
Quality Control in Dental Cone-Beam Computed Tomography


Abstract
:1. Introduction
2. Parameters and Methods
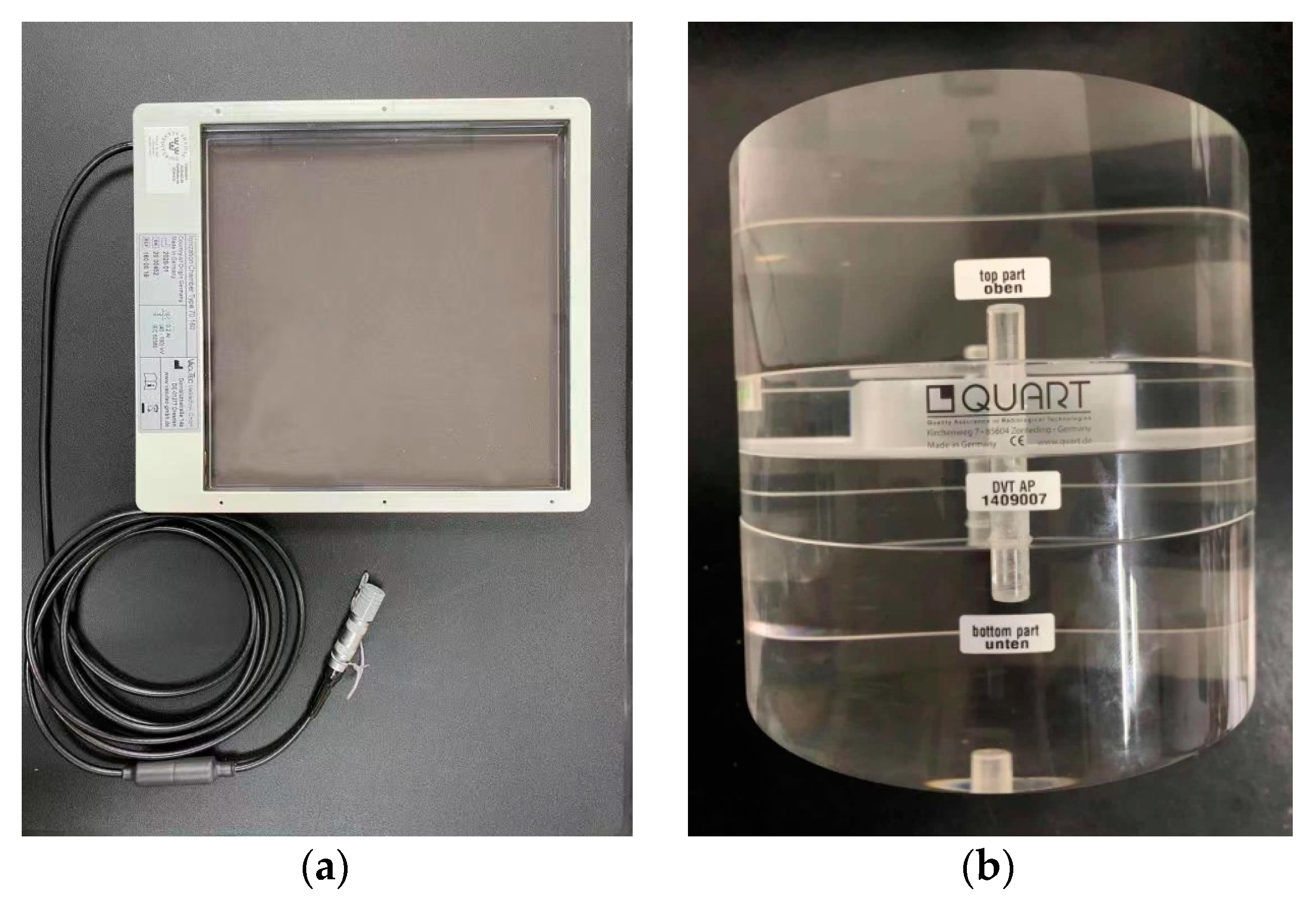
2.1. Experimental Setup
2.2. KAP
2.3. Spatial Resolution
- (1)
- Data acquisition
- (2)
- Finding the differential
- (3)
- Setting the limits
- (4)
- Fourier transform
- (5)
- Averaging
- (6)
- Plotting
2.4. Contrast-to-Noise Ratio Index (CNRI)
2.5. Uniformity Index
3. Results
- (1)
- The KAP normalized to the FOV 16 cm2 (the FOV was 4 cm × 4 cm) should not be larger than 250 mGy·cm2.
- (2)
- The spatial resolution defined by the 10% point of MTF should not be lower than 1 Lp/mm.
- (3)
- CNRI should be less than 20%.
- (4)
- The uniformity index should be larger than five.
4. Discussions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Abella, F.; Patel, S.; Durán-Sindreu, F.; Mercade, M.; Bueno, R.; Roig, M. An evaluation of the periapical status of teeth with necrotic pulps using periapical radiography and cone-beam computed tomography. Int. Endod. J. 2013, 47, 387–396. [Google Scholar] [CrossRef]
- Giudice, R.L.; Nicita, F.; Puleio, F.; Alibrandi, A.; Pantaleo, G. Accuracy of Periapical Radiography and CBCT in Endodontic Evaluation. Int. J. Dent. 2018, 2, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornstein, M.M.; Lauber, R.; Sendi, P.; Von Arx, T. Comparison of Periapical Radiography and Limited Cone-Beam Computed Tomography in Mandibular Molars for Analysis of Anatomical Landmarks before Apical Surgery. J. Endod. 2011, 37, 151–157. [Google Scholar] [CrossRef]
- De Paula-Silva, F.W.G.; Wu, M.K.; Leonardo, M.R.; da Silva, L.A.B.; Wesselink, P.R. Accuracy of periapical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. J. Endod. 2009, 35, 1009–1012. [Google Scholar] [CrossRef] [PubMed]
- Balasundaram, A.; Shah, P.; Hoen, M.M.; Wheater, M.A.; Bringas, J.S.; Gartner, A.; Geist, J.R. Comparison of Cone-Beam Computed Tomography and Periapical Radiography in Predicting Treatment Decision for Periapical Lesions: A Clinical Study. Int. J. Dent. 2012, 2012, 920815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moura, M.S.; Guedes, O.A.; De Alencar, A.H.G.; Azevedo, B.C.; Estrela, C. Influence of Length of Root Canal Obturation on Apical Periodontitis Detected by Periapical Radiography and Cone Beam Computed Tomography. J. Endod. 2009, 35, 805–809. [Google Scholar] [CrossRef] [PubMed]
- Naitoh, M.; Yamada, S.; Noguchi, T.; Ariji, E.; Nagao, J.; Mori, K.; Kitasaka, T.; Suenaga, Y. Three-dimensional display with quantitative analysis in alveolar bone resorption using cone-beam computerized tomography for dental use: A preliminary study. Int. J. Periodontics Restor. Dent. 2006, 26, 607–612. [Google Scholar]
- Hassan, B.; Metska, M.E.; Ozok, A.R.; van der Stelt, P.; Wesselink, P.R. Detection of Vertical Root Fractures in Endodontically Treated Teeth by a Cone Beam Computed Tomography Scan. J. Endod. 2009, 35, 719–722. [Google Scholar] [CrossRef] [PubMed]
- Estrela, C.; Bueno, M.R.; Leles, C.R.; Azevedo, B.; Azevedo, J.R. Accuracy of Cone Beam Computed Tomography and Panoramic and Periapical Radiography for Detection of Apical Periodontitis. J. Endod. 2008, 34, 273–279. [Google Scholar] [CrossRef]
- Misch, K.A.; Yi, E.S.; Sarment, D.P. Accuracy of Cone Beam Computed Tomography for Periodontal Defect Measurements. J. Periodontol. 2006, 77, 1261–1266. [Google Scholar] [CrossRef]
- Amoore, J. Quality improvement report: Learning from adverse incidents involving medical devices. BMJ 2002, 325, 272–275. [Google Scholar] [CrossRef]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.A.B. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Tammisalo, E.; Iwai, K.; Hashimoto, K.; Shinoda, K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac. Radiol. 1999, 28, 245–248. [Google Scholar] [CrossRef]
- Pauwels, R.; Stamatakis, H.; Manousaridis, G.; Walker, A.; Michielsen, K.; Bosmans, H.; Bogaerts, R.; Jacobs, R.; Horner, K.; Tsiklakis, K.; et al. Development and applicability of a quality control phantom for dental cone-beam CT. J. Appl. Clin. Med. Phys. 2011, 12, 3478. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R. CBCT Quality Assurance. In Maxillofacial Cone Beam Computed Tomography; Springer: Berlin/Heidelberg, Germany, 2017; pp. 213–226. [Google Scholar]
- SEDENTEXCT. Radiation Protection: Cone Beam CT for Dental and Maxillofacial Radiology, Evidence Based Guidelines 2011 (v2.0 Final). 2011. Available online: http://www.sedentexct.eu/files/guidelines_final.pdf (accessed on 31 August 2021).
- Du, L.Y.; Umoh, J.; Nikolov, H.N.; Pollmann, S.I.; Lee, T.-Y.; Holdsworth, D.W. A quality assurance phantom for the performance evaluation of volumetric micro-CT systems. Phys. Med. Biol. 2007, 52, 7087–7108. [Google Scholar] [CrossRef]
- Daly, M.J.; Siewerdsen, J.H.; Moseley, D.J.; Jaffray, D.A.; Irish, J.C. Intraoperative cone-beam CT for guidance of head and neck surgery: Assessment of dose and image quality using a C-arm prototype. Med. Phys. 2006, 33, 3767–3780. [Google Scholar] [CrossRef]
- Deutsches Institut für Normung (DIN). Sicherung der Bildqualität in Röntgendiagnostischen Betrieben—Teil 161: Abnahmeprüfung nach RöV an Zahnmedizinischen Röntgeneinrichtungen zur Digitalen Volumentomographie; Rep. No. 6868-161; DIN: Berlin, Germany, 2013. [Google Scholar]
- Gala, H.D.L.H.; Torresin, A.; Dasu, A.; Rampado, O.; Delis, H.; Girón, I.H.; Theodorakou, C.; Andersson, J.; Holroyd, J.; Nilsson, M.; et al. Quality control in cone-beam computed tomography (CBCT) EFOMP-ESTRO-IAEA protocol (summary report). Phys. Med. 2017, 39, 67–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Electrotechnical Commission (IEC). Evaluation and Routine Testing in Medical Imaging Departments—Part 3–5: Acceptance Tests—Imaging Performance of Computed Tomography X-Ray Equipment; IEC Report No. 61223-3-5; IEC: Geneva, Switzerland, 2004. [Google Scholar]
- Larsson, J.P.; Persliden, J.; Sandborg, M.; Carlsson, G.A. Transmission ionization chambers for measurements of air collision kerma integrated over beam area. Factors limiting the accuracy of calibration. Phys. Med. Biol. 1996, 41, 2381–2398. [Google Scholar] [CrossRef] [PubMed]
- International Atomic Energy Agency. Dosimetry in Diagnostic Radiology: An International Code of Practice; Technical Reports Series No. 457; IAEA: Vienna, Austria, 2007. [Google Scholar]
- Judy, P.F. The line spread function and modulation transfer function of a computed tomographic scanner. Med. Phys. 1976, 3, 233–236. [Google Scholar] [CrossRef]
- Maidment Andrew, D.A.; Albert, M. Conditioning data for calculation of the modulation transfer function. Med. Phys. 2003, 30, 2. [Google Scholar] [CrossRef] [PubMed]
- Rossmann, K. Point spread-function, line spread-function, and modulation transfer function. Tools for the study of imaging systems. Radiology 1969, 93, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Thilander-Klang, A.; Ledenius, K.; Hansson, J.; Sund, P.; Båth, M. Evaluation of subjective assessment of the low-contrast visibility in constancy control of computed tomography. Radiat. Prot. Dosim. 2010, 139, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Steiding, C.; Kolditz, D.; Kalender, W.A. A quality assurance framework for the fully automated and objective evaluation of image quality in cone-beam computed tomography. Med. Phys. 2014, 41, 031901. [Google Scholar] [CrossRef] [PubMed]
- Dixon, R.; Anderson, J.; Bakalyar, D.; Boedeker, K.; Boone, J.; Cody, D.; Fahrig, R.; Jaffray, D.; Kyprianou, I.; McCollough, C.; et al. Comprehensive Methodology for the Evaluation of Radiation Dose in X-Ray Computed Tomography. In Comprehensive Methodology for the Evaluation of Radiation Dose in X-ray Computed Tomography; American Association of Physicists in Medicine (AAPM): Alexandria, VA, USA, 2010. [Google Scholar]
- International Atomic Energy Agency (IAEA). Status of Computed Tomography Dosimetry for Wide Cone Beam Scanners; Rep. No. 5; IAEA: Vienna, Austria, 2011. [Google Scholar]
- Droege, R.T.; Morin, R.L. A practical method to measure the MTF of CT scanners. Med. Phys. 1982, 9, 758–760. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.-J.P.; Beck, T.J.; Borras, C.; Cohen, G.; Jucius, R.A.; Kriz, R.J.; Nickoloff, E.L.; Rothenberg, L.N.; Strauss, K.J.; Villafana, T. AAPM Task Group Report No 39: Specification and Acceptance Testing of Computed Tomography Scanners; American Association of Physicists in Medicine: New York, NY, USA, 1993. [Google Scholar]
- Chiarot, C.B.; Siewerdsen, J.H.; Haycocks, T.; Moseley, D.J.; Jaffray, D.A. An innovative phantom for quantitative and qualitative investigation of advanced x-ray imaging technologies. Phys. Med. Biol. 2005, 50, N287–N297. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Site | Manufacturer | Model | Settings | Measurements/mGy·cm2 | |
|---|---|---|---|---|---|---|
| kV | mAs | |||||
| 1 | Shenyang Shenhe Dental Clinic | Kavo | Kavo3Dexam | 120 | 30.89 | 54.9 |
| 2 | Stomatological Hospital, Jilin University | Carestream | CS9300 | 90 | 56.5 | 105.3 |
| 3 | Heilongjiang Oral Disease Prevention and Treatment Institute | Kavo | Kavo3Dexam | 120 | 37.07 | 77.4 |
| 4 | Shanghai Xinhua Hospital | Kavo | Kavo3Dexam | 120 | 30.89 | 65.5 |
| 5 | Shanghai Huashan Hospital | Kavo | Kavo3Dexam | 110 | 30.5 | 78.9 |
| 6 | Beijing Jinsong Dental Clinic | Sirona | Galileos | 85 | 21 | 39.6 |
| 7 | Nanjing Stomatological Hospital | Kavo | Kavo3Dexam | 120 | 36.07 | 75.3 |
| 8 | Jiangsu Provincial Stomatological Hospital | Kavo | Kavo3Dexam | 120 | 36.12 | 75.5 |
| 9 | Shenyang Stomatological Hospital | Kavo | Kavo3Dexam | 120 | 30.76 | 54.6 |
| 10 | China Medical University School&Hospital of Stomatology | Newtom | NewTom VG | AutomaticExposure Control | / | Not applicable |
| Action level | KAP larger than 250 mGy·cm2 | |||||
| No. | Site | Manufacturer | Model | Spatial Resolution/(Lp/mm) | Uniformity Index | CNI /(%) |
|---|---|---|---|---|---|---|
| 1 | Shenyang Shenhe Dental Clinic | Kavo | Kavo3Dexam | 1.52 | 23 | 6.718 |
| 2 | China Medical University School&Hospital of Stomatology | Newtom | NewTom VG | 1.21 | 36 | 5.432 |
| 3 | Stomatological Hospital, Jilin University | Carestream | CS9300 | 1.49 | 25 | 7.015 |
| 4 | Heilongjiang Oral Disease Prevention and Treatment Institute | Kavo | Kavo3Dexam | 1.62 | 24 | 6.892 |
| 5 | Shanghai Xinhua Hospital | Kavo | Kavo3Dexam | 1.57 | 26 | 6.810 |
| 6 | Shanghai Huashan Hospital | Kavo | Kavo3Dexam | 1.61 | 23 | 6.975 |
| 7 | Beijing Jinsong Dental Clinic | Sirona | Galileos | 1.34 | 19 | 5.331 |
| 8 | Nanjing Stomatological Hospital | Kavo | Kavo3Dexam | 1.53 | 21 | 7.112 |
| 9 | Jiangsu Provincial Stomatological Hospital | Kavo | Kavo3Dexam | 1.56 | 23 | 6.962 |
| 10 | Shenyang Stomatological Hospital | Kavo | Kavo3Dexam | 1.52 | 27 | 6.773 |
| Action level | <1 | ≤5 | ≥20 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.-F.; Chen, X.-Z.; Wang, H. Quality Control in Dental Cone-Beam Computed Tomography. Appl. Sci. 2021, 11, 8162. https://doi.org/10.3390/app11178162
Huang J-F, Chen X-Z, Wang H. Quality Control in Dental Cone-Beam Computed Tomography. Applied Sciences. 2021; 11(17):8162. https://doi.org/10.3390/app11178162
Chicago/Turabian StyleHuang, Jin-Feng, Xiao-Zhao Chen, and Hong Wang. 2021. "Quality Control in Dental Cone-Beam Computed Tomography" Applied Sciences 11, no. 17: 8162. https://doi.org/10.3390/app11178162