
Retrospective Evaluation of Subpleural Consolidations Using Lung Ultrasound in 634 Dogs and 347 Cats

Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ultrasound Machine Settings and Probe Selection
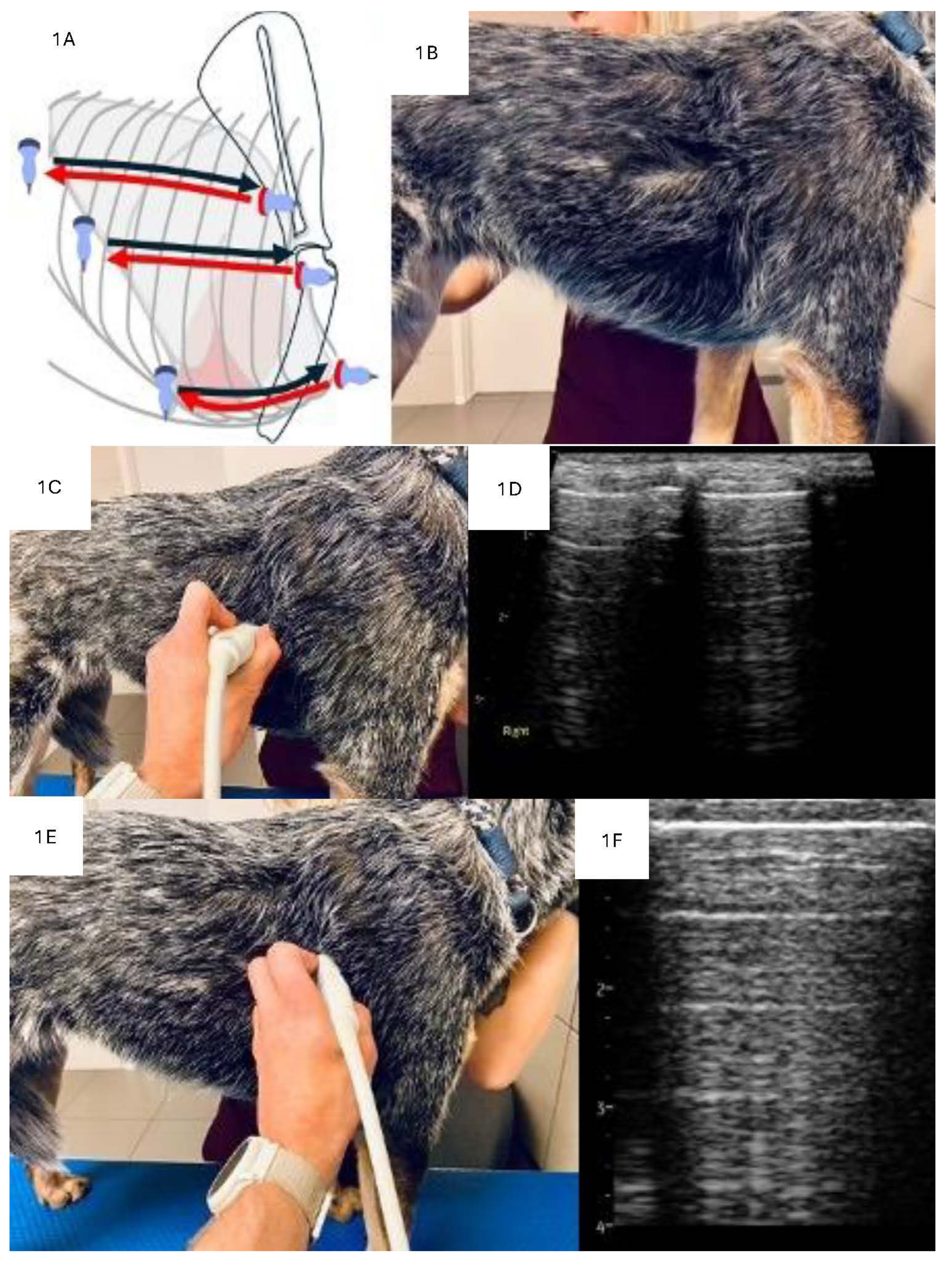
2.3. LUS Examination Technique
2.4. Analysis of Consolidations in 2D
2.5. Analysis of Consolidations in Color/Power Doppler Mode
2.6. Diagnosis
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Analysis of the Consolidations
3.3. Analysis of Bronchograms
3.4. Analysis of Vascularity
3.5. Analysis of Types of Consolidations in Terms of Diagnosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARDS | Acute respiratory distress syndrome |
| ASLT | Airless subpleural lung tissue |
| ATLP | Atelectatic tissue-like pattern |
| BAL | Bronchoalveolar lavage |
| CD | Color Doppler |
| CHF | Congestive heart failure |
| CT | Computed tomography |
| FNA | Fine needle aspiration |
| LUS | Lung ultrasound |
| M | Mass |
| N | Nodule-type consolidation |
| PD | Power Doppler |
| PLD | Parenchymal lung disease |
| PTE | Pulmonary thromboembolism |
| TRX | Thoracic radiograph |
| S | Shred-type consolidation |
| T | Tissue-type consolidation |
| W | Wedge-type consolidation |
References
- Pelchat, J.; Chalhoub, S.; Boysen, S.R. The use of veterinary point-of-care ultrasound by veterinarians: A nationwide Canadian survey. Can. Vet. J. 2020, 61, 1278–1282. [Google Scholar] [PubMed]
- Ward, J.L.; DeFrancesco, T.C. The Role of Point-of-Care Ultrasound in Managing Cardiac Emergencies. Vet. Clin. N. Am. Small Anim. Pract. 2023, 53, 1429–1443. [Google Scholar] [CrossRef] [PubMed]
- Kraszewska, K.G.M.; Boysen, S. Case report: Application of color Doppler sonography for the assessment of pulmonary consolidations in a dog. Front. Vet. Sci. 2023, 10, 1275929. [Google Scholar] [CrossRef]
- Rodrigues, N.F.; Giraud, L.; Bolen, G.; Fastrès, A.; Clercx, C.; Boysen, S.; Billen, F.; Gommeren, K. Comparison of lung ultrasound, chest radiographs, C-reactive protein, and clinical findings in dogs treated for aspiration pneumonia. J. Vet. Intern. Med. 2022, 36, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Venco, L.; Colaneri, G.; Formaggini, L.; De Franco, M.; Rishniw, M. Utility of thoracic ultrasonography in a rapid diagnosis of angiostrongylosis in young dogs presenting with respiratory distress. Vet. J. 2021, 271, 105649. [Google Scholar] [CrossRef]
- Łobaczewski, A.; Czopowicz, M.; Moroz, A.; Mickiewicz, M.; Sapierzyński, R.; Tarka, S.; Frymus, T.; Mądry, W.; Buczyński, M.; Szaluś-Jordanow, O. Integrated Basic Heart and Lung Ultrasound Examination for the Differentiation between Bacterial Pneumonia and Lung Neoplasm in Dogs-A New Diagnostic Algorithm. Animals 2022, 12, 1154. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Lo, P.Y.; Lam, M.C.; Wu, H.-D. Usefulness of Chest Ultrasonography in Predicting Diagnosis in Non-emergency Small Animal Patients With Lung Parenchymal and Pleural Disease. Front. Vet. Sci. 2020, 7, 616882. [Google Scholar] [CrossRef] [PubMed]
- Buda, N.; Kosiak, W.; Radzikowska, E.; Olszewski, R.; Jassem, E.; Grabczak, E.M.; Pomiecko, A.; PiotrkowskI, J.; Piskunowicz, M.; Sołtysiak, M.; et al. Polish recommendations for lung ultrasound in internal medicine (POLLUS-IM). J. Ultrason. 2018, 18, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Silva, F.; Radeos, M. Real-time lung ultrasound for the diagnosis of alveolar consolidation and interstitial syndrome in the emergency department. Eur. J. Emerg. Med. 2010, 17, 63–72. [Google Scholar] [CrossRef]
- Demi, L.; Wolfram, F.; Klersy, C.; De Silvestri, A.; Ferretti, V.V.; Muller, M.; Miller, D.; Feletti, F.; Wełnicki, M.; Buda, N.; et al. New International Guidelines and Consensus on the Use of Lung Ultrasound. J. Ultrasound Med. 2023, 42, 309–344. [Google Scholar] [CrossRef]
- Copetti, R.; Soldati, G.; Copetti, P. Chest sonography: A useful tool to differentiate acute cardiogenic pulmonary edema from acute respiratory distress syndrome. Cardiovasc. Ultrasound 2008, 6, 16. [Google Scholar] [CrossRef]
- Huang, D.; Ma, H.; Xiao, Z.; Blaivas, M.; Chen, Y.; Wen, J.; Guo, W.; Liang, J.; Liao, X.; Wang, Z.; et al. Diagnostic value of cardiopulmonary ultrasound in elderly patients with acute respiratory distress syndrome. BMC Pulm. Med. 2018, 18, 136. [Google Scholar] [CrossRef]
- Lichtenstein, D.A.; Mezière, G.A. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: The BLUE protocol. Chest 2008, 134, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Kameda, T.; Kamiyama, N.; Taniguchi, N. The Mechanisms Underlying Vertical Artifacts in Lung Ultrasound and Their Proper Utilization for the Evaluation of Cardiogenic Pulmonary Edema. Diagnostics 2022, 12, 252. [Google Scholar] [CrossRef]
- Schmickl, C.N.; Menon, A.A.; Dhokarh, R.; Seth, B.; Schembri, F. Optimizing B-lines on lung ultrasound: An in-vitro to in-vivo pilot study with clinical implications. J. Clin. Monit. Comput. 2020, 34, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Matthias, I.; Panebianco, N.L.; Maltenfort, M.G.; Dean, A.J.; Baston, C. Effect of Machine Settings on Ultrasound Assessment of B-lines. J. Ultrasound Med. 2020, 40, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Yang, P.C.; Lee, L.; Wu, H.-D.; Kuo, S.-H.; Luh, K.-T.; Chen, W.-J.; Lin, F.-Y. Reactive pulmonary artery vasoconstriction in pulmonary consolidation evaluated by color Doppler ultrasonography. Ultrasound Med. Biol. 2000, 26, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, V.L.; Abbott, J.; Chetboul, V.; Côté, E.; Fox, P.R.; Häggström, J.; Kittleson, M.D.; Schober, K.; Stern, J.A. ACVIM consensus statement guidelines for the classification, diagnosis, and management of cardiomyopathies in cats. J. Vet. Intern. Med. 2020, 34, 1062–1077. [Google Scholar] [CrossRef]
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.; Borgarelli, M.; Scansen, B.A. ACVIM consensus statement guidelines for the diagnosis, classification, treatment, and monitoring of pulmonary hypertension in dogs. J. Vet. Intern. Med. 2020, 34, 549–573. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, D.A. Lung Ultrasound in the Critically III; Springer: London, UK, 2016. [Google Scholar]
- Lisciandro, G.R.; Lisciandro, S.C. Lung Ultrasound Fundamentals, “Wet Versus Dry” Lung, Signs of Consolidation in Dogs and Cats. Vet. Clin. N. Am. Small Anim. Pract. 2021, 51, 1125–1140. [Google Scholar] [CrossRef] [PubMed]
- Lisciandro, G.R.; Puchot, M.L.; Gambino, J.M.; Lisciandro, S.C. The wedge sign: A possible lung ultrasound sign for pulmonary thromboembolism. J. Vet. Emerg. Crit. Care 2022, 32, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Boysen, S.; Gommeren, K.; Chalhoub, S. The Essentials of Veterinary Point of Care Ultrasound: Pleural Space and Lung; Edra Publishing: Palm Beach Gardens, FL, USA, 2022. [Google Scholar]
- Yang, P.C.; Luh, K.T.; Wu, H.D.; Chang, D.B.; Lee, L.N.; Kuo, S.H.; Yang, S.P. Lung tumors associated with obstructive pneumonitis: US studies. Radiology 1990, 174, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Gorg, C.; Seifart, U.; Gorg, K.; Zugmaier, G. Color Doppler sonographic mapping of pulmonary lesions: Evidence of dual arterial supply by spectral analysis. J. Ultrasound Med. 2003, 22, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Yang, P.C.; Chang, D.B. Pulmonary infarction: Use of color Doppler sonography for diagnosis and assessment of reperfusion of the lung. AJR Am. J. Roentgenol. 1993, 160, 419–420. [Google Scholar] [CrossRef] [PubMed]
- Buda, N.; Kosiak, W. Is a linear probe helpful in diagnosing diseases of pulmonary interstitial spaces? J. Ultrason. 2017, 17, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Sripathi, S.; Mahajan, A. Comparative study evaluating the role of color Doppler sonography and computed tomography in predicting chest wall invasion by lung tumors. J. Ultrasound Med. 2013, 32, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Chang, D.B.; Yu, C.J.; Kuo, S.H.; Luh, K.T.; Yang, P.C. Color Doppler sonography of benign and malignant pulmonary masses. AJR Am. J. Roentgenol. 1994, 163, 545–549. [Google Scholar] [CrossRef]
- Gorg, C.; Bert, T. Transcutaneous colour Doppler sonography of lung consolidations: Review and pictorial essay. Part 1: Pathophysiologic and colour Doppler sonographic basics of pulmonary vascularity. Ultraschall Med. 2004, 25, 221–226. [Google Scholar] [CrossRef]
- Burnotte, P.; Graziano, N.; Gommeren, K. A retrospective study on parapneumonic effusion in 130 dogs with a clinical diagnosis of pneumonia. Front. Vet. Sci. 2023, 10, 1144148. [Google Scholar] [CrossRef]
- Buda, N.; Kosiak, W.; Wełnicki, M.; Skoczylas, A.; Olszewski, R.; Piotrkowski, J.; Skoczyński, S.; Radzikowska, E.; Jassem, E.; Grabczak, E.M.; et al. Recommendations for Lung Ultrasound in Internal Medicine. Diagnostics 2020, 10, 597. [Google Scholar] [CrossRef] [PubMed]
- Rick, T.; Kleiter, M.; Schwendenwein, I.; Ludewig, E.; Reifinger, M.; Hittmair, K.M. Contrast-enhanced ultrasonography characteristics of intrathoracic mass lesions in 36 dogs and 24 cats. Vet. Radiol. Ultrasound 2019, 60, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Linta, N.; Toaldo, M.B.; Bettini, G.; Cordella, A.; Quinci, M.; Pey, P.; Galli, V.; Cipone, M.; Diana, A. The feasibility of contrast enhanced ultrasonography (CEUS) in the diagnosis of non-cardiac thoracic disorders of dogs and cats. BMC Vet. Res. 2017, 13, 141. [Google Scholar] [CrossRef]
- Yang, P.C. Color doppler ultrasound of pulmonary consolidation. Eur. J. Ultrasound 1996, 3, 169–178. [Google Scholar] [CrossRef]
- Hsu, W.H.; Ikezoe, J.; Chen, C.Y.; Kwan, P.C.; Hsu, C.P.; Hsu, N.Y.; Chiang, C.D.; Ho, W.L. Color Doppler ultrasound signals of thoracic lesions. Correlation with resected histologic specimens. Am. J. Respir. Crit. Care Med. 1996, 153, 1938–1951. [Google Scholar] [CrossRef] [PubMed]
- Mathis, G.; Gehmacher, O. Ultrasound-guided diagnostic and therapeutic interventions in peripheral pulmonary masses. Wien. Klin. Wochenschr. 1999, 111, 230–235. [Google Scholar] [PubMed]
- Mathis, G. Thoraxsonography—Part II: Peripheral pulmonary consolidation. Ultrasound Med. Biol. 1997, 23, 1141–1153. [Google Scholar] [CrossRef]
- Pacholec, C.; Lisciandro, G.; Masseau, I.; Donnelly, L.; DeClue, A.; Reinero, C. Lung ultrasound nodule sign for detection of pulmonary nodule lesions in dogs: Comparison to thoracic radiography using computed tomography as the criterion standard. Vet. J. 2021, 275, 105727. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.S.; Ramsey, I.K.; Thompson, H.; Cave, T.A.; Barr, F.J.; Rudorf, H.; Williams, A.; Sullivan, M. Thoracic high-resolution computed tomography in the diagnosis of metastatic carcinoma. J. Small Anim. Pract. 2004, 45, 134–143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Type of Airless Lung Tissue | Morphology | Types of Bronchogram | Echogenicity | Margins |
|---|---|---|---|---|
| Nodule |  |
| Hypoechoic | Smooth |
| Mass |  |
| Varied | Smooth |
| Shred |  |
| Hypoechoic | Irregular |
| Tissue |  |
| Varied | Smooth |
| Wedge |  |
| Hypoechoic | Smooth |
| Species | Breed | n | % |
|---|---|---|---|
| Canine | Mix breed | 179 | 28.20% |
| Yorkshire Terrier | 93 | 14.70% | |
| Cavalier King Charles Spaniel | 35 | 5.50% | |
| West Highland White Terrier | 29 | 4.60% | |
| Miniature Schnauzer | 23 | 3.60% | |
| French Bulldog | 21 | 3.30% | |
| Chihuahua | 20 | 3.20% | |
| Shih Tzu | 19 | 3.00% | |
| Dachshund | 18 | 2.80% | |
| Jack Russell Terrier | 17 | 2.70% | |
| Border Collie | 15 | 2.40% | |
| Maltese | 15 | 2.40% | |
| Beagle | 11 | 1.70% | |
| German Shepard | 11 | 1.70% | |
| Labrador Retriever | 10 | 1.60% | |
| Pug | 10 | 1.60% | |
| Maltipoo | 8 | 1.30% | |
| Miniature Pincher | 8 | 1.30% | |
| Other breeds | 92 | 14.5% | |
| Feline | DSH | 135 | 38.90% |
| Mix breed | 92 | 26.50% | |
| Maine Coon | 31 | 8.90% | |
| BSH | 24 | 6.90% | |
| Persian | 20 | 5.80% | |
| Syberian | 14 | 4.00% | |
| Oriental | 5 | 1.40% | |
| Ragdoll | 5 | 1.40% | |
| NFC | 5 | 1.40% | |
| Sphinx | 5 | 1.40% | |
| RBC | 4 | 1.20% | |
| Other breeds | 9 | 2.10% |
| Consolidation Type | n | % |
|---|---|---|
| Shred | 460 | 47.10% |
| Shred/Tissue | 145 | 14.80% |
| Mass | 99 | 10.10% |
| Nodule | 82 | 8.40% |
| Tissue | 77 | 7.90% |
| Mass/Tissue | 32 | 3.30% |
| Wedge | 25 | 2.60% |
| Shred/Wedge | 19 | 1.90% |
| Mass/Nodule | 18 | 1.80% |
| Shred/Nodule | 13 | 1.30% |
| Nodule/Tissue | 4 | 0.30% |
| Tissue/Wedge | 4 | 0.30% |
| Nodule/Wedge | 2 | 0.10% |
| All | 981 | 100.0% |
| Consolidation Type | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bronchogram Classification | S | S/T | M | N | T | M/T | W | S/W | M/N | S/N | χ2 | p | Vc | |
| Absent (n = 219) | n | 3 | 1 | 89 | 76 | 0 | 11 | 17 | 4 | 15 | 3 | 2073.85 | <0.001 | 0.57 |
| % | 1.0% | 0.7% | 93.7% | 97.4% | 0.0% | 34.4% | 94.4% | 30.8% | 93.8% | 27.3% | ||||
| Dynamic (n = 230) | n | 229 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 73.2% | 0.7% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Static (n = 42) | n | 18 | 5 | 0 | 0 | 17 | 0 | 0 | 1 | 0 | 1 | |||
| % | 5.8% | 3.5% | 0.0% | 0.0% | 23.9% | 0.0% | 0.0% | 7.7% | 0.0% | 9.1% | ||||
| Fluid (n = 16) | n | 1 | 0 | 0 | 0 | 13 | 2 | 0 | 0 | 0 | 0 | |||
| % | 0.3% | 0.0% | 0.0% | 0.0% | 18.3% | 6.3% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Dynamic and static (n = 137) | n | 59 | 73 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 2 | |||
| % | 18.8% | 50.7% | 1.1% | 0.0% | 1.4% | 3.1% | 0.0% | 0.0% | 0.0% | 18.2% | ||||
| Static and fluid (n = 52) | n | 3 | 11 | 0 | 0 | 38 | 0 | 0 | 0 | 0 | 0 | |||
| % | 1.0% | 7.6% | 0.0% | 0.0% | 53.5% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Dynamic, static and fluid (n = 54) | n | 0 | 53 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | |||
| % | 0.0% | 36.8% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 9.1% | ||||
| Dynamic and absent (n = 11) | n | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 | 0 | 3 | |||
| % | 0.0% | 0.0% | 0.0% | 1.3% | 0.0% | 3.1% | 5.6% | 38.5% | 0.0% | 27.3% | ||||
| Static and absent (n = 30) | n | 0 | 0 | 5 | 1 | 2 | 17 | 0 | 3 | 1 | 1 | |||
| % | 0.0% | 0.0% | 5.3% | 1.3% | 2.8% | 53.1% | 0.0% | 23.1% | 6.3% | 9.1% | ||||
| Consolidation Type | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vascularisation Type | S | S/T | M | N | T | M/T | W | S/W | M/N | S/N | χ2 | p | Vc | |
| Tree (n = 173) | n | 146 | 24 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 2 | 1011.32 | <0.001 | 0.69 |
| % | 88.0% | 30.0% | 0.0% | 0.0% | 2.7% | 0.0% | 0.0% | 0.0% | 0.0% | 33.3% | ||||
| Residual (n = 119) | n | 19 | 56 | 0 | 1 | 35 | 3 | 0 | 0 | 1 | 4 | |||
| % | 11.4% | 70.0% | 0.0% | 14.3% | 94.6% | 13.0% | 0.0% | 0.0% | 9.1% | 66.7% | ||||
| Chaotic (n = 91) | n | 0 | 0 | 59 | 6 | 0 | 16 | 0 | 0 | 10 | 0 | |||
| % | 0.0% | 0.0% | 86.8% | 85.7% | 0.0% | 69.6% | 0.0% | 0.0% | 90.9% | 0.0% | ||||
| Chaotic and penetrating (n = 8) | n | 0 | 0 | 6 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 8.8% | 0.0% | 0.0% | 8.7% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Penetrating (n = 5) | n | 0 | 0 | 3 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 4.4% | 0.0% | 0.0% | 8.7% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| “Vascular sign” (n = 31) | n | 1 | 0 | 0 | 0 | 1 | 0 | 17 | 12 | 0 | 0 | |||
| % | 0.6% | 0.0% | 0.0% | 0.0% | 2.7% | 0.0% | 100.0% | 100.0% | 0.0% | 0.0% | ||||
| Consolidation Type | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis | S | S/T | M | N | T or ATLP | M/T or ATLP | W | S/W | M/N | S/N | χ2 | p | Vc | |
| ARDS (n = 32) | n | 29 | 0 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 5040.92 | <0.001 | 0.76 |
| % | 6.3% | 0.0% | 0.0% | 0.0% | 2.6% | 0.0% | 4.0% | 0.0% | 0.0% | 0.0% | ||||
| PLD (n = 36) | n | 33 | 2 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |||
| % | 7.2% | 1.4% | 0.0% | 0.0% | 0.0% | 0.0% | 4.0% | 0.0% | 0.0% | 0.0% | ||||
| Tumor (n = 94) | n | 1 | 0 | 80 | 5 | 2 | 4 | 0 | 0 | 1 | 1 | |||
| % | 0.2% | 0.0% | 81.6% | 6.1% | 2.6% | 12.9% | 0.0% | 0.0% | 5.6% | 7.7% | ||||
| Tumor/Atelectasis (n = 42) | n | 0 | 1 | 11 | 1 | 3 | 25 | 0 | 0 | 1 | 0 | |||
| % | 0.0% | 0.7% | 11.2% | 1.2% | 3.9% | 80.6% | 0.0% | 0.0% | 5.6% | 0.0% | ||||
| Tumor/Metastasis (n = 24) | n | 0 | 0 | 3 | 5 | 0 | 0 | 0 | 0 | 16 | 2 | |||
| % | 0.0% | 0.0% | 3.1% | 6.1% | 0.0% | 0.0% | 0.0% | 0.0% | 88.9% | 15.4% | ||||
| Tumor/Granuloma (n = 1) | n | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 1.2% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Tumor/CHF (n = 3) | n | 0 | 0 | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 2.0% | 0.0% | 0.0% | 3.2% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Atelectasis (n = 41) | n | 1 | 8 | 0 | 0 | 30 | 0 | 0 | 0 | 0 | 1 | |||
| % | 0.2% | 5.5% | 0.0% | 0.0% | 39.0% | 0.0% | 0.0% | 0.0% | 0.0% | 7.7% | ||||
| Atelectasis/HF (n = 24) | n | 0 | 1 | 0 | 0 | 23 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.7% | 0.0% | 0.0% | 29.9% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Atelectasis/CHF/Parenchymal lung disease (n = 1) | n | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.7% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Pulmonary edema (n = 1) | n | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.2% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Metastases (n = 65) | n | 0 | 0 | 0 | 64 | 0 | 0 | 0 | 0 | 0 | 1 | |||
| % | 0.0% | 0.0% | 0.0% | 78.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 7.7% | ||||
| Metastases/Atelectasis (n = 5) | n | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 3 | |||
| % | 0.0% | 0.0% | 0.0% | 2.4% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 23.1% | ||||
| Pneumonia/ARDS (n = 15) | n | 10 | 3 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | |||
| % | 2.2% | 2.1% | 0.0% | 0.0% | 0.0% | 0.0% | 4.0% | 5.3% | 0.0% | 0.0% | ||||
| Pneumonia (n = 281) | n | 248 | 30 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 1 | |||
| % | 53.9% | 20.7% | 0.0% | 0.0% | 2.6% | 0.0% | 0.0% | 0.0% | 0.0% | 7.7% | ||||
| Pneumonia/PLD (n = 23) | n | 19 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 4.1% | 2.8% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Pneumonia/Atelectasis (n = 111) | n | 17 | 84 | 1 | 0 | 6 | 1 | 0 | 0 | 0 | 2 | |||
| % | 3.7% | 57.9% | 1.0% | 0.0% | 7.8% | 3.2% | 0.0% | 0.0% | 0.0% | 15.4% | ||||
| Pneumonia/Atelectasis/CHF (n = 2) | n | 0 | 8 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 5.5% | 0.0% | 0.0% | 2.6% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Pneumonia/Abscess (n = 3) | n | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |||
| % | 0.0% | 0.0% | 1.0% | 0.0% | 1.3% | 0.0% | 0.0% | 0.0% | 0.0% | 7.7% | ||||
| Pneumonia/PTE (n = 15) | n | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 12 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 12.0% | 63.2% | 0.0% | 0.0% | ||||
| Pneumonia/PTE/ARDS (n = 2) | n | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 10.5% | 0.0% | 0.0% | ||||
| Pneumonia/Granuloma (n = 1) | n | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 7.7% | ||||
| Pneumonia/CHF (n = 103) | n | 98 | 3 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | |||
| % | 21.3% | 2.1% | 0.0% | 0.0% | 2.6% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| Pneumonia/CHF/tracheal collapse (n = 1) | n | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.2% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| PTE (n = 18) | n | 1 | 0 | 0 | 0 | 0 | 0 | 14 | 3 | 0 | 0 | |||
| % | 0.2% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 56.0% | 15.8% | 0.0% | 0.0% | ||||
| Metastases/ARDS (n = 5) | n | 0 | 0 | 0 | 0 | 1 | 0 | 4 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 1.3% | 0.0% | 16.0% | 0.0% | 0.0% | 0.0% | ||||
| PTE/Metastasis (n = 0) | n | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| PTE/CHF (n = 2) | n | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 4.0% | 5.3% | 0.0% | 0.0% | ||||
| Granuloma (n = 4) | n | 0 | 0 | 0 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.0% | 0.0% | 0.0% | 4.9% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
| CHF (n = 4) | n | 1 | 0 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | |||
| % | 0.2% | 0.0% | 0.0% | 0.0% | 3.9% | 0.0% | 0.0% | 0.0% | 0.0% | 0.0% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kraszewska, K.; Gajewski, M.; Boysen, S.; Buda, N. Retrospective Evaluation of Subpleural Consolidations Using Lung Ultrasound in 634 Dogs and 347 Cats. Animals 2025, 15, 549. https://doi.org/10.3390/ani15040549
Kraszewska K, Gajewski M, Boysen S, Buda N. Retrospective Evaluation of Subpleural Consolidations Using Lung Ultrasound in 634 Dogs and 347 Cats. Animals. 2025; 15(4):549. https://doi.org/10.3390/ani15040549
Chicago/Turabian StyleKraszewska, Katarzyna, Michał Gajewski, Søren Boysen, and Natalia Buda. 2025. "Retrospective Evaluation of Subpleural Consolidations Using Lung Ultrasound in 634 Dogs and 347 Cats" Animals 15, no. 4: 549. https://doi.org/10.3390/ani15040549
APA StyleKraszewska, K., Gajewski, M., Boysen, S., & Buda, N. (2025). Retrospective Evaluation of Subpleural Consolidations Using Lung Ultrasound in 634 Dogs and 347 Cats. Animals, 15(4), 549. https://doi.org/10.3390/ani15040549