The Combined Effect of Indoor Air Quality and Socioeconomic Factors on Health in Northeast China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
- -
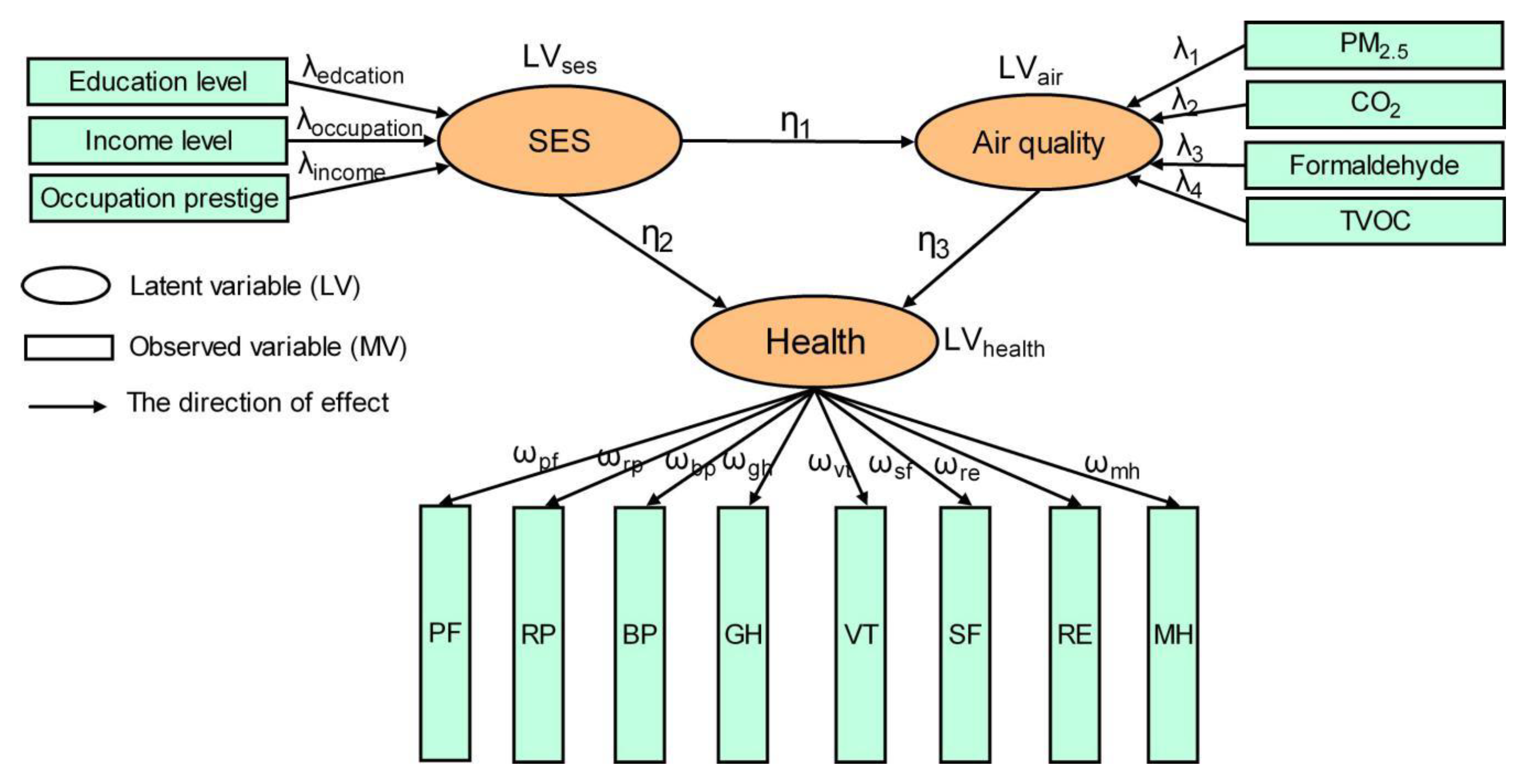
- Health variables: Health was measured by the widely used tool—the Short Form 8 Health Survey (SF-8) (as shown in Table S1). The reliability and validity of the Chinese version of the SF-8 Health Survey were confirmed [31]. The SF-8 Health Survey includes physical and mental components, and each component covers four sub-scales, the physical health: Physical functioning (PF), role physical (RP), bodily pain (BP) and general health (GH); the mental health: Vitality (VT), social functioning (SF), role emotional (RE) and mental health (MH). For example, role emotional refers to ‘have you had problems with your work or other regular daily activities (such as walking or climbing stairs) as a result of any emotional problems?’ Bodily pain indicates ‘how much bodily pain have you had?’ Each sub-scale was scored on a scale of 1 to 4 (1 represents the worst and 4 the best health status).
- -
- Socioeconomic status: Socioeconomic factors are typically determined by the level of education, income, and occupation prestige [32]. This survey used the combinations of education level (1 = ‘primary school’, 2 = ‘middle school’, 3 = ‘professional’, 4 = ‘university’, 5 = ‘master, PhD, or specialization’), income level (1 = ‘low’: <5000 yuan/month, 2 = ‘middle’:5000 ~ 10,000 yuan/month, 3 = ‘high’: >10,000 yuan/month), and occupation prestige (1 = ‘low’, 2 = ‘middle’, 3 = ‘high’) as the measurement.
- -
- Lifestyle: smoking status and alcohol consumption (‘Frequently’ = 0, ‘Sometimes’ = 1, ‘Rarely’ = 2, and ‘Not at all’ = 3);
- -
- Personal characteristics: Gender, age, and length of residence
2.2. Structure Equation Modeling
2.2.1. The Measurement Model
2.2.2. The Structural Model
2.2.3. Model Evaluation
3. Results
3.1. The Houses Measured and Respondents
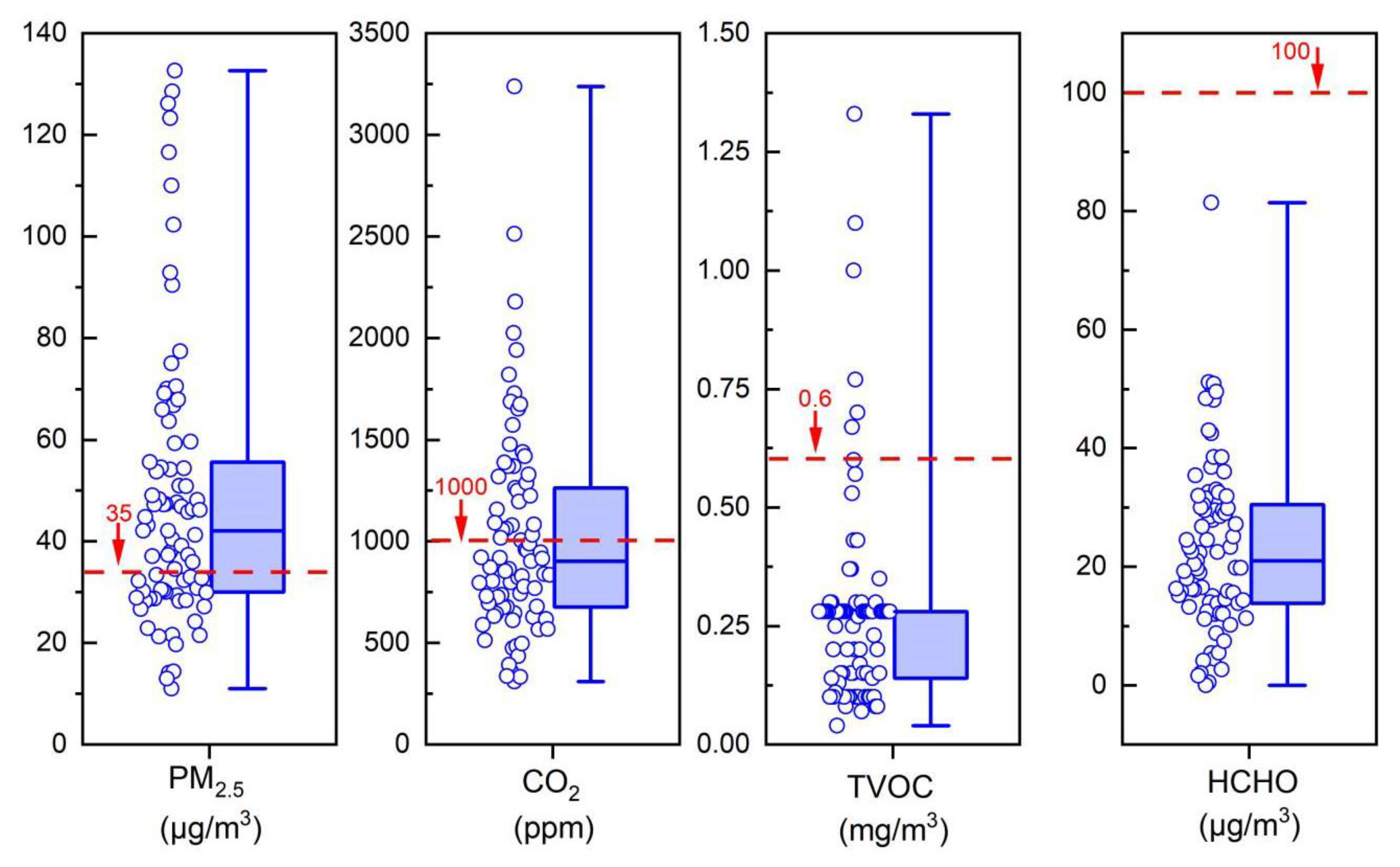
3.2. Description of the Indoor Air Pollution Level
3.3. Model Result and Evaluation
4. Discussion
4.1. Link Between Socioeconomic Factors, Indoor Air Quality, and Health
4.2. Multiple Group Analysis
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A. Global, regional, and national comparative risk assessment of 79 behavioral, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Organization for Economic Co-operation and Development. The Cost of Air Pollution: Health Impacts of Road Transport; OECD Publishing: Paris, France, 2014; pp. 1–8. [Google Scholar]
- Duan, X.L.; Zhao, X.G.; Wang, B.B. Highlights of the Chinese Exposure Factors Handbook (Adults); Science Press: Beijing, China, 2015; pp. 89–90. [Google Scholar]
- Brasche, S.; Bischof, W. Daily time spent indoors in German homes—Baseline data for the assessment of indoor exposure of German occupants. Int. J. Hyg. Environ. Health 2005, 208, 247–253. [Google Scholar] [CrossRef]
- Liu, Y.L.; Luo, K.L.; Li, L.; Shahid, M.Z. Fluoride and sulfur dioxide indoor pollution situation and control in coal-burning endemic area in Zhaotong, Yunnan, China. Atmos. Environ. 2013, 77, 725–737. [Google Scholar] [CrossRef]
- Kornartit, C.; Sokhi, R.S.; Burton, M.A.; Ravindra, K. Activity pattern and personal exposure to nitrogen dioxide in indoor and outdoor microenvironments. Environ. Int. 2010, 36, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, C.S.; Zhang, J.F.; Sigsgaard, T.; Jantunen, M.; Lioy, P.J.; Samson, R.; Karol, M.H. Current State of the Science: Health Effects and Indoor Environmental Quality. Environ. Health Perspect. 2007, 115, 958–964. [Google Scholar] [CrossRef] [Green Version]
- Morawska, L.; Afshari, A.; Bae, G.N.; Buonanno, G.; Chao, C.Y.H.; Hanninen, O.; Hofmann, W.; Isaxon, C.; Jayaratne, E.R.; Pasanen, P.; et al. Indoor aerosols: From personal exposure to risk assessment. Indoor Air 2013, 23, 462–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.D.; Wei, W.J.; Weschler, L.B.; Salthammer, T.; Kan, H.D.; Bu, Z.M.; Zhang, Y.P. Indoor formaldehyde concentrations in urban China: Preliminary study of some important influencing factors. Sci. Total Environ. 2017, 590, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Y.; You, X.B.; Hu, R.Y. Indoor radon survey in indoor environments in Zhuhai city, China. Radiat. Meas. 2005, 39, 205–207. [Google Scholar]
- Weschler, C.J. Changes in indoor pollutants since the 1950s. Atmos. Environ. 2009, 43, 153–169. [Google Scholar] [CrossRef]
- Weschler, C.J. Chemistry in indoor environments: 20 years of research. Indoor Air 2011, 21, 205–218. [Google Scholar] [CrossRef]
- Lewis, R.G. Pesticides. In Indoor Air Quality Handbook; Spengler, J.D., Samet, J.M., Eds.; McGraw-Hill: New York, NY, USA, 2001; Volume 1, pp. 1–21. [Google Scholar]
- Wang, L.X.; Zhao, B.; Liu, C.; Lin, H.; Yang, X.; Zhang, Y.P. Indoor SVOC pollution in China: A review. Chin. Sci. Bull. 2010, 55, 1469–1478. [Google Scholar] [CrossRef]
- Arcus-Arth, A.; Broadwin, R.; Lam, R. Impact of Socioeconomic Factors on Residential Indoor Air Quality and Human Health. In Environmental Toxicology and Human Health; Tetsuo, S., Ed.; Encyclopedia of Life Support Systems: Oxford, UK, 2009; Volume 2, pp. 126–154. [Google Scholar]
- Gordon, S.B.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.B. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.; Dassonville, C.; Derbez, M.; Ramalho, O.; Kirchner, S.; Crump, D.; Mandin, C. Relationships between socioeconomic and lifestyle factors and indoor air quality in French dwellings. Environ. Res. 2015, 140, 85–396. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. The Future of the Public’s Health in the 21st Century; National Academies Press: Washington, DC, USA, 2002; pp. 26–28. [Google Scholar]
- Friel, S.; Marmot, M.G. Action on the Social Determinants of Health and Health Inequities Goes Global. Annu Rev. Public Health 2011, 32, 225–236. [Google Scholar] [CrossRef] [Green Version]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Williams, D.R.; Pamuk, E. Socioeconomic disparities in health in the United States: What the patterns tell us. Am. J. Public Health 2010, 14, 20–35. [Google Scholar] [CrossRef]
- Rumchev, K.; Zhao, Y.; Spickett, J. Health Risk Assessment of Indoor Air Quality, Socioeconomic and House Characteristics on Respiratory Health among Women and Children of Tirupur, South India. Int. J. Environ. Res. Pub. He 2017, 14, 429. [Google Scholar] [CrossRef] [Green Version]
- Schlink, U.; Thiem, A.; Kohajda, T.; Richter, M.; Strebel, K. Quantile regression of indoor air concentrations of volatile organic compounds (VOC). Sci. Toral Environ. 2010, 408, 3840–3851. [Google Scholar] [CrossRef]
- Byun, H.; Bae, H.; Kim, D.; Shin, H.; Yoon, C. Effects of socioeconomic factors and human activities on children’s PM10 exposure in inner-city households in Korea. Int. Arch. Occup. Environ. Health 2010, 83, 867–878. [Google Scholar] [CrossRef]
- Loupa, G.; Fotopoulou, S.; Tsagarakis, K.P. A tool for analysing the interdependence of indoor environmental quality and reported symptoms of the hospitals’ personnel. J. Risk Res. 2017, 20, 678–691. [Google Scholar] [CrossRef]
- Tharim, A.H.A.; Samad, M.H.A.; Ismail, M. Relationship between Indoor Environmental Quality (IEQ), Occupant’s Satisfaction and Productivity in GBI Rated Office Building using SEM-PLS. Pertanika J. Soc. Sci. Hum. 2017, 25, 319–329. [Google Scholar]
- Kamaruzzaman, S.N.; Egbu, C.O.; Zawawi, E.M.A.; Karim, S.B.A.; Woon, C.J. Occupants’ satisfaction toward building environmental quality: Structural equation modeling approach. Environ. Monit. Assess. 2015, 187, 242. [Google Scholar] [CrossRef] [PubMed]
- Finell, E.; Tolvanen, A.; Haverinen-Shaughnessy, U.; Laaksonen, S.; Karvonen, S.; Sund, R.; Luopa, P.; Pekkanen, J.; Stahl, T. Indoor air problems and the perceived social climate in schools: A multilevel structural equation analysis. Sci. Total Environ. 2018, 624, 1504–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Bureau of Statistics. Available online: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm (accessed on 3 February 2020).
- Jokl, M.V. Indoor Air Quality Assessment Based on human Physiology-Part 3. Applications. Acta Polytech. 2003, 43, 38–46. [Google Scholar]
- Inspection and Quarantine of the People’s Republic of China; National health commission of the People’s Republic of China. Indoor Air Quality Standard (GB/T 18883-2002); China Architecture & Building Press: Beijing, China, 2002; pp. 1–12. [Google Scholar]
- Lang, L.H.; Zhang, L.C.; Zhang, P.; Li, Q.; Jiang, B.; Guo, Y. Evaluating the reliability and validity of SF-8 with a large representative sample of urban Chinese. Health Qual. Life Outcome 2018, 16, 55–63. [Google Scholar] [CrossRef] [Green Version]
- Ensminger, M.; Fotherill, K. A decade of measuring SES: What it tells us and where to go from here. In Socioeconomic Status, Parenting, and Child. Development; Bornstein, M., Bradley, R., Eds.; Lawrence Erlbaum: Mahwah, NJ, USA, 2003; pp. 25–36. [Google Scholar]
- Jarvis, C.B.; MacKenzie, S.B.; Podsakoff, P.M. A critical review of construct indicators and measurement model misspecification in marketing and consumer research. J. Consum. Res. 2003, 30, 199–218. [Google Scholar] [CrossRef]
- Humphreys, M.A. Quantifying occupant comfort: Are combined indices of the indoor environment practicable? Build. Res. Inf. 2005, 33, 317–325. [Google Scholar] [CrossRef]
- Sarstedt, M.; Hair, J.F.; Ringle, C.M.; Thiele, K.O.; Gudergan, S.P. Estimation issues with PLS and CBSEM: Where the bias lies! J. Bus. Res. 2016, 69, 3998–4010. [Google Scholar] [CrossRef] [Green Version]
- SmartPLS. Available online: https://www.smartpls.com/ (accessed on 18 January 2020).
- Hair, J.F.; Hult, G.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage: Los Angeles, LA, USA, 2014; pp. 95–205. [Google Scholar]
- Henseler, J.; Chin, W.W. A comparison of approaches for the analysis of interaction effects between latent variables using partial least squares path modeling. Struct. Equ. Modeling 2010, 17, 82–109. [Google Scholar] [CrossRef]
- European Committee for Standardization. Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics (BS EN15251); European Committee for Standardization: Brussels, Belgium, 2007; pp. 11–51. [Google Scholar]
- U.S. Environmental Protection Agency. Available online: http://www.epa.Gov/air/criteria.html (accessed on 5 February 2020).
- Finish Society of Indoor Air Quality and Climate, Building Information Foundation RTS, Finnish Association of Architects, Finnish Association of Building Owners and Construction Clients, Finnish Association of Consulting Firms. Classification of Indoor Environment 2008: Target Values, Design Guidance and Product Requirements; Painotalo Trinket Oy: Helsinki, Finland, 2010. [Google Scholar]
- Huang, K.L.; Feng, G.H.; Li, H.X.; Yu, S. Opening window issue of residential buildings in winter in north China: A case study in Shenyang. Energ. Build. 2014, 84, 567–574. [Google Scholar] [CrossRef]
- Hou, J.; Zhang, Y.F.; Sun, Y.X.; Wang, P.; Zhang, Q.N.; Kong, X.R.; Sundell, J. Air change rates at night in northeast Chinese homes. Build. Environ. 2018, 132, 273–281. [Google Scholar] [CrossRef]
- Huang, K.L.; Song, J.S.; Feng, G.H.; Chang, Q.P.; Jiang, B.; Wang, J.; Sun, W.; Li, H.X.; Wang, J.M.; Fang, X.S. Indoor air quality analysis of residential buildings in northeast China based on field measurements and long time monitoring. Build. Environ. 2018, 144, 171–183. [Google Scholar] [CrossRef]
- America’s Health Rankings. Available online: https://www.americashealthrankings.org/ (accessed on 7 February 2020).
- Booske, B.C.; Athens, J.K.; Kindig, D.A.; Park, H.; Remington, P.L. Different perspectives for assigning weights to determinants of health. Univ. Wis. Popul. Health Inst. 2010, 1, 1–20. [Google Scholar]
- Athens, J.K. Assessing the validity of health determinants in the Wisconsin County Health Rankings. Master’s Thesis, University of Wisconsin: Madison, WI, USA, 2008. [Google Scholar]
- Braveman, P.; Egerter, S.; Williams, D.R. The Social Determinants of Health: Coming of Age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- County Health Ranking & Roadmaps. Available online: https://www.countyhealthrankings.org (accessed on 15 February 2020).
- Gabel, J.; Levitt, L.; Holve, E.; Pickreign, J.; Whitemore, H. Job-based health benefifits in 2002: Some important trends. Health Aff. 2002, 21, 143–151. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen, Dioxide and Sulfur Dioxide—Global Update 2005; World Health Organization Press: Geneva, Switzerland, 2005; pp. 10–12. [Google Scholar]
- Ni, Y.M.; Shi, G.C.; Qu, J.M. Indoor PM2.5, tobacco smoking and chronic lung diseases: A narrative review. Environ. Res. 2020, 181, 1–10. [Google Scholar] [CrossRef]
- Lance, W. Indoor Particles: A Review. J. Air Waste Manage. 1996, 46, 98–126. [Google Scholar]
- Guo, H.; Lee, S.C.; Li, W.M.; Cao, J.J. Source characterization of BTEX in indoor micro environments in Hong Kong. Atmos. Environ. 2003, 37, 73–82. [Google Scholar] [CrossRef]
- Tobacco Use in Canada. Available online: https://uwaterloo.ca/tobacco-use-canada/adult-tobacco-use (accessed on 16 February 2020).
- Arday, D.R.; Giovino, G.A.; Schulman, J.; Nelson, D.E.; Mowery, P.; Samet, J.M. Cigarette smoking and self-reported health problems among U.S. high school seniors, 1982–1989. Am. J. Health Promot. 1995, 10, 111–117. [Google Scholar] [CrossRef]
- Salomon, J.A.; Nordhagen, S.; Oza, S.; Murray, C.J. Are Americans feeling less healthy? The puzzle of trends in self-rated health. Am. J. Epidemiol. 2009, 170, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Lyyra, T.M.; Heikkinen, E.; Lyyra, A.L. Self-rated health and mortality: Could clinical and performance-based measures of health and functioning explain the association? Arch. Gerontol. Geriat. 2006, 42, 277–288. [Google Scholar] [CrossRef]
- Amélie, Q.V. Self-rated health: Caught in the crossfire of the quest for ‘true’ health? Int. J. Epidemiol. 2007, 36, 1161–1164. [Google Scholar]
- Qi, Y.Q. Reliability and Validity of Self-Rated General Health. Chn. J. Soc. 2004, 6, 196–215, (Chinese version). [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | Instrument | Range | Accuracy |
|---|---|---|---|
| CO2 | MCH-383SD | 0 ~ 4000 ppm | ±5% |
| PM2.5 | SHINYEI PM SENSOR | 1 ~ 1000 μg/m3 | ±1% |
| HCHO | SHINYEI IAQ SENSING | 0 ~ 5 mg/m3 | ±2% |
| TVOC | GC112A | 0 ~ 1000 ppm | ±2% |
| Indicator | Category | |||
|---|---|---|---|---|
| I | II | III | IV | |
| CO2 (ppm) | 700 | 700–850 | 850–1150 | >1150 |
| PM2.5 (μg/m3) | 15 | 15–40 | 40–65 | >65 |
| HCHO (μg/m3) | <30 | 30–65 | 65–100 | >100 |
| TVOC (μg/m3) | <200 | 200–400 | 400–600 | >600 |
| Information | N (%) | Information | N (%) |
|---|---|---|---|
| Houses | Education level | ||
| Construction date | Master, PhD, or specialization | 26 (17.2%) | |
| Before 1990 | 9 (11.1%) | University or Professional | 74 (49.0%) |
| 1990–2000 | 16 (19.8%) | Middle school or less | 51 (33.8%) |
| 2000–2010 | 42 (51.9%) | Length of residence | |
| After 2010 | 14 (17.3%) | ≤5 years | 38 (25.2%) |
| Number of people per floor area (person/m2) | 5 ~ 10 years | 55 (36.4%) | |
| ≤0.02 | 15 (18.5%) | ≥10 years | 58 (38.4%) |
| 0.02–0.03 | 22 (27.2%) | Lifestyle | |
| 0.03–0.04 | 21 (25.9%) | Smoking status | |
| ≥0.04 | 23 (28.4%) | Yes | 44 (29.2%) |
| Respondents | No | 107 (70.8%) | |
| Sex | Alcohol consumption | ||
| Men | 72 (47.7%) | Yes | 96 (63.8%) |
| Women | 79 (52.3%) | No | 55 (36.2%) |
| Age | |||
| ≤30 | 22 (14.6%) | ||
| 30–50 | 101 (66.9%) | ||
| ≥50 | 28 (18.5%) |
| Formative Measurement Model | |||||||
| Latent Variables | Indicators | Outer Weight | VIF | Latent Variables | Indicators | Outer Weight | VIF |
| SES | education level | 0.551 * | 1.011 | Air quality | PM2.5 | 0.813 * | 1.039 |
| occupation prestige | 0.508 * | 1.005 | CO2 | 0.385 * | 1.055 | ||
| income level | 0.595 * | 1.009 | HCHO | 0.142 * | 1.050 | ||
| TVOC | 0.218 * | 1.072 | |||||
| Reflective Measurement Model | |||||||
| Latent Variables | Indicators | Outer Loading | Composite Reliability | Discriminant Validity | AVE | ||
| Health | physical functioning | 0.849 | 0.853 | YES | 0.637 | ||
| role physical | 0.677 | ||||||
| bodily pain | 0.545 | ||||||
| general health | 0.564 | ||||||
| vitality | 0.736 | ||||||
| social functioning | 0.491 | ||||||
| role emotional | 0.773 | ||||||
| mental health | 0.565 | ||||||
| Structural Model | |||||||
| Relation | Path Coefficient | VIF | Coefficient of Determination | Predictive Relevance | |||
| IAQ→Health | 0.105 * | 1.136 | 0.305 | 0.283 | |||
| SES→Health | 0.413 * | 1.216 | 0.305 | 0.283 | |||
| SES→IAQ | 0.381 * | 1.272 | 0.220 | 0.110 | |||
| Item | Content | Mean ± SD | |||
|---|---|---|---|---|---|
| PM2.5 (μg/m3) | CO2 (ppm) | TVOC (mg/m3) | HCHO (ug/m3) | ||
| Education | Master, PhD, or specialization (26) | 42.67 ± 20.16 | 954.19 ± 398.83 | 0.23 ± 0.13 | 21.57 ± 13.35 |
| University or Professional (74) | 47.04 ± 28.57 | 986.47 ± 464.41 | 0.23 ± 0.10 | 21.44 ± 11.20 | |
| Middle school or less (51) | 51.35 ± 29.83 | 1100.48 ± 581.42 | 0.33 ± 0.26 | 23.10 ± 15.34 | |
| Income | High (47) | 38.19 ± 25.32 | 897.54 ± 369.73 | 0.23 ± 0.12 | 19.49 ± 13.24 |
| Middle (56) | 42.98 ± 18.80 | 982.74 ± 402.66 | 0.21 ± 0.12 | 25.56 ± 15.43 | |
| Low (48) | 62.71 ± 32.51 | 1180.05 ± 669.20 | 0.35 ± 0.25 | 21.35 ± 10.99 | |
| Occupantion | High (52) | 43.35 ± 22.08 | 928.67 ± 414.64 | 0.23 ± 0.11 | 23.31 ± 14.87 |
| Middle (50) | 49.81 ± 30.19 | 1051.38 ± 475.13 | 0.24 ± 0,10 | 22.42 ± 13.92 | |
| Low (49) | 49.88 ± 30.08 | 1083.10 ± 588.81 | 0.32 ± 0.27 | 21.04 ± 12.20 | |
| Item | Content | SES→Health | IAQ→Health | SES→IAQ |
|---|---|---|---|---|
| Gender | Men | 0.427 | 0.217 | 0.337 |
| Women | 0.318 | 0.114 | 0.304 | |
| Average | 0.373 | 0.166 | 0.321 | |
| SD | 0.055 | 0.052 | 0.017 | |
| Age | ≤30 years | 0.427 | 0.141 | 0.440 |
| 30 ~ 50 years | 0.381 | 0.116 | 0.343 | |
| ≥50 years | 0.405 | 0.210 | 0.295 | |
| Average | 0.404 | 0.156 | 0.359 | |
| SD | 0.023 | 0.040 | 0.060 | |
| Length of residence | <5 years | 0.467 | 0.173 | 0.333 |
| 5–10 years | 0.454 | 0.136 | 0.374 | |
| >10 years | 0.354 | 0.107 | 0.336 | |
| Average | 0.408 | 0.138 | 0.347 | |
| SD | 0.062 | 0.029 | 0.029 | |
| The initial model | 0.413 | 0.105 | 0.381 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Chen, B. The Combined Effect of Indoor Air Quality and Socioeconomic Factors on Health in Northeast China. Appl. Sci. 2020, 10, 2827. https://doi.org/10.3390/app10082827
Chen Y, Chen B. The Combined Effect of Indoor Air Quality and Socioeconomic Factors on Health in Northeast China. Applied Sciences. 2020; 10(8):2827. https://doi.org/10.3390/app10082827
Chicago/Turabian StyleChen, Yu, and Bin Chen. 2020. "The Combined Effect of Indoor Air Quality and Socioeconomic Factors on Health in Northeast China" Applied Sciences 10, no. 8: 2827. https://doi.org/10.3390/app10082827
APA StyleChen, Y., & Chen, B. (2020). The Combined Effect of Indoor Air Quality and Socioeconomic Factors on Health in Northeast China. Applied Sciences, 10(8), 2827. https://doi.org/10.3390/app10082827