
Canal Transportation and Volumetric Dentin Removal Abilities of Ni-Ti Rotary File Systems in Curved Primary Root Canals: CBCT Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Selection and Preparation of Specimens
2.3. Preoperative CBCT Investigation of Specimens
2.4. Determination of Groups
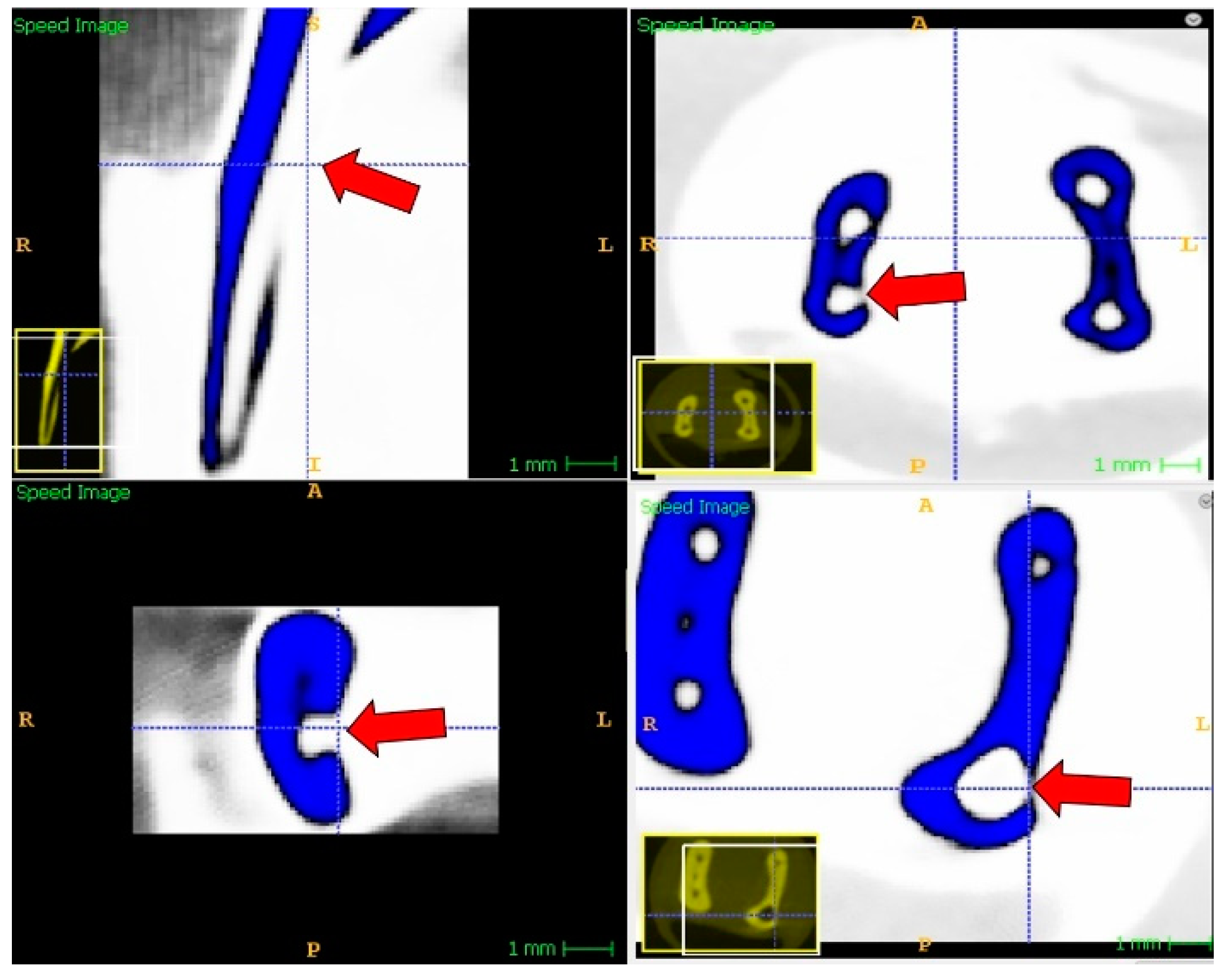
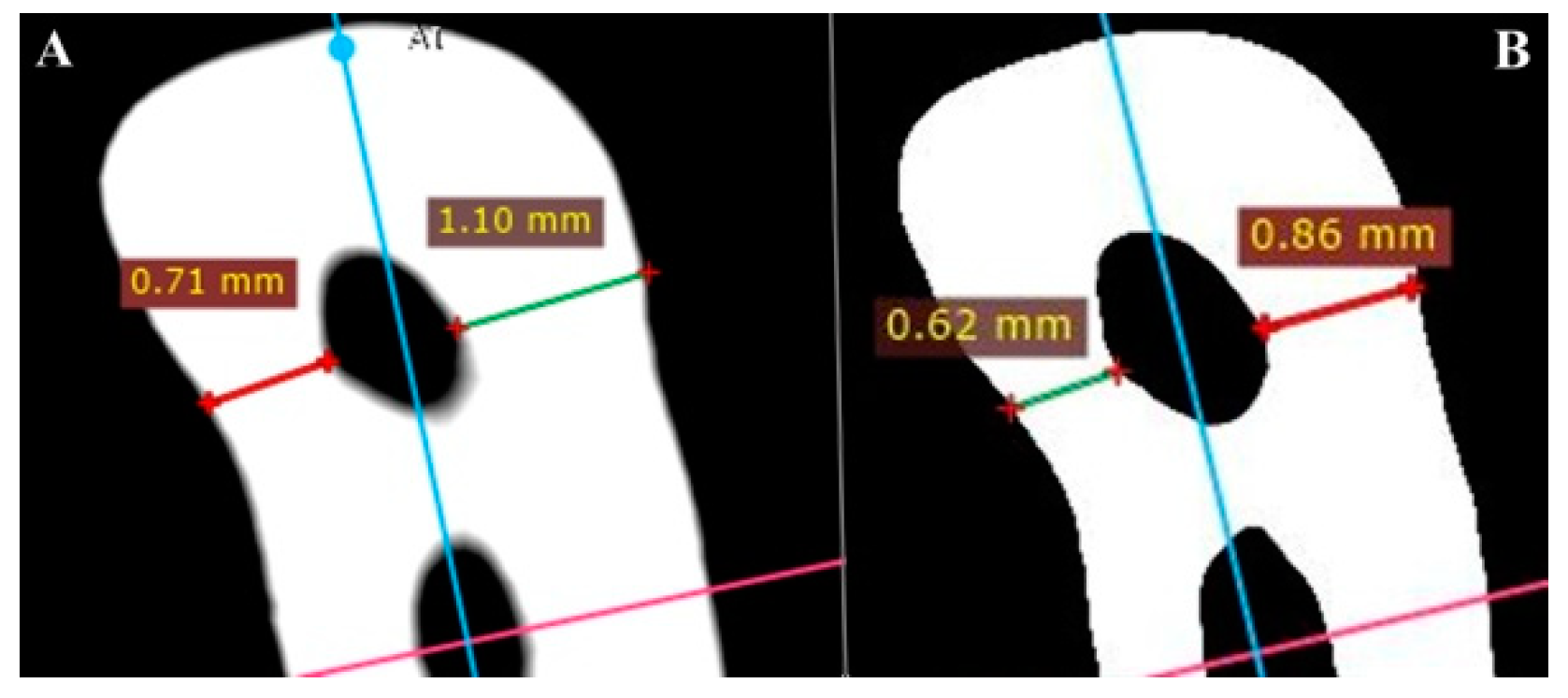
2.5. Postoperative CBCT Investigation of Specimens and the Determination of Canal Transportation
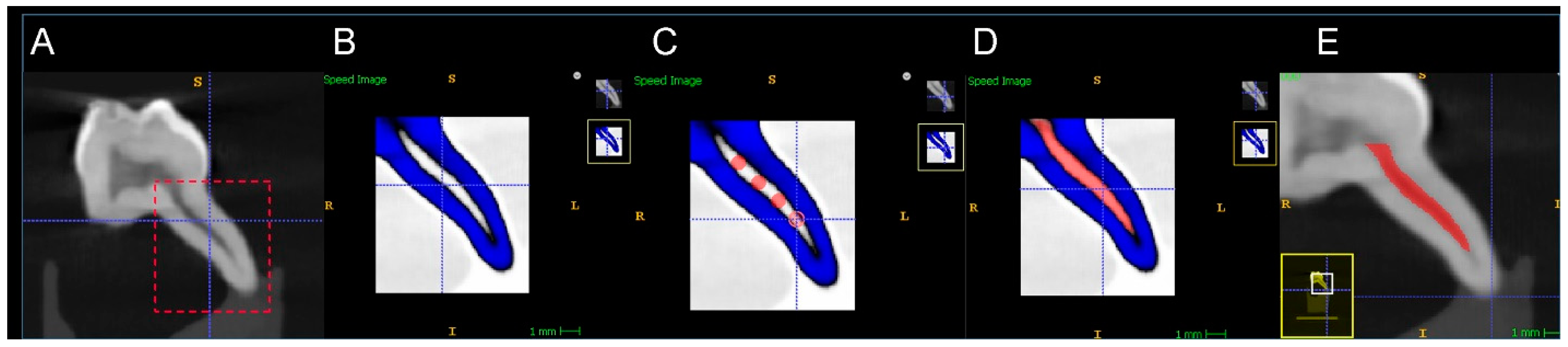
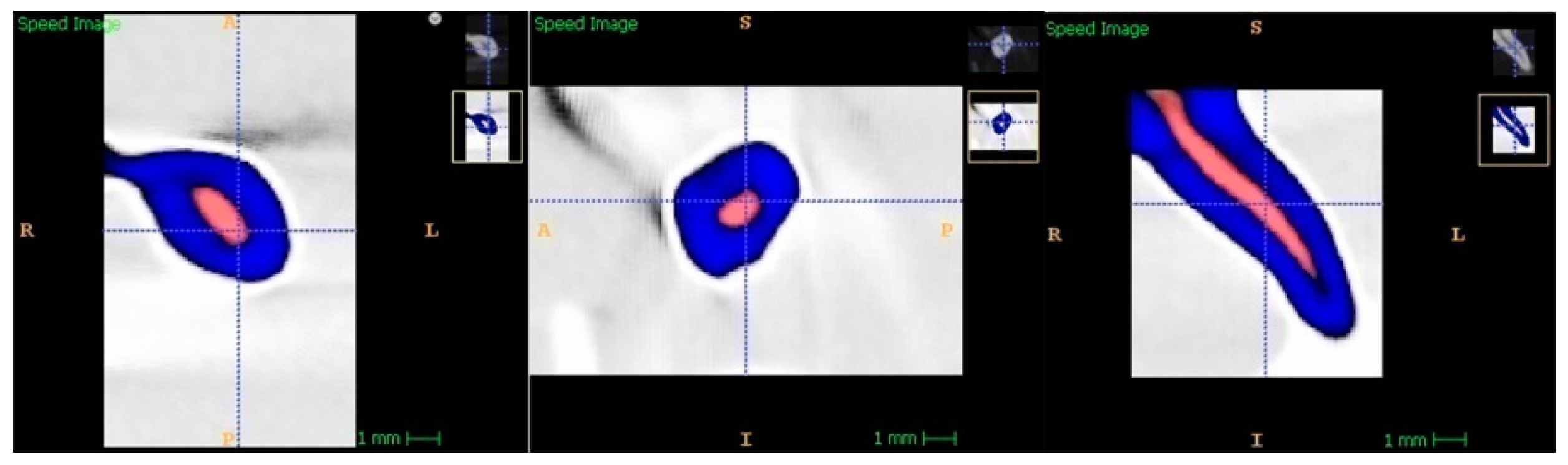
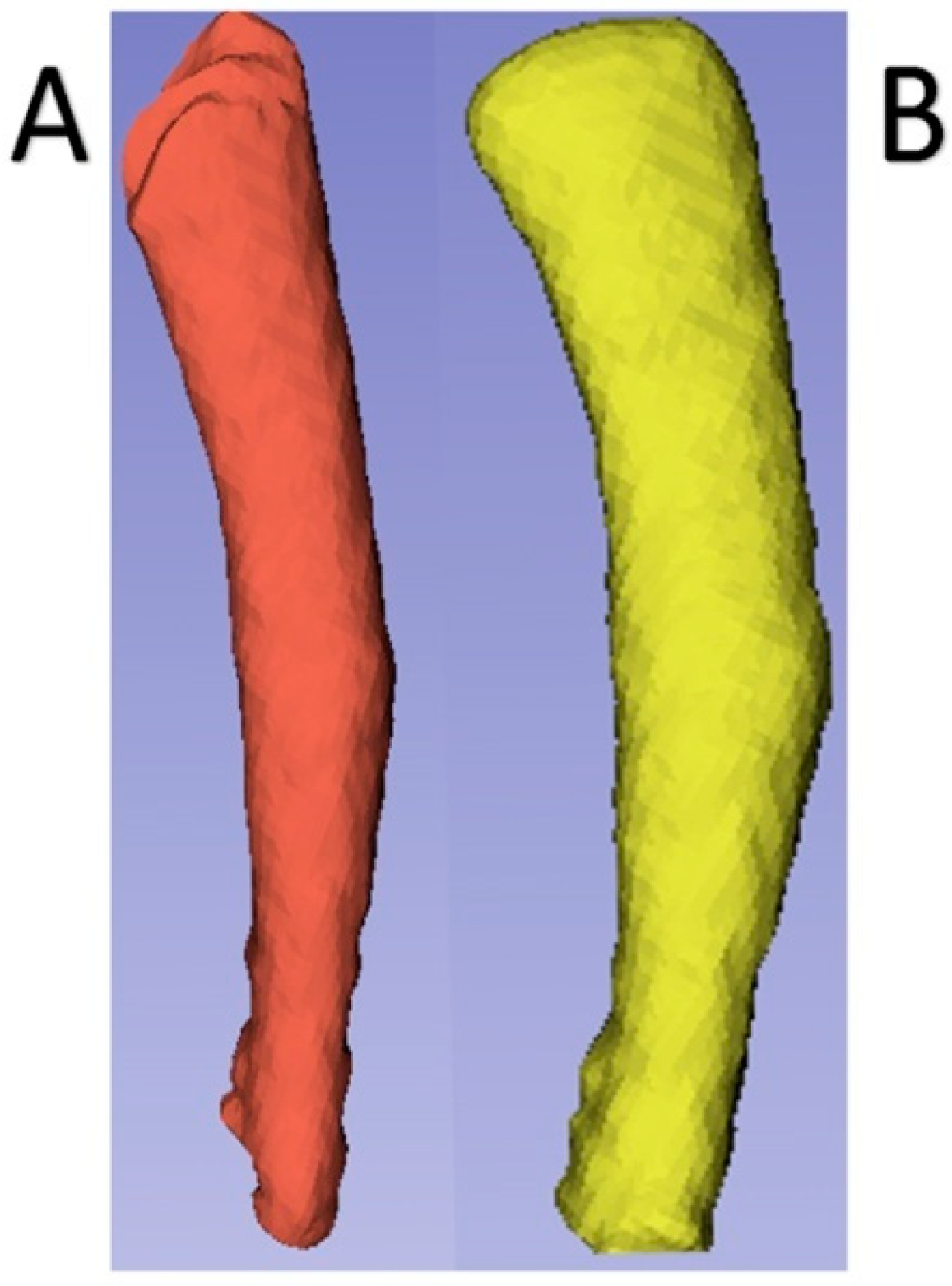
2.6. Volumetric Determination of Dentin Removal
2.7. Statistical Analysis
3. Results
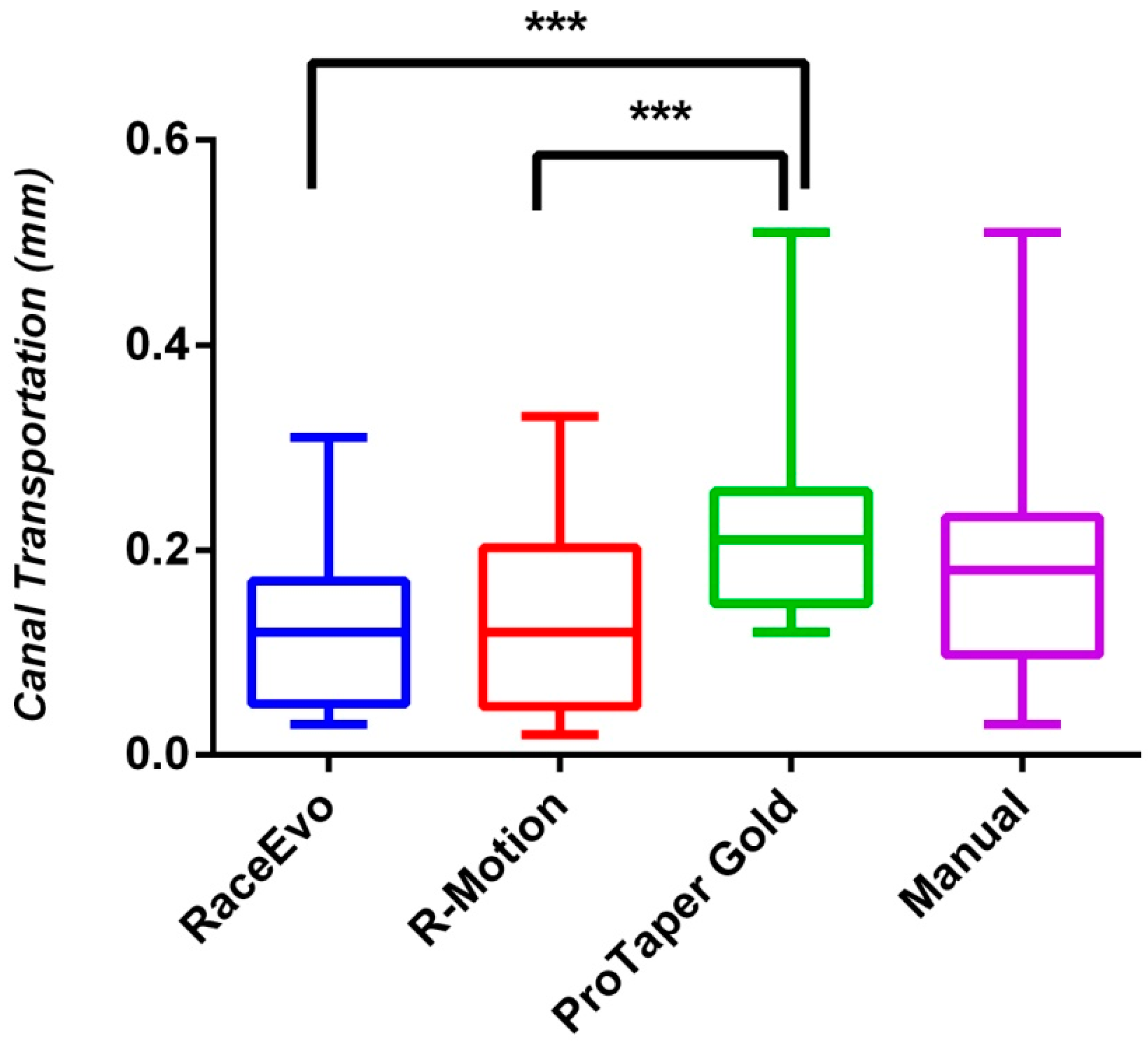
3.1. Assessment of Canal Transportation
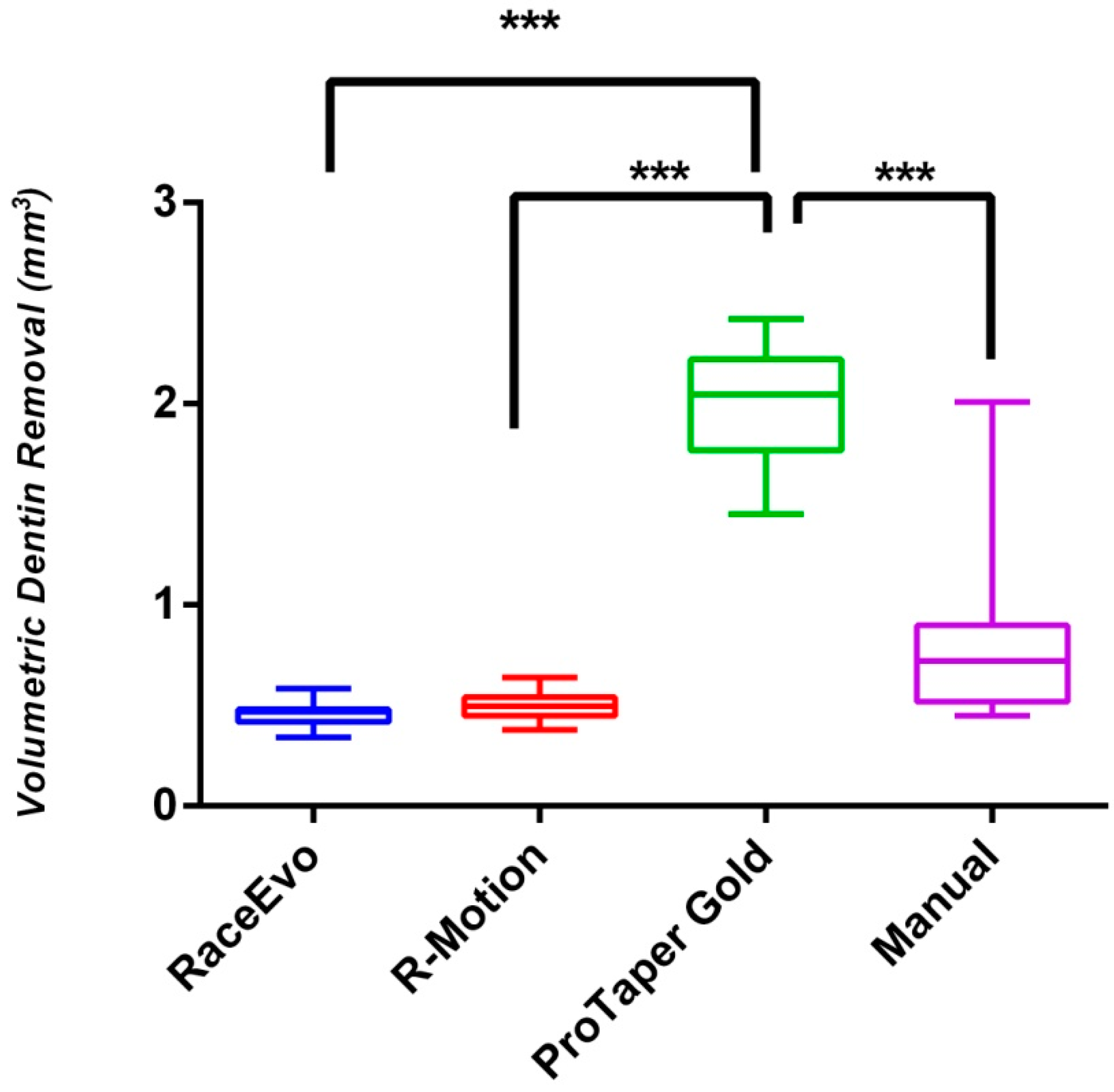
3.2. Assessment of Volumetric Dentin Removal
4. Discussion
- The presence of beam hardening, cupping, and doming artifacts;
- Divergence of the X-ray beam;
- Axial slice variability due to different masses of each slice;
- High image noise (which has a minor effect on small-region examinations such as in the current study);
- Absence of GV calibrations in CBCT units by some manufacturers;
- Differences in GVs for the same matter in different CBCT models.
5. Conclusions
- The newly generated R-Motion and RaceEvo rotary systems exhibited superior preparative results by producing less overall canal transportation and less volumetric dentin removal compared to ProTaper Gold and manual instrumentation techniques;
- R-Motion and RaceEvo rotary systems could be used as a reliable alternative without causing adverse mechanical effects and maintaining original root canal anatomy of curved primary root canal systems compared to ProTaper Gold rotary systems with manual instrumentation;
- Generally, more supportive studies evaluating the abilities of newly introduced rotary systems on curved primary root canals using detailed CBCT analyses are required.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pinheiro, S.L.; Araujo, G.; Bincelli, I.; Cunha, R.; Bueno, C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int. Endod. J. 2012, 45, 379–385. [Google Scholar] [CrossRef]
- Cleghorn, B.M.B.; Boorberg, N.B.; Christie, W.H. Primary human teeth and their root canal systems. Endod. Topics 2012, 23, 6–33. [Google Scholar] [CrossRef]
- Yu, Y.; Zhou, X.; Zheng, L.W. Advanced research on root canal therapy for primary teeth. West China J. Stomatol. 2020, 38, 205–210. [Google Scholar]
- MohdAriffin, S.; Dalzell, O.; Hardiman, R.; Manton, D.J.; Parashos, P.; Rajan, S. Root canal morphology of primary maxillary second molars: A micro-computed tomography analysis. Eur. Arch. Paediatr. Dent. 2020, 21, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Fumes, A.C.; Sousa-Neto, M.D.; Leoni, G.B.; Versiani, M.A.; da Silva, L.A.; da Silva, R.A.; Consolaro, A. Root canal morphology of primary molar: A micro-computed tomogrophy study. Eur. Arch. Paediatr. Dent. 2014, 15, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.Y.; Zhou, Z.X.; Tseng, W.J.; Karabucak, B. Comparison of canal transportation and centering ability of manual K-files and reciprocating files in glide path preparation: A micro-computed tomography study of constricted canals. BMC Oral Health 2021, 21, 83. [Google Scholar] [CrossRef]
- Fabbro, M.D.; Afrashtehfar, K.I.; Corbella, S.; El-Kabbaney, A.; Perondi, I.; Taschieri, S. In Vivo and In Vitro Effectiveness of Rotary Nickel-Titanium vs Manual Stainless Steel Instruments for Root Canal Therapy: Systematic Review and Meta-analysis. J. Evid. Based Dent. Pract. 2018, 18, 59–69. [Google Scholar] [CrossRef]
- Barr, E.S.; Kleier, D.J.; Barr, N.V. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr. Dent. 2000, 22, 77–78. [Google Scholar] [PubMed]
- Alnassar, I.; Alsafadi, A.S.; Kouchaji, C. Assessment of the apically extruded debris between a rotary system, a reciprocating system and hand files during the root canal instrumentation of the deciduous molars. Dent. Med. Probl. 2019, 56, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Katge, F.; Patil, D.; Poojari, M.; Pimpale, J.; Shitoot, A.; Rusawat, B. Comparison of instrumentation time and cleaning efficacy of manual instrumentation, rotary systems and reciprocating systems in primary teeth: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2014, 32, 311–316. [Google Scholar] [CrossRef]
- Jeevanandan, G. Kedo S paediatric rotary files for root canal preparation in primary teeth—Case report. J. Clin. Diagn. Res. 2017, 11, 3–5. [Google Scholar] [CrossRef]
- George, S.; Anandaraj, S.; Isaac, J.S.; John, S.A.; Harris, S. Rotary endodontics in primary teeth—A review. Saudi Dent. J. 2016, 28, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Eliasz, W.; Kubiak, K.; Poncyljusz, W.; Surdacka, A. Root Canal Transportation after Root Canal Preparation with ProTaper Next, WaveOne Gold, and Twisted Files. J. Clin. Med. 2020, 9, 3661. [Google Scholar] [CrossRef]
- Yalniz, H.; Koohnavard, M.; Oncu, A.; Celikten, B.; Orhan, A.I.; Orhan, K. Comparative evaluation of dentin volume removal and centralization of the root canal after shaping with the ProTaper Universal, ProTaper Gold, and One-Curve instruments using micro-CT. J. Dent. Res. Dent. Clin. Dent. Prospects 2021, 15, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Elnaghy, A.M.; Elsaka, S.E. Shaping ability of ProTaper gold and ProTaper universal files by using cone-beam computed tomography. Indian J. Dent. Res. 2016, 27, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Grande, N.M.; Plotino, G.; Pecci, R.; Bedini, R.; Pameijer, C.H.; Somma, F. Micro-computerized tomographic analysis of radicular and canal morphology of premolars with long oval canal. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, e70–e76. [Google Scholar] [CrossRef] [PubMed]
- Shahriari, S.; Abedi, H.; Hashemi, M.; Jalalzadeh, S.M. Comparison of removed dentin thickness with hand and rotary instruments. Iran. Endod. J. 2009, 4, 69–73. [Google Scholar]
- Lopez, F.U.; Fachin, E.V.; Camargo-Fontanella, V.R.; Barletta, F.B.; So, M.V.; Grecca, F.S. Apical transportation: A comparative evaluation of three root canal instrumentation techniques with three different apical diameters. J. Endod. 2008, 34, 1545–1548. [Google Scholar] [CrossRef]
- Musale, P.K.; Jain, K.R.; Kothare, S.S. Comparative assessment of dentin removal following hand and rotary instrumentation in primary molars using cone-beam computed tomography. J. Ind. Soc. Pedod. Prev. Dent. 2019, 37, 80–86. [Google Scholar] [CrossRef]
- Adisen, M.Z.; Yılmaz, S.; Misirlioglu, M.; Atil, F. Evaluation of volumetric measurements on CBCT images using stafne bone cavities as an example. Med. Oral Patol. Oral Cir. Bucal 2015, 20, 580–586. [Google Scholar] [CrossRef]
- FKG R-Motion. Available online: https://www.fkg.ch/products/endodontics/canal-shaping-and-cleaning/r-motion (accessed on 4 September 2021).
- FKG Race-Evo. Available online: https://www.fkg.ch/sites/default/files/FKG_RACE%20EVO_Brochure_EN_WEB_202006.pdf (accessed on 4 September 2021).
- Hashem, A.B.R.; Ghoneim, A.G.; Lutfy, R.A.; Foda, M.Y.; Omar, G.A.F. Geometric Analysis of Root Canals Prepared by Four Rotary NiTi Shaping Systems. J. Endod. 2012, 38, 996–1000. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, R.S.; Agarwal, J.; Jain, P.; Chandra, A. Comparative Analysis of canal centering ability of different single file systems using cone beam computed tomography—An in vitro study. J. Clin. Diagn. Res. 2015, 9, ZC06–ZC10. [Google Scholar] [CrossRef] [PubMed]
- Boscornea-Puşcu, A.S.; Orel, L.; Velea-Barta, O.A.; Horhat, R.M.; Negrutiu, M.L.; Nica, L.M.; Duma, V.F.; Stoia, D.I.; Opriş, C.; Sinescu, C. Experimental Study of the Effects of Torsional Loading on Three Types of Nickel-Titanium Endodontic Instruments. Appl. Sci. 2021, 11, 7224. [Google Scholar] [CrossRef]
- Reham, H.; Roshdy, N.; Issa, N. Comparison of canal transportation and centering ability of Xp Shaper, WaveOne and Oneshape: A cone beam computed tomography study in curved root canals. Acta Odontol. 2018, 31, 67–74. [Google Scholar]
- Singh, S.; Abdul, M.S.M.; Sharma, U.; Sainudeen, S.; Jain, C.; Kalliath, J.T. An in vitro comparative evaluation of volume of removed dentin, canal transportation, and centering ratio of 2Shape, WaveOne Gold, and ProTaper Gold files using cone-beam computed tomography. J. Int. Soc. Prev. Community Dent. 2019, 9, 481–485. [Google Scholar]
- Dentsply ProTaper Gold. Available online: https://www.dentsply.com/content/dam/dentsply/pim/manufacturer/Endodontics/Glide_Path__Shaping/Rotary__Reciprocating_Files/Shaping/ProTaper_Gold_Rotary_Files/ProTaper-Gold-Brochure-p7btcwy-en-1502.pdf (accessed on 4 September 2021).
- Kummer, T.R.; Calvo, M.C.; Cordeiro, M.M.; de Souza, V.R.; de Carvalho, R.M.J. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, e84–e92. [Google Scholar] [CrossRef]
- Tabassum, S.; Zafar, K.; Umer, F. Nickel-Titanium Rotary File Systems: What’s New? Eur. Endod. J. 2019, 3, 111–117. [Google Scholar]
- Silva, E.J.N.L.; Martins, J.N.R.; Lima, C.O.; Vieira, V.T.L.; Braz Fernandes, F.M.; De-Deus, G.; Versiani, M.A. Mechanical Tests, Metallurgical Characterization, and Shaping Ability of Nickel-TitaniumRotary Instruments: A Multimethod Research. J. Endod. 2020, 46, 1485–1494. [Google Scholar] [CrossRef]
- Pereira, F.; Martins, R.F.; Ginjeira, A. Cyclic fatigue resistance of ProTaper Gold and comparison with ProTaper Universal instruments. Rev. Port. Estamol. Med. Dent. Cir. Maxillofac. 2018, 59, 75–79. [Google Scholar] [CrossRef]
- Duque, J.A.; Vıvan, R.R.; Cavenago, B.C.; Amorosso-Silva, P.A.; Bernardes, R.A.; de Vasconcelos, B.C.; Duarte, M.A.H. Influence of NiTi alloy on the root canal shaping capabilities of the ProTaper Universal and ProTaper Gold rotary instrument systems. J. Appl. Oral Sci. 2017, 25, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Roane, J.B.; Sabala, C.L.; Duncanson, M.G. The “balanced force” concept for instrumentation of curved canals. J. Endod. 1985, 11, 203–211. [Google Scholar] [CrossRef]
- Nishijo, M.; Ebihara, A.; Tokita, D.; Doi, H.; Hanawa, T.; Okiji, T. Evaluation of selected mechanical properties of niti rotary glide path files manufactured from controlled memory wires. Dent. Mater. J. 2018, 37, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Prabhakar, A.R.; Yavagal, C.; Dixit, K.; Naik, S.V. Reciprocating vs Rotary Instrumentation in Pediatric Endodontics: Cone Beam Computed Tomographic Analysis of Deciduous Root Canals using Two Single-file Systems. Int. J. Clin. Ped. Dent. 2016, 9, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Pauwels, R.; Jacobs, R.; Singer, S.R.; Mupparapu, M. CBCT-based bone quality assessment: Are Hounsfield units applicable? Dentomaxillofac. Radiol. 2015, 44, 20140238. [Google Scholar] [CrossRef] [Green Version]
- Schulze, R.; Heil, U.; Gross, D.; Bruellmann, D.D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A review. Dentomaxillofac. Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauwels, R.; Araki, K.; Siewerdsen, J.H.; Thongvigitmanee, S.S. Technical aspects of dental cone-beam CT: State of the art. Dentomaxillofac. Radiol. 2014, 44, 20140224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molteni, R. Prospects and challenges of rendering tissue density in Hounsfield units for cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 105–119. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Multiple Comparisons of Canal Transportation across Experimental Groups | p-Value | ||
|---|---|---|---|
| Race Evo vs. R-Motion | 0.1329± 0.013 | 0.1386 ± 0.014 | >0.9999 |
| Race Evo vs. ProTaper Gold | 0.1329 ± 0.013 | 0.2255 ± 0.015 | 0.0002 *** |
| Race Evo vs. Manual | 0.1329 ± 0.013 | 0.1781 ± 0.016 | 0.2086 |
| R-Motion vs. ProTaper Gold | 0.1386 ± 0.014 | 0.2255 ± 0.015 | 0.0006 *** |
| R-Motion vs. Manual | 0.1386 ± 0.014 | 0.1781 ± 0.016 | 0.4603 |
| ProTaper Gold vs. Manual | 0.2255 ± 0.015 | 0.1781 ± 0.016 | 0.2126 |
| Multiple Comparisons of Volumetric Dentin Removal across Experimental Groups | p-Value | ||
|---|---|---|---|
| Race Evo vs. R-Motion | 0.4629 ± 0.018 | 0.4957 ± 0.017 | 0.679 |
| Race Evo vs. ProTaper Gold | 0.4629 ± 0.019 | 2.015 ± 0.074 | 0.000 *** |
| Race Evo vs. Manual | 0.4629 ± 0.020 | 0.8427 ± 0.11 | 0.014 * |
| R-Motion vs. ProTaper Gold | 0.4957 ± 0.017 | 2.015 ± 0.074 | 0.000 *** |
| R-Motion vs. Manual | 0.4957 ± 0.018 | 0.8427 ± 0.11 | 0.027 * |
| ProTaper Gold vs. Manual | 2.015 ± 0.074 | 0.8427 ± 0.12 | 0.000 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
İslam, A.; Ünsal, G.; Almashharawi, A. Canal Transportation and Volumetric Dentin Removal Abilities of Ni-Ti Rotary File Systems in Curved Primary Root Canals: CBCT Study. Appl. Sci. 2021, 11, 9053. https://doi.org/10.3390/app11199053
İslam A, Ünsal G, Almashharawi A. Canal Transportation and Volumetric Dentin Removal Abilities of Ni-Ti Rotary File Systems in Curved Primary Root Canals: CBCT Study. Applied Sciences. 2021; 11(19):9053. https://doi.org/10.3390/app11199053
Chicago/Turabian Styleİslam, Aylin, Gürkan Ünsal, and Alaa Almashharawi. 2021. "Canal Transportation and Volumetric Dentin Removal Abilities of Ni-Ti Rotary File Systems in Curved Primary Root Canals: CBCT Study" Applied Sciences 11, no. 19: 9053. https://doi.org/10.3390/app11199053
APA Styleİslam, A., Ünsal, G., & Almashharawi, A. (2021). Canal Transportation and Volumetric Dentin Removal Abilities of Ni-Ti Rotary File Systems in Curved Primary Root Canals: CBCT Study. Applied Sciences, 11(19), 9053. https://doi.org/10.3390/app11199053