Premature Ejaculation: Aetiology and Treatment Strategies

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. International Society of Sexual Medicine Definition of PE and Classification
- Ejaculation which always or nearly always occurs prior to or within about one minute of vaginal penetration from the first sexual experience (lifelong), or, a clinically significant reduction in latency time, often to about 3 min or less (acquired).
- The inability to delay ejaculation on all or nearly all vaginal penetrations.
- Negative personal consequences, such as distress, bother, frustration and/or the avoidance of sexual intimacy [4].
3. Pathophysiology of Premature Ejaculation
3.1. Sexual Response Cycle
3.2. Process of Ejaculation
3.3. Peripheral Control
3.4. Spinal Control
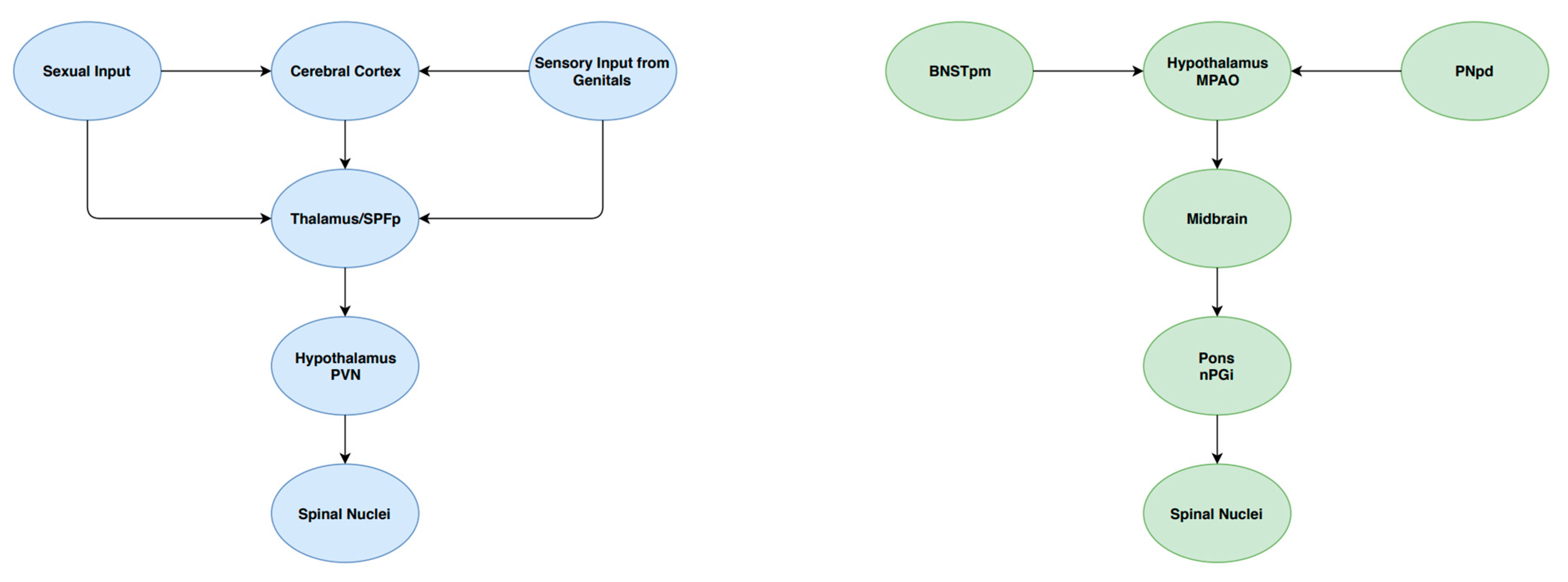
3.5. Cerebral Control
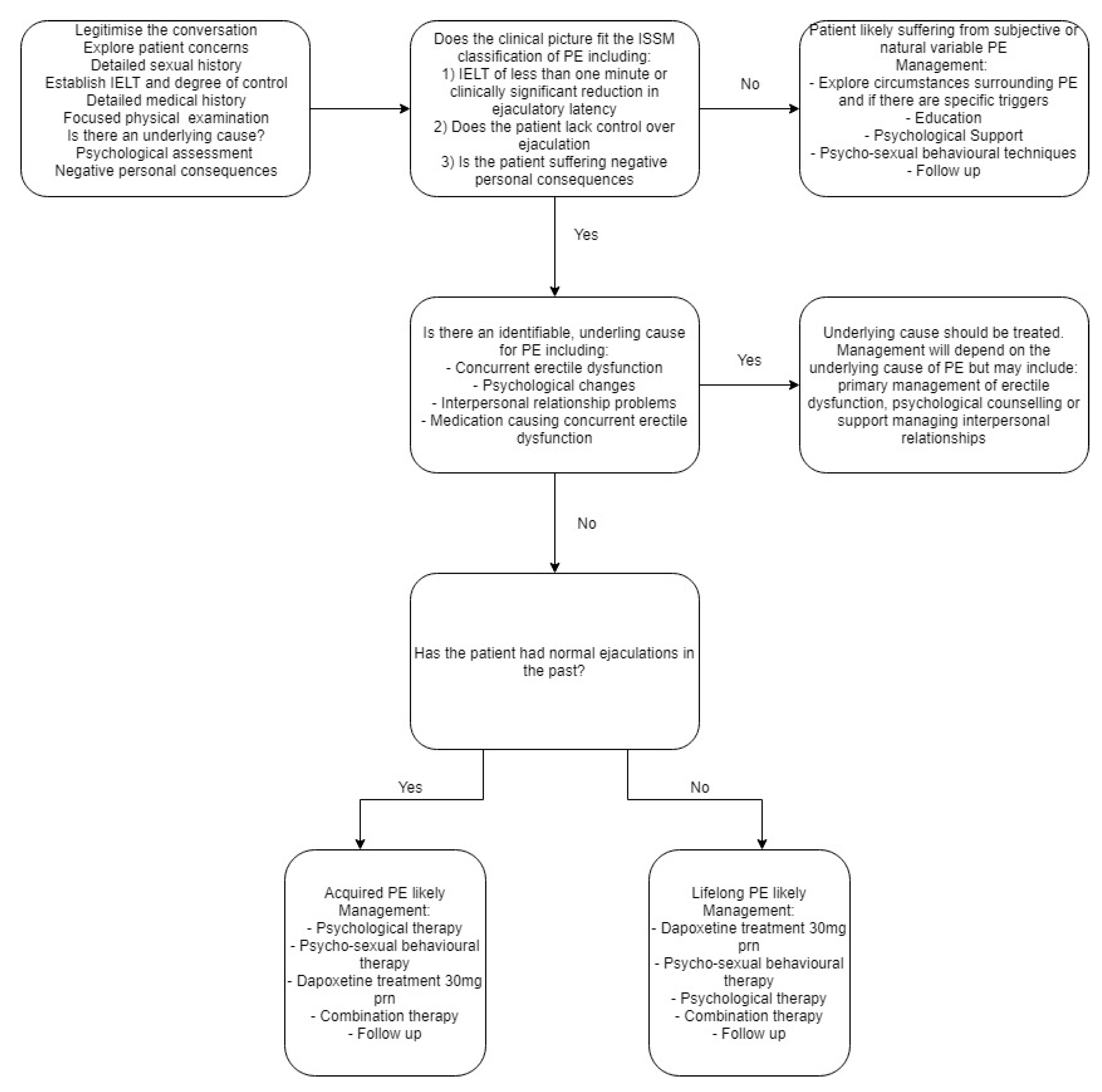
4. Patient Assessment
- Permission: This is the first stage in which the clinician gives the client permission to feel comfortable about and discuss a particular facet of their sexual health. It is imperative the clinician maintains a professional, non-judgmental attitude during this time in order to facilitate the conversation.
- Limited Information: In this stage, the patient is provided with limited information about a topic or issue. It is important in this stage that the clinician learns about specific topics the patient wishes to discuss surrounding their sexual health and provide information for the specific subject.
- Specific Suggestion: Here, the clinician provides patients with specific advice on particular topics relating to the patient’s sexual health. This is completed after full patient evaluation surrounding the topic. Information includes suggested behavioural changes as well as treatment options for a specific concern.
- Intensive Therapy: This is the last stage in which the patient begins psychological and/or pharmacological therapy to remediate a specific issue the patient is suffering from regarding their sexual health. This may include referral to a specialist for further treatment and management.
5. Patient Management Options and Scientific Rationale
5.1. Role of Serotonin (5-HT) in Ejaculatory Control
5.2. Selective Serotonin Reuptake Inhibitors
5.3. Other Proposed Pharmacological Management Options
5.4. Psychological and Psychosexual Behavioural Therapy
6. Patient Management
Combined Therapy for the Treatment of Premature Ejaculation
7. Conclusions
Funding
Conflicts of Interest
References
- Porst, H.; Montorsi, F.; Rosen, R.C.; Gaynor, L.; Grupe, S.; Alexander, J. The Premature Ejaculation Prevalence and Attitudes (PEPA) Survey: Prevalence, Comorbidities, and Professional Help-Seeking. Eur. Urol. 2007, 51, 816–824. [Google Scholar] [PubMed]
- Laumann, E.O.; Nicolosi, A.; Glasser, D.B.; Paik, A.; Gingell, C.; Moreira, E.; Wang, T. Sexual problems among women and men aged 40–80 y: Prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int. J. Impot. Res. 2005, 17, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Saitz, T.R.; Serefoglu, E.C. The epidemiology of premature ejaculation. Transl. Androl. Urol. 2016, 5, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serefoglu, E.C.; McMahon, C.G.; Waldinger, M.D.; Althof, S.E.; Shindel, A.; Adaikan, G.; Becher, E.F.; Dean, J.; Giuliano, F.; Hellstrom, W.J.G.; et al. An Evidence-Based Unified Definition of Lifelong and Acquired Premature Ejaculation: Report of the Second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2014, 11, 1423–1441. [Google Scholar] [CrossRef] [PubMed]
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Waldinger, M.D. The pathophysiology of lifelong premature ejaculation. Transl. Androl. Urol. 2016, 5, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMahon, C.G.; Althof, S.E.; Waldinger, M.D.; Porst, H.; Dean, J.; Sharlip, I.D.; Adaikan, P.G.; Becher, E.; Broderick, G.A.; Buvat, J.; et al. An Evidence-Based Definition of Lifelong Premature Ejaculation: Report of the International Society for Sexual Medicine (ISSM) Ad Hoc Committee for the Definition of Premature Ejaculation. J. Sex. Med. 2008, 5, 1590–1606. [Google Scholar] [CrossRef]
- Waldinger, M.D.; Schweitzer, D.H. Changing Paradigms from a Historical DSM-III and DSM-IV View Toward an Evidence-Based Definition of Premature Ejaculation. Part II-Proposals for DSMV and ICD-11. J. Sex. Med. 2006, 3, 693–705. [Google Scholar] [CrossRef]
- Waldinger, M.D.; Schweitzer, D.H. The Use of Old and Recent DSM Definitions of Premature Ejaculation in Observational Studies: A Contribution to the Present Debate for a New Classification of PE in the DSM-V. J. Sex. Med. 2005, 5, 1079–1087. [Google Scholar] [CrossRef]
- Althof, S.E.; Abdo, C.H.N.; Dean, J.; Hackett, G.; McCabe, M.; McMahon, C.G.; Rosen, R.C.; Sadovsky, R.; Waldinger, E.; Becher, E.; et al. International Society for Sexual Medicine’s Guidelines for the Diagnosis and Treatment of Premature Ejaculation. J. Sex. Med. 2010, 7, 2947–2969. [Google Scholar] [CrossRef]
- Janssen, P.K.; van Schaik, R.; Zwinderman, A.H.; Olivier, B.; Waldinger, M.D. The 5-HT1A receptor C (1019) G polymorphism influences the intravaginal ejaculation latency time in Dutch Caucasian men with lifelong premature ejaculation. Pharmacol. Biochem. Behav. 2014, 121, 184–188. [Google Scholar] [CrossRef]
- Janssen, P.K.; Schaik, R.V.; Olivier, B.; Waldinger, M.D. The 5-HT2C receptor gene Cys23Ser polymorphism influences the intravaginal ejaculation latency time in Dutch Caucasian men with lifelong premature ejaculation. Asian J. Androl. 2014, 16, 607–610. [Google Scholar] [PubMed]
- McMahon, C.G.; Jannini, E.A.; Serefoglu, E.C.; Hellstrom, W.J.G. The pathophysiology of acquired premature ejaculation. Transl. Androl. Urol. 2016, 5, 434–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgiadis, J.R.; Kringelbach, M.L. The human sexual response cycle: Brain imaging evidence linking sex to other pleasures. Prog. Neurobiol. 2012, 98, 49–81. [Google Scholar] [CrossRef] [PubMed]
- Buvat, J. Pathophysiology of Premature Ejaculation. J. Sex. Med. 2011, 8, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Clement, P.; Giuliano, F. Physiology and Pharmacology of Ejaculation. Basic Clin. Pharmacol. Toxicol. 2016, 119, 18–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerstenberg, T.C.; Levin, R.J.; Wagner, G. Erection and ejaculation in man. Assessment of the electromyographic activity of the bulbocavernosus and ischiocavernosus muscles. Br. J. Urol. 1990, 65, 395–402. [Google Scholar] [CrossRef]
- Alwaal, A.; Breyer, B.N.; Lue, T.F. Normal male sexual function: Emphasis on orgasm and ejaculation. Fertil. Steril. 2015, 104, 1051–1060. [Google Scholar] [CrossRef]
- Chéhensse, C.; Bahrami, S.; Denys, P.; Clément, P.; Bernabé, J.; Giuliano, F. The spinal control of ejaculation revisited: A systematic review and meta-analysis of anejaculation in spinal cord injured patients. Hum. Reprod. Update 2013, 19, 507–526. [Google Scholar] [CrossRef]
- Hsieh, J.T.; Kuo, Y.C.; Chang, H.C.; Liu, S.P.; Chen, J.H.; Tsai, V.F.S. The role of sympathetic and parasympathetic nerve systems on the smooth muscle of rat seminal vesicles—Experimental results and speculation for physiological implication on ejaculation. Andrology 2014, 2, 59–64. [Google Scholar] [CrossRef]
- Xu, C.; Giuliano, F.; Yaici, E.D.; Conrath, M.; Trassard, O.; Benoit, G.; Verge, D. Identification of lumbar spinal neurons controlling simultaneously the prostate and the bulbospongiosus muscles in the rat. Neuroscience 2006, 138, 561–573. [Google Scholar] [CrossRef]
- Borgdorff, A.J.; Bernabé, J.; Denys, P.; Alexandre, L.; Giuliano, F. Ejaculation Elicited by Microstimulation of Lumbar Spinothalamic Neurons. Eur. Urol. 2008, 54, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Truitt, W.A.; Coolen, L.M. Identification of a Potential Ejaculation Generator in the Spinal Cord. Science 2002, 297, 1566. [Google Scholar] [CrossRef] [PubMed]
- Chéhensse, C.; Facchinetti, P.; Bahrami, S.; Andrey, P.; Soler, J.M.; Chrétien, F.; Bernabé, J.; Clément, P.; Denys, P.; Giuliano, F. Human spinal ejaculation generator. Ann. Neurol. 2017, 81, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Veening, J.G.; Coolen, L.M. Neural mechanisms of sexual behavior in the male rat: Emphasis on ejaculation-related circuits. Pharmacol. Biochem. Behav. 2014, 121, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Annon, J.S. The PLISSIT Model: A Proposed Conceptual Scheme for the Behavioral Treatment of Sexual Problems. J. Sex Educ. Ther. 1976, 2, 1–15. [Google Scholar] [CrossRef]
- Symonds, T.; Perelman, M.A.; Althof, S.; Giuliano, F.; Martin, M.; May, K.; Abraham, L.; Crossland, A.; Morris, M. Development and Validation of a Premature Ejaculation Diagnostic Tool. Eur. Urol. 2007, 52, 565–573. [Google Scholar] [CrossRef]
- Waldinger, M.D.; Quinn, P.; Dilleen, M.; Mundayat, R.; Schweitzer, D.H.; Boolell, M. Original Research-2014; Ejaculation Disorders: A Multinational Population Survey of Intravaginal Ejaculation Latency Time. J. Sex. Med. 2005, 2, 492–497. [Google Scholar] [CrossRef]
- Hull, E.M.; Muschamp, J.W.; Sato, S. Dopamine and serotonin: Influences on male sexual behavior. Physiol. Behav. 2004, 83, 291–307. [Google Scholar] [CrossRef]
- Motofei, I.G.; Rowland, D.L. Neurophysiology of the ejaculatory process: Developing perspectives. BJU Int. 2005, 96, 1333–1338. [Google Scholar] [CrossRef]
- Hillegaart, V.; Ahlenius, S. Facilitation and inhibition of male rat ejaculatory behaviour by the respective 5-HT1A and 5-HT1B receptor agonists 8-OH-DPAT and anpirtoline, as evidenced by use of the corresponding new and selective receptor antagonists NAD-299 and NAS-181. Br. J. Pharmacol. 1998, 125, 1733–1743. [Google Scholar] [CrossRef]
- Foreman, M.M.; Hall, J.L.; Love, R.L. The role of the 5-HT2 receptor in the regulation of sexual performance of male rats. Life Sci. 1989, 45, 1263–1270. [Google Scholar] [CrossRef]
- Ahlenius, S.; Larsson, K. Evidence for an involvement of 5-HT1B receptors in the inhibition of male rat ejaculatory behavior produced by 5-HTP. Psychopharmacology 1998, 137, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, F.; Clément, P. Serotonin and Premature Ejaculation: From Physiology to Patient Management. Eur. Urol. 2006, 50, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Mathes, C.W.; Smith, E.R.; Popa, B.R.; Davidson, J.M. Effects of intrathecal and systemic administration of buspirone on genital reflexes and mating behavior in male rats. Pharmacol. Biochem. Behav. 1990, 36, 63–68. [Google Scholar] [CrossRef]
- Higgins, A.; Nash, M.; Lynch, A.M. Antidepressant-associated sexual dysfunction: Impact, effects, and treatment. Drug Healthc. Patient Saf. 2010, 2, 141–150. [Google Scholar] [CrossRef]
- Buvat, J.; Tesfaye, F.; Rothman, M.; Rivas, D.A.; Giuliano, F. Dapoxetine for the Treatment of Premature Ejaculation: Results from a Randomized, Double-Blind, Placebo-Controlled Phase 3 Trial in 22 Countries. Eur. Urol. 2009, 55, 957–968. [Google Scholar] [CrossRef]
- Hellstrom, W.; Gittelman, M.; Althof, S.; Ho, K.; Kell, S. Dapoxetine HCl for the treatment of premature ejaculation: A Phase II, randomised, double-blind, placebo controlled study. J. Sex. Med. 2004, 1 (Suppl. 1), 59. [Google Scholar]
- Kaufman, J.M.; Rosen, R.C.; Mudumbi, R.V.; Tesfaye, F.; Hashmonay, R.; Rivas, D. Treatment benefit of dapoxetine for premature ejaculation: Results from a placebo-controlled phase III trial. BJU Int. 2009, 103, 651–658. [Google Scholar] [CrossRef]
- McMahon, C.; Kim, S.W.; Park, N.C.; Chang, C.P.; Rivas, D.; Tesfaye, F.; Rothman, M.; Aquilina, J. Treatment of Premature Ejaculation in the Asia-Pacific Region: Results from a Phase III Double-blind, Parallel-group Study of Dapoxetine. J. Sex. Med. 2010, 7, 256–268. [Google Scholar] [CrossRef]
- Pryor, J.L.; Althof, S.E.; Steidle, C.; Rosen, R.C.; Hellstrom, W.J.; Shabsigh, R.; Miloslavsky, M.; Kell, S.; Dapoxetine Study Group. Efficacy and tolerability of dapoxetine in treatment of premature ejaculation: An integrated analysis of two double-blind, randomised controlled trials. Lancet 2006, 368, 929–937. [Google Scholar] [CrossRef]
- Li, J.; Liu, D.; Wu, J.; Fan, X.; Dong, Q. Dapoxetine for the treatment of premature ejaculation: A meta-analysis of randomized controlled trials with trial sequential analysis. Ann. Saudi Med. 2018, 38, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Abu El-Hamd, M.; Abdelhamed, A. Comparison of the clinical efficacy and safety of the on-demand use of paroxetine, dapoxetine, sildenafil and combined dapoxetine with sildenafil in treatment of patients with premature ejaculation: A randomised placebo-controlled clinical trial. Andrologia 2018, 50, e12829. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Capogrosso, P.; Ventimiglia, E.; La Croce, G.; Boeri, L.; Montorsi, F.; Salonia, A. Efficacy and safety of dapoxetine in treatment of premature ejaculation: An evidence-based review. Int. J. Clin. Pract. 2016, 70, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Gengo, P.J.; Giuliano, F.; McKenna, K.E.; Chester, A.; Lovenberg, T.; Bonaventure, P.; Gupta, S.K. 878: Monoaminergic Transporter Binding and Inhibition Profile of Dapoxetine, A Medication for The Treatment of Premature Ejaculation. J. Urol. 2005, 173, 239. [Google Scholar]
- Hellstrom, W.J.G. Emerging treatments for premature ejaculation: Focus on dapoxetine. Neuropsychiatr. Dis. Treat. 2009, 5, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Haensel, S.M.; Rowland, D.L.; Kallan, K.T.; Slob, K.A. Clomipramine and Sexual Function in Men with Premature Ejaculation and Controls. J. Urol. 1996, 156, 1310–1315. [Google Scholar] [CrossRef]
- Khan, A.H.; Rasaily, D. Tramadol use in premature ejaculation: Daily versus sporadic treatment. Indian J. Psychol. Med. 2013, 35, 256–259. [Google Scholar] [CrossRef]
- McMahon, C.G.; McMahon, C.N.; Leow, L.J.; Winestock, C.G. Efficacy of type-5 phosphodiesterase inhibitors in the drug treatment of premature ejaculation: A systematic review. BJU Int. 2006, 98, 259–272. [Google Scholar] [CrossRef]
- Waldinger, M.D. Recent advances in the classification, neurobiology and treatment of premature ejaculation. Adv. Psychosom. Med. 2008, 29, 50–69. [Google Scholar]
- Melnik, T.; Althof, S.; Atallah, Á.; Puga, M.; Glina, S.; Riera, R. Psychosocial interventions for premature ejaculation. Cochrane Database Syst. Rev. 2011, 8, CD008195. [Google Scholar] [CrossRef]
- Semans, J.H. Premature ejaculation: A new approach. South Med. J. 1956, 49, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Masters, W.H.; Johnson, V.E. Human Sexual Inadequacy; Little, Brown: Boston, MA, USA, 1970. [Google Scholar]
- Hawton, K.; Catalan, J.; Martin, P.; Fagg, J. Long-term outcome of sex therapy. Behav. Res. Ther. 1986, 24, 665–675. [Google Scholar] [CrossRef]
- Jannini, E.A.; Simonelli, C.; Lenzi, A. Sexological approach to ejaculatory dysfunction. Int. J. Androl. 2002, 25, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Palmer, N.R.; Stuckey, B.G. Premature ejaculation: A clinical update. Med. J. Aust. 2008, 188, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Cormio, L.; Massenio, P.; La Rocca, R.; Verze, P.; Mirone, V.; Carrieri, G. The Combination of Dapoxetine and Behavioral Treatment Provides Better Results than Dapoxetine Alone in the Management of Patients with Lifelong Premature Ejaculation. J. Sex. Med. 2015, 12, 1609–1615. [Google Scholar] [CrossRef] [PubMed]



© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gillman, N.; Gillman, M. Premature Ejaculation: Aetiology and Treatment Strategies. Med. Sci. 2019, 7, 102. https://doi.org/10.3390/medsci7110102
Gillman N, Gillman M. Premature Ejaculation: Aetiology and Treatment Strategies. Medical Sciences. 2019; 7(11):102. https://doi.org/10.3390/medsci7110102
Chicago/Turabian StyleGillman, Nicholas, and Michael Gillman. 2019. "Premature Ejaculation: Aetiology and Treatment Strategies" Medical Sciences 7, no. 11: 102. https://doi.org/10.3390/medsci7110102