Epidemiology of Bladder Cancer

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Epidemiology
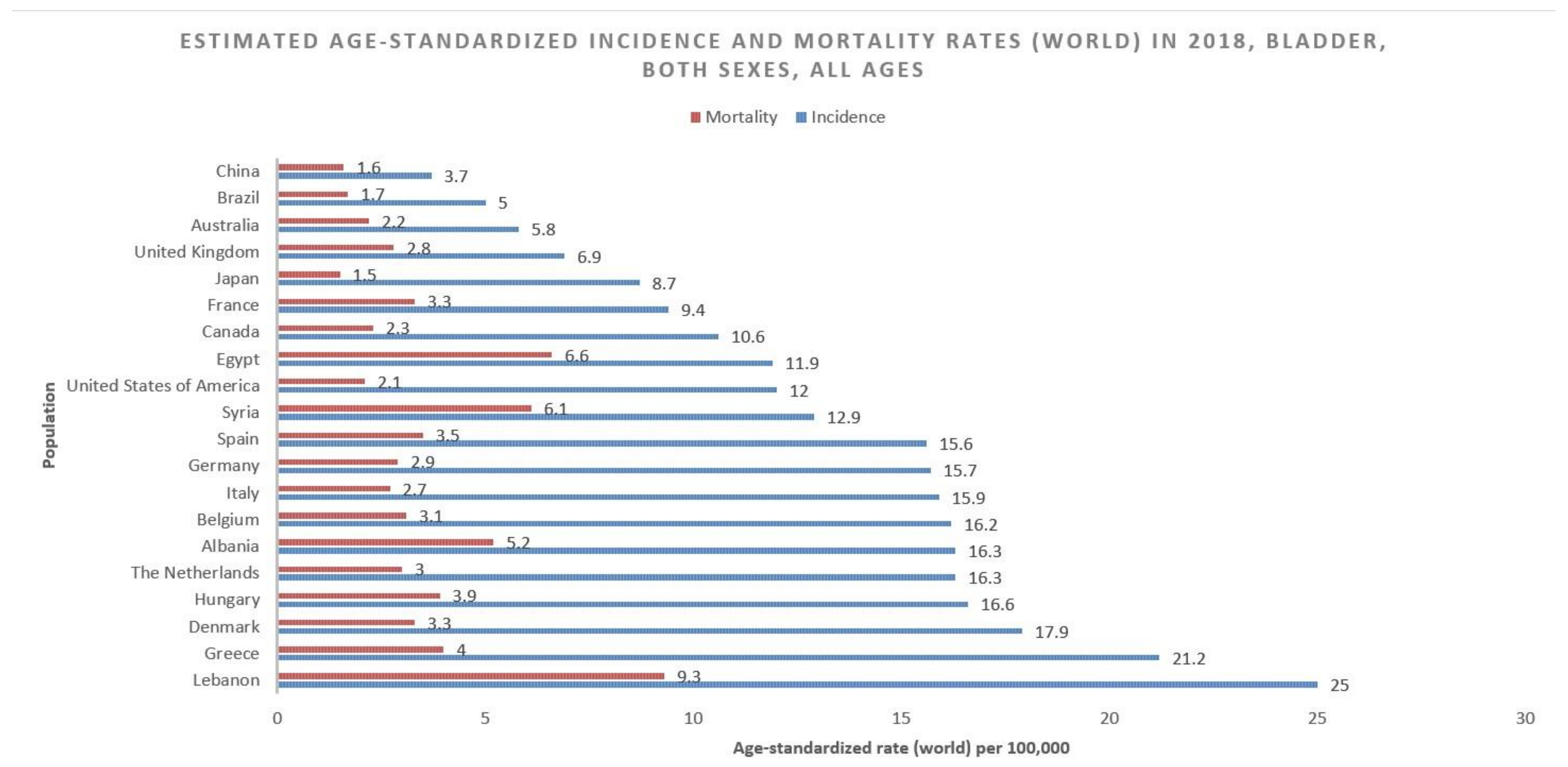
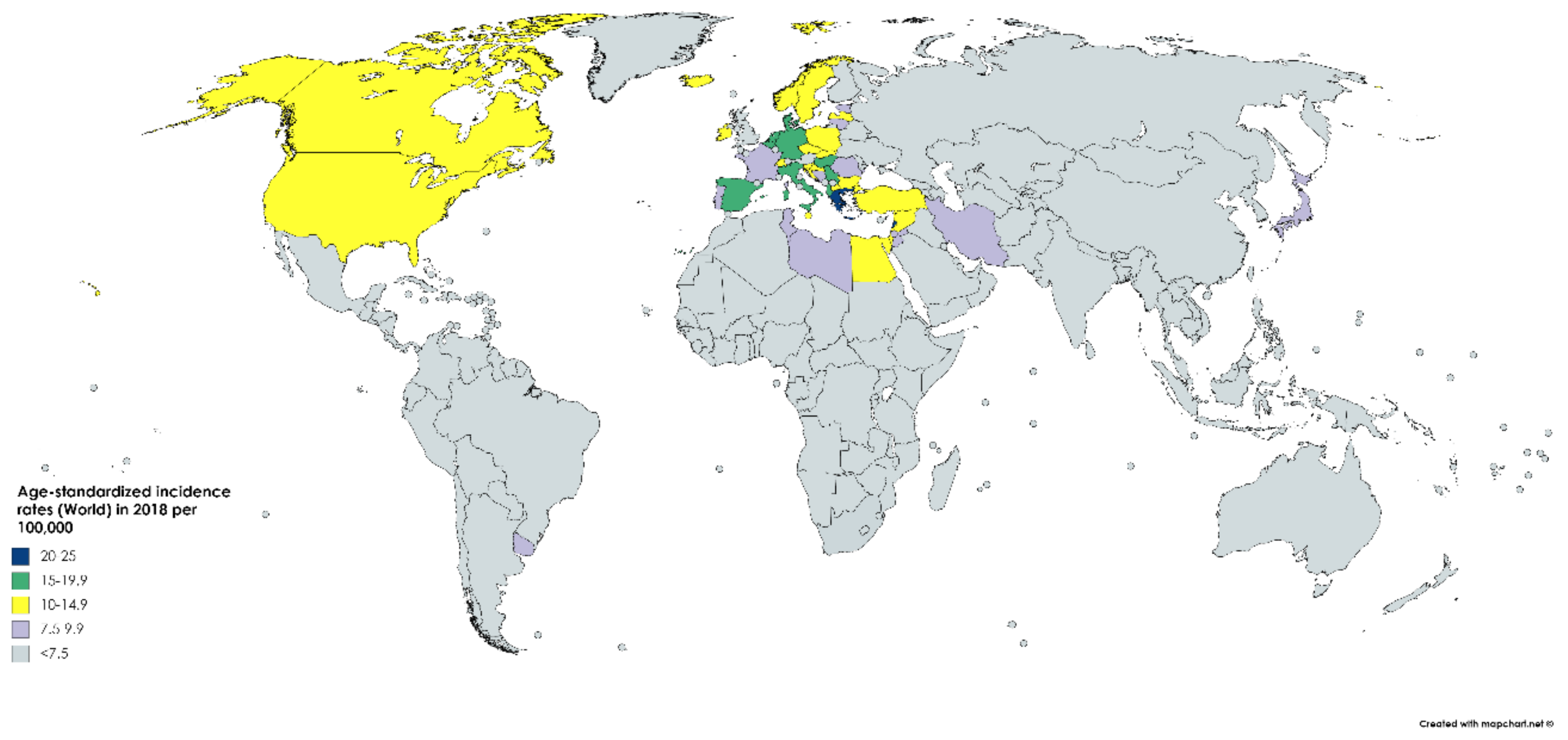
2.1. Incidence
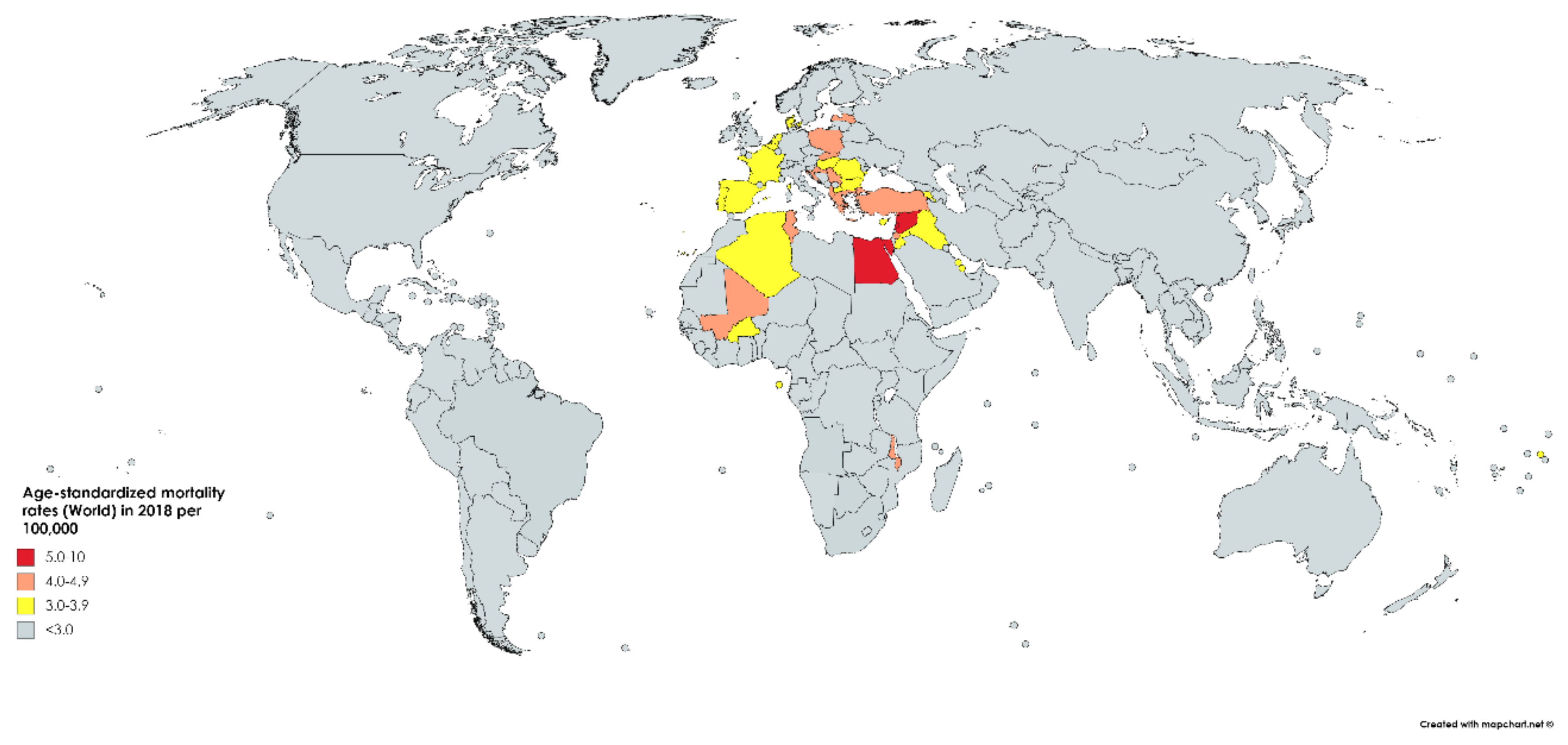
2.2. Mortality
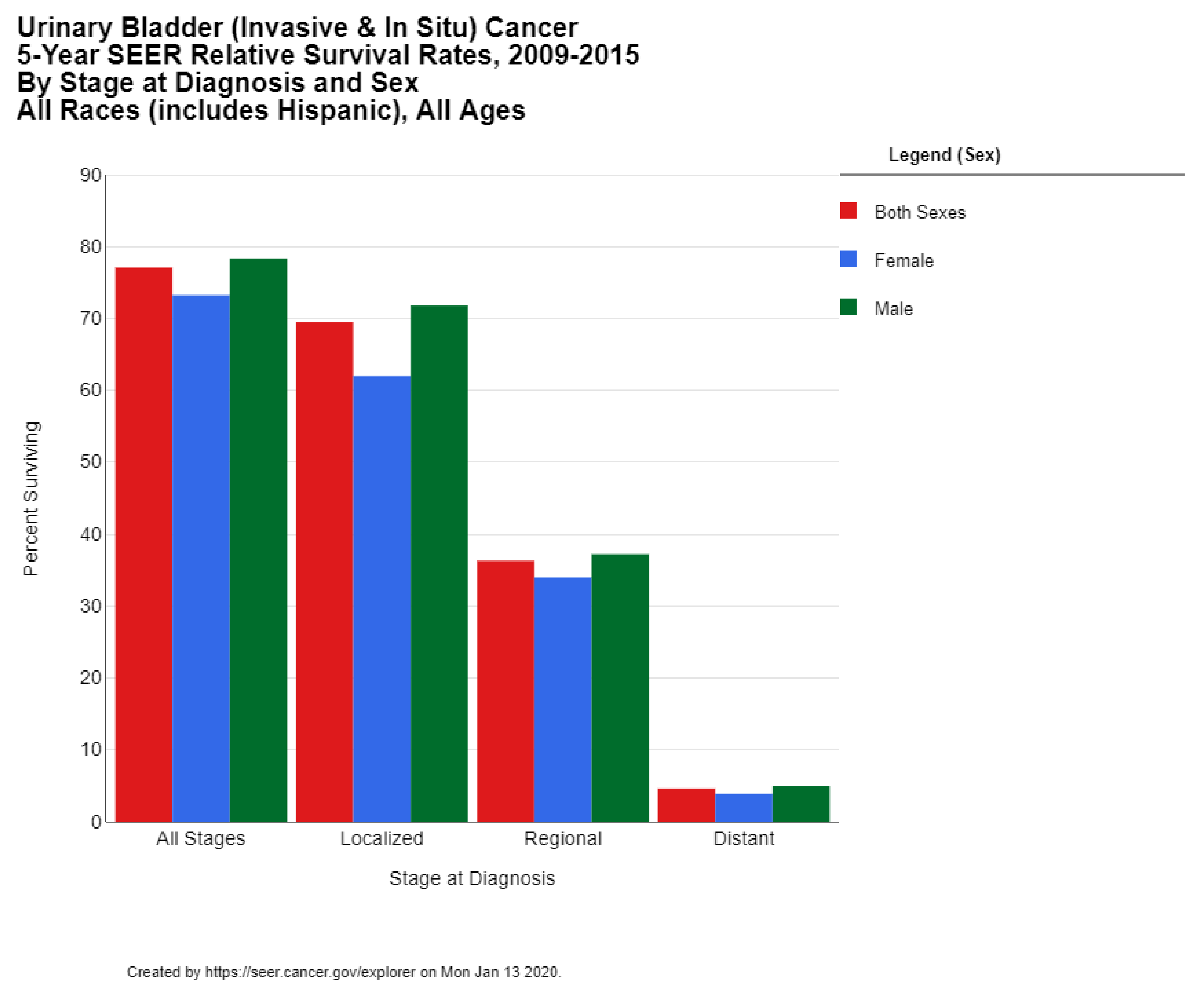
2.3. Survival
3. Etiology
4. Risk Factors
4.1. Gender
4.2. Age
4.3. Hereditary and Genetic Factors
4.4. Smoking
4.5. Environmental and Occupational Exposure
4.6. Alcohol
4.7. Red Meat
4.8. Obesity
4.9. Pathogens
5. Prevention
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2018; Available online: https://gco.iarc.fr/ (accessed on 10 January 2020).
- Andersson, K.-E.; Arner, A. Urinary Bladder Contraction and Relaxation: Physiology and Pathophysiology. Physiol. Rev. 2004, 84, 935–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushtaq, J.; Thurairaja, R.; Nair, R. Bladder Cancer. Surgery 2019, 37, 529–537. [Google Scholar] [CrossRef]
- Mostafa, M.H.; Sheweita, S.; O’Connor, P.J. Relationship between Schistosomiasis and Bladder Cancer. Clin. Microbiol. Rev. 1999, 12, 97–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.; Fung, F.D.H.; Leung, C.; Cheung, W.W.L.; Goggins, W.B.; Ng, A.C.F. The global epidemiology of bladder cancer: a joinpoint regression analysis of its incidence and mortality trends and projection. Sci. Rep. 2018, 8, 1129. [Google Scholar] [CrossRef] [PubMed]
- Jamal, A.; Phillips, E.; Gentzke, A.S.; Homa, D.M.; Babb, S.D.; King, B.A.; Neff, L.J. Current cigarette smoking among adults—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association Between Smoking and Risk of Bladder Cancer Among Men and Women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef]
- Al-Zalabani, A.; Stewart, K.; Wesselius, A.; Schols, A.M.W.J.; Zeegers, M. Modifiable risk factors for the prevention of bladder cancer: A systematic review of meta-analyses. Eur. J. Epidemiol. 2016, 31, 811–851. [Google Scholar] [CrossRef] [Green Version]
- SEER. SEER Cancer Statistics Review 1975–2015; Noone, A.M., Howlader, N., Krapcho, M., Miller, D., Brest, A., Yu, M., Ruhl, J., Tatalovich, Z., Mariotto, A., Lewis, D.R., et al., Eds.; National Cancer Institute: Bethesda, MD, USA, 2018. [Google Scholar]
- Silverman, D.T.; Koutros, S.; Figueroa, J.D.; Prokunina-Olsson, L.; Rothman, N. Bladder cancer. In Cancer Epidemiology and Prevention; Thun, M.J., Linet, M.S., Cerhan, J.R., Haiman, C.A., Schottenfeld, D.E., Eds.; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- SEER*Explorer. Available online: https://seer.cancer.gov/explorer/ (accessed on 13 January 2020).
- Zaghloul, M.S. Bladder cancer and schistosomiasis. J. Egypt. Natl. Cancer Inst. 2012, 24, 151–159. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO global report: Mortality attributable to tobacco. Available online: https://www.who.int/tobacco/publications/surveillance/rep_mortality_attributable/en/ (accessed on 5 January 2020).
- Hinotsu, S.; Akaza, H.; Miki, T.; Fujimoto, H.; Shinohara, N.; Kikuchi, E.; Mizutani, Y.; Koga, H.; Okajima, E.; Okuyama, A.; et al. Bladder cancer develops 6 years earlier in current smokers: Analysis of bladder cancer registry data collected by the cancer registration committee of the Japanese Urological Association. Int. J. Urol. 2008, 16, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Linn, J.F.; Sesterhenn, I.; Mostofi, F.K.; Schoenberg, M. THE MOLECULAR CHARACTERISTICS OF BLADDER CANCER IN YOUNG PATIENTS. J. Urol. 1998, 159, 1493–1496. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Wu, X. Genetic susceptibility to bladder cancer risk and outcome. Pers. Med. 2011, 8, 365–374. [Google Scholar] [CrossRef] [Green Version]
- Kiemeney, L.A.; Thorlacius, S.; Sulem, P.; Geller, F.; Aben, K.K.; Stacey, S.N.; Gudmundsson, J.; Jakobsdottir, M.; Bergthorsson, J.T.; Sigurdsson, A.; et al. Sequence variant on 8q24 confers susceptibility to urinary bladder cancer. Nat. Genet. 2008, 40, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Hildebrandt, M.A.T.; Chang, D.W. Genome-wide association studies of bladder cancer risk: a field synopsis of progress and potential applications. Cancer Metastasis Rev. 2009, 28, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Hein, D.W. Molecular genetics and function of NAT1 and NAT2: role in aromatic amine metabolism and carcinogenesis. Mutat. Res. Mol. Mech. Mutagen. 2002, 506, 65–77. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Closas, M.; Malats, N.; Silverman, D.; Dosemeci, M.; Kogevinas, M.; Hein, D.W.; Tardon, A.; Serra, C.; Carrato, A.; García-Closas, R.; et al. NAT2 slow acetylation and GSTM1 null genotypes increase bladder cancer risk: results from the Spanish Bladder Cancer Study and meta-analyses. Lancet 2005, 366, 649–659. [Google Scholar] [CrossRef] [Green Version]
- Gu, J.; Liang, N.; Wang, Y.; Lu, C.; Wu, X. Effects of N-acetyl transferase 1 and 2 polymorphisms on bladder cancer risk in Caucasians. Mutat. Res. Toxicol. Environ. Mutagen. 2005, 581, 97–104. [Google Scholar] [CrossRef]
- Rothman, N.; Garcia-Closas, M.; Chatterjee, N.; Malats, N.; Wu, X.; Figueroa, J.D.; Real, F.X.; Berg, D.V.D.; Matullo, G.; Baris, D.; et al. A multi-stage genome-wide association study of bladder cancer identifies multiple susceptibility loci. Nat. Genet. 2010, 42, 978–984. [Google Scholar] [CrossRef] [Green Version]
- Riegert-Johnson, D.; Gleeson, F.; E Roberts, M.; Tholen, K.; Youngborg, L.; Bullock, M.; Boardman, L.A. Cancer and Lhermitte-Duclos disease are common in Cowden syndrome patients. Hered. Cancer Clin. Pr. 2010, 8, 6. [Google Scholar] [CrossRef] [Green Version]
- Van Der Post, R.S.; Kiemeney, L.A.; Ligtenberg, M.J.L.; Witjes, J.A.; De Kaa, C.A.H.-V.; Bodmer, D.; Schaap, L.; Kets, C.M.; Van Krieken, J.H.J.M.; Hoogerbrugge, N. Risk of urothelial bladder cancer in Lynch syndrome is increased, in particular among MSH2 mutation carriers. J. Med Genet. 2010, 47, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Phelan, A.; Lopez-Beltran, A.; Montironi, R.; Zhang, S.; Raspollini, M.R.; Cheng, M.; Kaimakliotis, H.Z.; O Koch, M.; Cheng, L. Inherited forms of bladder cancer: a review of Lynch syndrome and other inherited conditions. Future Oncol. 2018, 14, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Casadei, C.; Dizman, N.; Schepisi, G.; Cursano, M.C.; Basso, U.; Santini, D.; Pal, S.K.; De Giorgi, U. Targeted therapies for advanced bladder cancer: new strategies with FGFR inhibitors. Ther. Adv. Med Oncol. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Esrig, D.; Elmajian, D.; Groshen, S.; Freeman, J.A.; Stein, J.P.; Chen, S.-C.; Nichols, P.W.; Skinner, D.G.; Jones, P.A.; Cote, R.J. Accumulation of Nuclear p53 and Tumor Progression in Bladder Cancer. N. Engl. J. Med. 1994, 331, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Malats, N.; Bustos-Moreno, A.; Murta-Nascimento, C.; Fernandez, F.; Rivas, M.; Puente, D.; Kogevinas, M.; Real, F.X. P53 as a prognostic marker for bladder cancer: a meta-analysis and review. Lancet Oncol. 2005, 6, 678–686. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (US); National Center for Chronic Disease Prevention and Health Promotion (US); Office on Smoking and Health (US). How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General; Center for Disease Control, and Prevention: Atlanta, GE, USA, 2010; ISBN 13: 978-0-16-084078-4. [Google Scholar]
- Burger, M.; Catto, J.W.; Dalbagni, G.; Grossman, H.B.; Herr, H.; Karakiewicz, P.; Kassouf, W.; Kiemeney, L.A.; La Vecchia, C.; Shariat, S.; et al. Epidemiology and Risk Factors of Urothelial Bladder Cancer. Eur. Urol. 2013, 63, 234–241. [Google Scholar] [CrossRef]
- Zeegers, M.P.; Kellen, E.; Buntinx, F.; van den Brandt, P.A. The association between smoking, beverage consumption, diet and bladder cancer: A systematic literature review. World J. Urol. 2004, 21, 392–401. [Google Scholar] [CrossRef]
- Yan, H.; Ying, Y.; Xie, H.; Li, J.; Wang, X.; He, L.; Jin, K.; Tang, J.; Xu, X.; Zheng, X. Secondhand smoking increases bladder cancer risk in nonsmoking population: A meta-analysis. Cancer Manag. Res. 2018. [Google Scholar] [CrossRef] [Green Version]
- Zeegers, M.; Swaen, G.M.H.; Kant, I.; Goldbohm, R.; Brandt, P.A.V.D. Occupational risk factors for male bladder cancer: results from a population-based case cohort study in the Netherlands. Occup. Environ. Med. 2001, 58, 590–596. [Google Scholar] [CrossRef] [Green Version]
- Golka, K.; Wiese, A.; Assennato, G.; Bolt, H.M. Occupational exposure and urological cancer. World J. Urol. 2004, 21, 382–391. [Google Scholar] [CrossRef]
- Chen, H.I.; Liou, S.H.; Loh, C.H.; Uang, S.N.; Yu, Y.C.; Shih, T.S. Bladder cancer screening and monitoring of 4,4′-methylenebis(2-chloroaniline) exposure among workers in Taiwan. Urology 2005, 66, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Marshall, G.; Ferreccio, C.; Yuan, Y.; Bates, M.N.; Steinmaus, C.; Selvin, S.; Liaw, J.; Smith, A.H. Fifty-Year Study of Lung and Bladder Cancer Mortality in Chile Related to Arsenic in Drinking Water. J. Natl. Cancer Inst. 2007, 99, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurttio, P.; Pukkala, E.; Kahelin, H.; Auvinen, A.; Pekkanen, J. Arsenic concentrations in well water and risk of bladder and kidney cancer in Finland. Environ. Health Perspect. 1999, 107, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Meliker, J.R.; Nriagu, J.O. Arsenic in drinking water and bladder cancer: Review of epidemiological evidence. Trace Met. other Contam. Environ. 2007, 9, 551–584. [Google Scholar]
- Zeegers, M.; Volovics, A.; Dorant, E.; Goldbohm, R.A.; Brandt, P.A.V.D. Alcohol Consumption and Bladder Cancer Risk: Results from the Netherlands Cohort Study. Am. J. Epidemiol. 2001, 153, 38–41. [Google Scholar] [CrossRef]
- Bagnardi, V.; Blangiardo, M.; La Vecchia, C.; Corrao, G. A meta-analysis of alcohol drinking and cancer risk. Br. J. Cancer 2001, 85, 1700–1705. [Google Scholar] [CrossRef]
- Wang, C.; Jiang, H. Meat intake and risk of bladder cancer: A meta-analysis. Med. Oncol. 2011, 29, 848–855. [Google Scholar] [CrossRef]
- Fei, L.; Wan-Long, T. Red and Processed Meat Intake and Risk of Bladder Cancer: A Meta-Analysis. Ann. Oncol. 2014, 25, iv489. [Google Scholar] [CrossRef]
- Bertram, J.; Craig, A. Specific induction of bladder cancer in mice by butyl-(4-hydroxybutyl)-nitrosamine and the effects of hormonal modifications on the sex difference in response. Eur. J. Cancer (1965) 1972, 8, 587–594. [Google Scholar] [CrossRef]
- Adeyeye, S.A.O. Heterocyclic Amines and Polycyclic Aromatic Hydrocarbons in Cooked Meat Products: A Review. Polycycl. Aromat. Compd. 2018, 1–11. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Cervellin, G. Meat consumption and cancer risk: a critical review of published meta-analyses. Crit. Rev. Oncol. 2016, 97, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.-W.; Zhao, L.-G.; Yang, Y.; Ma, X.; Wang, Y.-Y.; Xiang, Y.B. Obesity and Risk of Bladder Cancer: A Dose-Response Meta-Analysis of 15 Cohort Studies. PLoS ONE 2015, 10, e0119313. [Google Scholar] [CrossRef] [PubMed]
- Pollak, M. The insulin and insulin-like growth factor receptor family in neoplasia: An update. Nat. Rev. Cancer 2012, 12, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Keimling, M.; Behrens, G.; Schmid, D.; Jochem, C.; Leitzmann, M.F. The association between physical activity and bladder cancer: systematic review and meta-analysis. Br. J. Cancer 2014, 110, 1862–1870. [Google Scholar] [CrossRef]
- Ross, A.G.; Inobaya, M.T.; Olveda, R.M.; Chau, T.N.; Olveda, D.U. Prevention and control of schistosomiasis: A current perspective. Res. Rep. Trop. Med. 2014, 2014, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Rambau, P.; Chalya, P.L.; Jackson, K. Schistosomiasis and urinary bladder cancer in North Western Tanzania: A retrospective review of 185 patients. Infect. Agents Cancer 2013, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Kurahashi, N.; Inoue, M.; Liu, Y.; Iwasaki, M.; Sasazuki, S.; Sobue, T.; Tsugane, S.; for the JPHC Study Group. Passive smoking and lung cancer in Japanese non-smoking women: A prospective study. Int. J. Cancer 2007, 122, 653–657. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.; Cox, A.; Teare, M.D.; Catto, J.W.; Cumberbatch, M.M.G.K.; Catto, M.J.W.F. Contemporary Occupational Carcinogen Exposure and Bladder Cancer. JAMA Oncol. 2015, 1, 1. [Google Scholar] [CrossRef] [Green Version]
- Lotan, Y.; Goodman, P.J.; Youssef, R.F.; Svatek, R.S.; Shariat, S.F.; Tangen, C.M.; Thompson, I.M.; Klein, E.A. Evaluation of vitamin E and selenium supplementation for the prevention of bladder cancer in SWOG coordinated SELECT. J. Urol. 2012, 187, 2005–2010. [Google Scholar] [CrossRef] [Green Version]
- Inobaya, M.; Chau, T.N.; Ng, S.-K.; MacDougall, C.; Olveda, R.M.; Tallo, V.L.; Landicho, J.M.; Malacad, C.M.; Aligato, M.F.; Guevarra, J.R.; et al. Mass drug administration and the sustainable control of schistosomiasis: Community health workers are vital for global elimination efforts. Int. J. Infect. Dis. 2018, 66, 14–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. https://doi.org/10.3390/medsci8010015
Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of Bladder Cancer. Medical Sciences. 2020; 8(1):15. https://doi.org/10.3390/medsci8010015
Chicago/Turabian StyleSaginala, Kalyan, Adam Barsouk, John Sukumar Aluru, Prashanth Rawla, Sandeep Anand Padala, and Alexander Barsouk. 2020. "Epidemiology of Bladder Cancer" Medical Sciences 8, no. 1: 15. https://doi.org/10.3390/medsci8010015
APA StyleSaginala, K., Barsouk, A., Aluru, J. S., Rawla, P., Padala, S. A., & Barsouk, A. (2020). Epidemiology of Bladder Cancer. Medical Sciences, 8(1), 15. https://doi.org/10.3390/medsci8010015