Effect of Surface Treatment and Storage Time on Immediate Repair Bond Strength Durability of Methacrylate- and Ormocer-Based Bulk Fill Resin Composites



Abstract
:1. Introduction
2. Materials and Methods
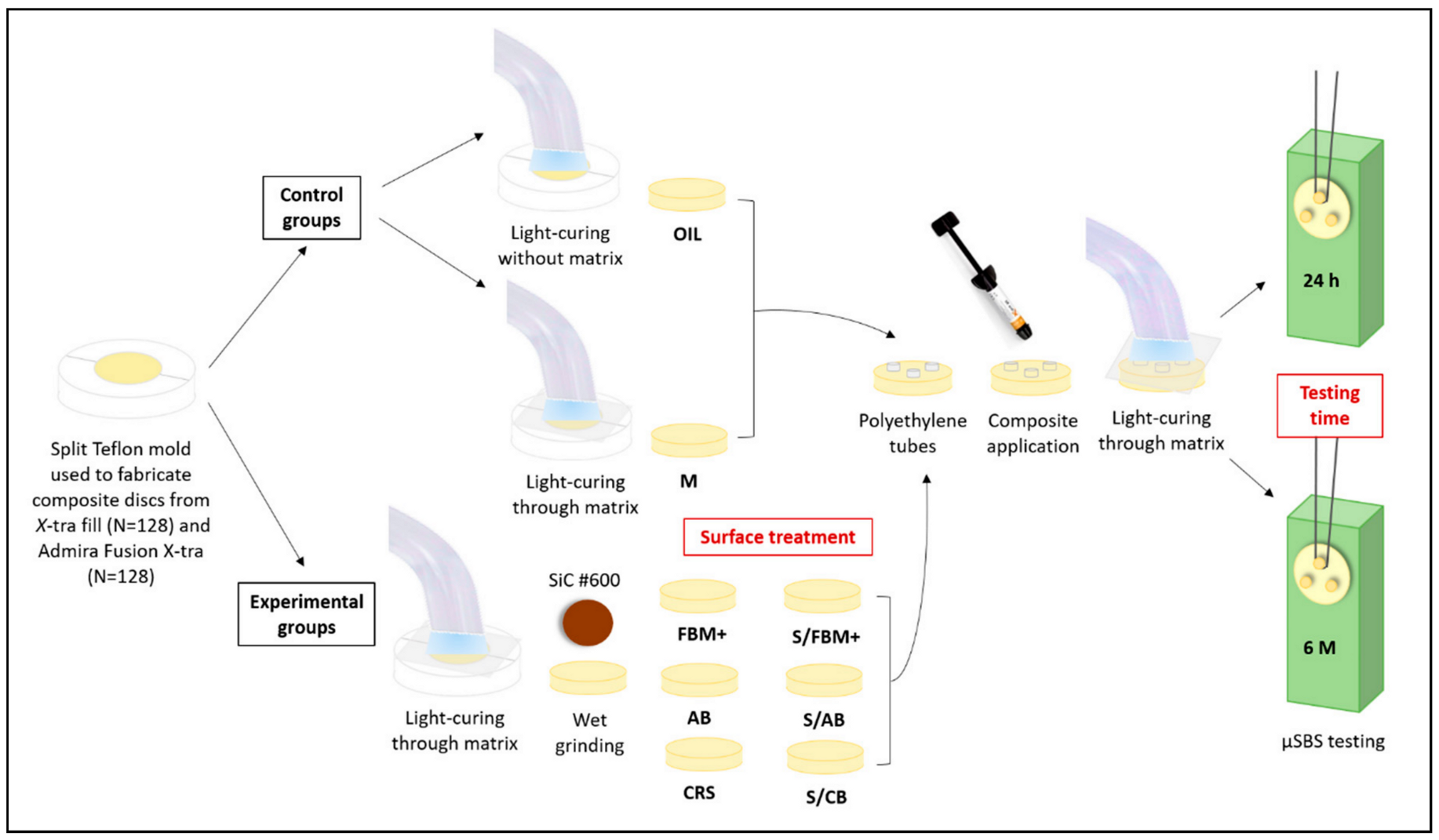
2.1. Study Design
2.2. Specimens Preparation and Surface Treatments
- 1.
- Oxygen-inhibited layer (OIL, n = 32 discs): In this group, a piece of Teflon tape was placed over the resin composite disc and gently pressed with a glass slide to extrude excess material and create a smooth flat surface. The glass slide and the Teflon tape were removed, and the material was photo-polymerized in contact with air for 10 s and 20 s (X-tra fil and Admira Fusion X-tra, respectively), following the manufacturer’s instructions, using LED photo-polymerization unit (Elipar, 3M ESPE, Seefeld, Germany; light output: 1200 mW/cm2). The discs were removed from the mold and no further surface treatments were performed. These discs were used to test the cohesive strength of each material (positive control).
- 2.
- Matrix (M, n = 32 discs): After the material was packed inside the mold, a piece of polyester strip was placed on the top of the resin composite and gently pressed with a glass slide as described for OIL. The glass slide was then removed and the material was photo-polymerized using the LED photo-polymerization unit for 10 s and 20 s (X-tra fil and Admira Fusion X-tra, respectively), following the manufacturer’s instructions. The discs were removed from the mold and no further surface treatments were performed. These discs served as negative control group.
- 3.
- Futurabond M+ adhesive (FBM+): The adhesive was applied with a microbrush (Single Tim, VOCO) and rubbed over the surface for 20 s, air-dried for 5 s and photo-polymerization for 10 s according to the manufacturer’s instructions.
- 4.
- Silane/Futurabond M+ adhesive (S/FBM+): Silane was applied with a microbrush and left to react for 2 min. The silane was not air-dried according to manufacturer’s instructions. The adhesive was applied and rubbed for 20 s, air-dried for 5 s, and photo-polymerized for 10 s.
- 5.
- Admira Bond (AB): Each disc was etched using 34.5% phosphoric acid etchant gel for 15 s, rinsed for 20 s and air-dried for 10 s. Adhesive was applied to disc surface using a microbrush and left undisturbed for 30 s. The adhesive was gently air-dried for 5 s and photo-polymerized for 10 s according to the manufacturer’s instructions.
- 6.
- Silane/Admira Bond (S/AB): Silane was applied and left to react for 2 min and no air dryness was performed. Admira Bond was applied for 30 s, air-dried for 5 s and photo-polymerized for 10 s.
- 7.
- Ceramic Repair System (CRS): Each composite disc was conditioned using a silicon carbide (SiC) grinding bur supplied by the manufacturer (Cimara bur, VOCO), in one direction for 5 s [20]. The bur rotated at 10,000 rpm using a slow speed handpiece (Sirona, T2 Revo-R 40, Sirona Dental System, Bensheim, Germany) mounted on electrically-controlled motor. The conditioned surface was thoroughly cleaned using gentle compressed air. Silane was applied and left to react for 2 min. Cimara adhesive was applied using a micro-brush, distributed over the surface using a gentle stream of air. The adhesive was left undisturbed for 20 s and photo-polymerization for 20 s according to manufacturer’s instructions.
- 8.
- Silane/Cimara Bond (S/CB): Silane was applied over the surface and left to react for 2 min, but no air dryness was performed. Adhesive was applied, gently distributed over the surface, left undisturbed for 20 s and photo-polymerized for 20 s.
2.3. Application of Repair Material
2.4. Micro-Shear Bond Strength (µSBS) Testing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- Immediate repair bond strength of methacrylate-based resin composite was superior to ormocer-based composite.
- Ceramic repair system can successfully repair both methacrylate- and ormocer-based resin composites.
- The use of universal adhesive with methacrylate-based composite and ormocer-based adhesive with ormocer-based composite showed promising results.
- Silane application before universal adhesive, improved the immediate repair bond strength of ormocer-based composite, with no effect on methacrylate-based one.
- Adhesive/resin composite matrix compatibility should be considered during immediate repair of resin composites with different resin matrix.
- None of the bonding protocols succeeded to maintain the repair bond strength after six months of storage, except for ormocer-based composite treated with silane/Cimara adhesive.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Watts, D. The quest for stable biomimetic repair of teeth: Technology of resin-bonded Composites. Dent. Mater. J. 2020, 39, 46–51. [Google Scholar]
- Van Meerbeek, B.; Yoshihara, K.; Yoshida, Y.; Mine, A.; De Munck, J.; Van Landuyt, K. State of the art of self-etch adhesives. Dent. Mater. 2011, 27, 17–28. [Google Scholar] [PubMed]
- Moorthy, A.; Hogg, C.H.; Dowling, A.H.; Grufferty, B.F.; Benetti, A.R.; Fleming, G.J.P. Cuspal deflection and microleakage in premolar teeth restored with bulk-fill flowable resin-based composite base materials. J. Dent. 2012, 40, 500–505. [Google Scholar] [PubMed]
- Fleming, G.J.P.; Awan, M.; Cooper, P.R.; Sloan, A.J. The potential of a resin-based composite to be cured to a 4 mm depth. Dent. Mater. 2008, 24, 522–529. [Google Scholar] [PubMed]
- Gerula-Szymańska, A.; Kaczor, K.; Lewusz-Butkiewicz, K.; Nowicka, A. Marginal integrity of flowable and packable bulk fill materials used for class II restorations-A systematic review and meta-analysis of in vitro studies. Dent. Mater. J. 2020, 39, 335–344. [Google Scholar]
- Lewis, G.; Johanson, W.; Martin, W.; Canerdy, A.; Claburn, M. Shear bond strength of immediately repaired light-cured composite resin restorations. Oper. Dent. 1998, 23, 121–127. [Google Scholar] [PubMed]
- Hickel, R.; Brüshaver, K.; Ilie, N. Repair of restorations—Criteria for decision making and clinical recommendations. Dent. Mater. 2013, 29, 28–50. [Google Scholar]
- Fawzy, A.; El-Askary, F.; Amer, M. Effect of surface treatments on the tensile bond strength of repaired water-aged anterior restorative micro-fine hybrid resin composite. J. Dent. 2008, 36, 969–976. [Google Scholar]
- Hisamatsu, N.; Atsuta, M.; Matsumura, H. Effect of Silane Primers and Unfilled Resin Bonding Agents on Repair Bond Strength of a Prosthodontic Microfilled Composite. J. Oral Rehab. 2002, 29, 644–648. [Google Scholar]
- Özcan, M.; Barbosa, S.; Melo, R.; Galhano, G.; Bottino, M. Effect of Surface Conditioning Methods on the Microtensile Bond Strength of Resin Composite to Composite After Aging Conditions. Dent. Mater. 2007, 23, 1276–1282. [Google Scholar]
- Shahadad, S.; Kennedy, J. Bond Strength of Repaired Anterior Composite Resins: An in Vitro Study. J. Dent. 1989, 26, 685–694. [Google Scholar]
- Ghavam, M.; Naeemi, M.; Hashemikamangar, S.; Ebrahimi, H.; Kharazifard, M. Repair bond strength of composite: Effect of surface treatment and type of composite. J. Clin. Exp. Dent. 2018, 10, e520–e527. [Google Scholar] [PubMed]
- Altinci, P.; Mutluay, M.; Tezvergil-Mutluay, A. Repair bond strength of nanohybrid composite resins with a universal adhesive. Acta Biomater. Odontol. Scand. 2018, 4, 10–19. [Google Scholar] [PubMed] [Green Version]
- Irmak, Ö.; Çeliksöz, Ö.; Begüm Yilmaz, B.; Yaman, B. Adhesive system affects repair bond strength of resin composite. J. Istanb. Univ. Fac. Dent. 2017, 51, 25–31. [Google Scholar] [PubMed] [Green Version]
- Kiomarsi, N.; Espahbodi, M.; Chiniforush, N.; Karazifard, M.; Kamangar, S. Invitro evaluation of repair bond strength of composite: Effect of surface treatments with bur and laser and application of universal adhesive. Laser Ther. 2017, 26, 173–180. [Google Scholar] [PubMed] [Green Version]
- Kiomarsi, N.; Saburian, P.; Chiniforush, N.; Karazifard, M.; Hashemikamangar, S. Effect of thermocycling and surface treatment on repair bond strength of composite. J. Clin. Exp. Dent. 2017, 9, e945–e951. [Google Scholar] [PubMed]
- Eliasson, S.; Dahl, J. Effect of curing and silanizing on composite repair bond strength using an improved micro-tensile test method. Acta Biomater. Odontol. Scand. 2017, 3, 21–29. [Google Scholar] [PubMed]
- El-Askary, F.; Fawzy, A.; Abd Elmohsen, H. Tensile Bond Strength of Immediately Repaired Anterior Microfine Hybrid Restorative Composite Using Nontrimmed Hourglass Specimens. J. Adhes. Dent. 2009, 11, 41–47. [Google Scholar] [PubMed]
- El-Askary, F.; El-Banna, A.; van Noort, R. Immediate versus delayed repair bond strength of a nano-hybrid resin composite. J. Adhes. Dent. 2012, 14, 265–274. [Google Scholar]
- Rinastiti, M.; Özcan, M.; Siswomihardjo, W.; Busscher, H. Immediate repair bond strengths of microhybrid, nanohybrid and nanofilled composites after different surface treatments. J. Dent. 2010, 38, 29–38. [Google Scholar]
- El-Askary, F.; Salah, M.; Anwar, M.; Özcan, M. Immediate and delayed repair bond strength of a new ormocer restorative material as a function of mechanical and chemical surface conditioning methods. J. Adhes. Sci. Technol. 2017, 31, 310–326. [Google Scholar]
- Loomans, B.; Cardoso, M.; Roeters, F.; Opdam, N.; De Munck, J.; Huysmans, M.; Van Meerbeek, B. Is there one optimal repair technique for all composites? Dent. Mater. 2011, 27, 701–709. [Google Scholar] [PubMed]
- Kanzow, P.; Wiegand, A.; Schwendicke, F.; Gostemeyer, G. Same, same, but different? A systematic review of protocols for restoration repair. J. Dent. 2019, 86, 1–16. [Google Scholar] [PubMed]
- Atalay, C.; Yazici, A.; Ozgunaltay, G. Bond strengths of bulk-fill resin composite repairs: Effect of different surface treatment protocols in vitro. J. Adhes. Sci. Technol. 2018, 32, 921–930. [Google Scholar]
- Oglakci, B.; Arhun, N. The shear bond strength of repaired high-viscosity bulk-fill resin composites with different adhesive systems and resin composite types. J. Adhes. Sci Technol. 2019, 33, 1584–1597. [Google Scholar]
- Şişmanglu, S.; Gürcan, A.; Yildirim-Bilmez, Z.; Gümüşta, B. Efficacy of different surface treatments and universal adhesives on the microtensile bond strength of bulk-fill composite repair. J. Adhes. Sci. Technol. 2020, 34, 1115–1127. [Google Scholar]
- Ayar, M.; Guven, M.; Burduroglu, H. Repair of aged bulk-fill composite with posterior composite: Effect of different surface treatments. J. Esthet. Restor. Dent. 2019, 31, 246–252. [Google Scholar]
- Cuevas-Suárez, C.; Nakanishi, L.; Isolan, C.; Ribeiro, J.; Moreira, G.; Piva, E. Repair bond strength of bulk-fill resin composite: Effect of different adhesive protocols. Dent. Mater. J. 2020, 39, 236–241. [Google Scholar]
- Eltahlah, D.; Lynch, C.; Chadwick, B.; Blum, I.; Wilson, N. An update on the reasons for placement and replacement of direct restorations. J. Dent. 2018, 72, 1–7. [Google Scholar]
- Gordan, V.; Mondragon, E.; Shen, C. Replacement of resin-based composite: Evaluation of cavity design, cavity depth, and shade matching. Quintessence Int. 2002, 33, 273–278. [Google Scholar]
- Rinastiti, M.; Ozcan, M.; Siswomihardjo, W.; Busscher, H.J. Effects of surface conditioning on repair bond strengths of non-aged and aged microhybrid, nanohybrid, and nanofilled composite resins. Clin. Oral Investig. 2011, 15, 625–633. [Google Scholar] [PubMed] [Green Version]
- Shawkat, E.; Shortall, A.; Addison, O.; Palin, W. Oxygen inhibition and incremental layer bond strengths of resin composites. Dent. Mater. 2009, 25, 1338–1346. [Google Scholar] [PubMed]
- Al-Ahdal, k.; Iliec, N.; Silikas, N.; Watts, D. Polymerization kinetics and impact of postpolymerization on the Degree of Conversion of bulk-fill resin-composite at clinically relevant depth. Dent. Mater. 2015, 31, 1207–1213. [Google Scholar]
- Eliades, G.; Caputo, A. The strength of layering technique in visible light-cured composites. J. Prosthet. Dent. 1989, 61, 31–38. [Google Scholar] [PubMed]
- Ilie, N.; Stawarczyk, B. Efficiency of different repair kits on bonding to aged dental resin composite substrates. Inter. J. Adhes. Adhes. 2015, 58, 7–12. [Google Scholar]
- Boyer, D.; Chan, K.; Rinhardet, J. Build-up and Repair of Light-cured Composites: Bond Strength. J. Dent. Res. 1984, 63, 1241–1244. [Google Scholar]
- Azarbal, P.; Boyer, D.; Chan, K. The effect of bonding agents on the interfacial bond strength of repaired composites. Dent. Mater. 1986, 2, 135–155. [Google Scholar]
- Kao, E.; Pryor, H.; Johnston, W. Strength of composites repaired by laminating with dissimilar composites. J. Prosthet. Dent. 1988, 60, 328–333. [Google Scholar]
- Ilie, N. Impact of light transmittance mode on polymerisation kinetics in bulk-fill resin-based composites. J. Dent. 2017, 63, 51–59. [Google Scholar]
- Tarle, Z.; Attin, T.; Marovic, D.; Andermatt, L.; Ristic, M.; Tauböck, T. Influence of irradiation time on subsurface degree of conversion and microhardness of high-viscosity bulk-fill resin composites. Clin. Oral Investig. 2015, 19, 831–840. [Google Scholar]
- Ozcan, M.; Matinlinna, J.; Vallittu, P.; Huysmans, M. Effect of drying time of 3-mathacryloxypropyltrimethoxy silane on the shear bond strength of a composite resin to silica-coated base/noble alloys. Dent. Mater. 2004, 20, 586–590. [Google Scholar]
- Aquino, C.; Mathias, C.; Barreto, S.; Cavalcanti, A.; Marchi, G.; Mathias, P. Repair Bond Strength and Leakage of Non-Aged and Aged Bulk-fill Composite. Oral Health Prev. Dent. 2020, 18, 783–791. [Google Scholar]
- Van Landuyt, K.L.; Snauwaert, J.; De Munck, J.; Peumans, M.; Yoshida, Y.; Poitevin, A.; Coutinho, E.; Suzuki, K.; Lambrechts, P.; Van Meerbeek, B. Systematic review of the chemical composition of contemporary dental adhesives. Biomaterials 2007, 28, 3757–3785. [Google Scholar]
- Park, S.; Jin, J. Effect of Silane Coupling Agent on Interphase and Performance of Glass Fibers/Unsaturated Polyester Composites. J. Colloid Interface Sci. 2001, 242, 174–179. [Google Scholar]
- Della Bona, A.; van Noort, R. Shear vs. Tensile Bond Strength of Resin Composite Bonded to Ceramic. J. Dent. Res. 1995, 74, 1591–1596. [Google Scholar] [PubMed]
- Karacolak, G.; Turkun, S.; Boyacioglu, H.; Ferracane, J. Influence of increment thickness on radiant energy and microhardness of bulk fill resin composites. Dent. Mater. 2018, 37, 206–213. [Google Scholar]
- Rizzante, F.; Duque, J.; Duarte, M.; Mondelli, R.; Mendonça, G.; Ishikiriama, S. Polymerization shrinkage, microhardness and depth of cure of bulk fill resin Composites. Dent. Mater. J. 2019, 38, 403–410. [Google Scholar] [PubMed] [Green Version]
- Xavier, T.; Meira, J.; Rodrigues, F.; Lima, R.; Ballester, R. Finite element analysis of shear versus torsion adhesive strength tests for dental resin composites. J. Adhes. Sci. Technol. 2009, 23, 1575–1589. [Google Scholar]
- Braz, R.; Sinhoreti, M.; Spazzin, A.; Loretto, S.; Lyra, A.; Meira-Júnior, A. Shear bond strength test using different loading conditions—A finite element analysis. Br. J. Oral Sci. 2010, 9, 439–442. [Google Scholar]
- Malacarne, J.; Carvahlo, R.; De Goes, M.; Svizero, N.; Pashley, D.; Tay, F.; Yiu, C.; Carrilho, M. Water sorption/solubility of dental adhesive resins. Dent. Mater. 2006, 22, 973–980. [Google Scholar]
- Tay, F.; Pashley, D. Have dentin adhesives become too hydrophilic? J. Can. Dent. Assoc. 2003, 96, 726–731. [Google Scholar]
- Blum, I.; Schriever, A.; Heidemann, D.; Mjör, I.; Wilson, N. Repair versus replacement of defective direct composite restorations in teaching programmes in United Kingdom and Irish dental schools. Eur. J. Prosthodont. Restor. Dent. 2002, 10, 151–155. [Google Scholar] [PubMed]
- Brunton, P.; Ghazali, A.; Tarif, Z.; Loch, C.; Lynch, C.; Wilson, N.; Blum, I. Repair vs replacement of direct composite restorations: A survey of teaching and operative techniques in Oceania. J. Dent. 2017, 59, 62–67. [Google Scholar] [PubMed]
- Kanzow, P.; Wiegand, A.; Wilson, N.; Lynch, C.; Blum, I. Contemporary teaching of restoration repair at dental schools in Germany-Close to universality and consistency. J. Dent. 2018, 75, 121–124. [Google Scholar]


{kind=link}
| Material (Description) | Composition (Batch #) | Manufacturer |
|---|---|---|
| X-tra fil (micro-hybrid bulk-fill resin composite) | Bis-GMA, UDMA, TEGDMA, silicate glass. Filler content: 86 wt% (1533445) | VOCO GmbH, Cuxhaven, Germany |
| Admira Fusion x-tra (ormocer-based bulk-fill resin composite) | Ormocer resin, silicon oxide fillers and glass fillers. Filler content: 84 wt% (1509036) | VOCO GmbH |
| Futurabond M+ (universal adhesive) | Dimethacrylates, fumed silica, acid-modified methacrylates, CQ, BHT, amine, ethanol, water (1428143) | VOCO GmbH |
| Admira Bond (ormocer-based etch-and-rinse adhesive) | Acid-etching gel: 34.5% phosphoric acid-etching gel (1411479) Bond: ormocer resin, dimethacrylates, HEMA, NaF, acid-modified methacrylates, CQ, BHT, acetone (1421529) | VOCO GmbH |
| Cimara (ceramic repair system) | SiC bur: SiC grinding low-speed bur Adhesive: dimethacrylates, carbon acid-modified dimethacrylates, CQ, BHT, Amine, acetone (1414216) Silane: Reactive silane, isopropanol, acetone, amine (1415052) | VOCO GmbH |
| 24 h | 6 Months | Percentage Drop | p-Value | |
|---|---|---|---|---|
| OIL | 21.5 ± 4.8 bcA | 16.2 ± 1.9 bB | 24.65% | 0.011 |
| M | 28.3 ± 4.3 aA | 10.9 ± 2.8 cB | 61.48% | <0.001 |
| FBM+ | 25.1 ± 3.6 abcA | 17.3 ± 2.1 abB | 31.07% | <0.001 |
| S/FBM+ | 27.4 ± 5.0 abA | 21.2 ± 2.9 aB | 22.63% | 0.009 |
| AB | 14.1± 2.2 dA | 10.4 ± 2.2 cB | 26.24% | 0.004 |
| S/AB | 19.3 ± 4.1 cdA | 15.3 ± 2.1 bB | 20.73% | 0.035 |
| CRS | 26.3 ± 5.1 abA | 20.5 ± 3.5 aB | 22.05% | 0.020 |
| S/CB | 25.2 ± 3.0 abcA | 18.6 ± 2.6 abB | 26.19% | <0.001 |
| 24 h | 6 Months | Percentage Drop | p-Value | |
|---|---|---|---|---|
| OIL | 12.9 ± 2.1 abcA | 9.6 ± 1.4 bcB | 25.6% | 0.003 |
| M | 11.9 ± 1.8 bcA | 7.5 ± 1.3 cB | 37% | <0.0001 |
| FBM+ | 11.6 ± 2.7 cA | 7.9 ±1.1 cB | 31.9% | 0.005 |
| S/FBM+ | 17.0 ± 3.7 aA | 8.4 ± 0.7 cB | 50.6% | <0.0001 |
| AB | 15.8 ± 3.3 abA | 8.6 ± 1.2 cB | 45.6% | <0.0001 |
| S/AB | 11.6 ± 2.0 cA | 8.1 ± 1.4 cB | 30.2% | 0.002 |
| CRS | 16.7 ± 2.3 aA | 11.1 ± 2.5 abB | 33.5% | <0.0001 |
| S/CB | 12.9 ± 2.4 abcA | 12.7 ± 1.2 aA | 1.6% | 0.860 |
| X-Tra Fil | Admira Fusion X-Tra | p-Value | ||
|---|---|---|---|---|
| 24 h | OIL | 21.5 ± 4.8 A | 12.9 ± 2.1 B | 0.001 |
| M | 28.3 ± 4.3 A | 11.9 ± 1.8 B | <0.0001 | |
| FBM+ | 25.1 ± 3.6 A | 11.6 ± 2.7 B | <0.0001 | |
| S/FBM+ | 27.4 ± 5.0 A | 17.0 ± 3.7 B | 0.001 | |
| AB | 14.1± 2.2 A | 15.8 ± 3.3 A | 0.275 | |
| S/AB | 19.3 ± 4.1 A | 11.6 ± 2.0 B | 0.001 | |
| CRS | 26.3 ± 5.1 A | 16.7 ± 2.3 B | 0.001 | |
| S/CB | 25.2 ± 3.0 A | 12.9 ± 2.4 B | <0.001 | |
| 6 months | OIL | 16.2 ± 1.9 A | 9.6 ± 1.4 B | <0.001 |
| M | 10.9 ± 2.8 A | 7.5 ± 1.3 B | 0.012 | |
| FBM+ | 17.3 ± 2.1 A | 7.9 ±1.1 B | <0.0001 | |
| S/FBM+ | 21.2 ± 2.9 A | 8.4 ± 0.7 B | <0.0001 | |
| AB | 10.4 ± 2.2 A | 8.6 ± 1.2 A | 0.060 | |
| S/AB | 15.3 ± 2.1 A | 8.1 ± 1.4 B | <0.0001 | |
| CRS | 20.5 ± 3.5 A | 11.1 ± 2.5 B | <0.0001 | |
| S/CB | 18.6 ± 2.6 A | 12.7 ± 1.2 B | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Askary, F.S.; Botros, S.A.; Özcan, M. Effect of Surface Treatment and Storage Time on Immediate Repair Bond Strength Durability of Methacrylate- and Ormocer-Based Bulk Fill Resin Composites. Appl. Sci. 2020, 10, 8308. https://doi.org/10.3390/app10228308
El-Askary FS, Botros SA, Özcan M. Effect of Surface Treatment and Storage Time on Immediate Repair Bond Strength Durability of Methacrylate- and Ormocer-Based Bulk Fill Resin Composites. Applied Sciences. 2020; 10(22):8308. https://doi.org/10.3390/app10228308
Chicago/Turabian StyleEl-Askary, Farid S., Sara A. Botros, and Mutlu Özcan. 2020. "Effect of Surface Treatment and Storage Time on Immediate Repair Bond Strength Durability of Methacrylate- and Ormocer-Based Bulk Fill Resin Composites" Applied Sciences 10, no. 22: 8308. https://doi.org/10.3390/app10228308