
Predictors of Vaccination Intentions and Behaviour during the COVID-19 Pandemic in Italy
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Research Overview
3. Study 1
3.1. Methods
3.1.1. Participants and Procedure
3.1.2. Measures
3.1.3. Data Analyses
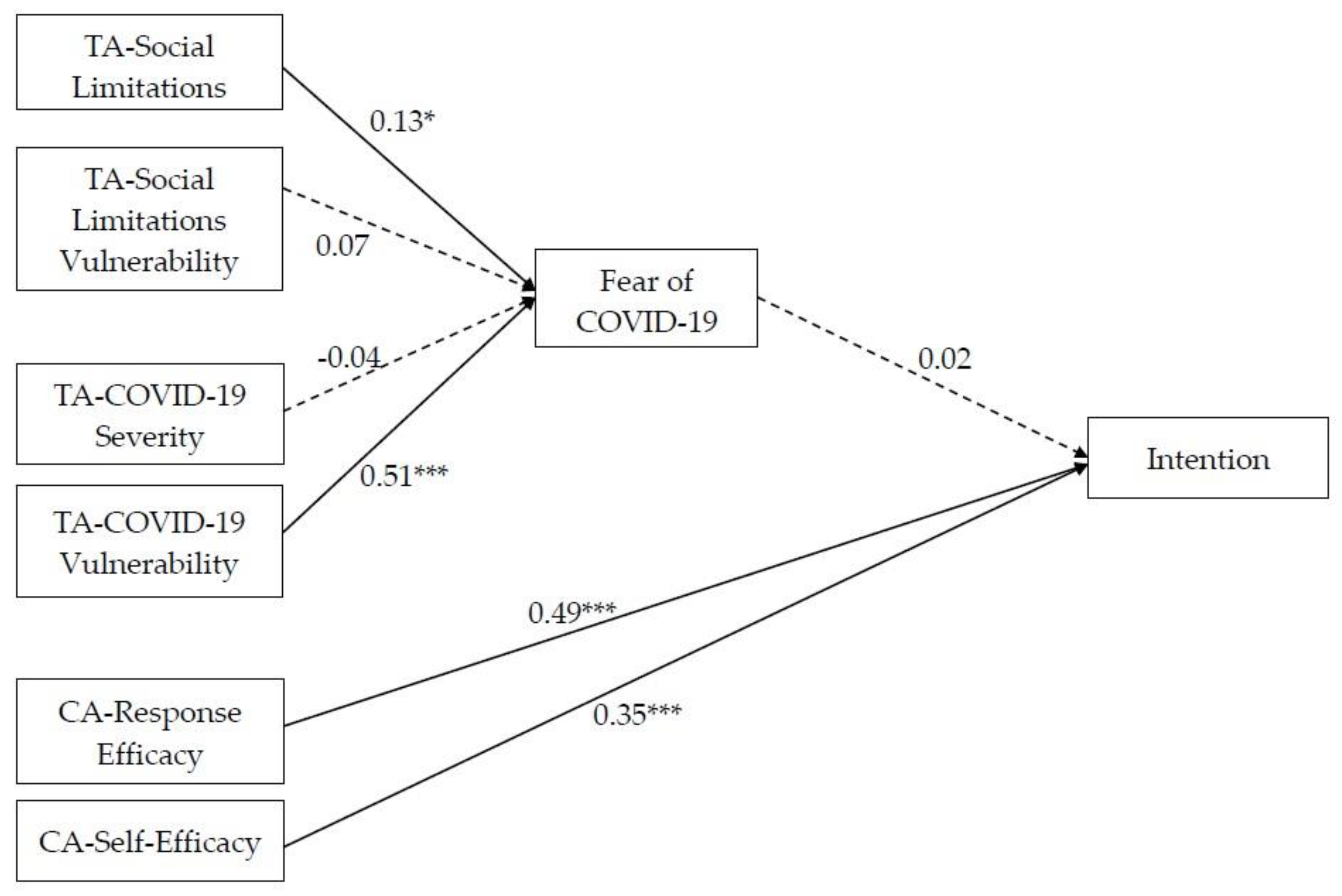
3.2. Results
4. Study 2
4.1. Methods
4.1.1. Participants and Procedure
4.1.2. Measures
4.2. Results
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 11 March 2020).
- Ministry of Health. Fase 2, Governo Vara Nuovo Dpcm Su Riaperture. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4772 (accessed on 19 November 2021).
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.W. Cognitive and physiological processes in fear appeals and attitude change: A revised theory of protection motivation. In Social Psychophysiology: A Source Book; Cacioppo, J.T., Petty, R.E., Eds.; Guilford Press: New York, NY, USA, 1983; pp. 153–176. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Boss, S.R.; Bentley University; Galletta, D.F.; Lowry, P.B.; Moody, G.D.; Polak, P. What do systems users have to fear? Using fear appeals to engender threats and fear that motivate protective security behaviors. MIS Q. 2015, 39, 837–864. [Google Scholar] [CrossRef]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A meta-analysis of research on protection motivation theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Ansari-Moghaddam, A.; Seraji, M.; Sharafi, Z.; Mohammadi, M.; Okati-Aliabad, H. The protection motivation theory for predict intention of COVID-19 vaccination in Iran: A structural equation modeling approach. BMC Public Health 2021, 21, 1165. [Google Scholar] [CrossRef]
- Li, L.; Wang, J.; Nicholas, S.; Maitland, E.; Leng, A.; Liu, R. The Intention to Receive the COVID-19 Vaccine in China: Insights from Protection Motivation Theory. Vaccines 2021, 9, 445. [Google Scholar] [CrossRef]
- Tong, K.K.; He, M.; Wu, A.M.S.; Dang, L.; Chen, J.H. Cognitive Factors Influencing COVID-19 Vaccination Intentions: An Application of the Protection Motivation Theory Using a Probability Community Sample. Vaccines 2021, 9, 1170. [Google Scholar] [CrossRef]
- Wang, P.-W.; Ahorsu, D.K.; Lin, C.-Y.; Chen, I.-H.; Yen, C.-F.; Kuo, Y.-J.; Griffiths, M.D.; Pakpour, A.H. Motivation to have COVID-19 vaccination explained using an extended protection motivation theory among university students in China: The role of information sources. Vaccines 2021, 9, 380. [Google Scholar] [CrossRef]
- Xiao, Q.; Liu, X.; Wang, R.; Mao, Y.; Chen, H.; Li, X.; Liu, X.; Dai, J.; Gao, J.; Fu, H.; et al. Predictors of Willingness to Receive the COVID-19 Vaccine after Emergency Use Authorization: The Role of Coping Appraisal. Vaccines 2021, 9, 967. [Google Scholar] [CrossRef]
- Nerini, A.; Matera, C.; Policardo, G.R.; Di Gesto, C. Containment measures against COVID-19 in Italy: The role of protection motivation and values. J. Hum. Behav. Soc. Environ. 2021, 32, 754–767. [Google Scholar] [CrossRef]
- Diaz, P.; Zizzo, J.; Balaji, N.C.; Reddy, R.; Khodamoradi, K.; Ory, J.; Ramasamy, R. Fear about adverse effect on fertility is a major cause of COVID-19 vaccine hesitancy in the United States. Andrologia 2022, 54, e14361. [Google Scholar] [CrossRef]
- Montagni, I.; Ouazzani-Touhami, K.; Mebarki, A.; Texier, N.; Schück, S.; Tzourio, C. The CONFINS group Acceptance of a COVID-19 vaccine is associated with ability to detect fake news and health literacy. J. Public Health 2021, 43, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Muric, G.; Wu, Y.; Ferrara, E. COVID-19 Vaccine Hesitancy on social media: Building a public twitter data set of antivaccine content, vaccine misinformation, and conspiracies. JMIR Public Health Surveill. 2021, 7, e30642. [Google Scholar] [CrossRef] [PubMed]
- Duradoni, M.; Veloso, M.V.; La Gamma, M.; Monciatti, A.M.; Guazzini, A. Italian version of the Vaccination Fear Scale (VFS-6): Internal and external validation. Mediterr. J. Clin. Psychol. 2022, 10, 1–19. [Google Scholar] [CrossRef]
- Hortal, M.; Di Fabio, J.L. Vaccine rejection and vaccination management: The grey areasRecusa vacinal e gestão da imunização: Nuances e contrastes. Rev. Panam. De Salud Publica Pan Am. J. Public Health 2019, 43, e54. [Google Scholar]
- Mellers, B.A.; McGraw, A.P. Anticipated emotions as guides to choice. Curr. Dir. Psychol. Sci. 2001, 10, S210–S214. [Google Scholar] [CrossRef]
- Sato, R.; Fintan, B. Fear, knowledge, and vaccination behaviors among women in Northern Nigeria. Hum. Vaccines Immunother. 2020, 16, 2438–2448. [Google Scholar] [CrossRef]
- Tahir, A.I.; Ramadhan, D.S.; Taha, A.A.; Abdullah, R.Y.; Karim, S.K.; Ahmed, A.K.; Ahmed, S.F. Public fear of COVID-19 vaccines in Iraqi Kurdistan region: A cross-sectional study. Middle East Curr. Psychiatry 2021, 28, 1–8. [Google Scholar] [CrossRef]
- SAGE Working Group. Report of the SAGE Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Ten Threats to Global Health in 2019. 2020. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 23 August 2023).
- Howard, M.C. The good, the bad, and the neutral: Vaccine hesitancy mediates the relations of Psychological Capital, the Dark Triad, and the Big Five with vaccination willingness and behaviors. Pers. Individ. Differ. 2022, 190, 111523. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Weston, R.; Gore, P.A., Jr. A brief guide to structural equation modeling. Couns. Psychol. 2006, 34, 719–751. [Google Scholar] [CrossRef]
- Bashirian, S.; Jenabi, E.; Khazaei, S.; Barati, M.; Karimi-Shahanjarini, A.; Zareian, S.; Rezapur-Shahkolai, F.; Moeini, B. Factors associated with preventive behaviours of COVID-19 among hospital staff in Iran in 2020: An application of the Protection Motivation Theory. J. Hosp. Infect. 2020, 105, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Roma, P.; Monaro, M.; Muzi, L.; Colasanti, M.; Ricci, E.; Biondi, S.; Napoli, C.; Ferracuti, S.; Mazza, C. How to improve compliance with protective health measures during the COVID-19 outbreak: Testing a moderated mediation model and machine learning algorithms. Int. J. Environ. Res. Public Health 2020, 17, 7252. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 4, 1–10. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The fear of COVID-19 scale: Development and initial validation. Int. J. Ment. Health Addict. 2020, 20, 1537–1545. [Google Scholar] [CrossRef] [PubMed]
- Rucker, D.D.; Preacher, K.J.; Tormala, Z.L.; Petty, R.E. Mediation analysis in social psychology: Current practices and new recommendations. Soc. Pers. Psychol. Compass 2011, 5, 359–371. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Chiorri, C.; Bracco, F.; Piccinno, T.; Modafferi, C.; Battini, V. Psychometric properties of a revised version of the ten item personality inventory. Eur. J. Psychol. Assess. 2015, 31, 109–119. [Google Scholar] [CrossRef]
- Gosling, S.D.; Rentfrow, P.J.; Swann, W.B., Jr. A Very Brief Measure of the Big-Five Personality Domains. J. Res. Pers. 2003, 37, 504–528. [Google Scholar] [CrossRef]
- Malas, O.; Tolsá, M.D. Vaccination Fear Scale (VFS-6): Development and Initial Validation. Mediterr. J. Clin. Psychol. 2021, 9, 2. [Google Scholar] [CrossRef]
- Everitt, B.S.; Landau, S.; Leese, M.; Stahl, D. Cluster Analysis; John Wiley & Sons: Hoboken, NY, USA, 2011. [Google Scholar]
- Brumbaugh, J.T.; Sokoto, K.C.; Wright, C.D.; Francis, S.E.; Hubbard, J.; Alexander, L.; McNeil, D.W. Vaccination intention and uptake within the Black community in Appalachia. Health Psychol. 2023, 42, 557–566. [Google Scholar] [CrossRef]
- Simione, L.; Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. How Implicit Attitudes toward Vaccination Affect Vaccine Hesitancy and Behaviour: Developing and Validating the V-IRAP. Int. J. Environ. Res. Public Health 2022, 19, 4205. [Google Scholar] [CrossRef] [PubMed]
- Lewin, K. Field Theory in Social Science: Selected Theoretical Papers; Harper & Brothers Publishers: Manhattan, NY, USA, 1951. [Google Scholar]
- Deutsch, M.; Gerard, H.B. A study of normative and informational social influences upon individual judgment. J. Abnorm. Soc. Psychol. 1955, 51, 629. [Google Scholar] [CrossRef] [PubMed]
- Kelman, H.C. Compliance, identification, and internalization three processes of attitude change. J. Confl. Resolut. 1958, 2, 51–60. [Google Scholar] [CrossRef]
- Guazzini, A.; Fiorenza, M.; Panerai, G.; Duradoni, M. What went wrong? Predictors of contact tracing adoption in Italy during COVID-19 pandemic. Future Internet 2021, 13, 286. [Google Scholar] [CrossRef]
- Matera, C.; Paradisi, M.; Boin, J.; Nerini, A. Perceived mattering in the face of COVID-19: Links with emotion regulation and psychological well-being. Psychol. Health 2022, 37, 1471–1491. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Min–Max | M (SD) |
|---|---|---|
| TA—Social limitations Severity | 1–5 | 3.94 (1.10) |
| TA—Social limitations Vulnerability | 1–5 | 4.38 (0.69) |
| TA—COVID-19 Severity | 1–5 | 4.59 (0.72) |
| TA—COVID-19 Vulnerability | 1–5 | 3.14 (1.03) |
| CA—Self-efficacy | 1–5 | 4.33 (0.81) |
| CA—Response Efficacy | 1–5 | 4.29 (0.87) |
| Fear of COVID-19 | 1–5 | 2.47 (0.86) |
| Intention to get vaccinated | 1–5 | 4.54 (0.89) |
| Variables | 1. | 2. | 3. | 4. | 5. | 6. | 7. |
|---|---|---|---|---|---|---|---|
| 1. TA—Social limitations Vulnerability | - | ||||||
| 2. TA—Social limitations Severity | 0.23 *** | - | |||||
| 3. TA—COVID-19 Severity | 0.23 *** | 0.50 *** | - | ||||
| 4. TA—COVID-19 Vulnerability | 0.23 *** | 0.33 *** | 0.32 *** | - | |||
| 5. CA—Self-efficacy | 0.29 *** | 0.42 *** | 0.42 *** | 0.29 *** | - | ||
| 6. CA—Response Efficacy | 0.36 *** | 0.60 *** | 0.57 *** | 0.37 *** | 0.62 *** | - | |
| 7. Fear of COVID-19 | 0.22 *** | 0.27 *** | 0.20 ** | 0.59 *** | 0.19 ** | 0.35 *** | - |
| 8. Intention to get vaccinated | 0.24 *** | 0.47 *** | 0.47 *** | 0.21 ** | 0.66 *** | 0.71 *** | 0.26 *** |
| Variables | Entire Sample | Females | Males |
|---|---|---|---|
| M (SD) | M (SD) | M (SD) | |
| Age | 38.33 (13.94) | 38.05 (13.82) | 38.67 (14.44) |
| Extraversion | 8.19 (2.76) | 8.38 (2.85) | 7.74 (2.50) |
| Agreeableness | 10.38 (2.03) | 10.49 (2.01) | 10.05 (2.08) |
| Conscientiousness | 10.42 (2.36) | 10.57 (2.28) | 10.12 (2.44) |
| Neuroticism | 7.62 (2.77) | 7.90 (2.73) | 6.94 (2.74) |
| Openness | 9.07 (2.12) | 9.09 (2.09) | 4.37 (2.31) |
| VF—Cognitive | 7.61 (4.07) | 7.74 (4.19) | 6.94 (3.66) |
| VF—Somatic | 5.00 (3.01) | 5.18 (3.19) | 4.37 (2.31) |
| VH—Confidence | 10.21 (1.35) | 10.18 (3.30) | 10.53 (3.46) |
| VH—Complacency | 5.44 (2.83) | 5.17 (2.60) | 5.94 (3.20) |
| VH—Constraints | 4.77 (2.29) | 4.66 (2.20) | 4.82 (2.35) |
| VH—Calculation | 11.03 (2.65) | 11.00 (2.53) | 11.00 (2.91) |
| VH—Collective responsibility | 11.95 (3.00) | 12.15 (2.84) | 11.66 (3.26) |
| Predictors | Coefficient |
|---|---|
| VH Confidence | 0.31 |
| VH Complacency | −0.23 |
| VH Constraints | ns |
| VH Calculation | −0.12 |
| VH Collective responsibility | 0.57 |
| Predictors | VH Confidence | VH Complacency | VH Calculation | VH Collective Responsibility |
|---|---|---|---|---|
| Age | −0.04 | −0.01 | 0.07 * | −0.06 * |
| Sex | 0.01 | −0.16 *** | −0.04 | 0.12 *** |
| Extraversion | 0.02 | 0.01 | 0.02 | −0.01 |
| Agreeableness | 0.01 | −0.06 * | 0.07 * | 0.02 |
| Conscientiousness | 0.02 | −0.02 | 0.04 | 0.01 |
| Neuroticism | 0.06 ** | −0.16 ** | −0.02 | 0.12 *** |
| Openness | −0.02 | 0.05 * | 0.01 | −0.02 |
| VF—Cognitive | −0.76 *** | 0.57 *** | 0.38 *** | −0.60 *** |
| VF—Somatic | −0.02 | 0.11 *** | 0.01 | −0.11 *** |
| R2 | 0.60 | 0.46 | 0.17 | 0.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nerini, A.; Duradoni, M.; Matera, C.; Guazzini, A.; Paradisi, M.; Schembri, A. Predictors of Vaccination Intentions and Behaviour during the COVID-19 Pandemic in Italy. Behav. Sci. 2023, 13, 950. https://doi.org/10.3390/bs13110950
Nerini A, Duradoni M, Matera C, Guazzini A, Paradisi M, Schembri A. Predictors of Vaccination Intentions and Behaviour during the COVID-19 Pandemic in Italy. Behavioral Sciences. 2023; 13(11):950. https://doi.org/10.3390/bs13110950
Chicago/Turabian StyleNerini, Amanda, Mirko Duradoni, Camilla Matera, Andrea Guazzini, Monica Paradisi, and Adriele Schembri. 2023. "Predictors of Vaccination Intentions and Behaviour during the COVID-19 Pandemic in Italy" Behavioral Sciences 13, no. 11: 950. https://doi.org/10.3390/bs13110950
APA StyleNerini, A., Duradoni, M., Matera, C., Guazzini, A., Paradisi, M., & Schembri, A. (2023). Predictors of Vaccination Intentions and Behaviour during the COVID-19 Pandemic in Italy. Behavioral Sciences, 13(11), 950. https://doi.org/10.3390/bs13110950