Featured Application
Root canal treatment in canals with oval cross section.
Abstract
Apical extrusion of debris (AED) by the full sequence of the self-adjusting file (SAF) system was compared with that of the XP-endo shaper plus sequence. Sixty permanent mandibular incisors were randomly assigned to two groups (n = 30) for root canal instrumentation: Group A: Stage 1—pre-SAF OS, pre-SAF 1 and pre-SAF 2 files, followed by Stage 2—1.5 mm SAF; and Group B: Stage 1— hand K-file 15/0.02, followed by Stage 2—XP-endo shaper and Stage 3—XP-endo finisher. The AED produced during instrumentation at each stage was collected in pre-weighed Eppendorf tubes. The weights of AED by the two methods were compared using t tests with significance level set at 5%. Group A produced significantly less total AED than Group B (p < 0.001), with no significant difference in debris extrusion between the two stages (p = 0.3014). Conversely, in Group B, a significant difference was noted between Stage 1 and Stages 2 and 3 (p < 0.01), with no significant difference between Stages 2 and 3 (p = 0.488). Both sequences resulted in measurable amounts of AED. Each phase, in either procedure, made its own contribution to the extrusion of debris.
1. Introduction
Prevention of the apical extrusion of intracanal bacteria and debris during root canal instrumentation is among the most important objectives of the endodontic treatment of teeth with apical periodontitis [1]. Cases with apical debris extrusion are often clinically associated with pain or swelling post-endodontic instrumentation [2]. Such extrusion during root canal instrumentation (Figure 1) may also have a detrimental effect on healing after endodontic treatment [3,4,5]. The extrusion of debris is an involuntary result of root canal instrumentation, regardless of the types of instruments used [6]. The amount of debris extrusion may vary on the basis of kinematics, number of files used, taper, cross-section, and cutting efficacy [3,7]. A common notion is that techniques involving a push–pull motion create a greater mass of extruded debris than do those involving a rotational action [4]. Thus, endodontic files systems that may minimize debris extrusion should be investigated.
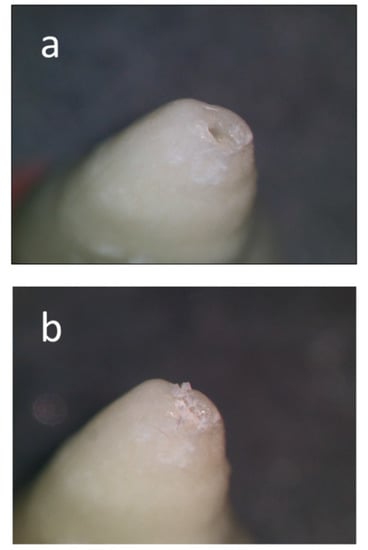
Figure 1.
Apical extrusion of debris. During root canal treatment, debris consisting of necrotic tissue, bacteria and dentin particles is often extruded through the apical foramen and into the periapical tissues. Such debris may cause severe response (“flare up”) and may jeopardize the long-term success of the root canal treatment. (a) Tip of the root with an apical foramen. (b) Debris extruded through the apical foramen during instrumentation of the root canal.
The aims of root canal instrumentation in infected oval root canals are hard to achieve, as common rotary and reciprocating files (Figure 2a) have a tendency to leave un-instrumented recesses, thus, leaving debris and unprepared root canal surfaces behind [8,9]. This limitation led to the development of two file systems that claim to be adaptive instrumentation methods: the SAF system and, more recently, the XP-endo system (Figure 2b,c).
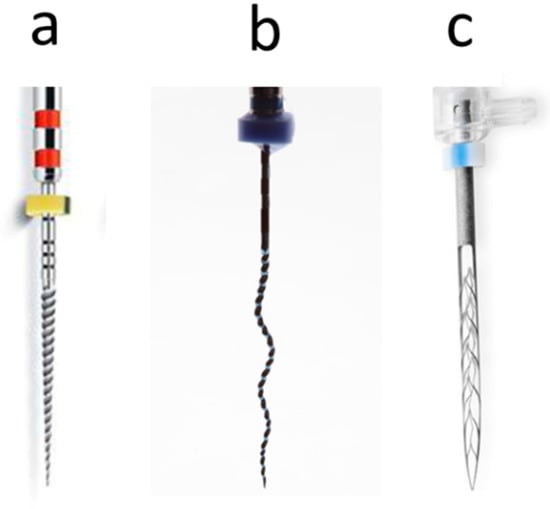
Figure 2.
Adaptive nickel-titanium mechanized instruments. (a) Traditional rotary file, which cannot adapt itself to an oval root canal. (b) XP-endo shaper with a snake like shape and motion. (c) Self-adjusting file (SAF) which can adapt its shape to an oval root canal.
The self-adjusting file (SAF) system (ReDent Nova, Ra’anana, Israel) was specifically designed to address the challenge of oval-shaped root canals. The SAF is a hollow, compressible file made of nickel-titanium (NiTi) lattice that is designed specifically to be compressed and adapt itself to the walls of root canals with any cross-section, including oval canals (Figure 3). It claims to overcome most of the constraints of motorized rotary and reciprocating nickel titanium (NiTi) files when used in oval canals [5,10,11]. The SAF is used with a pecking motion all the way to the working length, while continuous irrigation is delivered through the hollow file. Previously, the SAF was used after establishing a minimal glide path using a #20 K-file. Recently, the manufacturers have changed the guidelines for the use of the SAF system. The updated SAF sequence switched to a motorized glide path preparation, which includes the pre-SAF OS orifice shaper, (sized #40/0.10), the pre-SAF 1 for narrow canals, (sized #15/0.02), and the pre-SAF 2 (sized #20/0.04), thus, creating a glide path. Since the SAF is not a penetrating tool, the glide path should allow passive manual insertion of the 1.5-mm SAF to the working length, prior to cleaning and shaping the root canal with this instrument [3].
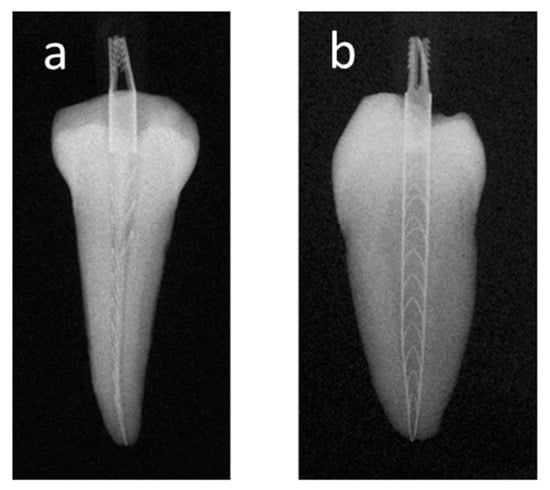
Figure 3.
Adaptation of the self-adjusting file (SAF) to an oval canal. Radiographs of a mandibular premolar with an oval canal, with the SAF adapted to an oval canal. (a) Bucco-lingual projection. (b) Mesio-distal projection.
The XP-endo system (FKG Dentaire, La Chaux-de-Fonds, Switzerland) consists of the XP-endo shaper (#30/0.01) and the XP-endo finisher (#25/0.00). The XP-endo shaper has a snake-like shape and is made of a MaxWire nickel-titanium alloy with a specific tip design (Figure 2b). The tip has a round non-active part, followed by six cutting edges that transit smoothly into the helical shaft. The file is affected by body temperature, which changes it into an austenitic phase to assume its functional shape. It is used in the root canal first as a penetrating instrument, and once reaching the working length (WL), it is used with an additional 15 pecking motion strokes to the working length [12]. The resultant final root canal size after XP-endo shaper instrumentation corresponds to #30/0.04. The XP-endo finisher file has a circular whip-shape and was initially introduced as a complementary universal instrument that can be used after root canal preparation with any file system and is aimed for cleaning complex morphologies and difficult-to-reach areas within the root canal system [1,3,13].
Recently, the manufacturers have introduced the XP-endo shaper plus sequence, which includes three stages: first, hand K-files (#10 and #15) are used to create a glide path, and then the XP-endo shaper is used, to be followed by the XP-endo finisher.
Several studies have addressed the issue of apical extrusion of debris by the SAF system [3,5,14]. It has been established that the SAF extruded less debris than rotary and reciprocating NiTi files [3,5,14]. However, it was recently suggested that the issue of apical extrusion of debris should evaluated for the full sequence of instruments of a given file system, as the initial stages of glide path preparation may contribute to the total amount of extruded debris and should not be omitted from such measurements [3,5,14].
The individual elements of the XP-endo system (XP-endo shaper, XP-endo finisher) have also been studied for their potential to extrude debris [1,3,15,16]. The XP-endo finisher, which preceded the XP-endo shaper, was also found to extrude debris when used after ProTaper Next files [3]. The more recently introduced XP-endo shaper was found in some studies to extrude less debris than Reciproc [16] or One-Shape files [15], while others have found that it extruded similar amounts of debris as Reciproc or HyFlex EDM files [1,16]. Only recently were these two instruments introduced as elements of the XP-endo shaper plus system.
A literature search revealed no studies investigating the amount of debris that may be apically extruded by the full XP-endo shaper plus sequence. Thus, the present study aimed to assess the amount of apical extrusion of debris when preparing oval root canals with either the full-sequence SAF system or the XP-endo shaper plus sequence. The null hypothesis was that the two file systems will not differ in terms of apical extrusion of debris when used in oval canals.
2. Materials and Methods
The current study was designed to quantify and compare the amount of debris extruded apically during instrumentation of oval canals in mandibular incisors using either the full-sequence SAF system (Group A: pre-SAF OS, pre-SAF 1 and pre-SAF 2 files, followed by 1.5-mm SAF), or the rotary XP-endo shaper plus sequence (Group B: hand K-file 15/0.02, followed by the XP-endo shaper and the XP-endo finisher).
2.1. Sample Selection and Preparation
The study and its design were approved by the Institutional Ethical Committee, College of Dental Science and Hospital Rau, Indore, India (CDSH/IEC/2019-2020/006).
Based on a previously conducted study [5], a power calculation was performed using G*Power 3.1 software (Heinrich Heine University, Dusseldorf, Germany). The calculation indicated that the sample size for each group must be a minimum of 30 teeth. Sixty mandibular incisor teeth were acquired from a pool of recently extracted teeth which were extracted for reasons not related to the present study. Two radiographs were taken for each tooth from bucco-lingual and mesio-distal directions to confirm a single straight root canal, a fully formed apex, no caries, no coronal restorations and no signs of resorption. In addition, only teeth with long:short canal diameter ratios of ≥2.5 at 5 mm from the apex were selected [17].
Standard oval endodontic access cavities were prepared, and a #10 K-file (Mani, Takanezawa, Japan) was introduced into the canal until it was visible at the apical foramen. The working length (WL) was established as 1 mm short of this length. For standardization of samples, the teeth with large canals, wherein a #15 k-file reached freely to the apex, were excluded. The samples were also ground coronally using a high-speed diamond straight fissure bur to further standardize all teeth to have a WL of 18 mm.
2.2. Debris Collection Apparatus
Modified apparatus of Myers and Montgomery [18], proposed by Lu et al. [19], was used in the current study for the quantitative evaluation of apically extruded debris during root canal instrumentation. To summarize the modification; 150 Eppendorf tubes were pre-weighed to 10−5 g precision using a microbalance (Sartorius Intec, Hamburg, Germany). Each tube was weighed three consecutive times, and a mean was calculated and recorded.
A hole was created in the middle of the cap of a scintillation glass vial, and the tooth was inserted, apex down, up to the cemento-enamel junction, and secured to the cap of the vial using Filtek Supreme Flowable Composite (3 M/ESPE, St Paul, MN, USA). A 25-gauge needle was also placed and secured in the vial cap to equalize the air pressure. A small holding socket was created on the bottom of the glass vial using silicon impression material (Coltene/Whaledent, Langenau, Germany), which served to hold and stabilize the Eppendorf tubes when the caps were fitted onto the vials. This was done so that the apical end of the root was positioned inside the prepositioned Eppendorf tube. The teeth with their vials were then randomly assigned to Groups A and B according to the instrumentation and debris collection protocols (see below). A Thermoline Dri-bath (Thermoline Scientific, Wetherill Park, Austria) adapted with channeled aluminum blocks (Thomas Scientific, Swedesboro, NJ, USA) was used to create a temperature-controlled environment that was adapted to 37 °C. The vials were adapted into the aluminum block and covered by a rubber dam to prevent the operator from viewing debris extrusion during tooth preparation. The entire apparatus was handled by the outer vial alone.
2.3. Root Canal Instrumentation
2.3.1. Group A: Full SAF Sequence
Stage 1: Glide Path Preparation with Pre-SAF OS and Pre-SAF Files 1 and 2
In this primary stage, a glide path was prepared according to the manufacturer’s instructions using a torque-limited electric endomotor (X-Smart Plus; Dentsply Maillefer, Ballaigues, Switzerland). The pre-SAF OS was used as an orifice shaper at 600 rpm and 1.5 Ncm for the coronal 3 mm of the root canal, which was followed by the Pre-SAF 1 (#15/0.02; 600 rpm and 1 Ncm) and pre-SAF 2 (#20/0.04; 600 rpm and 1.5 Ncm). The pre-SAFs 1 and 2 were used in 2–3 gentle pecking motions up to the WL. The canals were irrigated after each instrument with 2 mL of distilled water using a syringe and a 28-G needle (RC Twents; Prime Dental Products, Mumbai, India) with a total of 6 mL. At the end of the preparation, root canal patency was confirmed with a size 10 K-file, followed by a final flush with 2 mL of distilled water using a syringe and a 28-G needle.
Stage 2: Cleaning and Shaping with SAF 1.5 mm
The 1.5 mm SAF (21 mm length) was passively manually introduced into the canal up to the WL to test the glide path. The root canal was then instrumented for 4 min using a pre-programmed EndoStation (ReDent Nova) at a frequency of 5000 vibrations/min and an amplitude of 0.4 mm. A pecking motion was used while the file reached the WL (according to the manufacturer’s instructions). Irrigation was performed with distilled water, which was continuously provided through the hollow file by the in-built VATEA peristaltic pump (ReDent Nova), at a flow rate of 4 mL/min, with a total of 16 mL.
2.3.2. Group B: XP-Endo Shaper Plus Sequence
Stage 1: Glide Path Preparation with a #15 Hand K-File
In this stage, the root canals were initially instrumented with a #15 hand K-file up to the working length to create a glide path (according to the manufacturer’s instructions). The canals were irrigated repeatedly, before and after the instrument, with 2 mL of distilled water using a syringe and a 28-G needle.
Stage 2: Shaping with an XP-Endo Shaper
Following glide path preparation with the hand K-file, the root canals were irrigated with 4 mL of warmed distilled water (37 °C) using a syringe and 28-G needle. This allowed the XP-endo shaper (XPS; 21 mm) file to optimally work during the austenite phase. The XPS file was first placed passively until resistance was struck, the tip was then retracted, and the endomotor was activated. The XPS file was used at 800 rpm and 1 Ncm using a torque-limited electric endomotor (X-Smart Plus). The file was used in long gentle strokes 4–5 times towards the WL (according to the manufacturer’s instructions). If the file failed to reach the WL, the file was withdrawn and cleaned, the apical patency confirmed with a 15 k-file, the canal was irrigated using warm distilled water (2 mL), and the file was reintroduced in the canal and advanced further up to the WL. Once the WL was reached, the file was retracted, cleaned, apical patency was verified, the canal was flooded with warm distilled water (2 mL), and the file was used again for an additional 15 strokes up to the WL (according to the manufacturer’s instructions).
Stage 3: Cleaning with XP-Endo Finisher
Following root canal instrumentation with XPS, the root canal was flooded with warm distilled water (2 mL), the XP-endo finisher (XPF; 21 mm) was removed from its special plastic tube and the rubber stopper was adjusted to WL, and the file was operated at 800 rpm and 1 Ncm using an X-smart plus endomotor. The XPF was inserted to WL, the canal access cavity was filled with warmed distilled water, and the instrument was operated in the canal for 60 s using gentle 7- to 8-mm-long in-and-out strokes (according to the manufacturer’s instructions). This was followed by a final flush with 2 mL of distilled water.
2.4. Debris Collection
Following each stage, the Eppendorf tube was removed from the vial and replaced with a new one. The debris adhering to the apical root surface was collected by washing the root surface with 1 mL of distilled water into the Eppendorf tube. A new Eppendorf tube was assigned to each tooth and each instrumentation stage. This process resulted in 60 tubes for Group A (2 stages) and 90 tubes for Group B (3 stages). The Eppendorf tubes were then stored in an incubator at 70 °C for 5 days to evaporate all moisture content before weighing the dry debris. Three consecutive weights were obtained for each tube, and the mean value was calculated and recorded. The weight of the dried debris was calculated by subtracting the weight of the empty tube from the weight of the tube containing the debris.
2.5. Statistical Analysis
The weights presented a normal distribution corroborated using the D’Agostino-Pearson normality test. The amounts of extruded debris collected at each stage of Groups A and B were summed to provide the total amount of debris. The weights of extruded debris in the two groups were analyzed by applying the t test, whereas the stages within the groups were compared using a paired t test. The level of significance for statistical analysis was set at 5%. All statistical analyses were performed with Statistical Package for the Social Sciences version 20 for Mac (SPSS Inc., Chicago, IL, USA).
3. Results
In Group A (full-sequence SAF instrumentation), the mean weights of the debris extruded apically were 0.568 ± 0.434 mg in Stage 1 (pre-SAF OS, pre-SAF 1, and 2) and 0.471 ± 0.267 mg in Stage 2 (SAF 1.5 mm). The amount of debris extruded apically by the 2 stages did not exhibit a significant difference between them (p = 0.3014) (Figure 4).
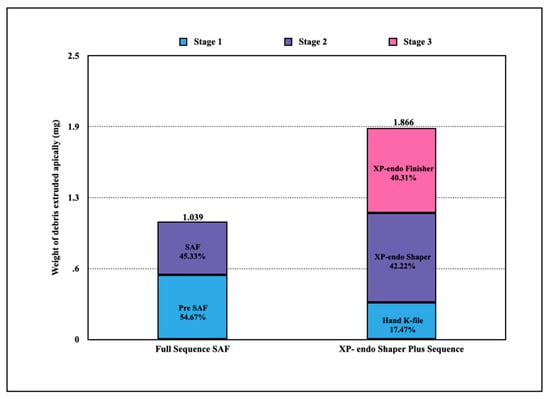
Figure 4.
Apical extrusion of debris by a full-sequence SAF system vs. XP-endo shaper plus sequence. The total debris extrusion of Group B was significantly higher than that of Group A (p < 0.001).
In Group B (XP-endo shaper plus sequence), the mean weights of the debris extruded apically were 0.326 ± 0.077 mg in Stage 1 (hand K-file), 0.788 ± 0.203 mg in Stage 2 (XPS), and 0.752 ± 0.197 in Stage 3 (XPF). The amount of debris extruded apically by the 3 stages exhibited a significant difference between them (p < 0.01) (Figure 4). Similar weights of debris were extruded in Stages 2 and 3 (p = 0.488).
The total amount of debris extruded in Group A was significantly less (1.039 ± 0.185 mg) compared to Group B (1.866 ± 0.289 mg) (p < 0.001). Distribution of the results is presented in Table 1.

Table 1.
Weight of apically extruded debris (mg). Data distribution.
4. Discussion
The current ex vivo study was conducted to quantify and compare the amount of debris extrusion that was caused during cleaning and shaping of oval-shaped root canals using two different instrumentation systems specifically designed to perform in non-round root canals: the full sequence SAF and the XP-endo shaper plus sequence.
Both instruments are made from NiTi alloy, but each using different characteristics of this unique alloy. The SAF is made from a NiTi tube which is cut to the form of a delicate lattice, with a special design that allows the instrument to be compressed from its 1.5 mm diameter to the dimensions of a #20 K file. This ability is based on the design of the lattice, combined with the high flexibility of the alloy and allows the file to adapt itself to any shape of root canal (Figure 3). It is used with pecking motion and with every inward move it goes through such compression (above) and back to its original form when moved outwards. The XP-endo shaper and finisher both use the extreme flexibility of the NiTi alloy, which in their case is formed as a wire, but they also use the thermal transformation which is unique to this alloy. These files have a more straight form at room temperature but when inserted into the canal and attaining body temperature their form changes, enhancing their envelope of motion when rotated, which allows them to enter and shape/clean irregular recesses of the root canal, such as the oval canals that were used in the present study.
Evidence indicates that with any file system, dentine particles and other debris can often be packed into the apical anatomical complexities and pushed beyond the apex with/by the attempts to reach the WL [3,14]. Both instrumentation sequences that were tested in the present study did push debris beyond the apical foramen.
Apical extrusion of debris by the full SAF sequence has been recently reported and was found to be less than that extruded by ProTaper Next, followed by XP-endo finisher [3]. To the best of the authors’ combined knowledge, the debris extrusion by the XP-endo shaper plus sequence is yet to be reported in the literature. In the present study, the full-sequence SAF exhibited significantly less debris extrusion compared to the XP-endo shaper plus sequence (p < 0.001). Thus, the null hypothesis had to be rejected.
When the SAF alone was previously compared with WaveOne as to their pushing of debris beyond the apex [14], glide path preparation was performed in both groups with #20 hand K files. Nevertheless, debris extrusion during this first stage of instrumentation was not recorded and not reported [14]. The present study took an approach similar to that of Kfir et al. [3], who reported that the contribution of the initial stage of glide path preparation to the total amount of debris extruded during the procedure may be substantial. The present results are in agreement and support this notion: the glide path preparation stage contributed 55% of the debris extrusion in the SAF group [3,11]. When the same concept was applied in the XP-endo shaper plus group, it was found that each part of the procedure contributed its share to the total extrusion of debris. The XP-endo shaper and the XP-endo finisher contributed 42% and 40% of the total amount of debris, respectively.
Both the SAF and XP-endo systems could be expected to cause debris extrusion, as both the SAF and the XP-endo shaper and finisher are used with repeated pecking motions once/after they have reached the working length. This approach is substantially different from rotary or reciprocating file systems, in which once the WL is reached, the procedure is done. Both systems have another common apparent problem: a potential difficulty to assure accurate working length. The SAF system is using in-and-out vibrations with an amplitude of 0.4 mm, which, when added to the pecking motion applied by the operator, may compromise the accuracy of the working length.
Both the XP-endo shaper, with its snake-like form, and the XP-endo finisher, with its whip-shape, may become shorter or longer when expansion and contraction occur when they are rotated, with a pecking motion, in the canal. Such inaccuracy in controlling the instruments at exactly the working length may have contributed to the finding that both systems extruded measurable amounts of debris beyond the apical foramen.
What could be the difference between the two file systems studied here that might explain the difference in their extrusion of debris? One such difference could be the cross-section of the apical part of the file. The guiding non-active part of the tip of the XP-endo shaper has a round cross-section, while the tip of the SAF has a rectangular cross-section [10,20]. The operator of the XP-endo shaper is directed by the manufacturer to perform 15 pecking motion strokes to the WL [12]. When the round guiding tip of the XP-endo shaper is moved in-and-out within the round apical part of the canal, it may act as a piston, pushing and extruding debris through the apical foramen. When the tip of the SAF is compressed into the round apical part of the canal with a 0.2-mm diameter, which was prepared during glide path preparation, it assumes a rectangular cross-section of 0.12 × 0.16 mm (two layers of its longitudinal beams, each with a cross-section of 0.12 mm by 0.8 mm) [10,20]. This rectangular part is changing its circular position continuously, thus maintaining the apical part of the canal in its round cross-section. When this rectangular tip of the file is moving in-and-out in the circular apical part of the canal, it does not act as a piston, as 40% of the cross-section of the canal is always free for back flow [10,20]. This difference may partially explain the difference in extrusion of debris.
Another difference between the two file systems is that the XP-endo shaper plus sequence is used with intermittent irrigation, using syringe and needle between file applications. In contrast, in the SAF system, irrigation is continuous, as the irrigant is delivered into the root canal through the hollow file throughout the operation. It could be that such continuous irrigation, which carries the debris coronally and out of the canal, better prevents the accumulation of debris, thus reducing the tendency to push such accumulated debris through the apical foramen.
A limitation of the present study was that there was no element representing the resistance of the periapical tissues to extrusion of debris. Uslu et al. [16] used 1.5% agar gel for such representation, but in such a method, only the total amount of extruded debris can be quantified. Since the present study was aimed to analyze the contribution of each stage of instrumentation to the amount of extruded debris, such a system was not applicable. Therefore, the present results may have to be considered as comparative values between the two systems, rather than as absolute amounts of debris.
Further studies are required to find ways and methods of instrumentation that will prevent or minimize the extrusion of debris during root canal instrumentation, but such studies should include all steps of the procedure, including initial glide path preparation.
5. Conclusions
Within the limitations of the current study, the following conclusions may be drawn:
- Both instrumentation sequences resulted in apical extrusion of debris from oval-shaped root canals of mandibular incisors.
- Each of the different stages of root canal instrumentations made their own contribution to debris extrusion.
- The XP-endo shaper plus sequence extruded significantly more debris than the full SAF sequence.
Author Contributions
Conceptualization, A.M.P., A.K. and A.B.; methodology, A.M.P. and A.K.; formal analysis, A.M.L.; investigation, A.M.P., B.A.P.; data curation, A.M.P. and B.A.P.; writing—original draft preparation, A.M.P. and A.K.; writing—review and editing, Z.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
The authors deny any conflicts of interest related to this study. Zvi Metzger served previously as a scientific consultant to ReDent Nova, manufacturer of the SAF system.
Conflicts of Interest
The authors declare no conflict of interest. Metzger was previously a scientific consultant to ReDent-Nova, manufacturer of the SAF system.
References
- Alves, F.-R.F.; Paiva, P.-L.; Marceliano-Alves, M.-F.; Cabreira, L.-J.; Lima, C.; Siqueira, J.-F., Jr.; Rôças, I.-N.; Provenzano, J.-C. Bacteria and hard tissue debris extrusion and intracanal bacterial reduction promoted by XP-endo Shaper and Reciproc instruments. J. Endod. 2003, 44, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.-F., Jr. Microbial causes of endodontic flare-ups. Int. Endod. J. 2003, 36, 453–463. [Google Scholar] [CrossRef] [PubMed]
- Kfir, A.; Moza-Levi, R.; Herteanu, M.; Weissman, A.; Wigler, R. Apical extrusion of debris during the preparation of oval root canals: A comparative study between a full-sequence SAF system and a rotary file system supplemented by XP-endo finisher file. Clin. Oral Investig. 2018, 22, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Metzger, Z. The self-adjusting file (SAF) system: An evidence-based update. J. Conserv. Dent. 2014, 17, 401–419. [Google Scholar] [CrossRef] [PubMed]
- Pawar, A.-M.; Pawar, M.-G.; Metzger, Z.; Kokate, S.-R. The self-adjusting file instrumentation results in less debris extrusion apically when compared to WaveOne and ProTaper NEXT. J. Conserv. Dent. 2015, 18, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Tanalp, J.; Güngör, T. Apical extrusion of debris: A literature review of an inherent occurrence during root canal treatment. Int. Endod. J. 2014, 47, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Tinoco, J.-M.; De Deus, G.; Tinoco, E.-M.; Saavedra, F.; Fidel, R.-A.; Sassone, L.-M. Apical extrusion of bacteria when using reciprocating single-file and rotary multifile instrumentation systems. Int. Endod. J. 2014, 47, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.-K.; Wesselink, P.-R. A primary observation on the preparation and obturation of oval canals. Int. Endod. J. 2001, 34, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Weiger, R.; El Aouti, A.; Löst, C. Efficiency of hand and rotary instruments in shaping oval root canals. J. Endod. 2002, 28, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Metzger, Z.; Teperovich, E.; Zary, R.; Cohen, R.; Holf, R. The Self-adjusting File (SAF). Part 1: Respecting the root canal anatomy-A new concept of endodontic files and its implementation. J. Endod. 2010, 36, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Pawar, A.-M.; Pawar, M.; Kfir, A.; Thakur, B.; Mutha, P.; Banga, K.-S. Effect of glide path preparation on apical extrusion of debris in root canals instrumented with three single-file systems: An ex vivo comparative study. J. Conserv. Dent. 2017, 20, 110–114. [Google Scholar] [CrossRef] [PubMed]
- De Deus, G.; Belladonna, -F.G.; Simões-Carvalho, M.; Cavalcante, D.-M.; Ramalho, C.-N.-M.-J.; Souza, E.-M.; Lopes, R.-T.; Silva, E.-J.-N.-L. Shaping efficiency as a function of time of a new heat-treated instrument. Int. Endod. J. 2019, 52, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Alves, F.-R.; Marceliano-Alves, M.-F.; Sousa, J.-C.; Silveira, S.-B.; Provenzano, J.-C.; Siqueira, J.-F., Jr. Removal of root canal fillings in curved canals using either reciprocating single- or rotary multiinstrument systems and a supplementary step with the XP-Endo Finisher. J. Endod. 2016, 42, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Farmakis, E.-T.; Sotiropoulos, G.-G.; Abràmovitz, I.; Solomonov, M. Apical debris extrusion associated with oval shaped canals: A comparative study of WaveOne vs. Self-Adjusting File. Clin. Oral Investig. 2016, 20, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Savadkouhi, S.; Esnaashari, E.; SHahzaidi, A.; Fazlyab, M.; Moshari, A. Comparison of debris extrusion in XP-endo-Shaper and One-Shape rotary systems: In vitro study. J. Res. Dent. Sci. 2018, 15, 93–98. [Google Scholar] [CrossRef]
- Uslu, G.; Özyürek, T.; Yılmaz, K.; Gündoğar, M.; Plotino, G. Apically extruded debris during root canal instrumentation with Reciproc blue, HyFlex EDM, and XP-endo shaper nickel-titanium files. J. Endod. 2018, 44, 856–859. [Google Scholar] [CrossRef] [PubMed]
- DeDeus, G.; Reis, C.; Beznos, D.; de Abranches, A.-M.; Coutinho-Filho, T.; Paciornik, S. Limited ability of three commonly used thermoplasticized gutta-percha techniques in filling oval-shaped canals. J. Endod. 2008, 34, 140–145. [Google Scholar]
- Myers, G.-L.; Montgomery, S. A comparison of weights of debris extruded apically by conventional filing and Canal Master techniques. J. Endod. 1991, 17, 275–279. [Google Scholar] [CrossRef]
- Lu, Y.; Wang, R.; Zhang, L.; Li, H.-L.; Zheng, Q.-H.; Zhou, X.-D.; Huang, D.-M. Apically extruded debris and irrigant with two Ni-Ti systems and hand files when removing root fillings: A laboratory study. Int. Endod. J. 2013, 46, 1125–1130. [Google Scholar] [CrossRef]
- Hof, R.; Perevalov, V.; Eltanani, M.; Zary, R.; Metzger, Z. The self-adjusting file (SAF). Part 2: Mechanical analysis. J. Endod. 2010, 36, 691–696. [Google Scholar] [CrossRef] [PubMed]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).