Traumatic Brain Injury, Sleep Disorders, and Psychiatric Disorders: An Underrecognized Relationship


Abstract
:1. Introduction
2. Anxiety
3. Major Depressive Disorder
4. ADHD
5. Post-Traumatic Stress Syndrome
6. Crossover Pathophysiology of TBI, Sleep, and Psychiatric Disorders
7. Evaluation and Treatment Options
8. Discussion and Future Direction
Conflicts of Interest
References
- Eme, R. ADHD: An integration with pediatric traumatic brain injury. Expert Rev. Neurother. 2012, 12, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Schachar, R.J.; Park, L.S.; Dennis, M. Mental Health Implications of Traumatic Brain Injury (TBI) in Children and Youth. J. Can. Acad. Child Adolesc. Psychiatry 2015, 24, 100–108. [Google Scholar] [PubMed]
- Veliz, P.; McCabe, S.E.; Eckner, J.T.; Schulenberg, J.E. Prevalence of concussion among us adolescents and correlated factors. JAMA 2017, 318, 1180–1182. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Liu, J. The effect of pediatric traumatic brain injury on behavioral outcomes: A systematic review. Dev. Med. Child Neurol. 2013, 55, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.L.; Hughes, S.J.; O’Connor, P.A. Preschool behavior problems and subsequent risk of injury. Pediatrics 1988, 82, 644–651. [Google Scholar] [PubMed]
- Bijur, P.E.; Haslum, M.; Golding, J. Cognitive and behavioral sequelae of mild head injury in children. Pediatrics 1990, 86, 337–344. [Google Scholar] [PubMed]
- McKinlay, A.; Kyonka, E.G.; Grace, R.C.; Horwood, L.J.; Fergusson, D.M.; MacFarlane, M.R. An investigation of the pre-injury risk factors associated with children who experience traumatic brain injury. Inj. Prev. 2010, 16, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Bijur, P.; Golding, J.; Haslum, M.; Kurzon, M. Behavioral predictors of injury in school-age children. Am. J. Dis. Child. 1988, 142, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Max, J.E.; Schachar, R.J.; Levin, H.S.; Ewing-Cobbs, L.; Chapman, S.B.; Dennis, M.; Saunders, A.; Landis, J. Predictors of attention-deficit/hyperactivity disorder within 6 months after pediatric traumatic brain injury. J. Can. Acad. Child Adolesc. Psychiatry 2005, 44, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.; Micky, C. Acute Concussion Evaluation (ACE): Physicial/Clincian Office Version. 27 April 2006. 2016. Available online: https://www.cdc.gov/headsup/pdfs/providers/ace-a.pdf (accessed on 19 September 2017).
- Kirkwood, M.W.; Yeates, K.O.; Taylor, H.G.; Randolph, C.; McCrea, M.; Anderson, V.A. Management of pediatric mild traumatic brain injury: A neuropsychological review from injury through recovery. Clin. Neuropsychol. 2008, 22, 769–800. [Google Scholar] [CrossRef] [PubMed]
- Mittenberg, W.; Wittner, M.S.; Miller, L.J. Postconcussion syndrome occurs in children. Neuropsychology 1997, 11, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Ponsford, J.; Willmott, C.; Rothwell, A.; Cameron, P.; Ayton, G.; Nelms, R.; Curran, C.; Ng, K.T. Cognitive and behavioral outcome following mild traumatic head injury in children. J. Head Trauma Rehabil. 1999, 14, 360–372. [Google Scholar] [CrossRef] [PubMed]
- Yeates, K.O.; Luria, J.; Bartkowski, H.; Rusin, J.; Martin, L.; Bigler, E.D. Postconcussive symptoms in children with mild closed head injuries. J. Head Trauma Rehabil. 1999, 14, 337–350. [Google Scholar] [CrossRef] [PubMed]
- McInnes, K.; Friesen, C.L.; MacKenzie, D.E.; Westwood, D.A.; Boe, S.G. Mild Traumatic Brain Injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS ONE 2017, 12, e0174847. [Google Scholar] [CrossRef] [PubMed]
- Coronado, V.G.; Haileyesus, T.; Cheng, T.A.; Bell, J.M.; Haarbauer-Krupa, J.; Lionbarger, M.R.; Flores-Herrera, J.; McGuire, L.C.; Gilchrist, J. Trends in Sports- and Recreation-Related Traumatic Brain Injuries Treated in US Emergency Departments: The National Electronic Injury Surveillance System-All Injury Program (NEISS-AIP) 2001–2012. J. Head Trauma Rehabil. 2015, 30, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Kenzie, E.S.; Parks, E.L.; Bigler, E.D.; Lim, M.M.; Chesnutt, J.C.; Wakeland, W. Concussion As a Multi-Scale Complex System: An Interdisciplinary Synthesis of Current Knowledge. Front. Neurol. 2017, 8, 513. [Google Scholar] [CrossRef] [PubMed]
- Nakase-Richardson, R.; Sherer, M.; Barnett, S.D.; Yablon, S.A.; Evans, C.C.; Kretzmer, T.; Schwartz, D.J.; Modarres, M. Prospective evaluation of the nature, course, and impact of acute sleep abnormality after traumatic brain injury. Arch. Phys. Med. Rehabil. 2013, 94, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Chaput, G.; Giguere, J.F.; Chauny, J.M.; Denis, R.; Lavigne, G. Relationship among subjective sleep complaints, headaches, and mood alterations following a mild traumatic brain injury. Sleep Med. 2009, 10, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.; Sharpe, M.H.; Metzer, J. Outcomes 5 years post-traumatic brain injury (with further reference to neurophysical impairment and disability). Brain Inj. 1997, 11, 661–675. [Google Scholar] [PubMed]
- Huang, C.T.; Lin, W.C.; Ho, C.H.; Tung, L.C.; Chu, C.C.; Chou, W.; Wang, C.H. Incidence of severe dysphagia after brain surgery in pediatric traumatic brain injury: A nationwide population-based retrospective study. J. Head Trauma Rehabil. 2014, 29, E31–E36. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.; Ward, E.; Murdoch, B.; Kennedy, B.; Murison, R. Incidence, characteristics, and predictive factors for dysphagia after pediatric traumatic brain injury. J. Head Trauma Rehabil. 2003, 18, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Max, J.E.; Keatley, E.; Wilde, E.A.; Bigler, E.D.; Levin, H.S.; Schachar, R.J.; Saunders, A.; Ewing-Cobbs, L.; Chapman, S.B.; Dennis, M.; et al. Anxiety disorders in children and adolescents in the first six months after traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 2011, 23, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.; Taylor, H.G.; Drotar, D.; Yeates, K.O.; Wade, S.L.; Stancin, T. Long-term behavior problems following pediatric traumatic brain injury: Prevalence, predictors, and correlates. J. Pediatr. Psychol. 2003, 28, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Catroppa, C.; Anderson, V.A.; Morse, S.A.; Haritou, F.; Rosenfeld, J.V. Outcome and predictors of functional recovery 5 years following pediatric traumatic brain injury (TBI). J. Pediatr. Psychol. 2008, 33, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Ellis, M.J.; Ritchie, L.J.; Koltek, M.; Hosain, S.; Cordingley, D.; Chu, S.; Selci, E.; Leiter, J.; Russell, K. Psychiatric outcomes after pediatric sports-related concussion. J. Neurosurg. Pediatr. 2015, 16, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Smyth, K.; Sandhu, S.S.; Crawford, S.; Dewey, D.; Parboosingh, J.; Barlow, K.M. The role of serotonin receptor alleles and environmental stressors in the development of post-concussive symptoms after pediatric mild traumatic brain injury. Dev. Med. Child Neurol. 2014, 56, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Shay, N.; Yeates, K.O.; Walz, N.C.; Stancin, T.; Taylor, H.G.; Beebe, D.W.; Caldwell, C.T.; Krivitzky, L.; Cassedy, A.; Wade, S.L. Sleep problems and their relationship to cognitive and behavioral outcomes in young children with traumatic brain injury. J. Neurotrauma 2014, 31, 1305–1312. [Google Scholar] [CrossRef] [PubMed]
- Kostyun, R.O.; Milewski, M.D.; Hafeez, I. Sleep disturbance and neurocognitive function during the recovery from a sport-related concussion in adolescents. Am. J. Sports Med. 2015, 43, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Hooper, S.R.; Alexander, J.; Moore, D.; Sasser, H.C.; Laurent, S.; King, J.; Bartel, S.; Callahan, B. Caregiver reports of common symptoms in children following a traumatic brain injury. NeuroRehabilitation 2004, 19, 175–189. [Google Scholar] [PubMed]
- Keightley, M.L.; Cote, P.; Rumney, P.; Hung, R.; Carroll, L.J.; Cancelliere, C.; Cassidy, J.D. Psychosocial consequences of mild traumatic brain injury in children: Results of a systematic review by the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95, S192–S200. [Google Scholar] [CrossRef] [PubMed]
- Ornstein, T.J.; Sagar, S.; Schachar, R.J.; Ewing-Cobbs, L.; Chapman, S.B.; Dennis, M.; Saunders, A.E.; Yang, T.T.; Levin, H.S.; Max, J.E. Neuropsychological performance of youth with secondary attention-deficit/hyperactivity disorder 6- and 12-months after traumatic brain injury. J. Int. Neuropsychol. Soc. 2014, 20, 971–981. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.A.; Kenardy, J.A.; Dow, B.L. PTSD perpetuates pain in children with traumatic brain injury. J. Pediatr. Psychol. 2014, 39, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Kovachy, B.; O’Hara, R.; Hawkins, N.; Gershon, A.; Primeau, M.M.; Madej, J.; Carrion, V. Sleep disturbance in pediatric PTSD: Current findings and future directions. J. Clin. Sleep Med. 2013, 9, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Ruff, R.L.; Blake, K. Pathophysiological links between traumatic brain injury and post-traumatic headaches. F1000Research 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Kenardy, J.; Le Brocque, R.; Hendrikz, J.; Iselin, G.; Anderson, V.; McKinlay, L. Impact of posttraumatic stress disorder and injury severity on recovery in children with traumatic brain injury. J. Clin. Child Adolesc. Psychol. 2012, 41, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Morse, A.M.; Tkachenko, N.; Kothare, S.V. Sleep Disorders Associated With Traumatic Brain Injury-A Review. Pediatr. Neurol. 2016, 60, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Masel, B.E.; DeWitt, D.S. Traumatic brain injury: A disease process, not an event. J. Neurotrauma 2010, 27, 1529–1540. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.R.; Levin, H.S.; Ewing-Cobbs, L.; Saunders, A.E.; Song, J.; Fletcher, J.M.; Kowatch, R.A. Lifetime and novel psychiatric disorders after pediatric traumatic brain injury. J. Can. Acad. Child Adolesc. Psychiatry 2001, 40, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Hajek, C.A.; Yeates, K.O.; Gerry Taylor, H.; Bangert, B.; Dietrich, A.; Nuss, K.E.; Rusin, J.; Wright, M. Relationships among post-concussive symptoms and symptoms of PTSD in children following mild traumatic brain injury. Brain Inj. 2010, 24, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Bock, S.; Grim, R.; Barron, T.F.; Wagenheim, A.; Hu, Y.E.; Hendell, M.; Deitch, J.; Deibert, E. Factors associated with delayed recovery in athletes with concussion treated at a pediatric neurology concussion clinic. Childs Nerv. Syst. 2015, 31, 2111–2116. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.H.; Gill, C.; Kuhn, E.N.; Rocque, B.G.; Menendez, J.Y.; O’Neill, J.A.; Agee, B.S.; Brown, S.T.; Crowther, M.; Davis, R.D.; et al. Predictors of delayed recovery following pediatric sports-related concussion: A case-control study. J. Neurosurg. Pediatr. 2016, 17, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, K.S.; Kark, S.M.; Gehrman, P.; Bogdanova, Y. Sleep disturbances, TBI and PTSD: Implications for treatment and recovery. Clin. Psychol. Rev. 2015, 40, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xu, Z.; Zhao, K.; Chen, T.; Ye, X.; Shen, Z.; Wu, Z.; Shen, X.; Li, S. Sleep Habits, Sleep Problems, Sleep Hygiene, and Their Associations With Mental Health Problems Among Adolescents. J. Am. Psychiatr. Nurses Assoc. 2017. [Google Scholar] [CrossRef] [PubMed]
- Luis, C.A.; Mittenberg, W. Mood and anxiety disorders following pediatric traumatic brain injury: A prospective study. J. Clin. Exp. Neuropsychol. 2002, 24, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Beesdo, K.; Knappe, S.; Pine, D.S. Anxiety and anxiety disorders in children and adolescents: Developmental issues and implications for DSM-V. Psychiatr. Clin. N. Am. 2009, 32, 483–524. [Google Scholar] [CrossRef] [PubMed]
- Vasa, R.A.; Gerring, J.P.; Grados, M.; Slomine, B.; Christensen, J.R.; Rising, W.; Denckla, M.B.; Riddle, M.A. Anxiety after severe pediatric closed head injury. J. Can. Acad. Child Adolesc. Psychiatry 2002, 41, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Ginsburg, G.S.; Kingery, J.N. Sleep-related problems among children and adolescents with anxiety disorders. J. Can. Acad. Child Adolesc. Psychiatry 2007, 46, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Weiner, C.L.; Meredith Elkins, R.; Pincus, D.; Comer, J. Anxiety sensitivity and sleep-related problems in anxious youth. J. Anxiety Disord. 2015, 32, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Cantor, J.B.; Bushnik, T.; Cicerone, K.; Dijkers, M.P.; Gordon, W.; Hammond, F.M.; Kolakowsky-Hayner, S.A.; Lequerica, A.; Nguyen, M.; Spielman, L.A. Insomnia, fatigue, and sleepiness in the first 2 years after traumatic brain injury: An NIDRR TBI model system module study. J. Head Trauma Rehabil. 2012, 27, E1-14. [Google Scholar] [CrossRef] [PubMed]
- Max, J.E.; Keatley, E.; Wilde, E.A.; Bigler, E.D.; Schachar, R.J.; Saunders, A.E.; Ewing-Cobbs, L.; Chapman, S.B.; Dennis, M.; Yang, T.T.; et al. Depression in children and adolescents in the first 6 months after traumatic brain injury. Int. J. Dev. Neurosci. 2012, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Max, J.E.; Koele, S.L.; Smith, W.L., Jr.; Sato, Y.; Lindgren, S.D.; Robin, D.A.; Arndt, S. Psychiatric disorders in children and adolescents after severe traumatic brain injury: A controlled study. J. Can. Acad. Child Adolesc. Psychiatry 1998, 37, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Jorge, R.E.; Robinson, R.G.; Moser, D.; Tateno, A.; Crespo-Facorro, B.; Arndt, S. Major depression following traumatic brain injury. Arch. Gen. Psychiatry 2004, 61, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Rao, V.; McCann, U.; Han, D.; Bergey, A.; Smith, M.T. Does acute TBI-related sleep disturbance predict subsequent neuropsychiatric disturbances? Brain Inj. 2014, 28, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Duong, H.T. The prospective association between sleep deprivation and depression among adolescents. Sleep 2014, 37, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Duong, H.T. Depression and insomnia among adolescents: A prospective perspective. J. Affect. Disord. 2013, 148, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Jorge, R.E.; Robinson, R.G.; Arndt, S.V.; Forrester, A.W.; Geisler, F.; Starkstein, S.E. Comparison between acute- and delayed-onset depression following traumatic brain injury. J. Neuropsychiatry Clin. Neurosci. 1993, 5, 43–49. [Google Scholar] [CrossRef] [PubMed]
- DiScala, C.; Lescohier, I.; Barthel, M.; Li, G. Injuries to children with attention deficit hyperactivity disorder. Pediatrics 1998, 102, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Hoare, P.; Beattie, T. Children with attention deficit hyperactivity disorder and attendance at hospital. Eur. J. Emerg. Med. 2003, 10, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Bonfield, C.M.; Lam, S.; Lin, Y.; Greene, S. The impact of attention deficit hyperactivity disorder on recovery from mild traumatic brain injury. J. Neurosurg. Pediatr. 2013, 12, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Gerring, J.P.; Brady, K.D.; Chen, A.; Vasa, R.; Grados, M.; Bandeen-Roche, K.J.; Bryan, R.N.; Denckla, M.B. Premorbid prevalence of ADHD and development of secondary ADHD after closed head injury. J. Can. Acad. Child Adolesc. Psychiatry 1998, 37, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Keenan, H.T.; Hall, G.C.; Marshall, S.W. Early head injury and attention deficit hyperactivity disorder: Retrospective cohort study. BMJ 2008, 337, a1984. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A. The ADHD and sleep conundrum: A review. J. Dev. Behav. Pediatr. 2005, 26, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, O.; Okuyaz, C.; Gunes, S.; Ekinci, N.; Orekeci, G.; Teke, H.; Cobanogullari Direk, M. Sleep and quality of life in children with traumatic brain injury and ADHD. Int. J. Psychiatry Med. 2017, 52, 72–87. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Harvey, A.G. Postconcussive symptoms and posttraumatic stress disorder after mild traumatic brain injury. J. Nerv. Ment. Dis. 1999, 187, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Levi, R.B.; Drotar, D.; Yeates, K.O.; Taylor, H.G. Posttraumatic stress symptoms in children following orthopedic or traumatic brain injury. J. Clin. Child Psychol. 1999, 28, 232–243. [Google Scholar] [CrossRef] [PubMed]
- de Vries, A.P.; Kassam-Adams, N.; Cnaan, A.; Sherman-Slate, E.; Gallagher, P.R.; Winston, F.K. Looking beyond the physical injury: Posttraumatic stress disorder in children and parents after pediatric traffic injury. Pediatrics 1999, 104, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Pinto, P.S.; Meoded, A.; Poretti, A.; Tekes, A.; Huisman, T.A. The unique features of traumatic brain injury in children. review of the characteristics of the pediatric skull and brain, mechanisms of trauma, patterns of injury, complications, and their imaging findings—Part 2. J. Neuroimaging 2012, 22, e18-41. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R. Post-traumatic stress disorder vs traumatic brain injury. Dialogues Clin. Neurosci. 2011, 13, 251–262. [Google Scholar] [PubMed]
- Guo, X.; Edmed, S.L.; Anderson, V.; Kenardy, J. Neurocognitive predictors of posttraumatic stress disorder symptoms in children 6 months after traumatic brain injury: A prospective study. Neuropsychology 2017, 31, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Ventura, T.; Harrison-Felix, C.; Carlson, N.; Diguiseppi, C.; Gabella, B.; Brown, A.; Devivo, M.; Whiteneck, G. Mortality after discharge from acute care hospitalization with traumatic brain injury: A population-based study. Arch. Phys. Med. Rehabil. 2010, 91, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Macera, C.A.; Aralis, H.J.; Rauh, M.J.; MacGregor, A.J. Do sleep problems mediate the relationship between traumatic brain injury and development of mental health symptoms after deployment? Sleep 2013, 36, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Viola-Saltzman, M.; Watson, N.F. Traumatic brain injury and sleep disorders. Neurol. Clin. 2012, 30, 1299–1312. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.L.; Scafidi, S.; McKenna, M.C.; Fiskum, G. Mitochondrial mechanisms of cell death and neuroprotection in pediatric ischemic and traumatic brain injury. Exp. Neurol. 2009, 218, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Kochanek, P.M.; Clark, R.S.; Ruppel, R.A.; Adelson, P.D.; Bell, M.J.; Whalen, M.J.; Robertson, C.L.; Satchell, M.A.; Seidberg, N.A.; Marion, D.W.; et al. Biochemical, cellular, and molecular mechanisms in the evolution of secondary damage after severe traumatic brain injury in infants and children: Lessons learned from the bedside. Pediatr. Crit. Care Med. 2000, 1, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.; Guger, S.; Roncadin, C.; Barnes, M.; Schachar, R. Attentional-inhibitory control and social-behavioral regulation after childhood closed head injury: Do biological, developmental, and recovery variables predict outcome? J. Int. Neuropsychol. Soc. 2001, 7, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Sesma, H.W.; Slomine, B.S.; Ding, R.; McCarthy, M.L. Executive functioning in the first year after pediatric traumatic brain injury. Pediatrics 2008, 121, e1686–e1695. [Google Scholar] [CrossRef] [PubMed]
- Tlustos, S.J.; Peter Chiu, C.Y.; Walz, N.C.; Wade, S.L. Neural substrates of inhibitory and emotional processing in adolescents with traumatic brain injury. J. Pediatr. Rehabil. Med. 2015, 8, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Saper, C.B.; Fuller, P.M.; Pedersen, N.P.; Lu, J.; Scammell, T.E. Sleep state switching. Neuron 2010, 68, 1023–1042. [Google Scholar] [CrossRef] [PubMed]
- Sukumaran, T.U. Pediatric sleep project. Indian Pediatr. 2011, 48, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Shekleton, J.A.; Parcell, D.L.; Redman, J.R.; Phipps-Nelson, J.; Ponsford, J.L.; Rajaratnam, S.M. Sleep disturbance and melatonin levels following traumatic brain injury. Neurology 2010, 74, 1732–1738. [Google Scholar] [CrossRef] [PubMed]
- Nardone, R.; Bergmann, J.; Kunz, A.; Caleri, F.; Seidl, M.; Tezzon, F.; Gerstenbrand, F.; Trinka, E.; Golaszewski, S. Cortical excitability changes in patients with sleep-wake disturbances after traumatic brain injury. J. Neurotrauma 2011, 28, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Baumann, C.R.; Stocker, R.; Imhof, H.G.; Trentz, O.; Hersberger, M.; Mignot, E.; Bassetti, C.L. Hypocretin-1 (orexin A) deficiency in acute traumatic brain injury. Neurology 2005, 65, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Nishino, S.; Ripley, B.; Overeem, S.; Lammers, G.J.; Mignot, E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000, 355, 39–40. [Google Scholar] [CrossRef]
- Brundin, L.; Bjorkqvist, M.; Petersen, A.; Traskman-Bendz, L. Reduced orexin levels in the cerebrospinal fluid of suicidal patients with major depressive disorder. Eur. Neuropsychopharmacol. 2007, 17, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.; Ponz, A.; Poryazova, R.; Werth, E.; Boesiger, P.; Khatami, R.; Bassetti, C.L. Abnormal activity in hypothalamus and amygdala during humour processing in human narcolepsy with cataplexy. Brain 2008, 131, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Chao, H.; Li, Z.; Xu, X.; Liu, Y.; Hou, L.; Liu, N.; Ji, J. Melatonin attenuates traumatic brain injury-induced inflammation: A possible role for mitophagy. J. Pineal Res. 2016, 61, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Tan, D.X.; Kim, S.J.; Cruz, M.H. Delivery of pineal melatonin to the brain and SCN: Role of canaliculi, cerebrospinal fluid, tanycytes and Virchow-Robin perivascular spaces. Brain Struct. Funct. 2014, 219, 1873–1887. [Google Scholar] [CrossRef] [PubMed]
- Seifman, M.A.; Adamides, A.A.; Nguyen, P.N.; Vallance, S.A.; Cooper, D.J.; Kossmann, T.; Rosenfeld, J.V.; Morganti-Kossmann, M.C. Endogenous melatonin increases in cerebrospinal fluid of patients after severe traumatic brain injury and correlates with oxidative stress and metabolic disarray. J. Cereb. Blood Flow Metab. 2008, 28, 684–696. [Google Scholar] [CrossRef] [PubMed]
- Parcell, D.L.; Ponsford, J.L.; Redman, J.R.; Rajaratnam, S.M. Poor sleep quality and changes in objectively recorded sleep after traumatic brain injury: A preliminary study. Arch. Phys. Med. Rehabil. 2008, 89, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Cajochen, C.; Krauchi, K.; Mori, D.; Graw, P.; Wirz-Justice, A. Melatonin and S-20098 increase REM sleep and wake-up propensity without modifying NREM sleep homeostasis. Am. J. Physiol. 1997, 272, R1189–R1196. [Google Scholar] [CrossRef] [PubMed]
- Liberman, A.R.; Kwon, S.B.; Vu, H.T.; Filipowicz, A.; Ay, A.; Ingram, K.K. Circadian Clock Model Supports Molecular Link Between PER3 and Human Anxiety. Sci. Rep. 2017, 7, 9893. [Google Scholar] [CrossRef] [PubMed]
- Charrier, A.; Olliac, B.; Roubertoux, P.; Tordjman, S. Clock Genes and Altered Sleep-Wake Rhythms: Their Role in the Development of Psychiatric Disorders. Int. J. Mol. Sci. 2017, 18, 938. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.M.; McAllister, T.W.; Arciniegas, D.B. Depression and cognitive complaints following mild traumatic brain injury. Am. J. Psychiatry 2009, 166, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Alderfer, B.S.; Arciniegas, D.B.; Silver, J.M. Treatment of depression following traumatic brain injury. J. Head Trauma Rehabil. 2005, 20, 544–562. [Google Scholar] [CrossRef] [PubMed]
- Arciniegas, D.B.; Anderson, C.A.; Topkoff, J.; McAllister, T.W. Mild traumatic brain injury: A neuropsychiatric approach to diagnosis, evaluation, and treatment. Neuropsychiatr. Dis. Treat. 2005, 1, 311–327. [Google Scholar] [PubMed]
- Arciniegas, D.B.; Silver, J.M. Pharmacotherapy of posttraumatic cognitive impairments. Behav. Neurol. 2006, 17, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Levin, H.; Hanten, G.; Max, J.; Li, X.; Swank, P.; Ewing-Cobbs, L.; Dennis, M.; Menefee, D.S.; Schachar, R. Symptoms of attention-deficit/hyperactivity disorder following traumatic brain injury in children. J. Dev. Behav. Pediatr. 2007, 28, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Willmott, C.; Ponsford, J. Efficacy of methylphenidate in the rehabilitation of attention following traumatic brain injury: A randomised, crossover, double blind, placebo controlled inpatient trial. J. Neurol. Neurosurg. Psychiatry 2009, 80, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Leonetti, A.; Jaffe, K.; Katon, W.J.; Cummings, P.; Thompson, R.S. Psychiatric illness and subsequent traumatic brain injury: A case control study. J. Neurol. Neurosurg. Psychiatry 2002, 72, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Max, J.E.; Lansing, A.E.; Koele, S.L.; Castillo, C.S.; Bokura, H.; Schachar, R.; Collings, N.; Williams, K.E. Attention deficit hyperactivity disorder in children and adolescents following traumatic brain injury. Dev. Neuropsychol. 2004, 25, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Seda, G.; Sanchez-Ortuno, M.M.; Welsh, C.H.; Halbower, A.C.; Edinger, J.D. Comparative meta-analysis of prazosin and imagery rehearsal therapy for nightmare frequency, sleep quality, and posttraumatic stress. J. Clin. Sleep Med. 2015, 11, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Ouellet, M.C.; Morin, C.M. Efficacy of cognitive-behavioral therapy for insomnia associated with traumatic brain injury: A single-case experimental design. Arch. Phys. Med. Rehabil. 2007, 88, 1581–1592. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Brent, D.; Bernet, W.; Bukstein, O.; Walter, H.; Benson, R.S.; Chrisman, A.; Farchione, T.; Greenhill, L.; Hamilton, J.; et al. Practice parameter for the assessment and treatment of children and adolescents with depressive disorders. J. Can. Acad. Child Adolesc. Psychiatry 2007, 46, 1503–1526. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, G.S.; Becker, E.M.; Keeton, C.P.; Sakolsky, D.; Piacentini, J.; Albano, A.M.; Compton, S.N.; Iyengar, S.; Sullivan, K.; Caporino, N.; et al. Naturalistic follow-up of youths treated for pediatric anxiety disorders. JAMA Psychiatry 2014, 71, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, G.S.; Kendall, P.C.; Sakolsky, D.; Compton, S.N.; Piacentini, J.; Albano, A.M.; Walkup, J.T.; Sherrill, J.; Coffey, K.A.; Rynn, M.A.; et al. Remission after acute treatment in children and adolescents with anxiety disorders: Findings from the CAMS. J. Consult. Clin. Psychol. 2011, 79, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.; Brown, L.; Brown, R.T.; DuPaul, G.; Earls, M.; Feldman, H.M.; Ganiats, T.G.; Kaplanek, B.; Meyer, B.; Perrin, J.; et al. ADHD: Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2011, 128, 1007–1022. [Google Scholar] [PubMed]
- Pliszka, S. Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J. Can. Acad. Child Adolesc. Psychiatry 2007, 46, 894–921. [Google Scholar] [CrossRef] [PubMed]
- Pliszka, S.R.; Crismon, M.L.; Hughes, C.W.; Corners, C.K.; Emslie, G.J.; Jensen, P.S.; McCracken, J.T.; Swanson, J.M.; Lopez, M. The Texas Children’s Medication Algorithm Project: Revision of the algorithm for pharmacotherapy of attention-deficit/hyperactivity disorder. J. Can. Acad. Child Adolesc. Psychiatry 2006, 45, 642–657. [Google Scholar] [CrossRef] [PubMed]
- Akinsanya, A.; Marwaha, R.; Tampi, R.R. Prazosin in Children and Adolescents With Posttraumatic Stress Disorder Who Have Nightmares: A Systematic Review. J. Clin. Psychopharmacol. 2017, 37, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.A.; Mannarino, A.P.; Murray, L.K. Trauma-focused CBT for youth who experience ongoing traumas. Child Abuse Negl. 2011, 35, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Connor, D.F.; Grasso, D.J.; Slivinsky, M.D.; Pearson, G.S.; Banga, A. An open-label study of guanfacine extended release for traumatic stress related symptoms in children and adolescents. J. Child Adolesc. Psychopharmacol. 2013, 23, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S.; Biswas, R.; Neumann, V.; Coughlan, A. The value of melatonin for sleep disorders occurring post-head injury: A pilot RCT. Brain Inj. 2004, 18, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Menn, S.J.; Yang, R.; Lankford, A. Armodafinil for the treatment of excessive sleepiness associated with mild or moderate closed traumatic brain injury: A 12-week, randomized, double-blind study followed by a 12-month open-label extension. J. Clin. Sleep Med. 2014, 10, 1181–1191. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, P.R.; Valko, P.O.; Werth, E.; Thomann, J.; Meier, J.; Stocker, R.; Bassetti, C.L.; Baumann, C.R. Modafinil ameliorates excessive daytime sleepiness after traumatic brain injury. Neurology 2010, 75, 1780–1785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastore, V.; Colombo, K.; Liscio, M.; Galbiati, S.; Adduci, A.; Villa, F.; Strazzer, S. Efficacy of cognitive behavioural therapy for children and adolescents with traumatic brain injury. Disabil. Rehabil. 2011, 33, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Wade, S.L.; Kurowski, B.G.; Kirkwood, M.W.; Zhang, N.; Cassedy, A.; Brown, T.M.; Nielsen, B.; Stancin, T.; Taylor, H.G. Online problem-solving therapy after traumatic brain injury: A randomized controlled trial. Pediatrics 2015, 135, e487–e495. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, K.L.; Ponsford, J.L.; Taffe, J.; Lockley, S.W.; Rajaratnam, S.M. Randomized controlled trial of light therapy for fatigue following traumatic brain injury. Neurorehabil. Neural Repair 2014, 28, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Zollman, F.S.; Larson, E.B.; Wasek-Throm, L.K.; Cyborski, C.M.; Bode, R.K. Acupuncture for treatment of insomnia in patients with traumatic brain injury: A pilot intervention study. J. Head Trauma Rehabil. 2012, 27, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Rhine, T.; Cassedy, A.; Yeates, K.O.; Taylor, H.G.; Kirkwood, M.W.; Wade, S.L. Investigating the Connection Between Traumatic Brain Injury and Posttraumatic Stress Symptoms in Adolescents. J. Head Trauma Rehabil. 2017. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.C.; Barraclough, B. Suicide as an outcome for mental disorders. A meta-analysis. Br. J. Psychiatry 1997, 170, 205–228. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Psychosocial characteristics of adolescents with a history of suicide attempt. J. Can. Acad. Child Adolesc. Psychiatry 1993, 32, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Teasdale, T.W.; Engberg, A.W. Suicide after traumatic brain injury: A population study. J. Neurol. Neurosurg. Psychiatry 2001, 71, 436–440. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| TBI Risk Factors |
|---|
| Low Socioeconomic Status |
| Overcrowded households |
| Disadvantaged neighborhoods |
| High incidence of adverse life events |
| Young maternal age |
| Older siblings with few younger siblings |
| Previous TBI |
| Retrospective | Prospective | Overlap | Discrepancy |
|---|---|---|---|
| Male gender Lower socioeconomic status (SES) Behavioral problems Attention deficit hyperactivity disorder (ADHD) Cognitive problems Contact Sports Participation Competitive Sports Participation | Male gender Behavioral problems Adverse family events during childhood Punitive parenting practices Maternal depression Maternal age Maternal education | Male Gender Behavioral Problems | SES status Maternal features Cognitive baseline Sports Participation |
| Post-Concussive Symptoms | Prevalence | |
|---|---|---|
| Physical | Headache | 25–47% |
| Nausea | 7–12% | |
| Dizziness | 30% | |
| Fatigue | 16–40% | |
| Problems with Balance and Gait | 24–34% | |
| Light and Sound Sensitivity | 1–4% | |
| Emotional | Emotional Lability | 1–40% |
| Increased Anxiety | 8–17% | |
| Cognitive | Cognitive Deficits | 7–22% |
| Language Impairment | 1–68% | |
| Disorientation and Amnesia | 21–30% | |
| Sleep | Sleep–Wake Disturbance | 13–67% |
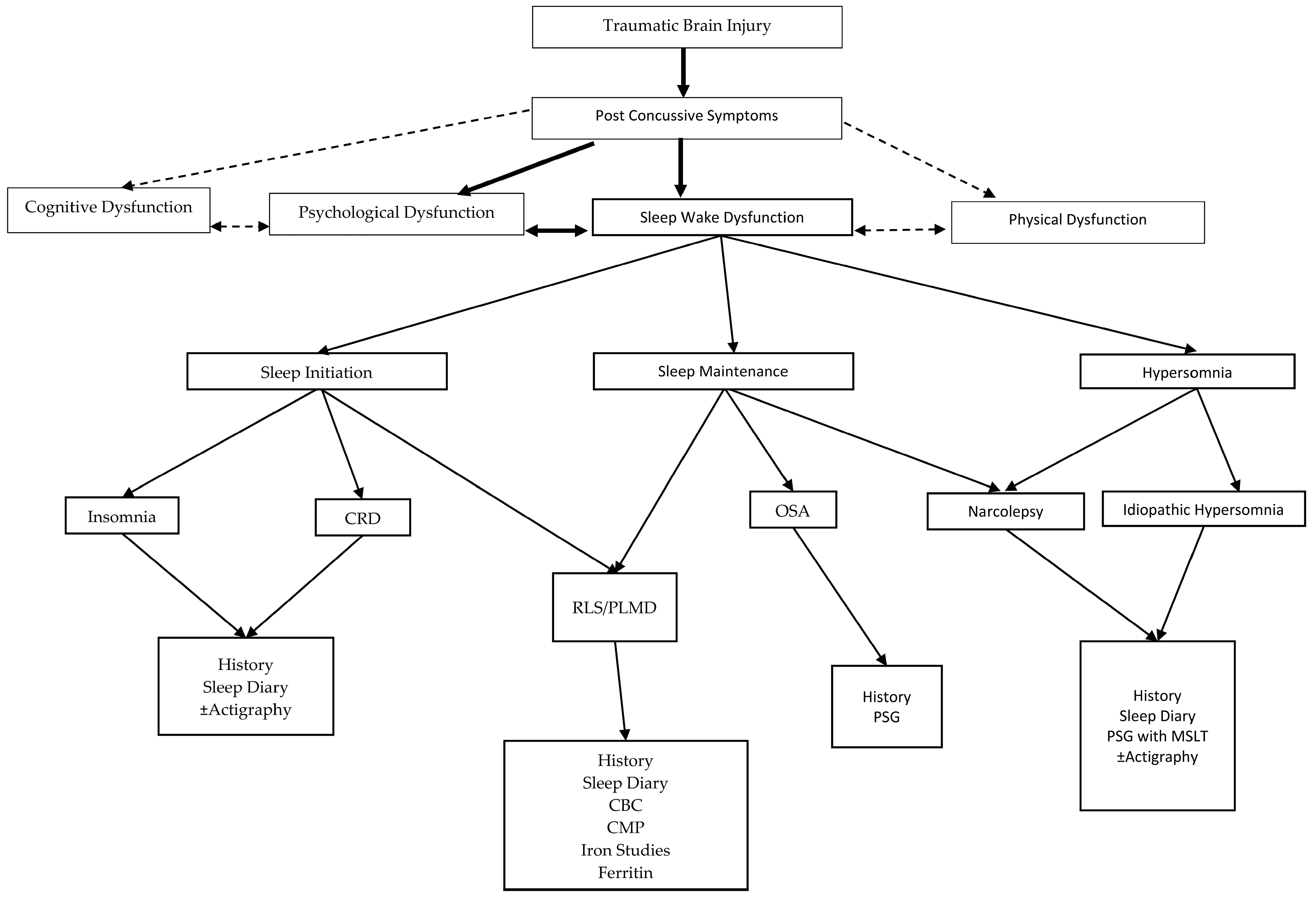
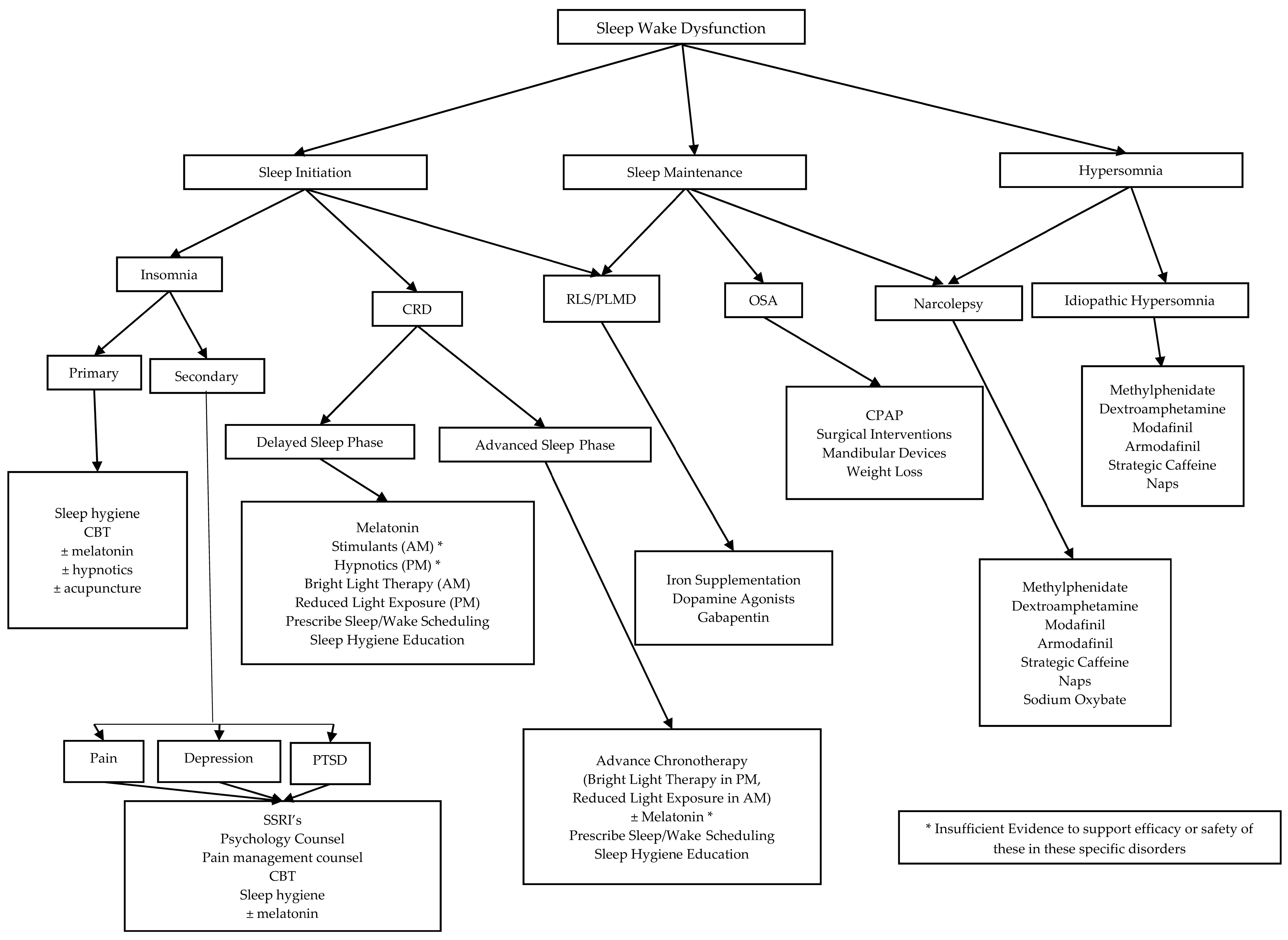
| Diagnoses | Signs and Symptoms | |
|---|---|---|
| Sleep–Wake | Insomnia | Difficulty falling/staying asleep, unrefreshing sleep, insufficient number of hours of sleep despite adequate opportunity |
| Sleep Apnea | Snoring, restlessness, apnea, enuresis, diaphoresis, open-mouth breathing, bruxism, sleep fragmentation | |
| Idiopathic Hypersomnia | Excessive daytime sleepiness, ± excessive number of hours asleep | |
| Narcolepsy | Excessive daytime sleepiness, cataplexy, sleep paralysis, sleep related hallucinations, sleep fragmentation | |
| PLMD/RLS * | PLMs >5/h on PSG; Restlessness, discomfort in arms or legs that interferes with sleep onset or maintenance, improves with movement | |
| CRD | Sleep difficulties that conflict with age typical circadian rhythm; When given opportunity sleeps appropriate number of hours for age | |
| Parasomnia | Sleep walking, sleep talking, confusional arousals, night terrors, REM behavior disorder/dream enactment behavior | |
| Psychiatric | Anxiety | Avoidance, phobias, obsessive compulsive symptoms, generalized anxious feelings |
| Depression | Fatigue, irritability, sadness, difficulty concentrating, difficulty with recall, suicidality | |
| ADHD | Impaired attention, hyperactivity, impaired working memory, impaired working speed | |
| PTSD | Headaches, decreased psychosocial recovery, sleep disturbance/nightmares, pain, flashbacks, amnesia, irritability/aggression, concentration difficulty |
| Risk Factors of Protracted Recovery |
|---|
| Pre-injury psychiatry history |
| Injury Severity |
| Family dysfunction |
| Sleep–Wake Dysfunction |
| Re-injury |
| Female gender |
| Referral to Rehabilitation Facility |
| Prescription for acute headache rescue therapy |
| Chronic headache treatment |
| Presenting SCAT2 * score <80 |
| Participation in a non-helmeted sport |
| Psychiatric Disorder | Treatment Options |
|---|---|
| Depression | |
| Mild | CBT ± Exercise |
| Severe | CBT + SSRI ± Exercise |
| Suicidality | CBT + SSRI ± Hospitalization ± Exercise |
| With psychotic features | CBT + Antidepressant + Antipsychotic ± Exercise |
| Refractory | CBT + Antidepressant + Antipsychotic ± Exercise ± ECT |
| Anxiety | First Line: CBT ± SSRI, SNRI |
| Second Line: CBT + SSRI, ± SNRI | |
| Third Line: CBT + SSRI + different SSRI or SNRI with Benzodiazepines used as a bridge | |
| until SSRI becomes effective. | |
| ADHD | Stimulants [111,112] (methylphenidate, amphetamine), ± CBT, non-stimulants (atomoxetine, guanfacine, clonidine) |
| PTSD | CBT, Ensure Safety, Treat Comorbidities, ± Antiadrenergic medications (clonidine, guanfacine, or prazosin *) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morse, A.M.; Garner, D.R. Traumatic Brain Injury, Sleep Disorders, and Psychiatric Disorders: An Underrecognized Relationship. Med. Sci. 2018, 6, 15. https://doi.org/10.3390/medsci6010015
Morse AM, Garner DR. Traumatic Brain Injury, Sleep Disorders, and Psychiatric Disorders: An Underrecognized Relationship. Medical Sciences. 2018; 6(1):15. https://doi.org/10.3390/medsci6010015
Chicago/Turabian StyleMorse, Anne M., and David R. Garner. 2018. "Traumatic Brain Injury, Sleep Disorders, and Psychiatric Disorders: An Underrecognized Relationship" Medical Sciences 6, no. 1: 15. https://doi.org/10.3390/medsci6010015