Abstract
Endocrowns are primarily recommended in a molar region with a standardized preparation design. The aim of the study was to evaluate the effect of different occlusal preparation depths, pulp chamber-radicular extension, and all-ceramic materials on the fracture resistance of premolar endocrowns. Ninety human premolar teeth were root canal treated, randomly divided into three main groups according to all-ceramic material used for fabrication as Lithium Disilicate (LD) ceramic, Polymer infiltrated ceramic (PIC) and High translucency zirconia (HTZ). They were further subdivided into three subgroups (n = 10) according to preparation design of 2 mm occlusal reduction, 4.5 mm occlusal reduction and 4.5 mm occlusal reduction with 2 mm radicular extension. The endocrowns from respective restorative materials were fabricated, surface conditioned, and cemented with self-adhesive resin cement. All samples were thermocycled for 5000 cycles and subjected to compressive static load at 45° angluation with the cross-head speed of 0.5 mm/minute until the fracture. The mean fracture resistance of LD ceramic at 2 mm, 4.5 mm thickness and radicular extension was 62.55 MPa, 45.80 MPa, 74.27 MPa respectively. The corresponding values for the PIC and HTZ ceramics were 26.30 MPa, 21.65 MPa, 25.66 Mpa and 23.47 MPa, 27.30 MPa, 37.29 MPa respectively. The LD ceramic and greater extension inside the pulp chamber had higher fracture resistance.
1. Introduction
Chronic apical periodontitis is the most prevalent diagnosed oral disease; several studies have highlighted the high prevalence of the root canal treated teeth in the population [1]. Rehabilitation of endodontically treated teeth (ETT) with extensive coronal loss is a clinical challenge due to the higher risk of biomechanical failure [2]. The conventional approach is to re-build the coronal structural defect with an adhesive restore material along with the post and full veneer crown. The material and shape of the post influence the biomechanical behavior of the ETT teeth; besides its limited application of a post in the short, wide, and curved root canals. The endodontic post presents an additional risk of accidental root perforation and root fracture because of the incompatible modulus of elasticity with radicular dentin [3].
Advances in adhesive dentistry and emphasis to develop conservative options to rehabilitate ETT lead to the proposal of endocrowns by Pissis in 1985 [4]. Later, Bindl et al. [5], and Lander et al. [6] reported the case reports and clinical evaluation of endocrowns. The endocrowns are monolithically restored with core and crown restoration. Endocrowns utilizes the macro-retentive support from pulp chamber walls and micromechanical retention from adhesive cementation [7]. The tooth preparation for monolithic endocrowns restorations is specific; required to satisfy the biomechanical principles to succeed for longer clinical service [8]. Definite guidelines recommended by the researchers include 2 mm occlusal thickness, butt joint margin of 1–1.25 mm and 5–7° divergence of coronal pulp chamber walls [9,10]. Fewer additional modifications like immediate dentin sealing, lesser occlusal height, and uniform ferrule are suggested to improve the esthetic and biomechanical performance [11,12]. Endocrowns provide advantages of reduced stress due to fewer different materials; unlike conventional crowns with numerous interfaces resulting from luting cement, post, core, and crown. The removal of radicular dentin to accommodate the post is not required and prevents the risk of recontamination of the canal. The secondary benefits are lesser gingival inflammation due to the supra-gingival positioning of the preparation margin and a reduced predisposition to recurrent caries. Previous investigators have reported the exceptional performance of endocrowns, particularly on molar teeth [13]. Otto [14] recorded no difference in survival rate between the molars restored with conventional full veneer crowns and endocrowns over 12 years of observation.
Lithium disilicate (LD) reinforced glass-ceramics with an improved flexural strength of 400 MPa and fracture toughness of 2.0 MPa is preferred monoblack material for endocrowns fabrication [15]. An additional advantage is its superior bond strength with the tooth substrate [16]. Utilization of CAD-CAM (Computer-aided design-computer aided milling) technology to fabricate the endocrowns resulted in the utility of numerous materials like resin composite, lithium disilicate, polymer infiltrated ceramic, hybrid ceramic, monolithic zirconia. The combined Physico-Mechanical Properties of ceramic and polymers are utilized to simulate the natural tooth structure in the polymer infiltrated ceramic (PIC). The PIC reported with a flexural strength of 130 MPa, fracture toughness at 1.4 MPa and comparable elastic modulus with dentin; is a promising material to be employed for the fabrication of endocrowns [17]. The PIC materials reported to bear occlusal force up to 1000 N; its mechanical properties and edge sharpness allow the fabrication of a thinner crown up to 0.2 mm [18]. Meanwhile, High translucency zirconia (HTZ) was introduced to overcome two common drawbacks of conventional zirconia including Veneer cracking and white opaque color. HTZ can be used for fabrication of monolithic, fully anatomical restorations; it is promising addition with enhanced esthetics and higher flexural strength compared to LD ceramic.
The commonly reported reasons for the clinical failures of endocrowns are tooth fracture and debonding of endocrowns [19]. Hence, researchers suggest occlusal thickness for the endocrowns to be at 1.5–2 mm. However limited scientific evidence is available to support this recommendation [5]. Clinicians routinely encounter the ETT with occlusal deficiency ranging from 3 to 7 mm. The reports from earlier researches regarding the effect of increased occlusal thickness on the endocrown fracture resistance are not conclusive. Zarone F et al. [20] report the enhanced fractured resistance with increased occlusal thickness, while Tsai YL et al. [21] recommended 3 mm for reducing catastrophic failures. The preparation height of over 4 mm would lead to shorter pulp chamber depth for retention and hamper the stress distribution. Sorensen et al. [22] recommended the retentive length including a post at least equaled to crown height. Thus, the extension into the root canal to enhance the retentive area equals to coronal height could be a significant model to be evaluated. The significant difference in biomechanical behavior between all-ceramic materials is also expected to influence the clinical performance of endocrowns. Occlusal forces on the molar region are predominantly is axial loading; whereas the premolar region chewing function is comprising of axial loading accompanied by lateral forces. Consequently, the durability of restorative material depends on the elasticity of modulus, along with resilience under shear stresses. Generally, the long-term success of endocrowns is dependent on the selection of appropriate ceramic material for each clinical situation. With the availability of a large number of ceramic materials, the dentist should select a suitable restorative material. Though the few researchers have explored the fracture resistance of endocrowns in different occlusal thickness, there is no literature exists on the fracture resistance of various all-ceramic crowns in different thicknesses along with radicular extension at premolar region. Thus, this in-vitro study aimed to evaluate the effect of different occlusal preparation depths, radicular extension and all-ceramic materials on the fracture resistance of premolar endocrowns. The null hypothesis of the study was (1) the occlusal preparation depth and radicular extension would not affect the fracture strength of endocrowns. (2) Different all-ceramic materials do not affect the fracture resistance of endocrowns. (3) The different preparation depth or materials would not affect the failure type.
2. Materials and Methods
Intuitional ethical review board authorization was obtained for the study proposal (SRC/ETH/2018-19/089). Ninety intact human premolar teeth were collected from oral surgery clinics. The teeth were extracted for orthodontic or periodontics therapeutic purposes. The average dimension of the teeth samples was similar with a single root canal and the average mean root length of 15.92 ± 1.86 mm. The root canal morphology was confirmed with mesiodistal, buccolingual intra-oral radiographs. The exclusion criteria for the teeth samples include caries, fractures, previous endodontic treatment, and dental anomalies. Teeth samples were stored in distilled until the preparation of the study.
2.1. Endodontic Treatment
The root canal treatment was initiated with adequate access cavity preparation and initial root canal exploration with a 10 K file (Mani, Tochigi, Japan). The working length was maintained one mm short of the apical foramen. The Root canals were prepared and shaped with until X3 size using Pro-Taper Next rotary system (ProTaper, Dentsply Maillefer, Tulsa, OK, USA). The root canals were intermittently irrigated with 2 mL of 3% Sodium hypochlorite solution after each nickel-titanium rotary file change. Root canal preparation was concluded with final irritation with 5 mL distilled water and dried with paper points. Subsequently, Root canals were obturated with Pro-Taper gutta-percha cones and a sealer (AHPlus, DentsplyMaillefer, Tulsa, OK, USA). The access cavity was restored with temporary restorative material (Cavit, 3M ESPE, Seefeld, Germany) and stored in distilled water for one week to enable the complete set of sealer. The teeth samples were randomly divided into three groups with each group consisting of 30 samples to fabricate endocrowns with different all-ceramic materials like lithium disilicate glass–ceramic (IPS Emax, Ivoclar Vivadent, Schaan, Lichtenstein, Germany). Highly translucent Monolithic zirconia (Ceramill Zolid HT +White, Amann Girrbach AG, Herrschaftswiesen, Koblach, Austria) and polymer infiltrated ceramic (Vita Enamic, VITA North America, Inc. Brea, CA, USA). Each group was subdivided into 3 subgroups (n = 10) according to preparation depth. The Group-I was with occlusal preparation depth of 2 mm, Group II received 4.5 mm occlusal preparation depth and Group III included 4.5 mm occlusal preparation and 2 mm radicular extension (Figure 1). Nine groups of 10 specimens each per testing group were determined according to previously published studies [23,24]. The sample size was calculated with G* Power software (version 3.1; University of Dusseldorf), with an effect size (d) of 0.4, α of 0.05, and 1-β (power) of 0.73 [25]. The effect size was calculated from the fracture resistance of the conventional crown to endocrowns from earlier studies [23,24].

Figure 1.
Endocrowns designs for different groups.
2.2. Endocrowns Preparation
Root canal treated teeth were vertically implanted inside no-shrink epoxy resin with the help of a vertical holding machine. The cementoenamel junction was kept 2 mm above the resin block surface. The occlusal preparation depth was completed according to the group. The teeth preparation depth was standardized with a graduated periodontal probe. The teeth preparation had retentive pulp chamber depth from the central groove at 7.0 mm and 8° taper of the pulp chamber. The teeth preparation taper was standardized with the help of a parallel milling machine (Bravo, Mariotti, Forli FC, Italy). Occlusal preparation was performed by a single researcher using tapered diamond bur (856F, Hager and Meisinger GmbH, Neuss, Germany). For group 3 samples, the Gutta-percha from root canal was removed up to 2 mm with hot endo-plugger. Radicular extension width was kept at 1.3 mm and depth at 2 mm, it was standardized with pre-calibrated endodontic post drill (Fibrekleer, Pentron clinical, Oranage, CA, USA) along with silicone rubber stopper to measure the length.
2.3. Fabrication of Endocrowns and Cementation
Group LD endocrowns were fabricated with pressable Lithium disilicate glass-ceramic. The wax patterns were fabricated directly over the teeth samples by the single dental technician. The dimension from the central groove to the pulpal floor in the wax pattern (Geo classic opak, Renfert, Germany) was verified with a digital caliper (fino Pra Ceci caliper; FINO GmbH, Bad Bocklet, Germany). The occlusal anatomy of all samples was standardized with the help of a single silicone mold. The wax patterns were invested (Pressvest speed, Ivoclar Vivadent, Liechtenstein, Germany), burn out in a furnace, and heat pressed with an IPS Empress, Programat, EP 5000 furnace (Ivoclar Vivadent AG Schaan, Liechtenstein, Germany) at 920 °C. The pressed endocrowns were finished with a brief sandblasting with 100 Al2O3 at 1 bar (15 psi) pressure and steam cleaned. In conclusion, the specimens were rinsed in an ultrasonic cleaner with distilled water for 10 min and were coated with a single layer of the neutral shade glaze by firing at 765 °C. The endocrowns fabrication from HTZ and PIC were fabricated utilizing the Amann Girrbach system (Amann Girrbach AG, Koblach, Austria). The digital impression of the endocrowns preparations was obtained by a laboratory scanner (Ceramil Map, Amann Girrbach AG, Koblach, Austria). The standardized endocrowns was designed (Ceramil mind, Amann Girrbach AG, Koblach, Austria) at a 2.5% lesser volume for uniform luting cement space during cementation. The milling of endocrowns was accomplished with a computer-aided milling machine (ceramill motion 2, Amann Girrbach AG, Koblach, Austria).
Intaglio surface of LD ceramic and PIC endocrowns were prepared by etching with 5% hydrofluoric acid (IPS ceramic etching gel) for 20 s and 60 s, respectively. Subsequently washed and ultrasonically cleaned for 10 min. Finally, mono-component silane (Monobond Plus, Ivoclar Vivadent AG, Schaan Liechtenstein) was applied and excess was air-dried. HTZ zirconia endocrowns surface was subjected to airborne-particle abrasion with 50 µm alumina oxide particles at 2 bar pressure for 1 min. Washed with water and ultrasonically cleaned for 10 min. Enamel surfaces were selectively etched with 37.5% phosphoric acid (Ultra-Etch, Ultradent Products, South Jordan, UT, USA), washed with water and gentle air-dried. All the endocrowns samples were cemented with self-adhesive luting cement (RelyX Unicem2 Automix, 3M ESPE, Seefeld, Germany), light-cured for 20 s for all the surfaces.
All samples were thermo-cycled (1100; SD Mechatronik, Feldkirchen-Westerham, Germany) for 5000 cycles between 5° and 55 °C with the dwell time of 30 s. Static load at a crosshead speed of 1 mm/min was exerted with a universal testing machine (Instron, Norwood, MA, USA). The Load was applied at 45-degree angulation over buccal cusp until the fracture (Figure 2). The maximum load at the fracture is expressed in MPa. The fractured samples were evaluated with a stereomicroscope ×10 (Olympus/DeTrey, Germany) to determine the failure mode. The fractures were classified [26] as unfavorable if it involved the vertical fracture or fracture below assumed alveolar bone level requiring tooth extraction in the clinical situation (Figure 3). The failures were categorized as favorable if it included the debonding, cohesive fracture or crack in the crown. Obtained data were statistically analyzed using SPSS 19 software (IBM Corporation, Armonk, NY, USA). The data were assessed by one-way ANOVA and Tukey HSD (honestly significant difference) tests. Significance was set to p < 0.05.
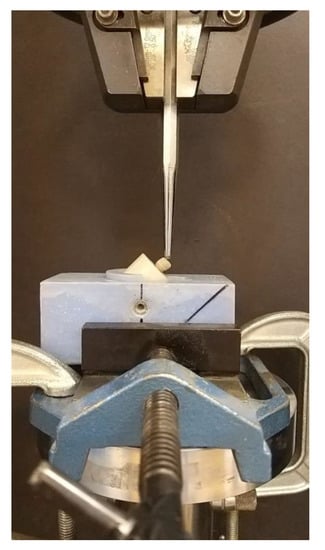
Figure 2.
Fracture resistance evaluation with a universal testing machine.
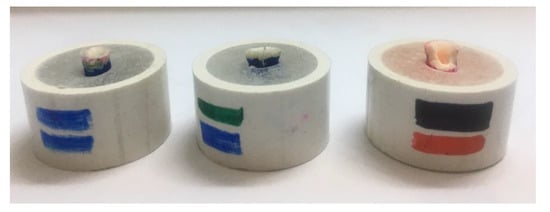
Figure 3.
Fractured teeth specimens to evaluate the failure mode.
3. Results
The mean fracture strength for all the tested groups is summarized in Table 1. The Mean fracture resistance for LD ceramic endocrowns at 2 mm occlusal thickness was 62.55 MPa, while at 4.5 mm thickness it was reduced to 45.80 MPa. The 2 mm radicular extension for 4.5 mm occlusal thickness LD ceramic endocrowns showed the improved fracture resistance at 74.27 MPa. The PIC endocrowns displayed the least fracture resistance in comparison to other tested groups. PIC endocrowns fracture resistance for varying occlusal thickness of 2 mm, 4.5 mm and 2 mm radicular extension recorded 26.30 MPa, 21.65 MPa, and 25.66 MPa respectively. HTZ endocrowns showed moderate fracture resistance across all the groups. 2 mm occlusal thickness recorded the fracture resistance of 23.47 MPa, 4.5 mm occlusal thickness of 27.30 MPa. However, a 2 mm radicular extension showed an enhanced fracture resistance of 37.29 MPa.

Table 1.
Descriptive statistics of the mean fracture resistance at maximum load (MPa) recorded in the different groups.
A One-way ANOVA (Table 2) was conducted to compare the effect of occlusal thickness and radicular extension on the fracture resistance of endocrowns fabricated from different all-ceramic materials. ANOVA analysis of variance showed that the effect of preparation design on fracture resistance was significant in LD ceramic endocrowns, F (2, 27) = 81.806, p = 0.000. Similar significant difference in fracture resistance was recorded with PIC ceramic, F (2, 27) = 30.289, p = 0.000 and Monolithic zirconia, F (2, 27) = 75.824, p = 0.000. The Shapiro-Wilk test for normality showed the p-values 0.06, 0.322 and 0.009 for LD, PIC and HTZ ceramics respectively; indicating normal distribution of data. Tukey HSD post hoc multiple comparison tests (Table 3) showed the significant difference between the majority of material fracture resistance except between 2 mm occlusal thickness and radicular extension groups from PIC ceramic with p = 0.597. The different types of failure types are presented in Table 4. The lithium silicate at with 2 mm thickness showed predominantly debonded favorable failures, while the increased thickness of 4.5 mm and radicular extension led to increased unfavorable failure with root fractures ranging from 80%–100%. Largely favorable fractured occurred in PIC endocrowns. HTZ endocrowns samples with an occlusal thickness of 4.5 mm thickness recorded 50% unfavorable failure with root fractures.
Table 2.
One-way analysis of variance of fracture resistance at maximum load between the groups.
Table 3.
Tukey HSD (honestly significant difference) post-hoc pairwise comparison for fracture resistance at maximum load between the groups.
Table 4.
Descriptive statistics of the failure modes in different groups.
4. Discussion
Endocrowns represent a conservative alternative for the full veneer crowns with multiple advantages like low cost, minimum clinical time, and short teeth preparation time [27]. They are equally applicable in the ETT with short, curved and calcified canals requiring endodontic post. Contradictory outcomes have been reported by the researchers, though the majority of researchers suggest the Endocrown restorations with higher fracture strength than conventional crowns associated with glass fiber posts and resin composite filling core [23,28]. While others [29] propose the conventional full veneer crowns including a post with higher fracture resistance. Endocrowns are mainly advocated in molar teeth due to the axial occlusal load and larger surface area for bonding. The present study explored the feasibility of endocrowns on premolar teeth, especially with greater occlusal thickness. The samples in the study were exposed to thermocycling and lateral occlusal loading to simulate the clinical condition [30]. The simulated lateral occlusal load is more unfavourable to resin bonding interfaces than axial loading [31].
The null hypothesis investigated was, where the endocrowns in various occlusal thickness and a radicular extension fabricated from different all-ceramic would not influence the fracture resistance. The results of the present study showed the endocrowns with radicular extension had higher mean fracture resistance; the endocrowns fabricated from LD ceramic displayed higher mean fracture resistance. Hence, both null hypotheses were rejected.
Our study has shown that the LD Ceramic endocrowns with significantly higher mean fractured resistance compared to PIC ceramic and HTZ endocrowns. The normal biting force at the premolar region is recorded at 222–445 N [32]. The mean fracture load observed in our study LD ceramic was well above the maximum bite force reported by earlier studies of 738 N [33]. Although the fracture resistance observed in HTZ and PIC endocrowns were lower, but at par with expected masticatory load at premolar region. Lin et al. [34] from Finite element analysis and Weibull analysis reported the similar performance of endocrowns and conventional crowns at premolar regions under fatigue load.
LD ceramic endocrowns had 62.55 MPa at 2 mm occlusal thickness, while at 4.5 mm occlusal thickness fracture resistance reduced to 45.80. The higher fracture resistance of LD ceramic could be attributed to its superior bonding strength to natural structure and biomechanical properties. LD glass-ceramics have a high flexural strength of between 300 and 400 MPa, high fracture toughness of between 2.8–3.5 MPa and elastic modulus of 95 GPa [35]. The superior mechanical strength of LD ceramics is credited to the interlocked microstructure and shape of crystals [36]. They are characterized by high crystallinity and high aspect ratio grains; which promote bridging and hinder crack propagation [37]. Hydrofluoric acid etching dissolves the glass phase within the matric, consequently creates micro-undercuts and enlarges the bonding surface [38]. The chemical bonding between the resin and ceramic is facilitated by the silane coupling agent application. The trialkoxy silane in methacrylic monomers initially hydrolyzed; interact with one another (hydrogen bonding), partner with silicate surface through a condensation polymerization and develops a covalent bond with hydroxyl (OH) groups on the ceramic surface [39]. El-Damanhoury et al. [40] concludes the better adhesion of LD ceramics to tooth structure facilitates the transmission of occlusal forces to pulp chamber walls. LD ceramics possess an excellent ability to resist damage induced by cyclic expansion and contraction from thermocycling due to combined outcomes of micromechanical and chemical bonding by the formation of Si–O–Si and –C–C– at the interface [41]. Higher fracture resistance of LD ceramic endocrowns observed in our study is also corroborated by GÜNGÖR et al. [42].
The 2 mm radicular extension demonstrated the improved fractured resistance even with 4.5 mm occlusal reduction. The result corroborates with the findings from Lise et al. [26]; they reported the higher loads-to-failure with 2.5 mm deep endocrowns irrespective of the material utilized for the fabrication. Rocca et al. [43] reported the Endocrowns with both 2-mm and 4-mm long endo-cores displayed results after fatigue load equivalent to classical crowns. Hence, they recommended the adhesive strategies should be complemented with the macro-mechanical retention in the root. Finite element analysis by Dartora et al. [44] showed lower intensity stress and better stress distribution in endocrowns with longer intra-coronal depth. The 2 mm radicular extension proposes providing the larger bonding surface area within the root and enhances micro-mechanical retention; hindering their displacement from the root cavity under lateral stresses. The improved fracture resistance could also be influenced by the modulus of elasticity of the material.
The results of our study suggested a substantial reduction in fracture resistance with higher occlusal thickens in both LD ceramic and PIC ceramics. The Fracture resistance of LD ceramic at 4.5mm thickness was reduced to 45.80 MPa from 62.55 MPa. These results were in agreement with the Finite element analysis reported by Hasan et al. [45]. They found that the Von Mises stress with the remaining tooth structure was 54–57 MPa with the load applied 5 mm above the restoration–tooth junction. The Von Mises stress was substantially increased to 87–90 MPa when the load was placed at a height of 8 mm. The total equivalent strain recorded was at 2000–2300 µɛ for 5 mm height load application, 3800–4200 µɛ for the loading height of 8 mm. The higher the crown height from the restoration-tooth junction, the stress and deformation are expected to rise because of an increase in lever arm length.
The PIC endocrowns showed lesser fracture resistance of 26.30 MPa at 2.5 mm occlusal thickness. The radicular extension indicated marginal improvement in the fracture resistance. The results were in agreement with the findings from Adel S et al. [46]; they reported no significant difference in fracture resistance between the preparation depths of 2 mm and 4 mm within the similar marginal design. Zhu et al. [47] reported as the thickness of restorative material increased, the von Mises stress in dentin increased. An increase in the elastic modulus of the material may benefit the durability of bonding between the endocrowns and the abutment tooth; however, it may cause a fracture of the residual tooth structure. Argyrou et al. [48] described the modulus of elasticity of PIC at 27.26 GPa, the lower modulus of elasticity could be the reason for the lower fracture resistance of PIC endocrowns. Hence the conservative teeth preparation for the endocrowns is likely to improve the fracture resistance, as confirmed from the results of our study.
The results of the study indicated the high HTZ endocrowns with the least fracture resistance of 23.47 MPa at 2 mm thickness. In contrast to other tested material, the fracture resistance was moderately enhanced to 27.30 MPa with an increased thickness of 4.5 mm. The radicular extension was a significant aid in increasing fracture resistance up to 37.29 MPa. The flexural strength and modulus of elasticity of HTZ zirconia is reported to be at 800–1100 MPa and 200 GPa. The HTZ has more natural esthetic properties with increased optical properties attributed to the inclusion of cubic zirconia [49]. Several studies concluded the lower mechanical properties of HTZ ceramic is due to the absence of transformation toughening mechanism [50]. High flexural strength and fracture resistance in zirconia is credited to volume expansion associated with transformation from the tetragonal to the monoclinic phase. Consequently, it creates the compressive stress behind the crack tip [51]. Reduced mechanical properties of HTZ restorations are due to the absence of monoclinic peaks and grains below 1 μm HTZ restorations [52]. Augmented fracture resistance of HTZ ceramic at increased thickness could be attributed to its correlation of fracture strength with thickness [53]. Ozer et al. [54] suggested the air-borne particle abrasion enhances the flexural strength. Previous studies have also reported a higher load-bearing capacity of LD ceramics compared to HTZ ceramics when bonded on to dentin [55]. Yamanel et al. [56] suggested that the more stress is transferred to restorative material with the high elastic modulus, predisposing it for the early fracture. Most unfavorable failures type was observed in LD ceramic with an increased incidence of root fracture. Zarone et al. [20] from their 3D FE analysis described the concentration of an equivalent von Mises stress at the interface of materials with different elastic modulus. The stiffer material with higher modulus elasticity affects the distribution of an equivalent von Mises stress. The difference in modulus of elasticity between resin luting cement, indirect crown, and dentin predisposes the ETT for root fracture. The PIC ceramics with mechanical properties closely matching the natural tooth hard tissues lower the frequency of unfavorable root fracture [57]. The clinical implications of Study results include the LD ceramics is material of choice for fabrication of endocrowns at premolar region. The larger occlusal thickness of the endocrowns needs to be compensated with comparable radicular extension to enhance fracture resistance.
Limitations of the study include, Even though due care is observed in the standardization of teeth samples some degree of variability is difficult to eliminate. The static load was applied for testing samples, unlike masticatory forces and a relatively small sample size. Since the hypothesis was tested on the premolar teeth, the angle of the load was at 45° angulation. Further studies suggested evaluating the fracture resistance with various occlusal thicknesses and radicular extension in molars with axial loading.
5. Conclusions
Within the limitations of the study following conclusions were drawn:
- (1)
- LD ceramic performed better as material for endocrowns fabrication at a standard thickness of 2.5 mm as well as at increased occlusal thickness at 4.5 mm with 62.55 MPa and 45.80 respectively.
- (2)
- Fracture resistance of endocrowns fabricated from PIC and HTZ was at a similar range and lower than LD ceramic.
- (3)
- The greater extension of endocrowns inside the pulp chamber and radicular extension provided better mechanical performance in LD ceramic and HTZ ceramics.
- (4)
- LD ceramic Endocrowns showed substantially higher fracture resistance than the average masticatory force. Hence, LD ceramic endocrowns can be clinically utilized for the fabrication of endocrowns in the premolar region.
Author Contributions
Conceptualization, S.B.H.; data curation S.B.H.; investigation, A.A.A., S.A.A. and D.S.A.; methodology, S.B.H., M.A.; supervision, S.B.H.; writing—original draft, S.B.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Loftus, J.J.; Keating, A.P.; McCartan, B.E. Periapical status and quality of endodontic treatment in an adult Irish population. Int. Endod. J. 2005, 38, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Sagsen, B.; Aslan, B. Effect of bonded restorations on the fracture resistance of root filled teeth. Int. Endod. J. 2006, 39, 900–904. [Google Scholar] [CrossRef]
- Genovese, K.; Lamberti, L.; Pappalettere, C. Finite element analysis of a new customized composite post system for endodontically treated teeth. J. Biomech. 2005, 38, 2375–2389. [Google Scholar] [CrossRef] [PubMed]
- Pissis, P. Fabrication of a metal-free ceramic restoration utilizing the monobloc technique. Pract. Periodontics Aesthetic Dent. 1995, 7, 83–94. [Google Scholar]
- Bindl, A.; Mormann, W.H. Clinical evaluation of adhesively placed Cerec endo-crowns after 2 years--preliminary results. J. Adhes. Dent. 1999, 1, 255–265. [Google Scholar] [PubMed]
- Lander, E.; Dietschi, D. Endocrowns: A clinical report. Quintessence Int. 2008, 39, 99–106. [Google Scholar]
- Mormann, W.H.; Bindl, A.; Luthy, H.; Rathke, A. Effects of preparation and luting system on all-ceramic computer-generated crowns. Int. J. Prosthodont. 1998, 11, 333–339. [Google Scholar]
- Pippin, D.J.; Mixson, J.M.; Soldan-Els, A.P. Clinical evaluation of restored maxillary incisors: Veneers vs. PFM crowns. J. Am. Dent. Assoc. 1995, 126, 1523–1529. [Google Scholar] [CrossRef]
- Bindl, A.; Richter, B.; Mormann, W.H. Survival of ceramic computer-aided design/manufacturing crowns bonded to preparations with reduced macroretention geometry. Int J. Prosthodont. 2005, 18, 219–224. [Google Scholar] [CrossRef]
- Fages, M.; Bennasar, B. The endocrown: A different type of all-ceramic reconstruction for molars. J. Can. Dent. Assoc. 2013, 79, d140. [Google Scholar]
- Belleflamme, M.M.; Geerts, S.O.; Louwette, M.M.; Grenade, C.F.; Vanheusden, A.J.; Mainjot, A.K. No post-no core approach to restore severely damaged posterior teeth: An up to 10-year retrospective study of documented endocrown cases. J. Dent. 2017, 63, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, M.; DuVall, N.; Wajdowicz, M.; Brewster, J.; Roberts, H. Preparation Ferrule Design Effect on Endocrown Failure Resistance. J. Prosthodont. 2019, 28, e237–e242. [Google Scholar] [CrossRef] [PubMed]
- Sedrez-Porto, J.A.; Rosa, W.L.; da Silva, A.F.; Munchow, E.A.; Pereira-Cenci, T. Endocrown restorations: A systematic review and meta-analysis. J. Dent. 2016, 52, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Otto, T.; Mormann, W.H. Clinical performance of chairside CAD/CAM feldspathic ceramic posterior shoulder crowns and endocrowns up to 12 years. Int. J. Comput. Dent. 2015, 18, 147–161. [Google Scholar]
- Qin, F.; Zheng, S.; Luo, Z.; Li, Y.; Guo, L.; Zhao, Y.; Fu, Q. Evaluation of machinability and flexural strength of a novel dental machinable glass-ceramic. J. Dent. 2009, 37, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Gohring, T.N.; Peters, O.A. Restoration of endodontically treated teeth without posts. Am. J. Dent. 2003, 16, 313–317. [Google Scholar]
- Swain, M.; Coldea, A.; Bilkhair, A.; Guess, P. Interpenetrating network ceramic-resin composite dental restorative materials. Dent. Mater. 2016, 32, 34–42. [Google Scholar] [CrossRef]
- El Zhawi, H.; Kaizer, M.R.; Chughtai, A.; Moraes, R.R.; Zhang, Y. Polymer infiltrated ceramic network structures for resistance to fatigue fracture and wear. Dent. Mater. 2016, 32, 1352–1361. [Google Scholar] [CrossRef]
- Bernhart, J.; Bräuning, A.; Altenburger, M.; Wrbas, K. Cerec3D endocrowns--two-year clinical examination of CAD/CAM crowns for restoring endodontically treated molars. Int. J. Comput. Dent. 2010, 13, 141–154. [Google Scholar]
- Zarone, F.; Sorrentino, R.; Apicella, D.; Valentino, B.; Ferrari, M.; Aversa, R.; Apicella, A. Evaluation of the biomechanical behavior of maxillary central incisors restored by means of endocrowns compared to a natural tooth: A 3D static linear finite elements analysis. Dent. Mater. 2006, 22, 1035–1044. [Google Scholar] [CrossRef]
- Tsai, Y.L.; Petsche, P.E.; Anusavice, K.J.; Yang, M.C. Influence of glass-ceramic thickness on Hertzian and bulk fracture mechanisms. Int. J. Prosthodont. 1998, 11, 27–32. [Google Scholar] [PubMed]
- Sorensen, J.A.; Martinoff, J.T. Clinically significant factors in dowel design. J. Prosthet. Dent. 1984, 52, 28–35. [Google Scholar] [CrossRef]
- Biacchi, G.R.; Basting, R.T. Comparison of fracture strength of endocrowns and glass fiber post-retained conventional crowns. Oper. Dent. 2012, 37, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, Z.; Li, X.; Sun, C.; Gao, E.; Li, H. A comparison of the fracture resistances of endodontically treated mandibular premolars restored with endocrowns and glass fiber post-core retained conventional crowns. J. Adv. Prosthodont. 2016, 8, 489–493. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Pedrollo Lise, D.; Van Ende, A.; De Munck, J.; Umeda Suzuki, T.Y.; Cardoso Vieira, L.C.; Van Meerbeek, B. Biomechanical behavior of endodontically treated premolars using different preparation designs and CAD/CAM materials. J. Dent. 2017, 59, 54–61. [Google Scholar] [CrossRef]
- Dietschi, D.; Duc, O.; Krejci, I.; Sadan, A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature, Part II (Evaluation of fatigue behavior, interfaces, and in vivo studies). Quintessence Int. 2008, 39, 117–129. [Google Scholar]
- Chang, C.Y.; Kuo, J.S.; Lin, Y.S.; Chang, Y.H. Fracture resistance and failure modes of CEREC endo-crowns and conventional post and core-supported CEREC crowns. J. Dent. Sci. 2009, 4, 110–117. [Google Scholar] [CrossRef]
- Forberger, N.; Gohring, T.N. Influence of the type of post and core on in vitro marginal continuity, fracture resistance, and fracture mode of lithia disilicate-based all-ceramic crowns. J. Prosthet. Dent. 2008, 100, 264–273. [Google Scholar] [CrossRef]
- Heintze, S.D. Clinical relevance of tests on bond strength, microleakage and marginal adaptation. Dent. Mater. 2013, 29, 59–84. [Google Scholar] [CrossRef]
- Gresnigt, M.M.; Ozcan, M.; van den Houten, M.L.; Schipper, L.; Cune, M.S. Fracture strength, failure type and Weibull characteristics of lithium disilicate and multiphase resin composite endocrowns under axial and lateral forces. Dent. Mater. 2016, 32, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Widmalm, S.E.; Ericsson, S.G. Maximal bite force with centric and eccentric load. J. Oral Rehabil. 1982, 9, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Bantleon, H.P.; Hnat, W.P.; Freudenthaler, J.W.; Marcotte, M.R.; Johnson, B.E. A study of bite force, part 1: Relationship to various physical characteristics. Angle Orthod. 1995, 65, 367–372. [Google Scholar] [PubMed]
- Lin, C.L.; Chang, Y.H.; Chang, C.Y.; Pai, C.A.; Huang, S.F. Finite element and Weibull analyses to estimate failure risks in the ceramic endocrown and classical crown for endodontically treated maxillary premolar. Eur. J. Oral Sci. 2010, 118, 87–93. [Google Scholar] [CrossRef]
- Sakaguchi, L.R.; Powers, J.M. Craig’s Restorative Dental Materials; Elsevier: Amsterdam, The Netherlands, 2012; pp. 256–264. [Google Scholar]
- Denry, I.; Holloway, J.A. Ceramics for Dental Applications: A Review. Materials 2010, 3, 351–368. [Google Scholar] [CrossRef]
- Hallmann, L.; Ulmer, P.; Kern, M. Effect of microstructure on the mechanical properties of lithium disilicate glass-ceramics. J. Mech. Behav. Biomed. Mater. 2018, 82, 355–370. [Google Scholar] [CrossRef]
- Kang, S.H.; Chang, J.; Son, H.H. Flexural strength and microstructure of two lithium disilicate glass ceramics for CAD/CAM restoration in the dental clinic. Restor Dent. Endod. 2013, 38, 134–140. [Google Scholar] [CrossRef]
- Alex, G. CE 1-Preparing Porcelain Surfaces for Optimal Bonding. Compendium 2008, 29, 324. [Google Scholar]
- El-Damanhoury, H.M.; Haj-Ali, R.N.; Platt, J.A. Fracture resistance and microleakage of endocrowns utilizing three CAD-CAM blocks. Oper. Dent. 2015, 40, 201–210. [Google Scholar] [CrossRef]
- Li, R.; Ma, S.Q.; Zang, C.C.; Zhang, W.Y.; Liu, Z.H.; Sun, Y.C.; Feng, Y.Y. Enhanced bonding strength between lithium disilicate ceramics and resin cement by multiple surface treatments after thermal cycling. PLoS ONE 2019, 14, e0220466. [Google Scholar] [CrossRef]
- GÜNGÖR, M.B.; Bal, B.T.; Yilmaz, H.; Aydin, C.; Nemli, S.K. Fracture strength of CAD/CAM fabricated lithium disilicate and resin nano ceramic restorations used for endodontically treated teeth. Dent. Mater. J. 2017. [Google Scholar] [CrossRef]
- Rocca, G.T.; Daher, R.; Saratti, C.M.; Sedlacek, R.; Suchy, T.; Feilzer, A.; Krejci, I. Restoration of severely damaged endodontically treated premolars: The influence of the endo-core length on marginal integrity and fatigue resistance of lithium disilicate CAD-CAM ceramic endocrowns. J. Dent. 2018, 68, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Dartora, N.R.; de Conto Ferreira, M.B.; Moris, I.C.M.; Brazão, E.H.; Spazin, A.O.; Sousa-Neto, M.D.; Silva-Sousa, Y.T.; Gomes, E.A. Effect of intracoronal depth of teeth restored with endocrowns on fracture resistance: In vitro and 3-dimensional finite element analysis. J. Endod. 2018, 44, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Hasan, I.; Frentzen, M.; Utz, K.H.; Hoyer, D.; Langenbach, A.; Bourauel, C. Finite element analysis of adhesive endo-crowns of molars at different height levels of buccally applied load. J. Dent. Biomech. 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- Adel, S.; Abo-Madina, M.M.; Abo-El Farag, S.A. Fracture Strength of Hybrid Ceramic Endocrown Restoration with Different Preparation Depths and Designs. IOSR J. Dent. Med. Sci. 2019, 18, 17–23. [Google Scholar]
- Zhu, J.; Rong, Q.; Wang, X.; Gao, X. Influence of remaining tooth structure and restorative material type on stress distribution in endodontically treated maxillary premolars: A finite element analysis. J. Prosthet. Dent. 2017, 117, 646–655. [Google Scholar] [CrossRef]
- Argyrou, R.; Thompson, G.A.; Cho, S.H.; Berzins, D.W. Edge chipping resistance and flexural strength of polymer infiltrated ceramic network and resin nanoceramic restorative materials. J. Prosthet. Dent. 2016, 116, 397–403. [Google Scholar] [CrossRef]
- Kontonasaki, E.; Giasimakopoulos, P.; Rigos, A.E. Strength and aging resistance of monolithic zirconia: An update to current knowledge. Jpn. Dent. Sci. Rev. 2020, 56, 1–23. [Google Scholar] [CrossRef]
- Elsayed, A.; Meyer, G.; Wille, S.; Kern, M. Influence of the yttrium content on the fracture strength of monolithic zirconia crowns after artificial aging. Quintessence Int. 2019, 50, 344–348. [Google Scholar]
- Tong, H.; Tanaka, C.B.; Kaizer, M.R.; Zhang, Y. Characterization of three commercial Y-TZP ceramics produced for their high-translucency, high-strength and high-surface area. Ceram. Int. 2016, 42, 1077–1085. [Google Scholar] [CrossRef]
- Heuer, A.; Claussen, N.; Kriven, W.M.; Ruhle, M. Stability of tetragonal ZrO2 particles in ceramic matrices. J. Am. Ceram. Soc. 1982, 65, 642–650. [Google Scholar] [CrossRef]
- Sun, T.; Zhou, S.; Lai, R.; Liu, R.; Ma, S.; Zhou, Z.; Longquan, S. Load-bearing capacity and the recommended thickness of dental monolithic zirconia single crowns. J. Mech. Behav. Biomed. Mater. 2014, 35, 93–101. [Google Scholar] [CrossRef]
- Ozer, F.; Naden, A.; Turp, V.; Mante, F.; Sen, D.; Blatz, M.B. Effect of thickness and surface modifications on flexural strength of monolithic zirconia. J. Prosthet. Dent. 2018, 119, 987–993. [Google Scholar] [CrossRef]
- Zhang, Y.; Lee, J.J.W.; Srikanth, R.; Lawn, B.R. Edge chipping and flexural resistance of monolithic ceramics. Dent. Mater. 2013, 29, 1201–1208. [Google Scholar] [CrossRef]
- Yamanel, K.; Çaglar, A.; Gülsahi, K.; Özden, U.A. Effects of different ceramic and composite materials on stress distribution in inlay and onlay cavities: 3-D finite element analysis. Dent. Mater. J. 2009, 28, 661–670. [Google Scholar] [CrossRef]
- Aversa, R.; Apicella, D.; Perillo, L.; Sorrentino, R.; Zarone, F.; Ferrari, M.; Apicella, A. Non-linear elastic three-dimensional finite element analysis on the effect of endocrown material rigidity on alveolar bone remodeling process. Dent. Mater. 2009, 25, 678–690. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).