
Effectiveness of Combined Stretching and Strengthening Exercise Using Rehabilitation Exercise System with a Linear Actuator and MR Damper on Static and Dynamic Sitting Postural Balance: A Feasibility Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
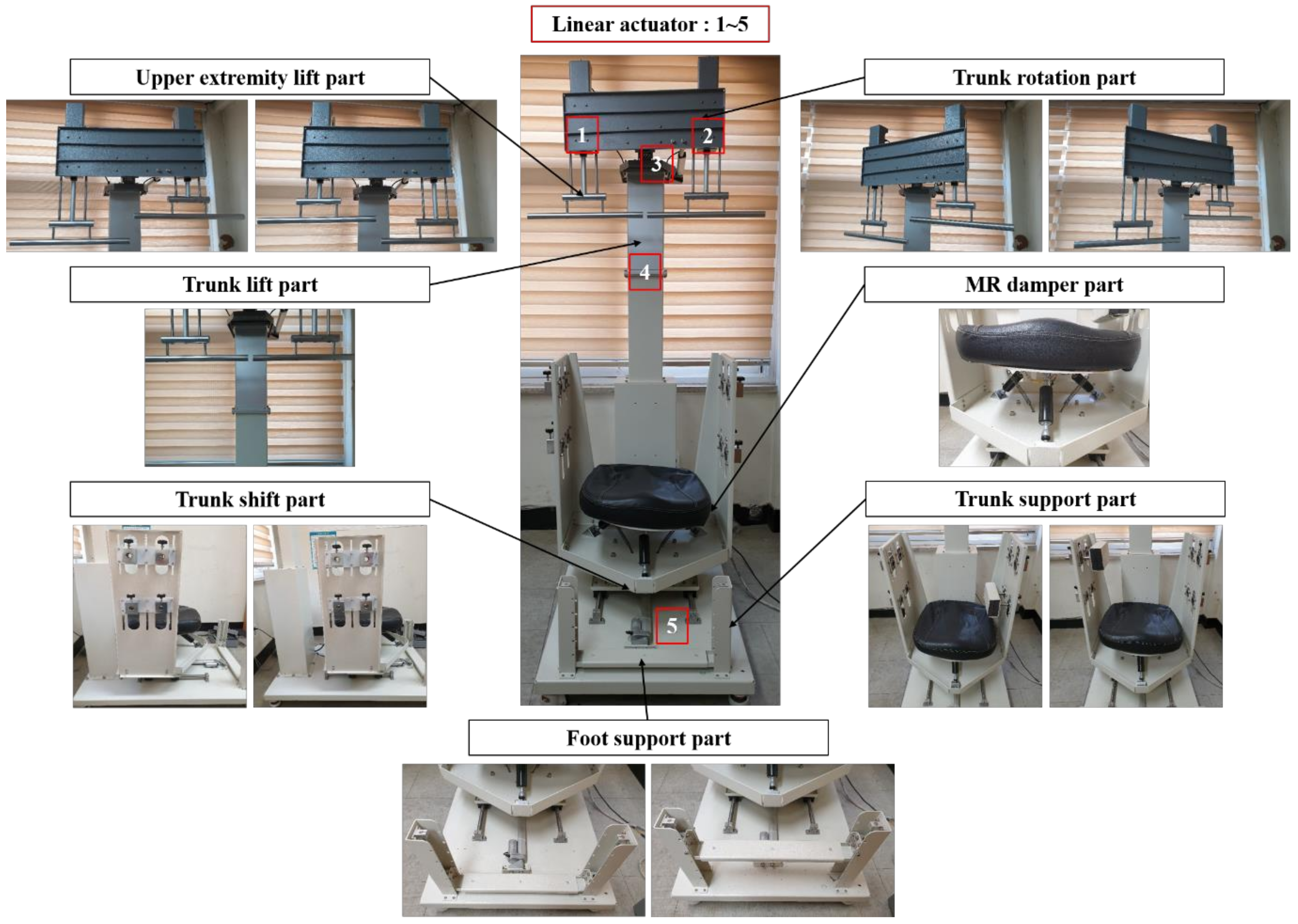
2.2. Rehabilitation Exercise System
- General warm up (5 min): static stretching exercises of chest and back muscles.
- Trunk elongation (1 min, 5 reps): subjects were asked to stretch the trunk as much as possible by elevating the upper extremity lift part, and then keep the maximum position for 10 s.
- Pelvic tilt exercise to the lateral direction (1 min, 3 reps), pelvic tilt exercise to the lateral and anterior direction (1 min, 3 reps), and pelvic tilt exercise to the lateral and posterior direction (1 min, 3 reps): for improving strength and flexibility of the spine, subjects were asked to move slowly until they reached the point of maximum inclination and to keep maximum position for 10 s. Then, subjects moved back slowly to the start point.
- Trunk elongation with pelvic tilt exercise to the lateral direction (2 min, 3 reps), trunk elongation with pelvic tilt exercise to the lateral and anterior direction (2 min, 3 reps), and trunk elongation with pelvic tilt exercise to the lateral and posterior direction (2 min, 3 reps): subjects performed lateral pelvic tilt exercise while maintaining trunk elongation.
- Trunk elongation and rotation with pelvic tilt exercise to the lateral direction (2 min, 3 reps), trunk elongation and rotation with pelvic tilt exercise to the lateral and anterior direction (2 min, 3 reps), trunk elongation and rotation with pelvic tilt exercise to the lateral and posterior direction (2 min, 3 reps): the trunk rotation was performed by rotating the trunk to the left or right side with the trunk rotation part when performing pelvic tilt exercises to the lateral, anterior and posterior direction with trunk elongation.
- General cool down (5 min): static stretching exercises of chest and back muscles.
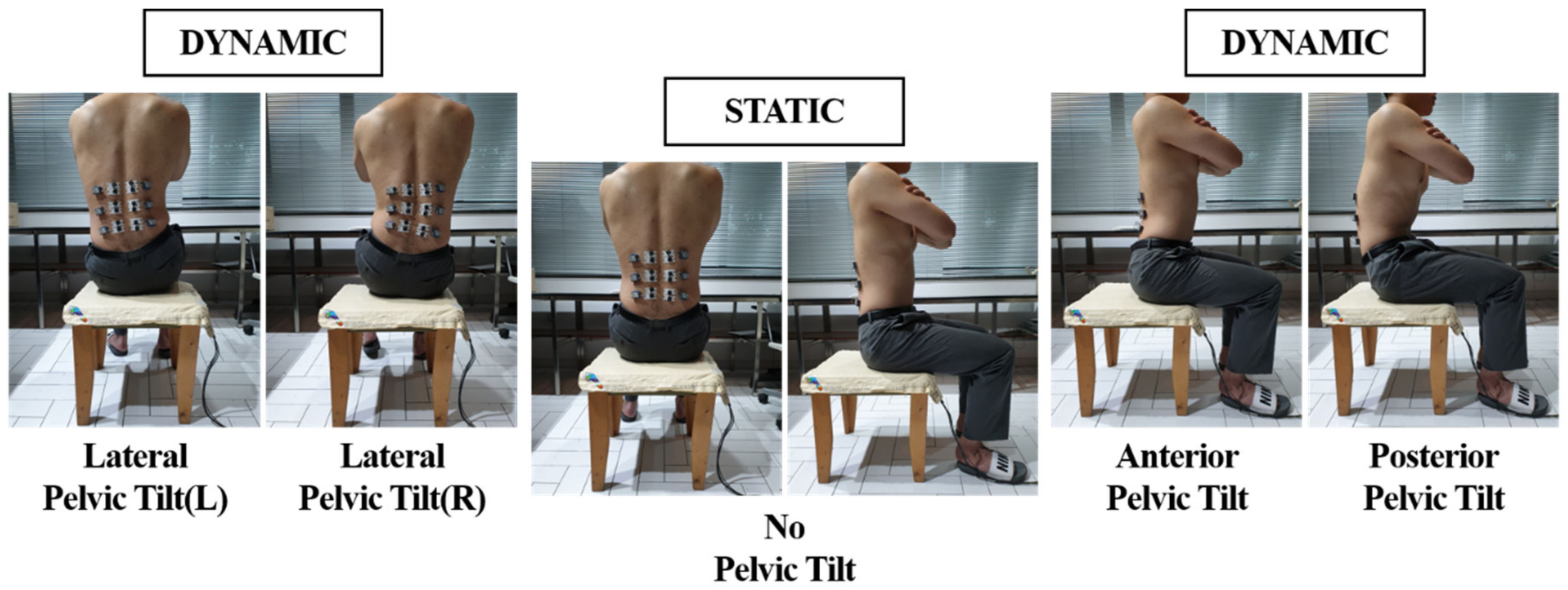
2.3. Experimental Procedure
2.4. Data Analysis
3. Results
3.1. Body Pressure Distribution
3.2. Trunk Muscle Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Godzik, J.G.; Frames, C.W.; Hussain, V.S.; Olson, M.C.; Kakarla, U.K.; Uribe, J.S.; Lockhart, T.E.; Turner, J.D. Postural stability and dynamic balance in adult spinal deformity: Prospective pilot study. World Neurosurg. 2020, 141, e783–e791. [Google Scholar] [CrossRef] [PubMed]
- Matusiak-Wieczorek, E.; Lipert, A.; Kochan, E.; Jegier, A. The time spent sitting does not always mean a low level of physical activity. BMC Public Health 2020, 20, 317. [Google Scholar] [CrossRef] [Green Version]
- Anwary, A.R.; Cetinkaya, D.; Vassallo, M.; Bouchachia, H. Smart-Cover: A real time sitting posture monitoring system. Sens. Actuators A Phys. 2020, 317, 112451. [Google Scholar] [CrossRef]
- Woo, H.S.; Oh, J.C.; Won, S.Y. Effects of asymmetric sitting on spinal balance. J. Phys. Ther. Sci. 2016, 28, 355–359. [Google Scholar] [CrossRef]
- Raichlen, D.A.; Pontzer, H.; Zderic, T.W.; Harris, J.A.; Mabulla, A.Z.P.; Hamilton, M.T.; Wood, B.M. Sitting, squatting, and the evolutionary biology of human inactivity. Proc. Natl. Acad. Sci. USA 2020, 117, 7115–7121. [Google Scholar] [CrossRef]
- Woo, E.H.C.; White, P.; Lai, C.W.K. Musculoskeletal impact of the use of various types of electronic devices on university students in Hong Kong: An evaluation by means of self-reported questionnaire. Man. Ther. 2016, 26, 47–53. [Google Scholar] [CrossRef]
- Waongenngarm, P.; Rajaratnam, B.S.; Janwantanakul, P. Perceived body discomfort and trunk muscle activity in three prolonged sitting postures. J. Phys. Ther. Sci. 2015, 27, 2183–2187. [Google Scholar] [CrossRef] [Green Version]
- Nakphet, N.; Chaikumarn, M.; Janwantanakul, P. Effect of different types of rest-break interventions on neck and shoulder muscle activity, perceived discomfort and productivity in symptomatic VDU operators: A randomized controlled trial. Int. J. Occup. Saf. Ergon. 2014, 20, 339–353. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.S.; Jung, J.H.; In, T.S.; Cho, H.Y. Effects of prolonged sitting with slumped posture on trunk muscular fatigue in adolescent with and without chronic lower back pain. Medicina 2021, 57, 3. [Google Scholar] [CrossRef]
- Tomita, Y.; Suzuki, Y.; Tanaka, Y.; Hasegawa, Y.; Yoshihara, Y.; Okura, K.; Matsuka, Y. Effects of sitting posture and jaw clenching on neck and trunk muscle activities during typing. J. Oral Rehabil. 2021, 48, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Korhan, O. Work-related musculoskeletal discomfort in the shoulder due to computer use. In Ergonomics—A Systems Approach; Isabel, L.N., Ed.; IntechOpen: London, UK, 2012; Volume 2, pp. 31–50. [Google Scholar] [CrossRef]
- Picelli, A.; Mazzocco, G.; Smania, N. Trunk posture adaptations during sitting on dynamic stool: A validation study. Appl. Sci. 2020, 10, 7567. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H.; Park, J.; Jee, K.K.; Lim, J.A.; Park, M.C. Real-time sitting posture correction system based on highly durable and washable electronic textile pressure sensors. Sens. Actuators A Phys. 2018, 269, 394–400. [Google Scholar] [CrossRef]
- Roh, J.; Hyeong, J.; Kim, S. Estimation of various sitting postures using a load-cell-driven monitoring system. Int. J. Ind. Ergon. 2019, 74, 102837. [Google Scholar] [CrossRef]
- Larson, C.A.; Tezak, W.D.; Malley, M.S.; Thornton, W. Assessment of postural muscle strength in sitting: Reliability of measures obtained with hand-held dynamometry in individuals with spinal cord injury. J. Neurol. Phys. Ther. 2010, 34, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.Y.; Heo, M.; Kim, J.J. Effects of a personalized exercise rehabilitation device on dynamic postural balance for scoliotic patients: A feasibility study. Electronics 2020, 9, 2100. [Google Scholar] [CrossRef]
- Smidt, N.; de Vet, H.C.W.; Bouter, L.M.; Dekker, J. Effectiveness of exercise therapy: A best-evidence summary of systematic reviews. Aust. J. Physiother. 2005, 51, 71–85. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.A.F.; Serpa, Y.R.; Macedo, D.V.; Sousa, E.S. A serious game to practice stretches and exercises for a correct and healthy posture. Entertain Comput. 2018, 28, 78–88. [Google Scholar] [CrossRef]
- Hrysomallis, C.; Goodman, C. A review of resistance exercise and posture realignment. J. Strength Cond. Res. 2001, 15, 385–390. [Google Scholar]
- Drzał-Grabiec, J.; Sneal, S.; Rykała, J.; Podgórska, J.; Truszczyńska, A. The influence of elongation exercises on the anterior-posterior spine curvatures. Biomed. Hum. Kinet. 2018, 6, 1–4. [Google Scholar] [CrossRef]
- Rigo, M.; Reiter, C.; Weiss, H.R. Effect of conservative management on the prevalence of surgery in patients with adolescent idiopathic scoliosis. Pediatr. Rehabil. 2003, 6, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.D.; Jolly, M.R. MR fluid, foam and elastomer devices. Mechatronics 2000, 10, 555–569. [Google Scholar] [CrossRef]
- Yassierli, Y.; Juraida, A. Effects of netbook and tablet usage postures on the development of fatigue, discomfort and pain. J. Eng. Technol. Sci. 2016, 48, 243–253. [Google Scholar] [CrossRef] [Green Version]
- Keawduangdee, P.; Puntumetakul, R.; Swangnetr, M.; Laohasiriwong, W.; Settheetham, D.; Yamauchi, J.; Boucaut, R. Prevalence of low back pain and associated factors among farmers during the rice transplanting process. J. Phys. Ther. Sci. 2015, 27, 2239–2245. [Google Scholar] [CrossRef] [Green Version]
- Yildirim, Y.; Gunay, S.; Karadibak, D. Identifying factors associated with low back pain among employees working at a package producing industry. J. Back Musculoskelet. Rehabil. 2014, 27, 25–32. [Google Scholar] [CrossRef]
- Kuukkanen, T.; Mälkiä, E. Effects of a three-month therapeutic exercise programme on flexibility in subjects with low back pain. Physiother. Res. Int. 2000, 5, 46–61. [Google Scholar] [CrossRef]
- Dong, S.; Lu, K.Q.; Sun, J.Q.; Rudolph, K. Rehabilitation device with variable resistance and intelligent control. Med. Eng. Phys. 2005, 27, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Kavanagh, J.; Barrett, R.; Morrison, S. The role of the neck and trunk in facilitating head stability during walking. Exp. Brain Res. 2006, 172, 454. [Google Scholar] [CrossRef]
- Czaprowski, D.; Stoliński, Ł.; Tyrakowski, M.; Kozinoga, M.; Kotwicki, T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis Spinal Disord. 2018, 13, 6. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, D.A.; Moseley, G.L.; Hodges, P.W. The lumbar multifidus: Does the evidence support clinical beliefs? Man. Ther. 2006, 11, 254–263. [Google Scholar] [CrossRef]
- Caneiro, J.P.; O’Sullivan, P.; Burnett, A.; Barach, A.; O’Neil, D.; Tveit, O.; Olafsdottir, K. The influence of different sitting postures on head/neck posture and muscle activity. Man. Ther. 2010, 15, 54–60. [Google Scholar] [CrossRef]
- O’Sullivan, P.B.; Grahamslaw, K.M.; Kendell, M.; Lapenskie, S.C.; Möller, N.E.; Richards, K.V. The effect of different standing and sitting postures on trunk muscle activity in a pain-free population. Spine 2002, 27, 1238–1244. [Google Scholar] [CrossRef]
- Lee, D.; Yu, S.; Song, S.; Lee, S.H.; An, S.; Cho, H.Y.; Cho, K.H.; Lee, G. Comparison of trunk electromyographic muscle activity depends on sitting postures. Work 2017, 56, 491–495. [Google Scholar] [CrossRef]
- Farahpour, N.; Younesian, H.; Bahrpeyma, F. Electromyographic activity of erector spinae and external oblique muscles during trunk lateral bending and axial rotation in patients with adolescent idiopathic scoliosis and healthy subjects. Clin. Biomech. 2015, 30, 411–417. [Google Scholar] [CrossRef]
- Guo, L.Y.; Wang, Y.L.; Huang, Y.H.; Yang, C.H.; Hou, Y.Y.; Harn, H.I.C.; You, Y.L. Comparison of the electromygraphic activation level and unilateral selectivity of erector spinae during different selected movements. Int. J. Rehabil. Res. 2012, 35, 345–351. [Google Scholar] [CrossRef]
- Wattananon, P.; Silfies, S.P.; Tretriluxana, J.; Jalayondeja, W. Lumbar multifidus and erector spinae muscle synergies in patients with nonspecific low back pain during prone hip extension: A cross-sectional study. PM&R 2019, 11, 694–702. [Google Scholar] [CrossRef]
- Masaki, M.; Ji, X.; Yamauchi, T.; Tateuchi, H.; Ichihashi, N. Effects of the trunk position on muscle stiffness that reflects elongation of the lumbar erector spinae and multifidus muscles: An ultrasonic shear wave elastography study. Eur. J. Appl. Physiol. 2019, 119, 1085–1091. [Google Scholar] [CrossRef]
- Nelson, R.T.; Bandy, W.D. Eccentric training and static stretching improve hamstring flexibility of high school males. J. Athl. Train. 2004, 39, 254–258. [Google Scholar]
- Song, G.B.; Kim, J.K.; Park, E.C. The effect of Swiss ball exercise and resistance exercise on balancing ability of scoliosis patients. J. Phys. Ther. Sci. 2015, 27, 3879–3882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, K.H.; Oh, J.S.; An, D.H.; Yoo, W.G.; Kim, J.M.; Kim, T.H. Difference in selective muscle activity of thoracic erector spinae during prone trunk extension exercise in subjects with slouched thoracic posture. PM&R 2014, 7, 479–484. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Conditions | Body Pressure Distribution | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean force (N) | DS | NDS | p a | p b | p c | |||
| Static | NPT | BF | 144.6 ± 38.3 | 113.1 ± 34.2 | 0.001 | 0.000 | 0.073 | |
| AF | 121.6 ± 31.9 | 106.5 ± 28.2 | 0.056 | |||||
| Dynamic | LPT | BF | 297.7 ± 45.8 | 228.4 ± 46.2 | 0.000 | 0.000 | 0.000 | |
| AF | 274.0 ± 39.3 | 259.5 ± 44.8 | 0.188 | |||||
| APT | BF | 235.4 ± 43.7 | 177.4 ± 41.7 | 0.000 | 0.000 | 0.000 | ||
| AF | 210.2 ± 40.9 | 201.8 ± 37.2 | 0.404 | |||||
| PPT | BF | 236.7 ± 37.1 | 167.9 ± 39.1 | 0.000 | 0.003 | 0.000 | ||
| AF | 215.1 ± 40.7 | 199.2 ± 37.0 | 0.121 | |||||
| Mean pressure (kPa) | Static | NPT | BF | 4.1 ± 0.9 | 3.4 ± 1.0 | 0.006 | 0.160 | 0.405 |
| AF | 3.8 ± 1.0 | 3.5 ± 1.2 | 0.254 | |||||
| Dynamic | LPT | BF | 7.7 ± 1.4 | 5.8 ± 1.3 | 0.000 | 0.344 | 0.000 | |
| AF | 7.4 ± 1.3 | 7.0 ± 1.4 | 0.254 | |||||
| APT | BF | 6.0 ± 1.1 | 4.5 ± 1.2 | 0.000 | 0.096 | 0.000 | ||
| AF | 5.6 ± 1.1 | 5.4 ± 1.1 | 0.463 | |||||
| PPT | BF | 6.1 ± 1.0 | 4.3 ± 1.0 | 0.000 | 0.282 | 0.000 | ||
| AF | 5.8 ± 1.2 | 5.4 ± 1.1 | 0.158 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.-Y.; Yang, C.-M.; Kim, J.-J. Effectiveness of Combined Stretching and Strengthening Exercise Using Rehabilitation Exercise System with a Linear Actuator and MR Damper on Static and Dynamic Sitting Postural Balance: A Feasibility Study. Appl. Sci. 2021, 11, 7329. https://doi.org/10.3390/app11167329
Jung J-Y, Yang C-M, Kim J-J. Effectiveness of Combined Stretching and Strengthening Exercise Using Rehabilitation Exercise System with a Linear Actuator and MR Damper on Static and Dynamic Sitting Postural Balance: A Feasibility Study. Applied Sciences. 2021; 11(16):7329. https://doi.org/10.3390/app11167329
Chicago/Turabian StyleJung, Ji-Yong, Chang-Min Yang, and Jung-Ja Kim. 2021. "Effectiveness of Combined Stretching and Strengthening Exercise Using Rehabilitation Exercise System with a Linear Actuator and MR Damper on Static and Dynamic Sitting Postural Balance: A Feasibility Study" Applied Sciences 11, no. 16: 7329. https://doi.org/10.3390/app11167329