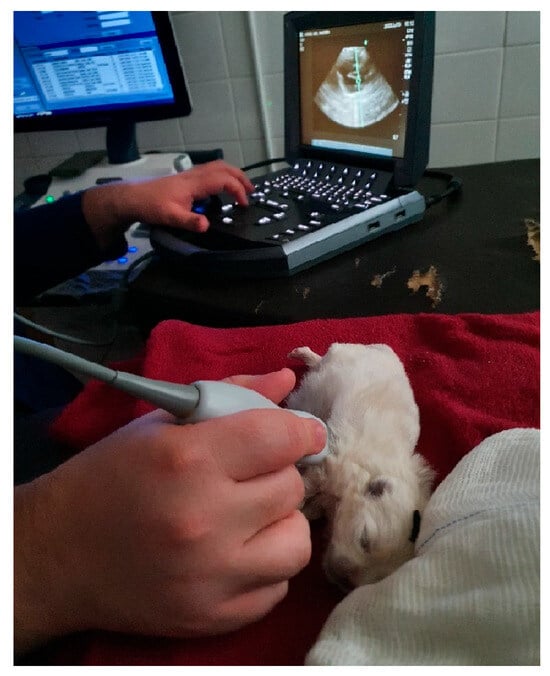
Figure 36.
Echocardiogram in a neonatal puppy.
Electrocardiographic Examination
With an electrocardiogram (Figure 37), it is possible to diagnose cardiac arrhythmias and/or electrical conduction disorders, being a practical method, and its use is viable in the neonatal period. To perform this exam, the newborn must be positioned in the right lateral decubitus position on a soft, heated surface, and the electrodes must be placed above the elbow and knee joints. It is advisable to wait until the newborn settles in and thus carry out the electrocardiographic examination calmly without much interference at baseline. During the first 30 days of life, variations in the amplitudes of the electrocardiographic waves Q, R, and S, changes in the orientation of the electrical axis, and in the R/S ratio are observed in puppies and kittens. Such changes demonstrate that during the first month of a newborn’s life, there is a change in the predominance of the right ventricle over the left ventricle [20,26]. Regarding the influence of the type of delivery, a study demonstrated that during the first 35 days of life, newborn puppies from emergency cesarean sections had lower heart rate variability than newborns from eutocic birth, with consequent delays in the autonomic influence on the heart. Concluding that the type of birth must be considered when evaluating the activity of the autonomic nervous system in newborns [20].

Figure 37.
Electrocardiogram in a neonatal puppy.
In small animal neonatology, reference standards for some complementary exams may not be available yet, providing a vast field for new research. It is important to emphasize that despite the various neonatal particularities, complementary exams are feasible for these patients and should be carried out when necessary.
4. Conclusions
Dogs and cats are altricial species, immature and dependent on the mother to survive the neonatal period. Several organic systems are under development, making the clinical assessment of neonatal patients different from adult animals in clinical, laboratory, and imaging. Veterinarians must be familiar with the physiological, anatomical, hematological, and biochemical neonates’ characteristics, recognizing sick patients and providing necessary assistance. Despite some limitations, the clinical examination of newborns can be effectively performed and should not be neglected. In general, to recognize a newborn at risk, it is necessary to carefully and constantly monitor the litter and the mother. Knowing the key points of healthy newborns will help in recognizing the sick ones: Healthy newborns have strong reflexes and muscle tone; continually gain weight; have consistent stools and defecate at least twice a day; have light yellow or transparent urine; after breastfeeding, they remain resting and do not vocalize constantly; newborns breathe with their mouth closed and have a regular breathing pattern; have an umbilical region free of erythema or purulent secretion; and have a pinkish body color.
5. Future Directions
Clinical, laboratory, and imaging parameters of neonatal puppies and kittens continue to be investigated. Data on the evolution of reference parameters over weeks of life are scarce, especially in kittens. Furthermore, to interpret what is normal in newborns, some physiological aspects still need to be characterized. For example, in the puppy, the neonatal kidney is morphologically and functionally immature; nephrogenesis continues for at least two weeks after birth [46]. However, there is a lack of information about nephrogenesis in cats. Consequently, there are only assumptions about the renal structure of feline newborns and some parameters, such as urine-specific gravity [1].
To fill in the gaps regarding physiology and normality parameters, more studies are needed. The main research needs are related to the maturity of systems, such as cardiovascular, respiratory, urinary, and immune systems, and the evolution of physical examination reference data during the neonatal period since most of them are focused on the moment after birth, such as heart rate, respiratory rate, blood pressure, blood glucose, temperature, and hydration. Updating hematological and biochemical parameters during the neonatal period is also necessary; some studies are old, and others are limited, with a lack of lymphocyte, eosinophil, monocyte, platelet, GGT, sodium, potassium, calcium, or phosphorus counts [58,60,62,63] or evaluating parameters only from 16 days of age [64]. Additionally, possible variations in the values of these exams between small, medium, large, and giant dogs should be investigated.
Studies on the measurements and aspects of imaging exams in newborns and their variations by race are essential. There are frequent doubts among clinicians about what would be normal or abnormal when evaluating neonatal radiographs, ultrasounds, or echocardiograms of puppies and kittens.
Knowing the reference parameters and how to carry out clinical assessment on the basis of specific studies is crucial for determining the appropriate time to initiate prophylactic and therapeutic approaches, impacting the reduction in neonatal mortality rates.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ani14233417/s1, Video S1. Assessment of heart rate in a neonatal puppy with vascular Doppler. Video S2. Assessment of the respiratory rate in a neonatal kitten. Video S3. Apgar score in neonatal puppy. Video S4. Apgar score in a neonatal kitten. Video S5. Sucking, breast seeking and vestibular righting reflexes in a neonatal puppy. Video S6. Sucking, breast seeking and vestibular righting reflexes in a neonatal kitten. Video S7. March reflex together with the newborn’s seeking reflex. Video S8. Muscle tone in a neonatal kitten. Video S9. Convulsion in a neonatal puppy, demonstrating generalized muscle rigidity, followed by the return of the neonate’s movements after the seizure ceased. Video S10. Convulsion in a neonatal puppy demonstrating pedaling movements. Video S11. Respiratory distress in a neonatal puppy due to perinatal asphyxia and severe hypoxia. Video S12. Blood collection through the jugular vein in a neonatal puppy.
Author Contributions
Conceptualization, methodology, writing—original draft preparation, writing—review and editing, K.H.N.P.P., K.d.M.F., J.C.M., G.M.X., D.R.C., R.K.S.C. and M.L.G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This review was supported by the São Paulo Research Foundation (FAPESP), process number 2022/10710–4.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grundy, S.A. Clinically relevant physiology of the neonate. Vet. Clin. N. Am. Small Anim. Pract. 2006, 36, 443–459. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.E.; Kutzler, M.A. Small Animal Pediatrics, 1st ed.; Elsevier: Saint Louis, MO, USA, 2011. [Google Scholar]
- Konde, A.M.; Gitau, G.K.; Kiptoon, J.; Gakuya, D. Puppy morbidity and mortality among breeding kennels in Nairobi, Kenya. Jacobs J. Vet. Sci. Res. 2015, 1, 19. [Google Scholar]
- Chastant-Maillard, S.; Mila, H.; Grellet, A.; Aurélie, F. NeoCare—5 Years of Science to Improve the Health of Newborn Puppies. 2016. Available online: https://www.researchgate.net/publication/303474554_NeoCare_5_years_of_science_to_improve_the_health_of_newborn_puppies (accessed on 2 March 2024).
- Mugnier, A.; Mila, H.; Guiraud, F.; Brévaux, J.; Lecarpentier, M.; Martinez, C.; Mariani, C.; Adib-Lesaux, A.; Chastant-Maillard, S.; Saegerman, C.; et al. Birth weight as a risk factor for neonatal mortality: Breed-specific approach to identify at-risk puppies. Prev. Vet. Med. 2019, 171, 104746. [Google Scholar] [CrossRef]
- Veronesi, M.C.; Fusi, J. Feline neonatology: From birth to commencement of weaning–what to know for successful management. J. Feline Med. Surg. 2022, 24, 232–242. [Google Scholar] [CrossRef]
- Axnér, E.; Axelsson, R.; Hermansson, U. Evaluation of Canine Neonatal Health by Breeders: A Prospective Questionnaire Study on the Association between Neonatal Scores (Modified APGAR), Parturition, Birth Weight, Growth, and Puppy Mortality. Animals 2023, 13, 3605. [Google Scholar] [CrossRef] [PubMed]
- Mugnier, A.; Gaillard, V.; Chastant, S. Impact of compensatory growth on survival in newborn kittens. Front. Vet. Sci. 2024, 11, 1419383. [Google Scholar] [CrossRef] [PubMed]
- Contreras, G.; Viegas, C.; Gama, A.; Silva, F.; Pires, I. Mortality in Stray Kittens under Eight Weeks Old: Focusing on Congenital Malformations. Vet. Sci. 2024, 11, 461. [Google Scholar] [CrossRef]
- Cohn, L.A.; Lee, J.A. Pediatric critical care: Part 1-diagnostic interventions. Clin. Brief. 2015, 35–40. [Google Scholar]
- Grundy, A.; Sophie, A. Canine neonatal health. Vet. Clin. N. Am. Small Anim. Pract. 2023, 53, 1161–1193. [Google Scholar] [CrossRef]
- Lawler, D.F. Neonatal and pediatric care of the puppy and kitten. Theriogenology 2008, 70, 384–392. [Google Scholar] [CrossRef]
- Silva, L.C.G.; Lucio, C.F.; Veiga, G.A.L.; Rodrigues, J.A.; Vannucchi, C.I. Neonatal clinical evaluation, blood gas and radiographic assessment after normal birth, vaginal dystocia or caesarean section in dogs. Reprod. Domest. Anim. 2009, 44, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, M.C.; Panzani, S.; Faustini, M.; Rota, A. An Apgar scoring system for routine assessment of newborn puppy viability and short-term survival prognosis. Theriogenology 2009, 72, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Batista, M.; Moreno, C.; Vilar, J.; Golding, M.; Brito, C.; Santana, M.; Alamo, D. Neonatal viability evaluation by Apgar score in puppies delivered by cesarean section in two brachycephalic breeds (English and French bulldog). Anim. Reprod. Sci. 2014, 146, 218–226. [Google Scholar] [CrossRef]
- Hibaru, V.Y.; Pereira, K.H.N.P.; Fuchs, K.d.M.; Lopes, M.D.; Alfonso, A.; de Souza, F.F.; Chiacchio, S.B.; Tsunemi, M.H.; Machado, L.H.d.A.; Lourenço, M.L.G. Topics in the routine assessment of newborn kitten vitality: Apgar score, reflexes and complementary assessments. J. Feline Med. Surg. 2022, 24, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Arango, A.; Rowe, M.I. The neonatal puppy as an experimental subject. Neonatology 1971, 18, 173–182. [Google Scholar] [CrossRef]
- Magrini, F. Hemodynamic determinants of the arterial blood pressure rise during growth in conscious puppies. Cardiovasc. Res. 1978, 12, 422–428. [Google Scholar] [CrossRef]
- Adelman, R.D.; Wright, J. Systolic blood pressure and heart rate in the growing beagle puppy. Dev. Pharmacol. Ther. 1985, 8, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, J.V.; Latini, C.D.; Santos, B.A.; Aleixo, A.S.C.; Pereira, K.H.N.P.; Tsunemi, M.H.; Machado, L.H.d.A.; Lourenço, M.L.G. Analysis of Heart Rate Variability in Newborns Dogs with Different Types of Delivery during the First 35 Days of Life. Vet. Sci. 2024, 11, 225. [Google Scholar] [CrossRef]
- Vassalo, F.G.; Simões, C.R.B.; Sudano, M.J.; Prestes, N.C.; Lopes, M.D.; Chiacchio, S.B.; Lourenço, M.L.G. Topics in the routine assessment of newborn puppy viability. Top. Companion Anim. Med. 2015, 30, 16–21. [Google Scholar]
- Cerejo, S.A.; Teixeira-Neto, F.J.; Garofalo, N.A.; Pimenta, E.L.; Zanuzzo, F.S.; Klein, A.V. Effects of cuff size and position on the agreement between arterial blood pressure measured by Doppler ultrasound and through a dorsal pedal artery catheter in anesthetized cats. Vet. Anaesth. Analg. 2020, 47, 191–199. [Google Scholar] [CrossRef]
- Garofalo, N.A.; Neto, F.J.T.; Alvaides, R.K.; de Oliveira, F.A.; Pignaton, W.; Pinheiro, R.T. Agreement between direct, oscillometric and Doppler ultrasound blood pressures using three different cuff positions in anesthetized dogs. Vet. Anaesth. Analg. 2012, 39, 324–334. [Google Scholar] [CrossRef] [PubMed]
- Poffenbarger, E.M.; Ralston, S.L.; Chandler, M.L.; Olson, P.N. Canine neonatology. Part I Physiologics differences between puppies and adults. Comp. Cont. EdU 1990, 12, 1601–1609. [Google Scholar]
- Abreu, R.A.; Almeida, L.L.; Rosa Filho, R.R.; Angrimani, D.D.S.R.; Brito, M.M.; Flores, R.B.; Vannucchi, C.I. Canine pulmonary clearance during feto-neonatal transition according to the type of delivery. Theriogenology 2024, 224, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, M.L.G.; Ferreira, H. Electrocardiography evaluation in cats from birth to 30 days of age. Can. Vet. J. 2003, 44, 914–917. [Google Scholar] [PubMed]
- Apgar, V. A proposal for a new method of evaluation of the newborn infant. Anesth. Analg. 1953, 32, 260–267. [Google Scholar] [CrossRef]
- Veronesi, M.C. Assessment of canine neonatal viability—The Apgar score. Reprod. Dom. Anim. 2016, 51, 46–50. [Google Scholar] [CrossRef]
- Groppetti, D.; Pecile, A.; Del Carro, A.P.; Copley, K.; Minero, M.; Cremonesi, F. Evaluation of newborn canine viability by means of umbilical vein lactate measurement, apgar score and uterine tocodynamometry. Theriogenology 2010, 74, 1187–1196. [Google Scholar] [CrossRef]
- Fusi, J.; Faustini, M.; Bolis, B.; Veronesi, M.C. Apgar score or birthweight in Chihuahua dogs born by elective Caesarean section: Which is the best predictor of the survival at 24 h after birth? Acta Vet. Scand. 2020, 62, 39. [Google Scholar] [CrossRef]
- Antończyk, A.; Ochota, M.; Niżański, W. Umbilical cord blood gas parameters and Apgar scoring in assessment of new-born dogs delivered by cesarean section. Animals 2021, 11, 685. [Google Scholar] [CrossRef]
- Srithunyarat, T.; Jitpean, S.; Wipoosak, P.; Nonthakotr, C.; Boonbal, N.; Kunkitti, P.; Seesupa, S. Apgar scores in puppies following the induction of etomidate compared with alfaxalone or propofol for cesarean section. Vet. World 2024, 17, 527. [Google Scholar] [CrossRef]
- Pereira, K.H.N.P.; Hibaru, V.Y.; Fuchs, K.d.M.; Correia, L.E.C.d.S.; Lopes, M.D.; Ferreira, J.C.P.; de Souza, F.F.; Machado, L.H.d.A.; Chiacchio, S.B.; Lourenço, M.L.G. Use of cardiac troponin I (cTnI) levels to diagnose severe hypoxia and myocardial injury induced by perinatal asphyxia in neonatal dogs. Theriogenology 2022, 180, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, M.C.; Faustini, M.; Probo, M.; Rota, A.; Fusi, J. Refining the APGAR score cutoff values and viability classes according to breed body size in newborn dogs. Animals 2022, 12, 1664. [Google Scholar] [CrossRef]
- Apgar, V. James LS. Further observations on the newborn scoring system. Am. J. Dis. Child. 1962, 104, 419–428. [Google Scholar] [PubMed]
- Lavely, J.A. Pediatric neurology of the dog and cat. Vet. Clin. N. Am. Small Anim. Pract. 2006, 36, 475–501. [Google Scholar] [CrossRef]
- Münnich, A. Fading kitten syndrome: Factors predisposing to ‘faders’ and treatment options. J. Feline Med. Surg. 2022, 24, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.T.; Newquist, K.L. Care of newborn animals. In Small Animal Pediatrics, 1st ed.; Peterson, M.E., Kutzler, M.A., Eds.; Elsevier: Saint Louis, MO, USA, 2011; pp. 44–52. [Google Scholar]
- Fuchs, K.M.; Pereira, K.H.N.P.; Xavier, G.M.; Mendonça, J.C.; Barreto, R.O.; Silva, R.C.; de Souza, F.F.; Lourenço, M.L.G. Neonatal hypoglycemia in dogs-pathophysiology, risk factors, diagnosis and treatment. Front. Vet. Sci. 2024, 11, 1345933. [Google Scholar] [CrossRef] [PubMed]
- Moon, P.F.; Massat, B.J.; Pascoe, P.J. Neonatal Critical Care. Vet. Clin. N. Am. Small Anim. Pract. 2001, 31, 343–367. [Google Scholar] [CrossRef]
- Plavec, T.; Knific, T.; Slapšak, A.; Raspor, S.; Lukanc, B.; Pipan, M.Z. Canine neonatal assessment by vitality score, amniotic fluid, urine, and umbilical cord blood analysis of glucose, lactate, and cortisol: Possible influence of parturition type? Animals 2022, 12, 1247. [Google Scholar] [CrossRef]
- Fuchs, K.D.M.; Pacífico Pereira, K.H.N.; de Sousa, G.C.; Xavier, G.M.; Camargo, G.D.A.; de Souza, F.F.; Lourenço, M.L.G. Hypoglycaemia management with a hypercaloric supplementation in neonatal puppies delivered by caesarean section. Reprod. Domest. Anim. 2023, 58, 1345–1351. [Google Scholar] [CrossRef]
- Mila, H.; Grellet, A.; Delebarre, M.; Mariani, C.; Feugier, A.; Chastant-Maillard, S. Monitoring of the newborn dog and prediction of neonatal mortality. Prev. Vet. Med. 2017, 143, 11–20. [Google Scholar] [CrossRef]
- Pereira, K.H.N.P.; Fuchs, K.d.M.; Hibaru, V.Y.; Correia, L.E.C.d.S.; Ferreira, J.C.P.; de Souza, F.F.; Machado, L.H.d.A.; Chiacchio, S.B.; Lourenço, M.L.G. Neonatal sepsis in dogs: Incidence, clinical aspects and mortality. Theriogenology 2022, 177, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Claus, M.A.; Levy, J.K.; MacDonald, K.; Tucker, S.J.; Crawford, P.C. Immunoglobulin concentrations in feline colostrum and milk, and the requirement of colostrum for passive transfer of immunity to neonatal kittens. J. Feline Med. Surg. 2006, 8, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Evan, A.P.; Stoeckel, J.A.; Loemker, V.; Baker, J.T. Development of the intrarenal vascular system of the puppy kidney. Anat. Rec. 1979, 194, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Olbing, H.; Blaufox, M.D.; Aschinberg, L.C.; Silkalns, G.I.; Bernstein, J.; Spitzer, A.; Edelmann, C.M. Postnatal changes in renal glomerular blood flow distribution in puppies. J. Clin. Investig. 1973, 52, 2885–2895. [Google Scholar] [CrossRef] [PubMed]
- Hay, D.A.; Evan, A.P. Maturation of the proximal tubule in the puppy kidney: A comparison to the adult. Anat. Rec. 1979, 195, 273–300. [Google Scholar] [CrossRef]
- Münnich, A.; Küchenmeister, U. Causes, diagnosis and therapy of common diseases in neonatal puppies in the first days of life: Cornerstones of practical approach. Reprod. Domest. Anim. 2014, 49, 64–74. [Google Scholar] [CrossRef]
- Lee, J.A.; Cohn, L.A. Fluid therapy for pediatric patients. Vet. Clin. North. Am. Small Anim. Pract. 2016, 47, 373. [Google Scholar] [CrossRef]
- Pereira, K.H.N.P.; Correia, L.E.C.d.S.; Oliveira, E.L.R.; Bernardo, R.B.; Jorge, M.L.N.; Gobato, M.L.M.; de Souza, F.F.; Rocha, N.S.; Chiacchio, S.B.; Lourenço, M.L.G. Incidence of congenital malformations and impact on the mortality of neonatal canines. Theriogenology 2019, 140, 52–57. [Google Scholar] [CrossRef]
- Münnich, A. The pathological newborn in small animals: The neonate is not a small adult. Vet. Res. Commun. 2008, 32, 81–85. [Google Scholar] [CrossRef]
- Meloni, T.; Martino, P.; Grieco, V.; Pisu, M.C.; Banco, B.; Rota, A.; Veronesi, M.C. A survey on bacterial involvement in neonatal mortality in dogs. Vet. Ital. 2014, 50, 293–299. [Google Scholar]
- Silvestre-Ferreira, A.C.; Pastor, J. Feline neonatal isoerythrolysis and the importance of feline blood types. Vet. Med. Int. 2010, 2010, 753726. [Google Scholar] [CrossRef] [PubMed]
- Wilborn, R.R. Small Animal Neonatal Health. Vet. Clin. N. Am. Small Anim. Pract. 2018, 48, 683–699. [Google Scholar] [CrossRef] [PubMed]
- Kajdič, L.; Plavec, T.; Zdovc, I.; Kalin, A.; Zakošek Pipan, M. Impact of type of parturition on colostrum microbiota composition and puppy survival. Animals 2021, 11, 1897. [Google Scholar] [CrossRef]
- Mugnier, A.; Chastant-Maillard, S.; Mila, H.; Lyazrhi, F.; Guiraud, F.; Adib-Lesaux, A.; Gaillard, V.; Saegerman, C.; Grellet, A. Low and very low birth weight in puppies: Definitions, risk factors and survival in a large-scale population. BMC Vet. Res. 2020, 16, 354. [Google Scholar] [CrossRef] [PubMed]
- Bounous, D.I.; Hoskins, J.D.; Boudreaux, M.K. The hematopoietic system. In Veterinary Pediatrics; Hoskins, J.D., Ed.; WB Saunders: Philadelphia, PA, USA, 1990; pp. 294–295. [Google Scholar]
- Veronesi, M.C.; Fusi, J. Biochemical factors affecting newborn survival in dogs and cats. Theriogenology 2023, 197, 150–158. [Google Scholar] [CrossRef]
- Meyers-Wallen, V.M.; Haskins, E.; Patterson, D.F. Hematologic values in healthy neonatal, weanling, and juvenile kittens. Am. J. Vet. Res. 1984, 45, 13–22. [Google Scholar]
- Johnston, S.D.; Kustritz, M.V.R.; Olson, P.N.S. The neonate—From birth to weaning. In Canine and Feline Theriogenology, 1st ed.; WB Saunders: Philadelphia, PA, USA, 2001; p. 151. [Google Scholar]
- Earl, F.L.; Melveger, B.E.; Wilson, R.L. The hemogram and bone marrow profile of normal neonatal and weanling beagle dogs. Lab. Anim. Sci. 1973, 23, 690–695. [Google Scholar]
- O'Brien, M.A.; McMichael, M.A.; Le Boedec, K.; Lees, G. Reference intervals and age-related changes for venous biochemical, hematological, electrolytic, and blood gas variables using a point of care analyzer in 68 puppies. J. Vet. Emerg. Crit. Care 2014, 24, 291–301. [Google Scholar] [CrossRef]
- Rørtveit, R.; Sævik, B.K.; Eggertsdóttir, A.V.; Skancke, E.; Lingaas, F.; Thoresen, S.I.; Jansen, J.H. Age-related changes in hematologic and serum biochemical variables in dogs aged 16–60 days. Vet. Clin. Pathol. 2015, 44, 47–57. [Google Scholar] [CrossRef]

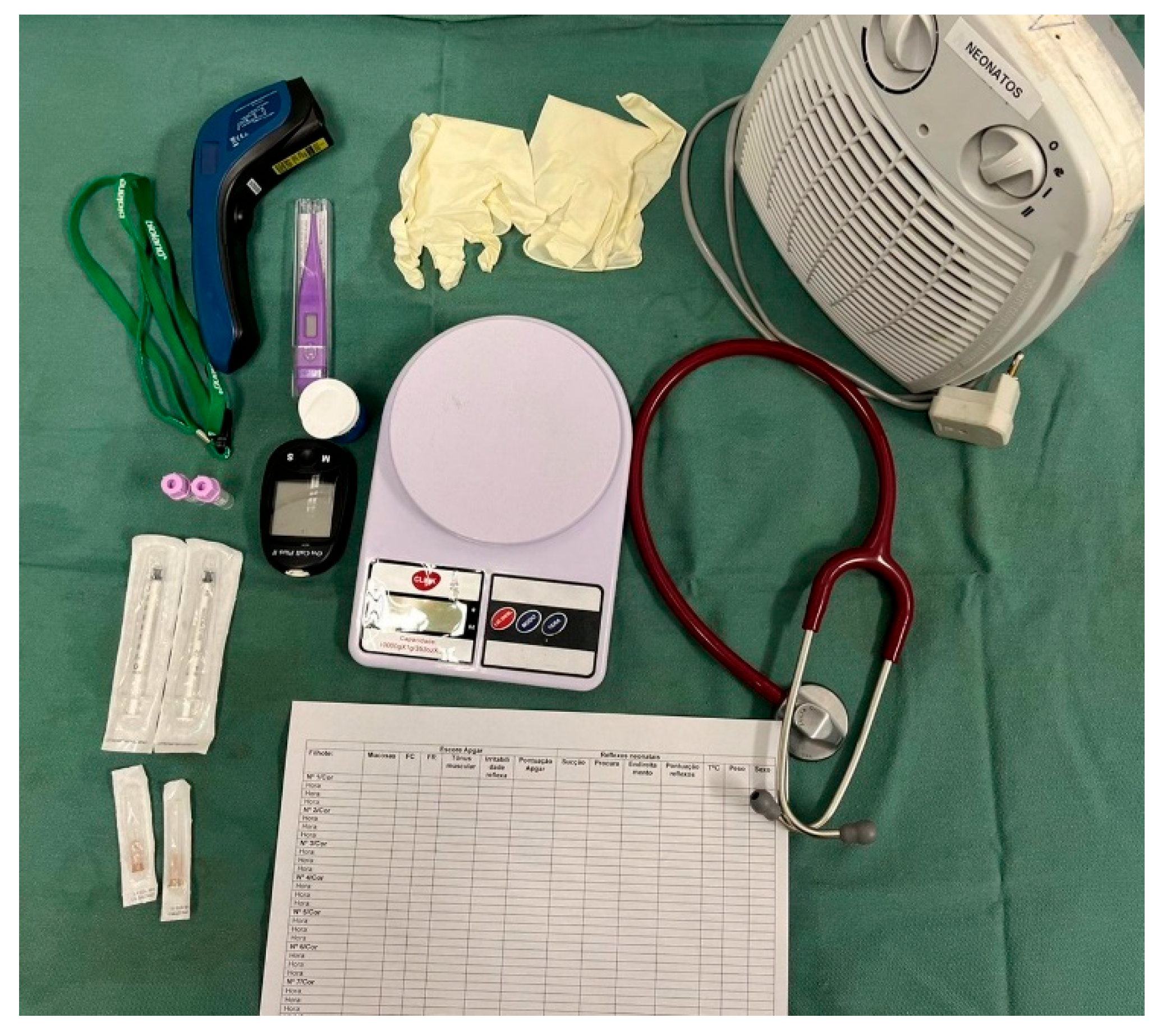
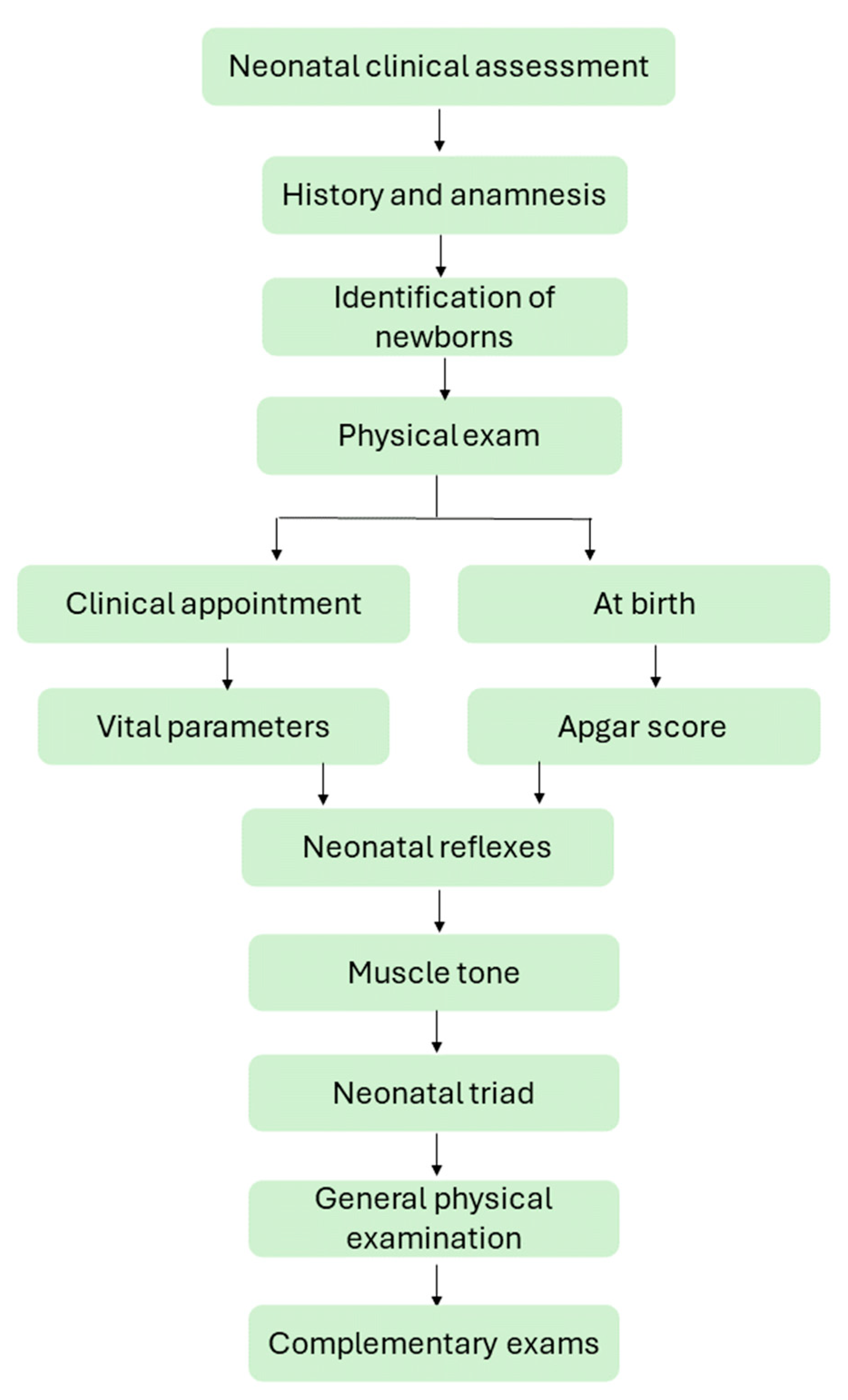
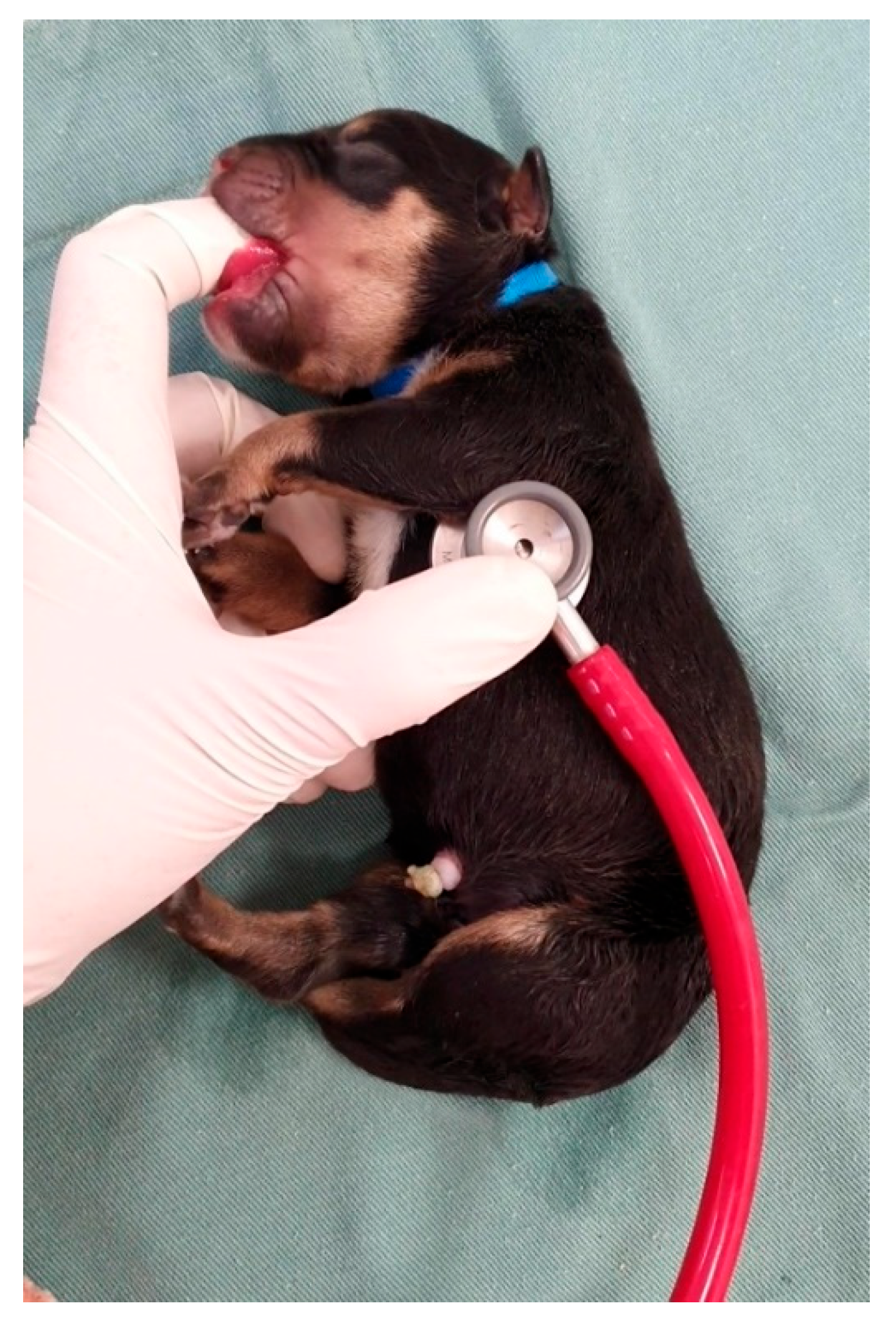
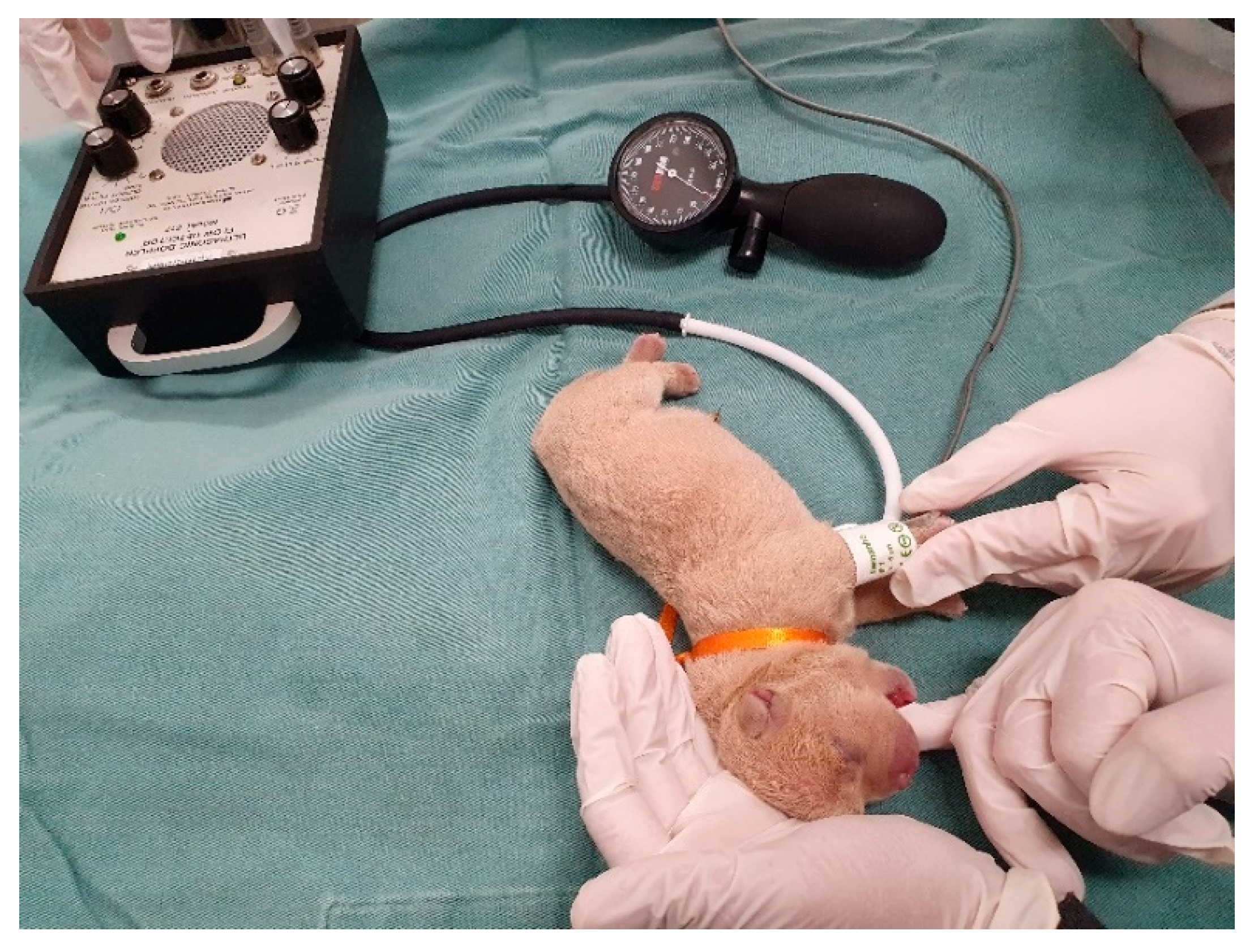



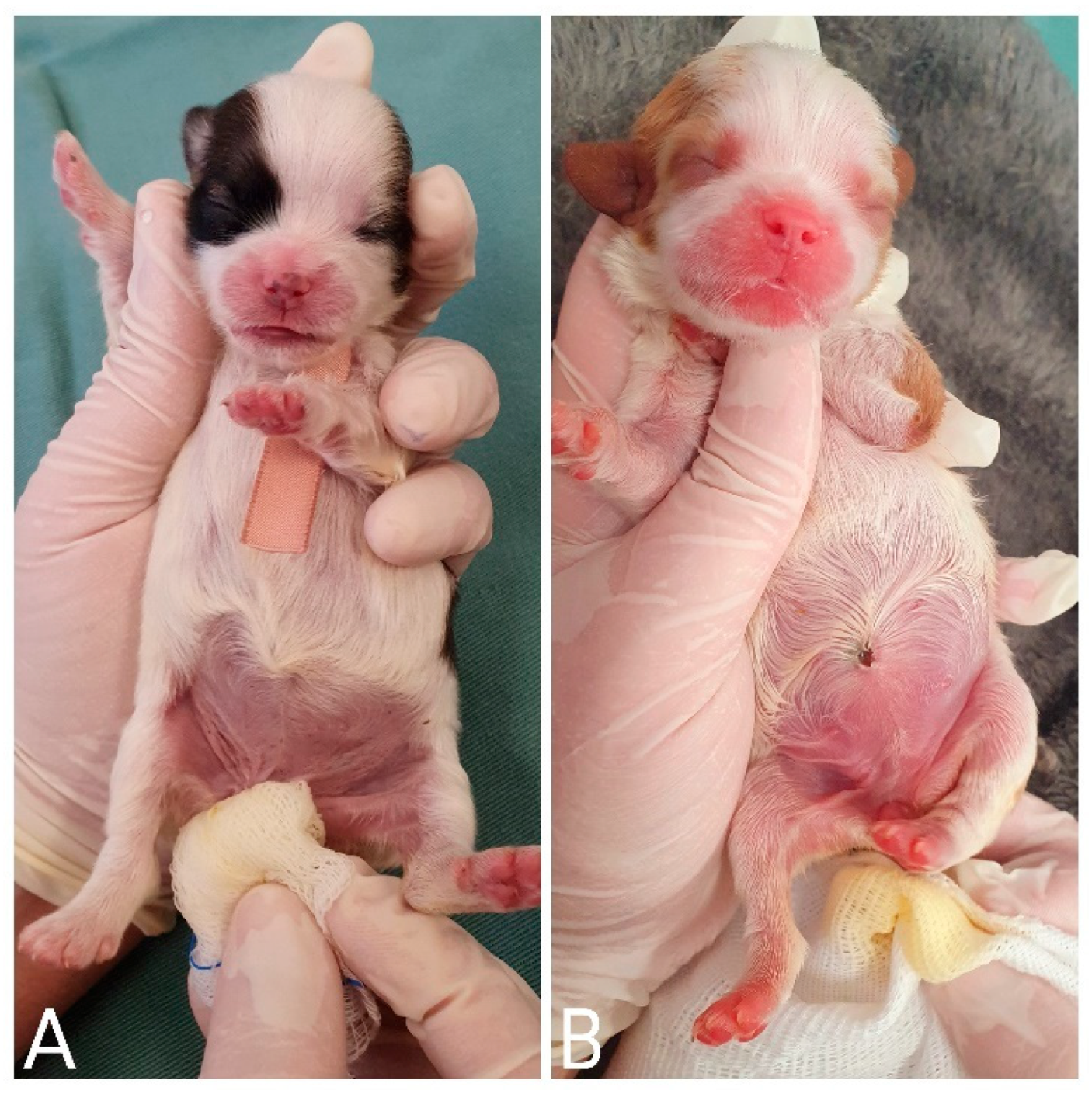



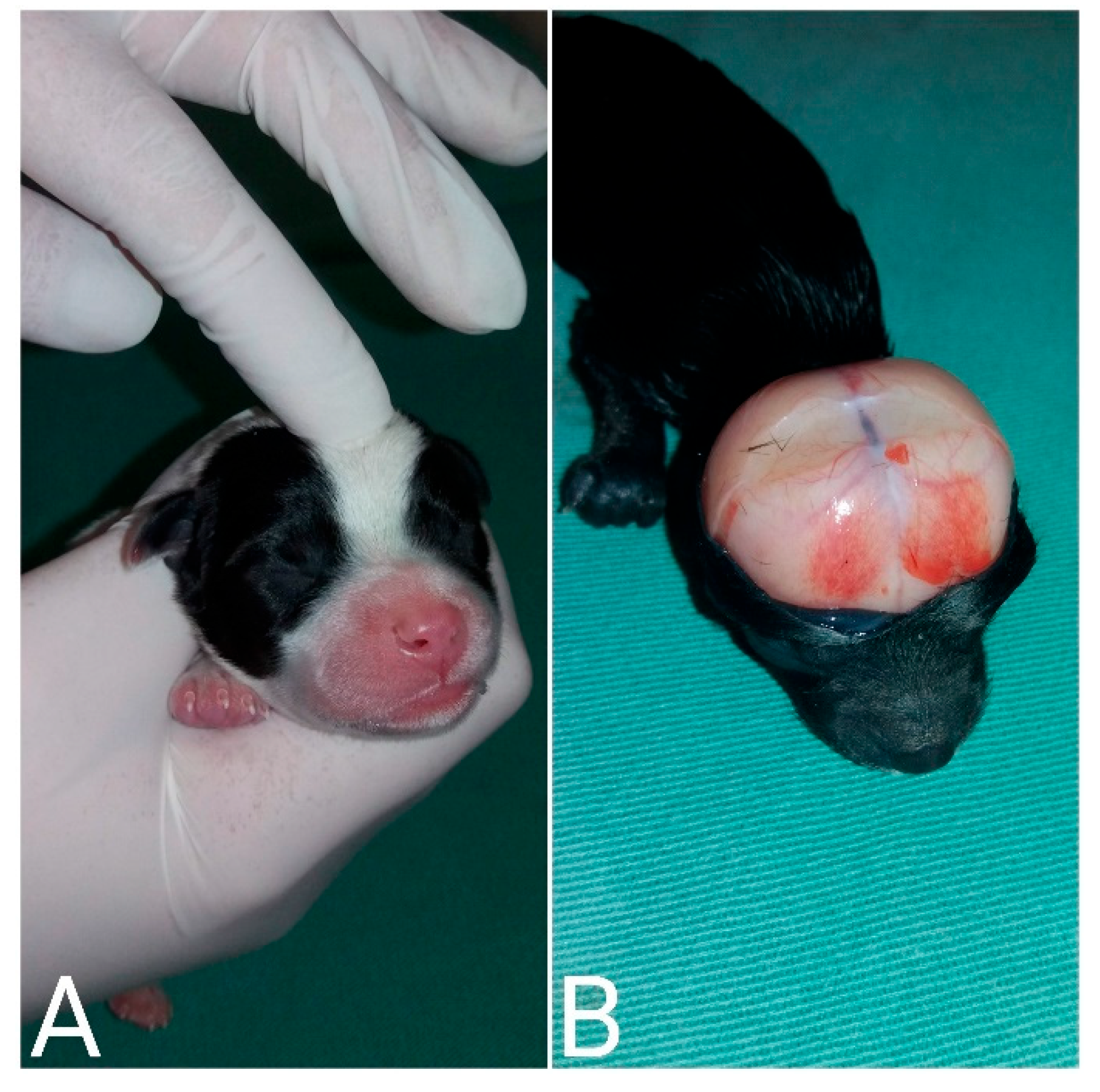
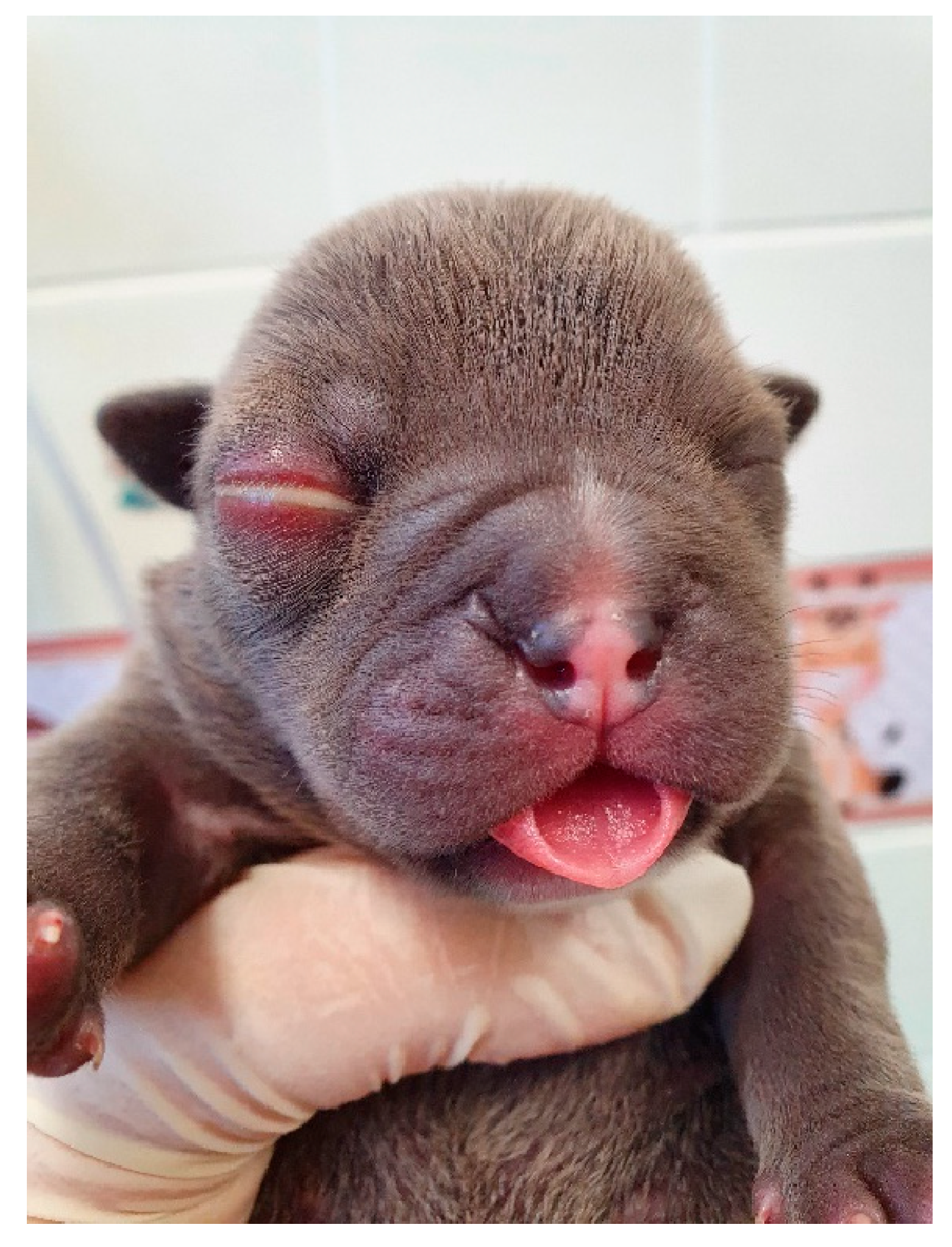
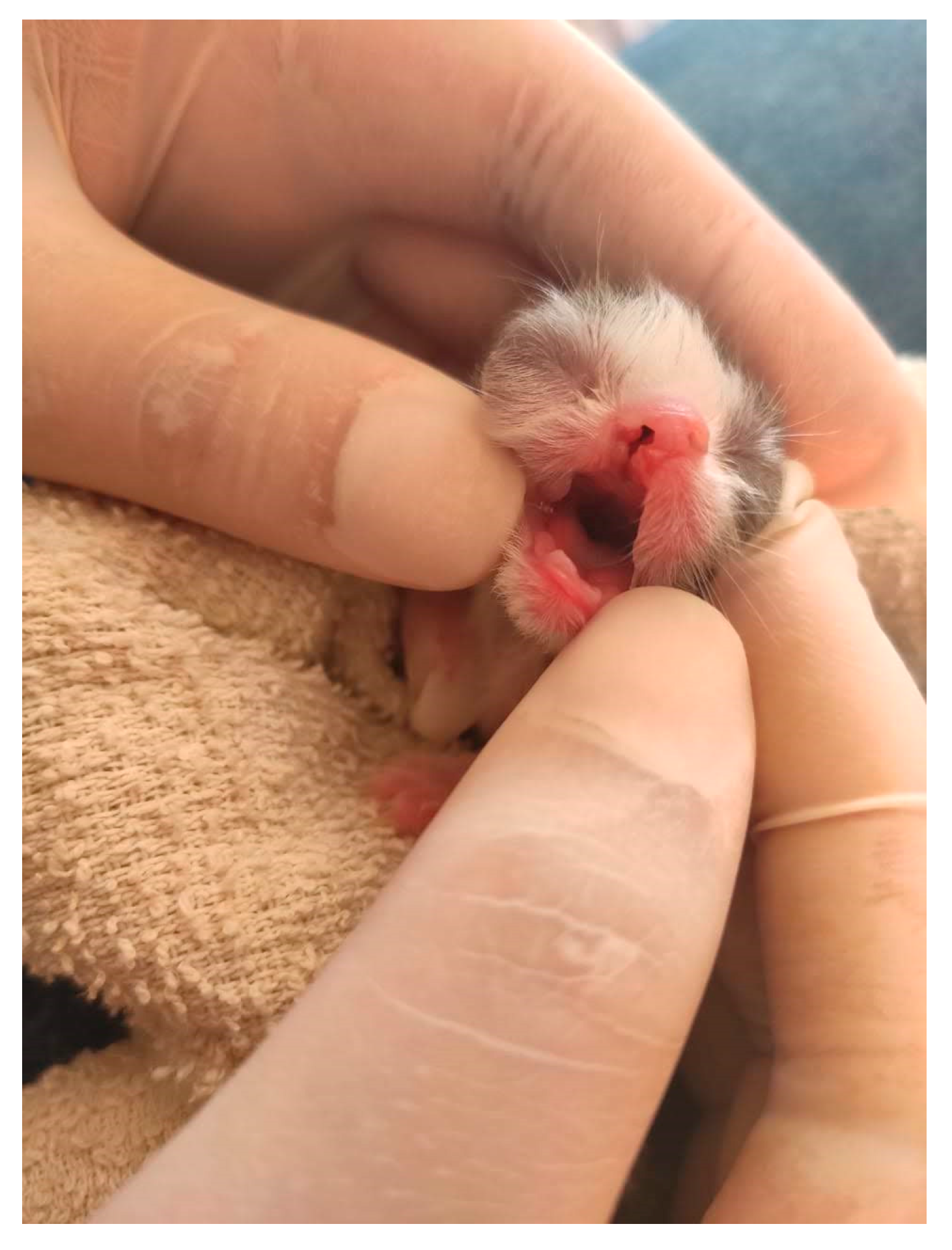
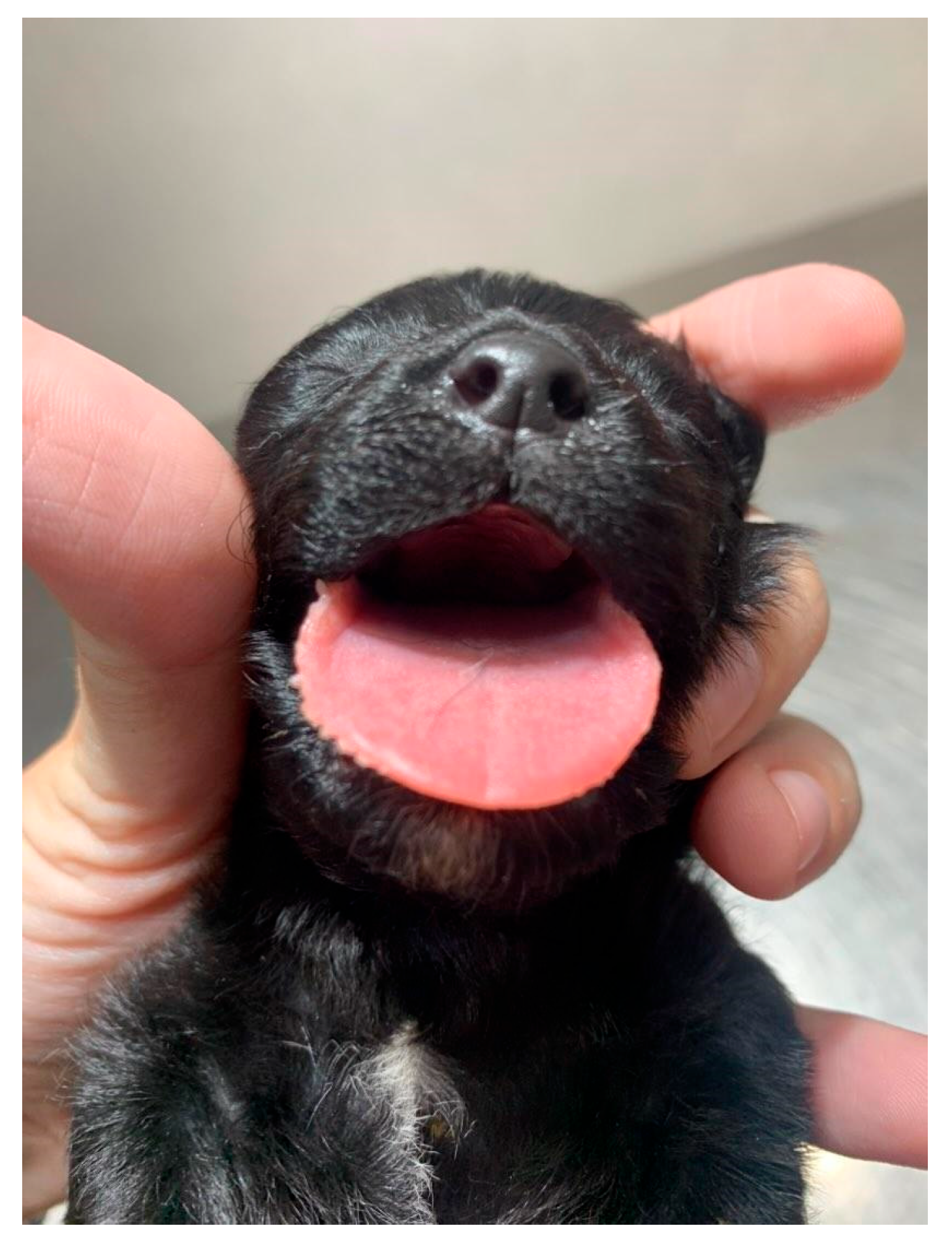
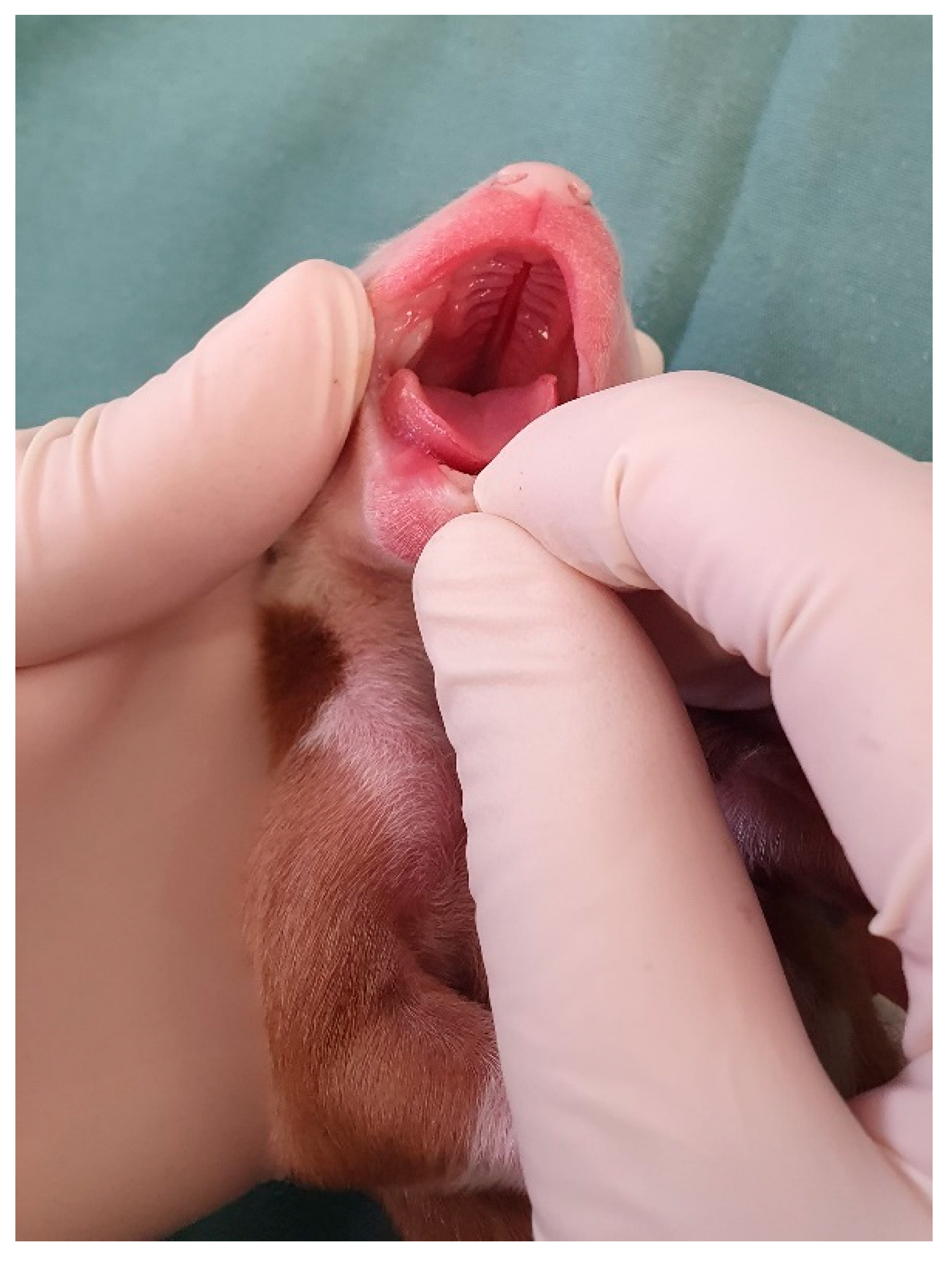




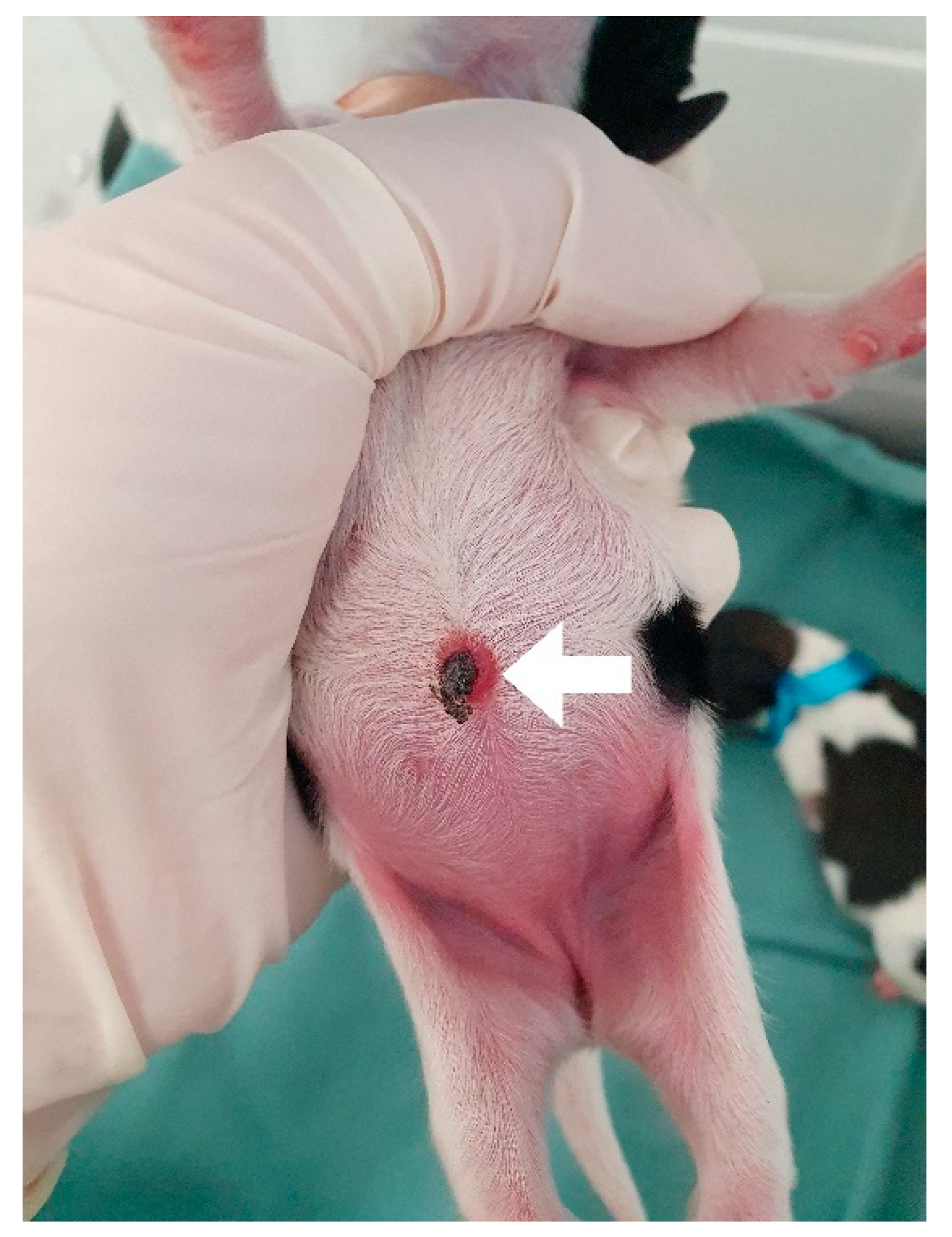

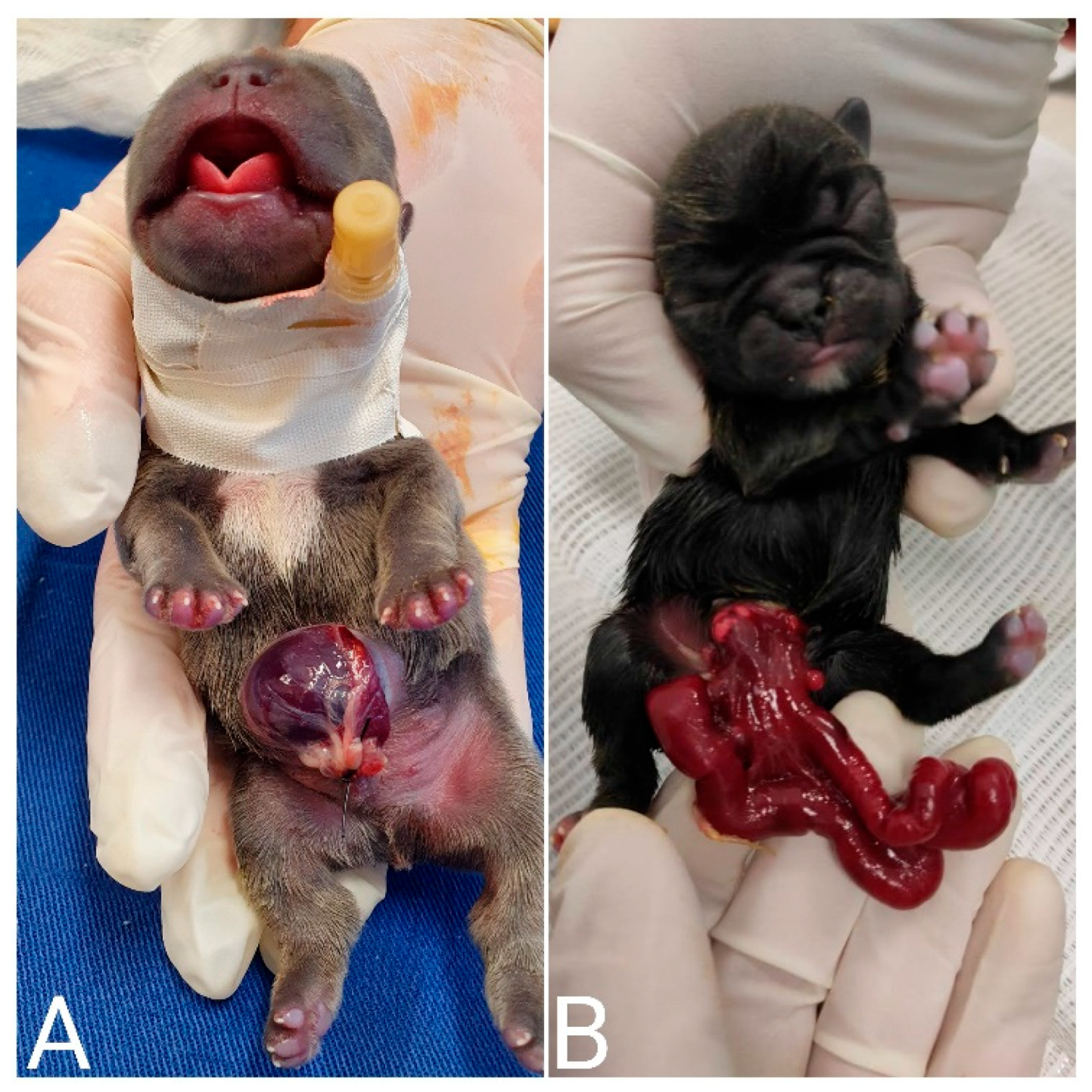
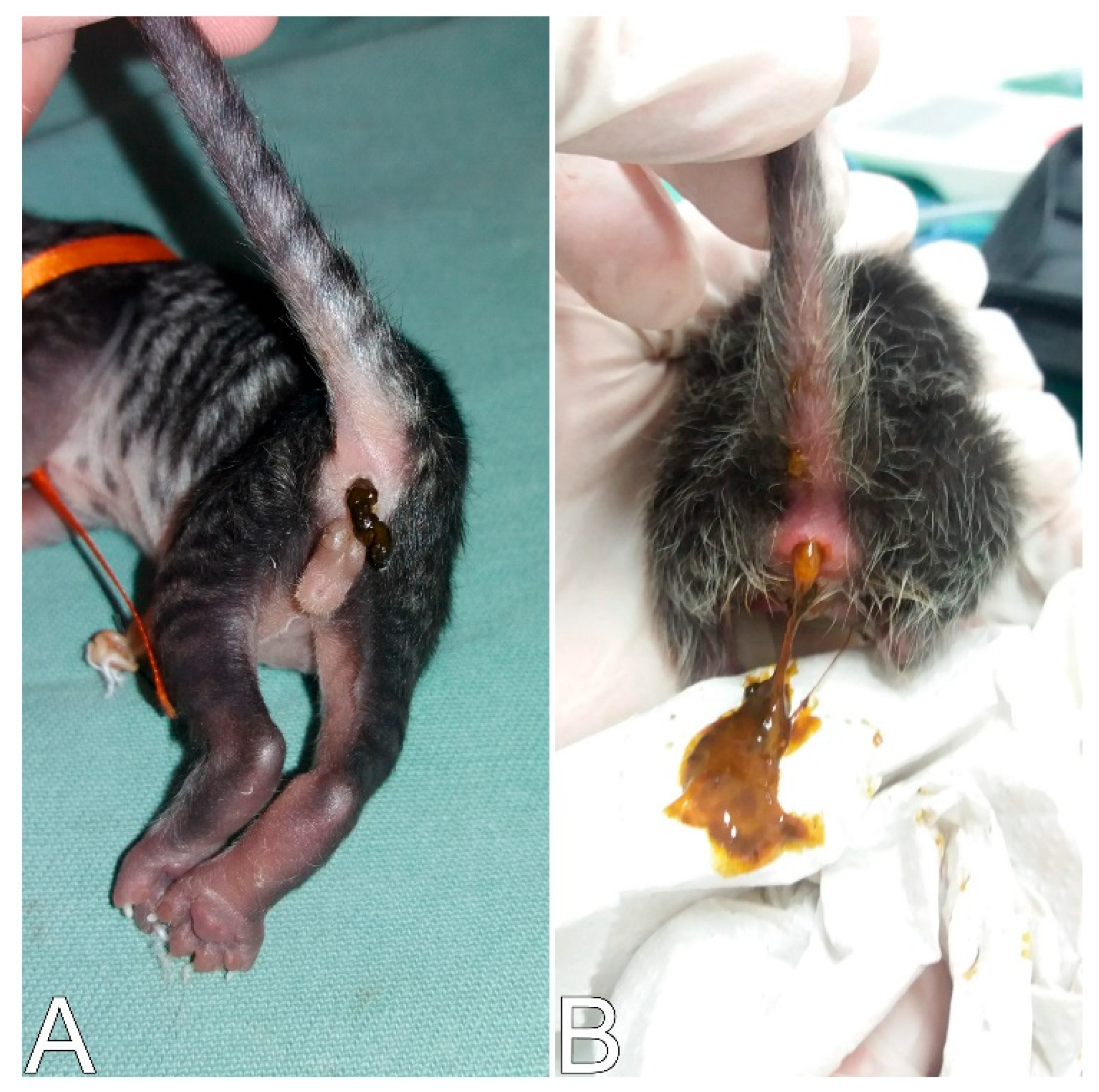








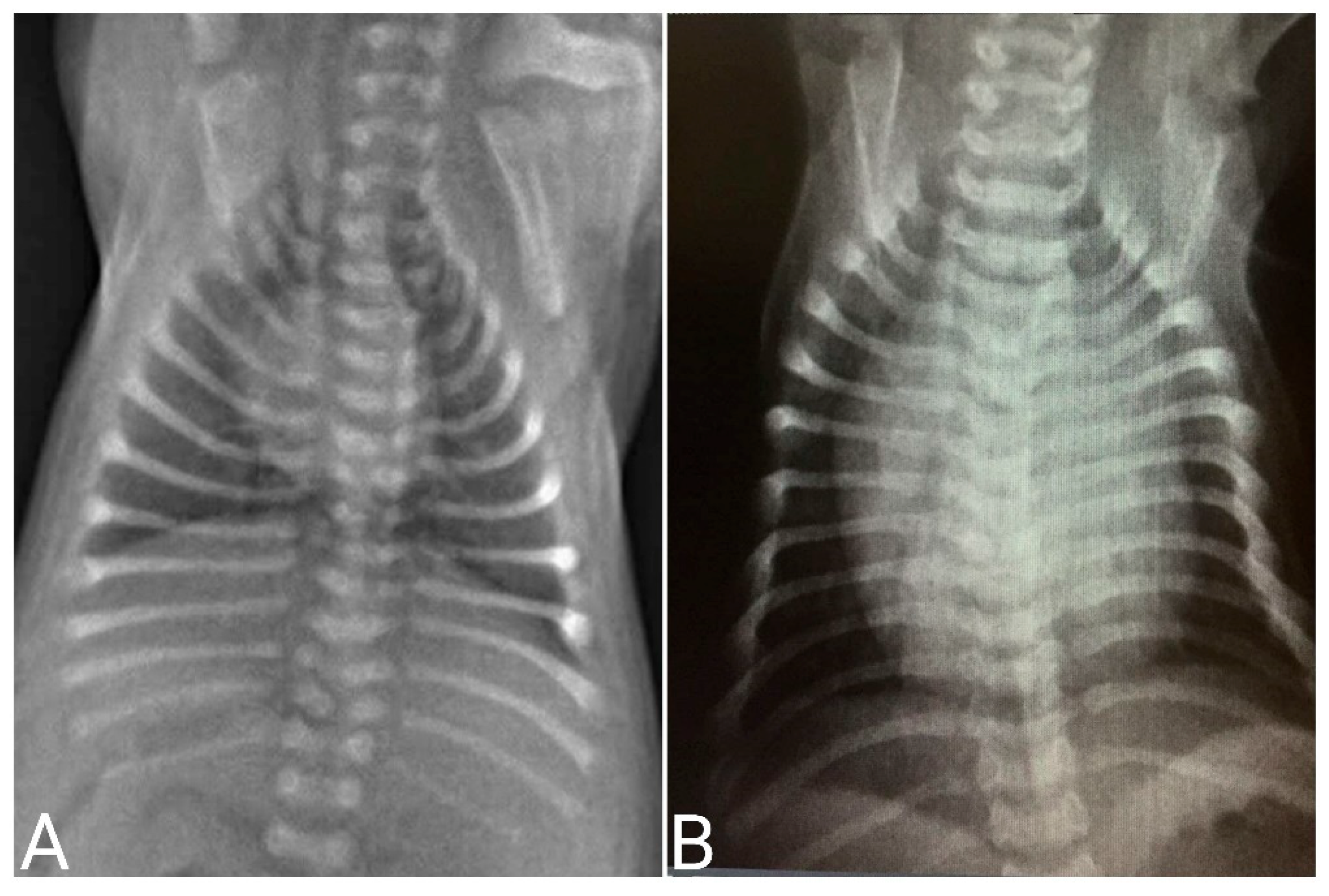
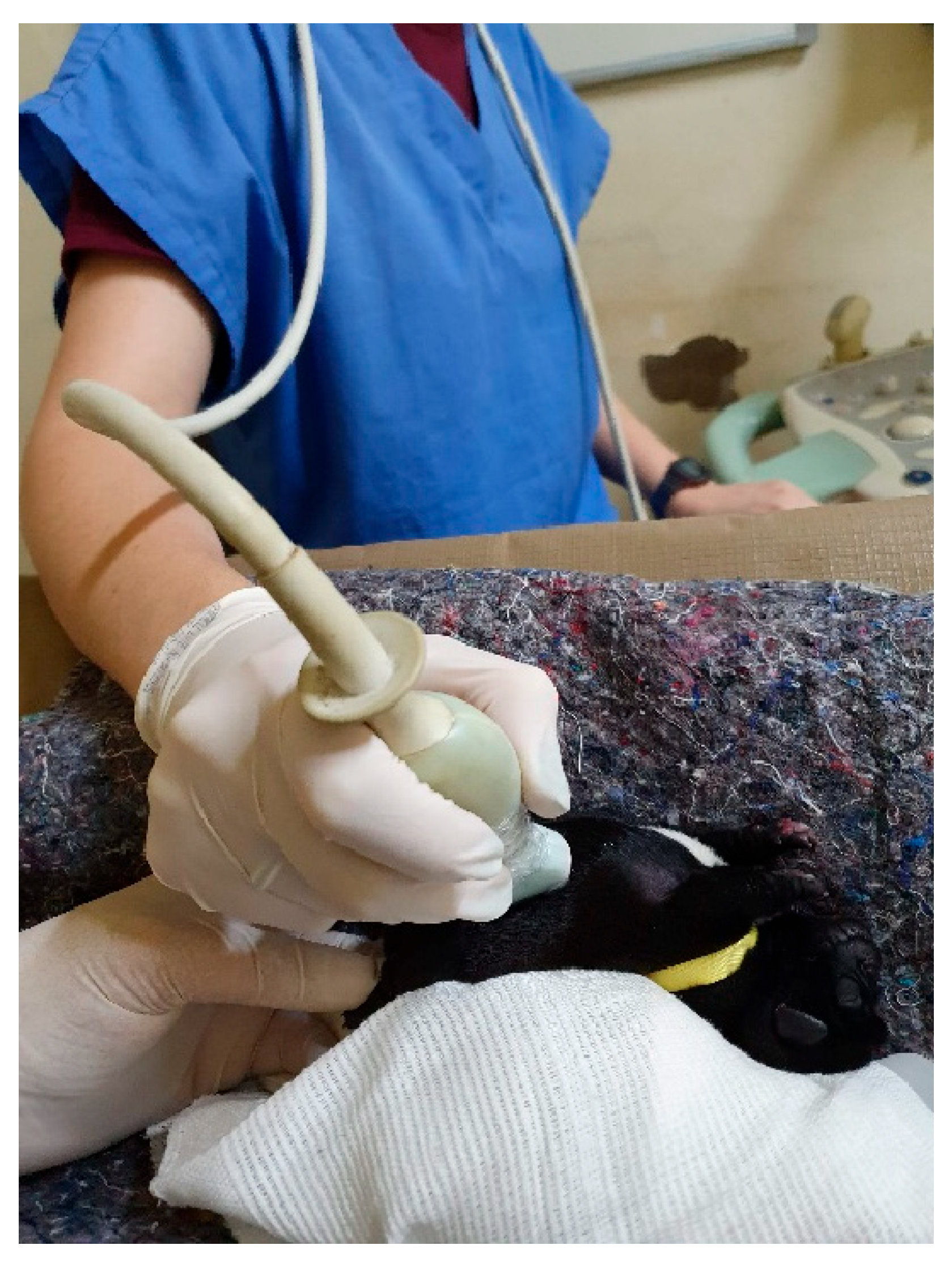
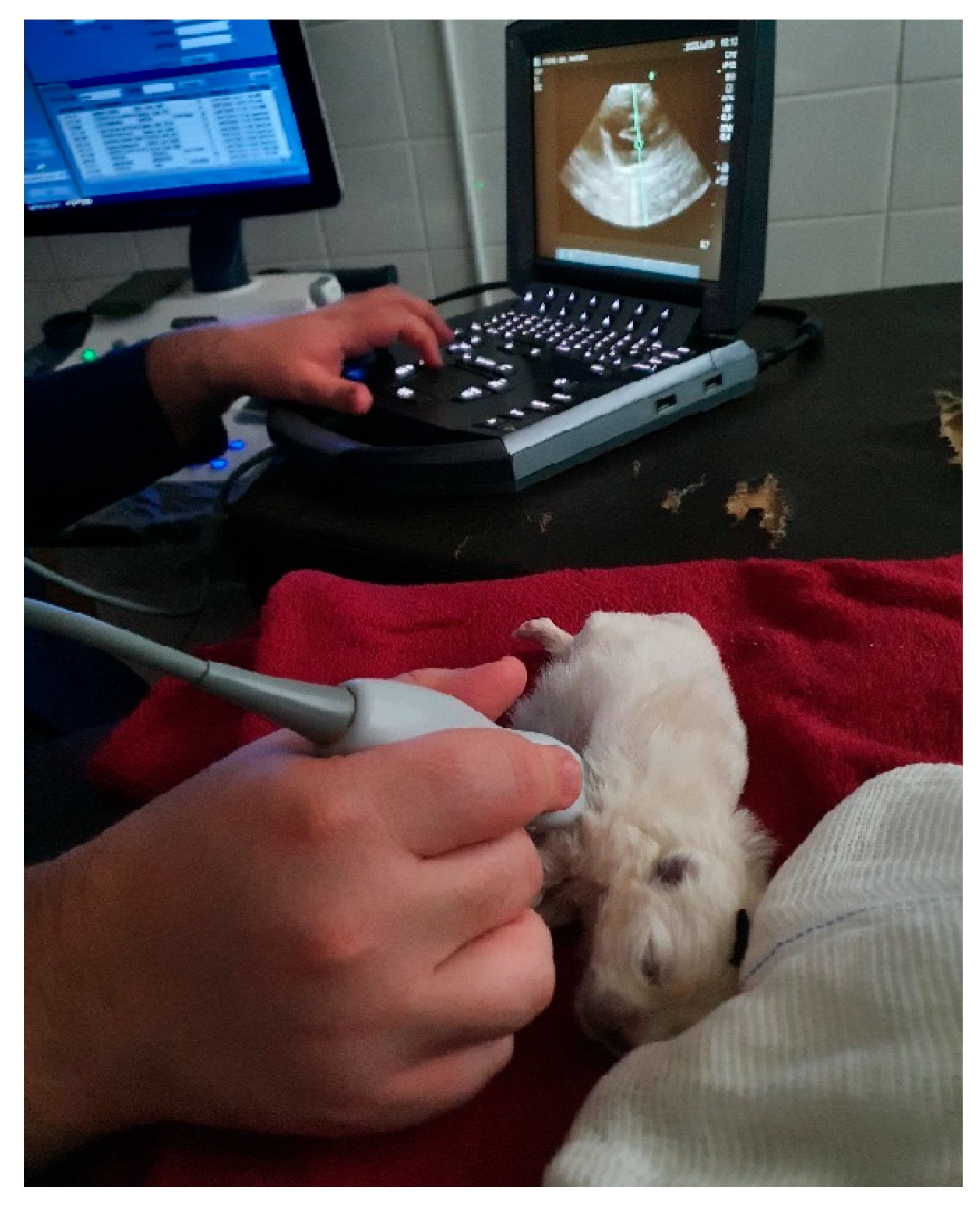
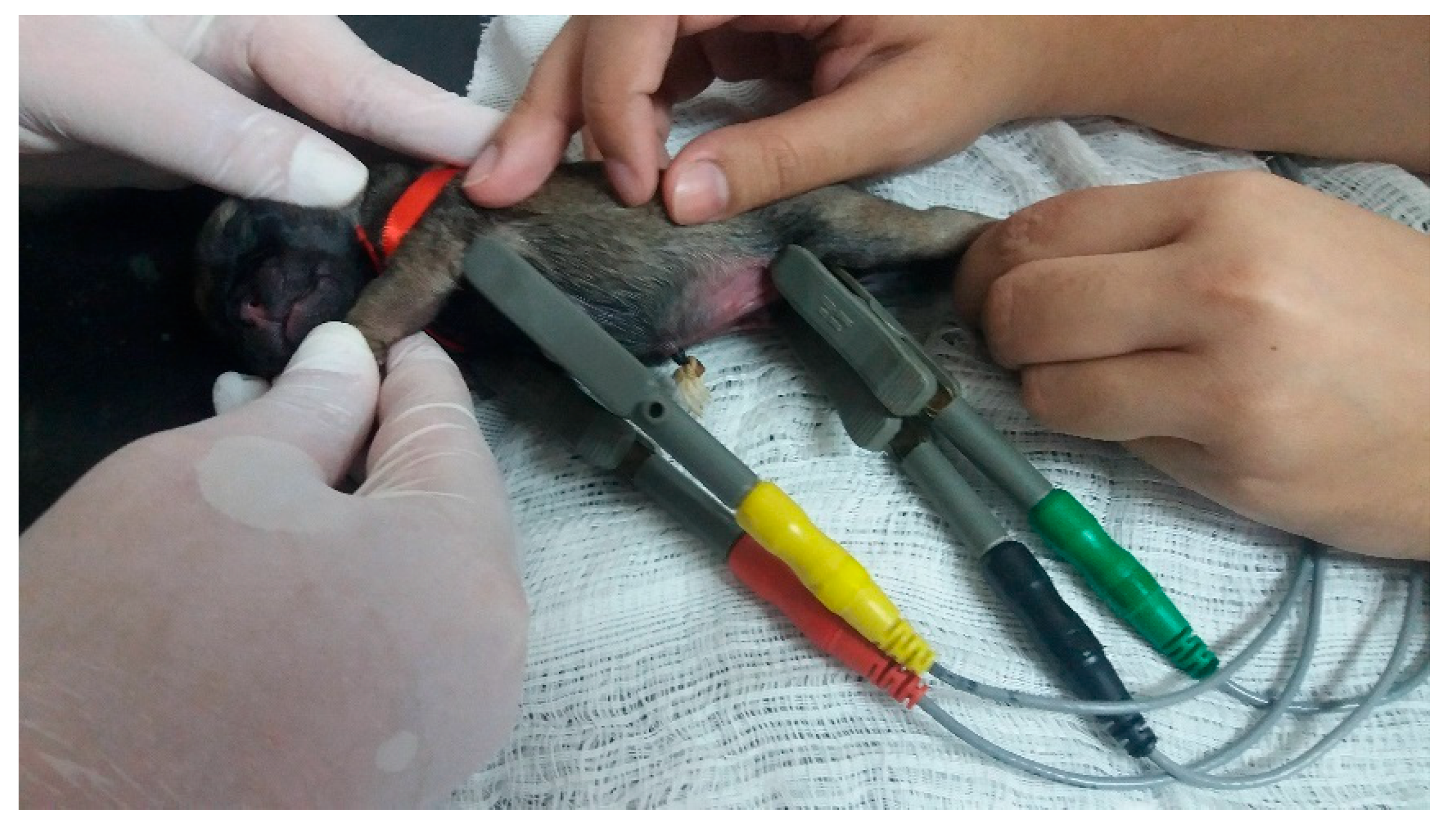
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).