
Psychological Resilience Interventions for Adolescents during the COVID-19 Pandemic

Abstract
:1. Introduction
- Are there differences in the levels of psychological resilience of junior high and high school students in different grades, and if so, how do these variations manifest?
- Does the resilience intervention for junior high and high school students have different effects due to their different development status?
- In which grades do interventions produce the best results?
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Intervention Group
Psychological Course Training
Physical Training
2.2.2. Control Group
2.3. Measures
2.4. Statistical Analyses
3. Results
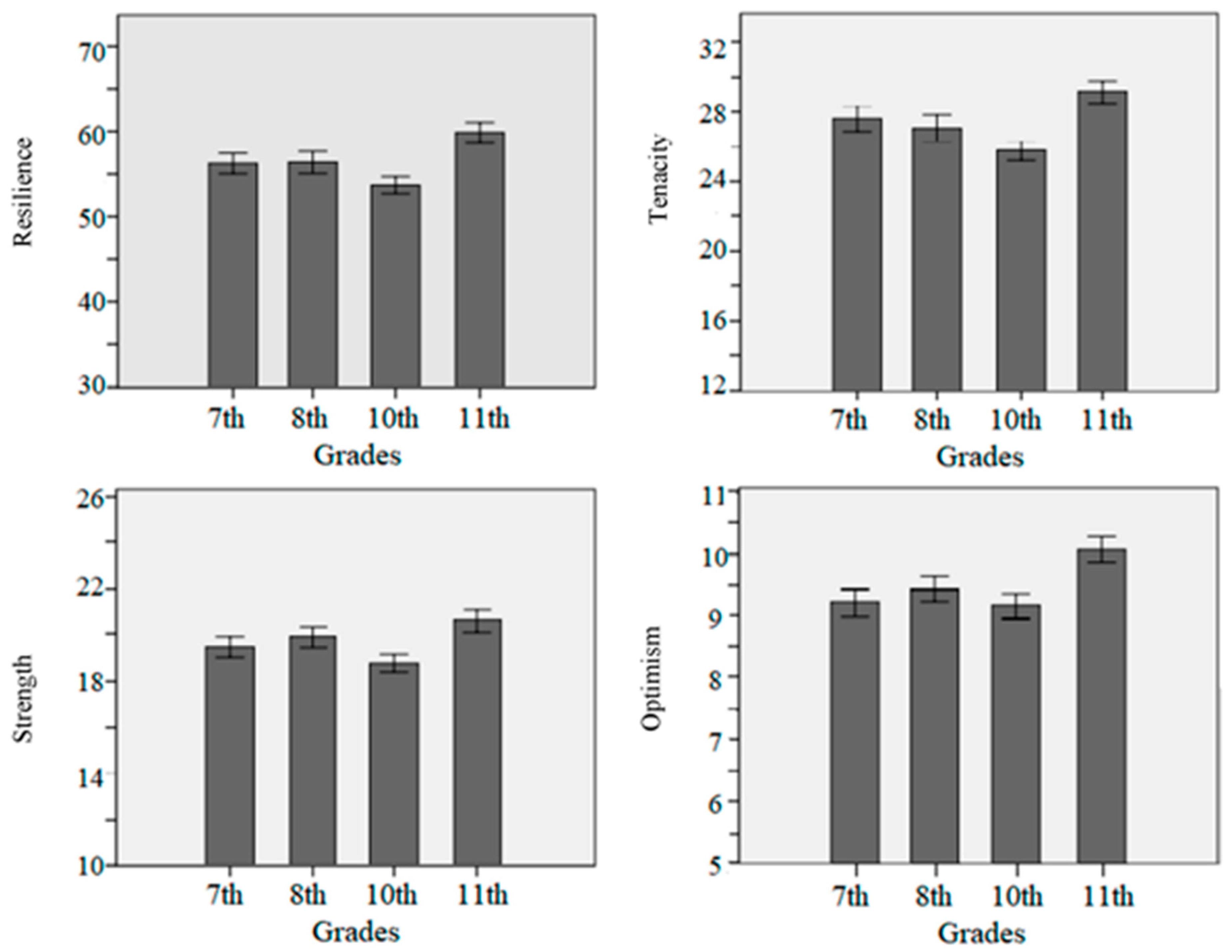
3.1. The Resilience Development Pattern in Adolescents
3.2. The Effects of Resilience Interventions for Adolescents of Various Grades
3.2.1. The Effect of Resilience Intervention in the Seventh Grade
3.2.2. The Effect of Resilience Intervention in the Eighth Grade
3.2.3. The Effect of Resilience Intervention in the 10th Grade
3.2.4. The Effect of Resilience Intervention in the 11th Grade
4. Discussion
4.1. The Resilience Development Pattern in Adolescents
4.2. The Critical Period of Resilience Intervention for Adolescents
4.3. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard; World Health Organization: Geneva, Switzerland, 2023; Available online: https://covid19.who.int/data/ (accessed on 1 December 2022).
- Jafri, M.R.; Zaheer, A.; Fatima, S.; Saleem, T.; Sohail, A. Mental health status of COVID-19 survivors: A cross sectional study. Virol. J. 2022, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Hamatani, S.; Shimizu, E.; Käll, A.; Andersson, G. Impact of post-COVID conditions on mental health: A cross-sectional study in Japan and Sweden. BMC Psychiatry 2022, 22, 237. [Google Scholar] [CrossRef]
- Pandey, K.; Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental health issues during and after COVID-19 vaccine era. Brain Res. Bull. 2021, 176, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Dixit, S.; Musa, A.; Sillva, A.B.; Reddy, R.S.; Abohashrh, M.; Kakaraparthi, V.N.; Asiri, F.; Caruso, F.R.; Govindappa, S.K.; Mohammed, A.A. The impact of post-traumatic stress of SARS-CoV-2 affliction on psychological and mental health of student survivors: Cross sectional study. Front. Public Health 2022, 10, 845741. [Google Scholar] [CrossRef]
- Prati, G. Mental health and its psychosocial predictors during national quarantine in Italy against the coronavirus disease 2019 (COVID-19). Anxiety Stress Coping 2021, 34, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Varma, P.; Junge, M.; Meaklim, H.; Jackson, M.L. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: A global cross-sectional survey. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 109, 110236. [Google Scholar] [CrossRef]
- Araújo, F.J.O.; Lima, L.S.A.; Cidade, P.I.M.; Nobre, C.B.; Neto, M.L.R. Impact of SARS-CoV-2 and its reverberation in global higher education and mental health. Psychiatry Res. 2020, 288, 112977. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef] [Green Version]
- Javed, B.; Sarwer, A.; Soto, E.B.; Mashwani, Z.R. Impact of SARS-CoV-2 (Coronavirus) pandemic on public mental health. Front. Public Health 2020, 8, 292. [Google Scholar] [CrossRef]
- Shi, W.; Zhao, L.; Liu, M.; Hong, B.; Jiang, L.; Jia, P. Resilience and mental health: A longitudinal cohort study of Chinese adolescents before and during COVID-19. Front. Psychiatry 2022, 13, 948036. [Google Scholar] [CrossRef]
- de Oliveira, J.M.D.; Butini, L.; Pauletto, P.; Lehmkuhl, K.M.; Stefani, C.M.; Bolan, M.; Guerra, E.; Dick, B.; De Luca Canto, G.; Massignan, C. Mental health effects prevalence in children and adolescents during the COVID- 19 pandemic: A systematic review. Evid.-Based Nurs. 2022, 19, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Shoshani, A.; Kor, A. The mental health effects of the COVID-19 pandemic on children and adolescents: Risk and protective factors. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 14, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.T. Mental health and its correlates among children and adolescents during COVID-19 school closure: The importance of parent-child discussion. J. Affect. Disord. 2021, 279, 353–360. [Google Scholar] [CrossRef]
- Martinsone, B.; Stokenberga, I.; Damberga, I.; Supe, I.; Simões, C.; Lebre, P.; Canha, L.; Santos, M.; Santos, A.C.; Fonseca, A.M.; et al. Adolescent social emotional skills, resilience and behavioral problems during the COVID-19 pandemic: A longitudinal study in three European countries. Front. Psychiatry 2022, 13, 942692. [Google Scholar] [CrossRef]
- World Health Organization. Adolescent Mental Health; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int (accessed on 1 December 2022).
- Cerit, E.; Simsek, N.A. social skills development training programme to improve adolescents’ psychological resilience and emotional intelligence level. Arch. Psychiatr. Nurs. 2021, 35, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Romeo, D.R. The Metamorphosis of Adolescent Hormonal Stress eactivity: A Focus on Animal Models. Front. Neuroendocrinol. 2018, 49, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.B.; Groenewald, C.B.; de la Vega, R.; Palermo, T.M. Long-term impact of adolescent chronic pain on young adult educational, vocational, and social outcomes. Pain 2020, 161, 439–445. [Google Scholar] [CrossRef]
- Ma, L.; Mazidi, M.; Li, K.; Li, Y.; Chen, S.; Kirwan, R.; Zhou, H.; Yan, N.; Rahman, A.; Wang, W.; et al. Prevalence of mental health problems among children and adolescents during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 293, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.J.; Barblanb, L.P.; Lory, I.; Landolt, M.A. Age-related effects of the COVID-19 pandemic on mental health of children and adolescents. Eur. J. Psychotraumatol. 2021, 12, 1901407. [Google Scholar] [CrossRef]
- Camacho-Thompson, D.E.; Gillen-O’Neel, C.; Gonzales, N.A.; Fuligni, A.J. Financial Strain, Major Family Life Events, and Parental Academic Involvement during Adolescence. J. Youth Adolesc. 2016, 45, 1065–1074. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.E.; Parra, L.A.; Ugarte, E.; Weissman, D.G.; Han, S.G.; Robins, R.W.; Guyer, A.E.; Hastings, P.E. Patterns of poverty across adolescence predict salivary cortisol stress responses in Mexican-origin youths. Psychoneuroendocrinology 2021, 132, 105340. [Google Scholar] [CrossRef] [PubMed]
- Imran, N.; Zeshan, M.; Pervaiz, Z. Mental health considerations for children & adolescents in COVID-19 Pandemic. Pak. J. Med. Sci. 2020, 36, S67–S72. [Google Scholar] [CrossRef] [PubMed]
- The National Child Traumatic Stress Network. Parent Tips for Helping School Age Children after Disaster; National Center for Child Traumatic Stress: Rockville, MD, USA, 2020; Available online: www.nctsn.org (accessed on 18 April 2020).
- Ye, Z.; Yang, X.; Zeng, C.; Wang, Y.; Shen, Z.; Li, X.; Lin, D. Resilience, social support, and coping as mediators between COVID-19-related stressful experiences and acute stress disorder among college students in China. Appl. Psychol. Health Well-Being 2020, 12, 1074–1094. [Google Scholar] [CrossRef] [PubMed]
- Kimhi, S.; Marciano, H.; Eshel, Y.; Adini, B. Resilience and demographic characteristics predicting distress during the COVID-19 crisis. Soc. Sci. Med. 2020, 265, 113389. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.S.; Taylor, E.C.; Cloonan, S.A.; Dailey, N.S. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020, 291, 113216. [Google Scholar] [CrossRef] [PubMed]
- Lai, B.S.; Esnard, A.M.; Lowe, S.R.; Peek, L. Schools and disasters: Safety and mental health assessment and interventions for children. Curr. Psychiatry Rep. 2016, 18, 109. [Google Scholar] [CrossRef]
- Niu, Y.; Jiang, N.; Jiang, X. Factors related to the resilience of Tibetan adolescent survivors ten years after the Yushu earthquake. Int. J. Disaster Risk Reduct. 2021, 65, 102554. [Google Scholar] [CrossRef]
- Pozuelo, R.J.; Kilford, J.E. Adolescent Health Series: Adolescent neurocognitive development in Western and Sub-Saharan African contexts. Trop. Med. Int. Health 2021, 26, 1333–1344. [Google Scholar] [CrossRef]
- Perica, M.I.; Calabro, F.J.; Larsen, B.; Foran, W.; Yushmanov, V.E.; Hetherington, H.; Tervo-Clemmens, B.; Moon, C.; Luna, B. Development of frontal GABA and glutamate supports excitation/inhibition balance from adolescence into adulthood. Prog. Neurobiol. 2022, 219, 102370. [Google Scholar] [CrossRef]
- Azad, A.; Cabeen, R.P.; Sepehrband, F.; Kim, R.; Campbell, C.E.; Lynch, K.; Tyszka, J.M.; Herting, M.M. Microstructural properties within the amygdala and affiliated white matter tracts across adolescence. NeuroImage 2021, 243, 118489. [Google Scholar] [CrossRef]
- Campbell, C.E.; Mezher, A.F.; Eckel, S.P.; Tyszka, M.J.; Pauli, W.M.; Nagel, B.J.; Herting, M.M. Restructuring of amygdala subregion apportion across adolescence. Dev. Cogn. Neurosci. 2021, 48, 100883. [Google Scholar] [CrossRef]
- Pan, P.M.; Sato, J.R.; Martinot, M.P.; Martinot, J.; Artiges, E.; Penttilä, J. Longitudinal Trajectory of the Link Between Ventral Striatum and Depression in Adolescence. Am. J. Psychiatry 2022, 179, 470–481. [Google Scholar] [CrossRef] [PubMed]
- Peters, K.Z.; Naneix, F. The role of dopamine and endocannabinoid systems in prefrontal cortex development: Adolescence as a critical period. Front. Neural Circuits 2022, 16, 939235. [Google Scholar] [CrossRef]
- Lynch, K.M.; Shi, Y.; Toga, A.W.; Clark, K.A. Hippocampal Shape Maturation in Childhood and Adolescence. Cereb. Cortex 2019, 19, 3651–3665. [Google Scholar] [CrossRef] [PubMed]
- Dow-Edwards, D.; MacMaster, F.P.; Peterson, B.S.; Niesink, R.; Andersen, S.; Braams, B.R. Experience during adolescence shapes brain development: From synapses and networks to normal and pathological behavior. Neurotoxicol. Teratol. 2019, 76, 106834. [Google Scholar] [CrossRef] [PubMed]
- Tso, W.W.Y.; Wong, R.S.; Tung, K.T.S.; Rao, N.; Fu, K.W.; Yam, J.C.S.; Chua, G.T.; Chen, E.Y.H.; Lee, T.M.C.; Chan, S.K.W.; et al. Vulnerability and resilience in children during the COVID-19 pandemic. Eur. Child Adolesc. Psychiatry 2022, 31, 161–176. [Google Scholar] [CrossRef]
- Foulkes, L.; Blakemore, S.J. Individual differences in adolescent mental health during COVID-19: The importance of peer relationship quality. Neuron 2021, 109, 3203–3205. [Google Scholar] [CrossRef]
- Zhang, C.; Ye, M.; Fu, Y.; Yang, M.; Luo, F.; Yuan, J.; Tao, Q. The psychological impact of the COVID-19 pandemic on teenagers in China. J. Adolesc. Health 2020, 67, 747–755. [Google Scholar] [CrossRef]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 11. [Google Scholar] [CrossRef]
- Cooper, K.; Hards, E.; Moltrecht, B.; Reynolds, S.; Shum, A.; McElroy, E.; Loades, M. Loneliness, social relationships, and mental health in adolescents during the COVID-19 pandemic. J. Affect. Disord. 2021, 289, 98–104. [Google Scholar] [CrossRef]
- Xing, J. A conceptual model of adolescentsattachment and resilience to daily stressors: Implications for COVID-19 normalization period and afterwards. Psychiatr. Danub. 2022, 34, 743–751. [Google Scholar] [CrossRef]
- Houston, J.B.; First, J.; Spialek, M.L.; Sorenson, M.E.; Mills-Sandoval, T.; Lockett, M.; First, N.L.; Nitiéma, P.; Allen, S.F.; Pfefferbaum, B. Randomized Controlled Trial of the Resilience and Coping Intervention (RCI) with Undergraduate University Students. J. Am. Coll. Health 2016, 65, 1–9. [Google Scholar] [CrossRef]
- Li, X.; Harrison, S.E.; Fairchild, A.J.; Chi, P.; Zhao, J.; Zhao, G. A randomized controlled trial of a resilience-based intervention on psychosocial well-being of children affected by HIV/AIDS: Effects at 6-and 12-month follow-up. Soc. Sci. Med. 2017, 190, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, S.L.; Gaede, C. A test of a resilience based intervention for mental health problems in Iraqi internally displaced person camps. Anxiety Stress Coping 2020, 33, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Vella, S.A.; Swann, C.; Batterham, M.; Boydell, K.M.; Eckermann, S.; Ferguson, H.; Fogarty, A.; Hurley, D.; Liddle, S.K.; Lonsdale, C.; et al. An intervention for mental health literacy and resilience in organized sports. Med. Sci. Sport. Exerc. 2021, 53, 139–149. [Google Scholar] [CrossRef]
- Moore, B.; Woodcock, S.; Dudley, D. Well-being warriors: A randomized controlled trial examining the effects of martial arts training on secondary students’ resilience. Br. J. Educ. Psychol. 2021, 91, 1369–1394. [Google Scholar] [CrossRef]
- Meade, J. Mental health effects of the COVID-19 pandemic on children and adolescents a review of the current research. Pediatr. Clin. N. Am. 2021, 68, 945–959. [Google Scholar] [CrossRef]
- Gee, G.D. Early Adversity and Development: Parsing Heterogeneity and Identifying Pathways of Risk and Resilience. Am. J. Psychiatry 2021, 178, 998–1013. [Google Scholar] [CrossRef]
- Casey, J.B.; Heller, S.A.; Gee, G.D.; Cohen, O.A. Development of the Emotional Brain. Neurosci. Lett. 2019, 693, 29–34. [Google Scholar] [CrossRef]
- Straub, J.; Brown, R.; Malejko, K.; Bonenberger, M.; Grön, G.; Plener, P.L.; Abler, B. Adolescent depression and brain development: Evidence from voxel-based morphometry. J. Psychiatry Neurosci. 2019, 44, 237–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Cheng, Z.; Wu, J. Risk factors for adolescents’ mental health during the COVID-19 pandemic: A comparison between Wuhan and other urban areas in China. Glob. Health 2020, 16, 96. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, A.L.; Kammeyer-Mueller, J.; Simon, L.; Corwin, E.S.; Morrison, H.; Whiting, S. Evaluating various sources of common method bias and psychological separation as an alternate remedy. Acad. Manag. Annu. Meet. Proc. 2020, 2020, 13501. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Zhang, J. Factor analysis and psychometric evaluation of the Connor–Davidson Resilience Scale (CD-RISC) with Chinese people. Soc. Behav. Personal. 2007, 35, 19–30. [Google Scholar] [CrossRef]
- Waddimba, A.C.; Baker, B.M.; Pogue, J.R.; McAuliffe, M.P.; Bennett, M.M.; Baxter, R.D.; Mohr, D.C.; Warren, A.M. Psychometric validity and reliability of the 10-and 2-item Connor–Davidson resilience scales among a national sample of Americans responding to the COVID-19 pandemic: An item response theory analysis. Qual. Life Res. 2022, 31, 2819–2836. [Google Scholar] [CrossRef]
- Mesman, E.; Vreeker, A.; Hillegers, M. Resilience and mental health in children and adolescents: An update of the recent literature and future directions. Curr. Opin. Psychiatry 2021, 34, 586. [Google Scholar] [CrossRef]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An investigation of mental health status of children and adolescents in china during the outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef]
- Niu, Y.; Jiang, X.L.; Ashong, Z.; Hou, J.F.; Bai, Y.B.; Bai, G.Z.; Xu, J.J.; Ren, W.Y.; Geng, G.Z. Developing a resilience intervention approach for adolescents living with natural hazards risks: A pilot randomized controlled trial. Int. J. Disaster Risk Reduct. 2021, 58, 102190. [Google Scholar] [CrossRef]
- Liang, Z.; Kang, D.; Zhang, M.; Xia, Y.; Zeng, Q. The Impact of the COVID-19 Pandemic on Chinese Postgraduate Students’ Mental Health. Int. J. Environ. Res. Public. Health 2021, 18, 11542. [Google Scholar] [CrossRef]
- Wang, C.; Tee, M.; Roy, A.E.; Fardin, M.A.; Srichokchatchawan, W.; Habib, H.A.; Tran, B.X.; Hussain, S.; Hoang, M.T.; Le, X.T.; et al. The impact of COVID-19 pandemic on physical and mental health of Asians: A study of seven middle-income countries in Asia. PLoS ONE 2021, 16, e0246824. [Google Scholar] [CrossRef]
- Brix, N.; Ernst, A.; Lauridsen, L.L.B.; Parner, E.; Støvring, H.; Olsen, J.; Henriksen, T.B.; Ramlau-Hansen, C.H. Timing of puberty in boys and girls: A population-based study. Paediatr. Perinat. Epidemiol. 2019, 33, 70–78. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. In The Promise of Adolescence: Realizing Opportunity for All Youth; The National Academies Press: Washington, DC, USA, 2019. [CrossRef]
- Rossi, R.; Jannini, B.T.; Socci, V.; Pacitti, F.; Lorenzo, D.G. Stressful Life Events and Resilience During the COVID-19 Lockdown Measures in Italy: Association with Mental Health Outcomes and Age. Front. Psychiatry 2021, 12, 635832. [Google Scholar] [CrossRef]
- Gunnar, M.R.; DePasquale, C.E.; Reid, B.M.; Donzella, B.; Miller, B.S. Pubertal stress recalibration reverses the effects of early life stress in postinstitutionalized children. Proc. Natl. Acad. Sci. USA 2019, 116, 23984–23988. [Google Scholar] [CrossRef]
- Branje, S.; Morris, A.S. The impact of the COVID-19 pandemic on adolescent emotional, social, and academic adjustment. J. Res. Adolesc. 2021, 31, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, T. The Power of the Adolescent brain: Strategies for Teaching Middle and High School Students; ASCD: Arlington, VA, USA, 2016. [Google Scholar]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens Through the Twenties; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Larsen, B.; Luna, B. Adolescence as a neurobiological critical period for the development of higher-order cognition. Neurosci. Biobehav. Rev. 2018, 94, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Malave, L.; van Dijk, M.T.; Anacker, C. Early life adversity shapes neural circuit function during sensitive postnatal developmental periods. Transl. Psychiatry 2022, 12, 306. [Google Scholar] [CrossRef] [PubMed]
- de Figueiredo, C.S.; Sandre, P.C.; Portugal, L.C.L.; Mázala-de-Oliveira, T.; da Silva Chagas, L.; Raony, Í.; Ferreira, E.S.; Giestal-de-Araujo, E.; Dos Santos, A.A.; Bomfim, P.O. COVID-19 pandemic impact on children and adolescents’ mental health: Biological, environmental, and social factors. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 106, 110171. [Google Scholar] [CrossRef]
- Crone, E.A.; Steinbeis, N. Neural perspectives on cognitive control development during childhood and adolescence. Trends Cogn. Sci. 2017, 21, 205–215. [Google Scholar] [CrossRef] [Green Version]
- Nash, C. Enhancing Hopeful Resilience Regarding Depression and Anxiety with a Narrative Method of Ordering Memory Effective in Researchers Experiencing Burnout. Challenges 2022, 13, 28. [Google Scholar] [CrossRef]
- Méndez Leal, A.S.M.; Silvers, J.A. Neurobiological Markers of Resilience to Early Life Adversity during Adolescence. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 238–247. [Google Scholar] [CrossRef]
- Kalisch, R.; Baker, D.G.; Basten, U.; Boks, M.P.; Bonanno, G.A.; Brummelman, E.; Chmitorz, A.; Fernàndez, G.; Fiebach, C.J.; Galatzer-Levy, I.; et al. The resilience framework as a strategy to combat stress-related disorders. Nat. Hum. Behav. 2017, 1, 784–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feder, A.; Fred-Torres, S.; Southwick, S.M.; Charney, D.S. The Biology of Human Resilience: Opportunities for Enhancing Resilience Across the Life Span. Biol. Psychiatry 2019, 86, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Montez, D.F.; Calabro, F.J.; Luna, B. The expression of established cognitive brain states stabilizes with working memory development. eLife 2017, 6, e25606. [Google Scholar] [CrossRef] [PubMed]
- Lancaster, M.R.; Callaghan, P. The effect of exercise on resilience, its mediators and moderators, in a general population during the UK COVID-19 pandemic in 2020: A cross-sectional online study. BMC Public Health 2022, 22, 827. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Xu, W.; Yao, Y.; Zhang, L.; Guo, L.; Fan, J.; Chen, J. Mental health status of students’ parents during COVID-19 pandemic and its influence factors. Gen. Psychiatry 2020, 33, e100250. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Time | Theme | Sample of Content |
|---|---|---|
| The 1st week | Strength | Module 1: Clap hands in 30 s without stopping and experience the unlimited potential you have. Module 2: Self-portrait—express yourself as a plant or an animal. Module 3: Write down three of your strengths, and group members will add more of your advantages. Module 4: Share your most successful experience in class and realize you are great. |
| The 2nd week | Optimism | Module 1: Read a story of a happy farmer, and learn to be content with what you have. Module 2: Watch a video of dancing during the pandemic, and feel the optimism of medical caregivers and patients. Module 3: Read the fable “a blessing in disguise” and share your ideas. Module 4: Judge events from different perspectives with teachers’ guidance by the ABC Theory of Emotion. |
| The 3rd week | Tenacity (part 1) | Module 1: Watch Churchill’s speech which said the secret of success is never giving up. Module 2: Fill in the blanks of famous poems which talk about hardiness. Module 3: Feel your own willpower through an arm-raising activity. Module 4: Watch the story of “Nick Vujicic” and acquire his spirit. |
| The 4th week | Tenacity (part 2) | Module 5: Read the psychologist’s experiment and internalize the importance of setting goals with respect to hardiness. Module 6: Play the game “Who is the Wooden Man”—the people who remain still until the end will be the winners. Module 7: Stand on one foot and keep your body balanced, count how long you persist, then share your feelings. |
| 7th Grade (n = 147) | 8th Grade (n = 148) | 10th Grade (n = 131) | 11th Grade (n = 133) | |
|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | |
| Resilience | 56.26 (14.90) | 56.39 (16.05) | 53.69 (11.53) | 59.86 (13.59) |
| Strength | 19.44 (5.24) | 19.88 (5.70) | 18.76 (4.33) | 20.64 (4.97) |
| Optimism | 9.20 (2.82) | 9.43 (2.76) | 9.15 (2.24) | 10.08 (2.37) |
| Tenacity | 27.62 (8.61) | 27.08 (9.07) | 25.79 (6.42) | 29.15 (7.47) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xing, J.; Xu, X.; Li, X.; Luo, Q. Psychological Resilience Interventions for Adolescents during the COVID-19 Pandemic. Behav. Sci. 2023, 13, 543. https://doi.org/10.3390/bs13070543
Xing J, Xu X, Li X, Luo Q. Psychological Resilience Interventions for Adolescents during the COVID-19 Pandemic. Behavioral Sciences. 2023; 13(7):543. https://doi.org/10.3390/bs13070543
Chicago/Turabian StyleXing, Jingwen, Xiaofeng Xu, Xing Li, and Qing Luo. 2023. "Psychological Resilience Interventions for Adolescents during the COVID-19 Pandemic" Behavioral Sciences 13, no. 7: 543. https://doi.org/10.3390/bs13070543