1. Introduction
The advent of the Internet and new digital technologies has completely changed the way we communicate. In recent years, a widespread phenomenon is that of social media, a group of Internet-based applications that allow the creation and exchange of user-generated contents [
1]. Due to the diffusion of smartphones into people’s daily routines, these technologies offer the innovative opportunity to reach a large audience and represent an inexpensive, rapid, and powerful way to communicate and disseminate information [
2]. An exponentially increasing number of publications in medicine and dentistry have focused on the importance of using social media for health promotion interventions [
3,
4] and evidence suggests that new technologies can effectively contribute to improve knowledge and behavioral changes [
5,
6]. Social media have demonstrated to be a promising resource to facilitate chronic diseases self-management, medication adherence, tobacco cessation and support for mental health conditions [
5,
7,
8]. Other recent studies used digital platforms to disseminate information related to skin cancer prevention [
6], human papillomavirus vaccination [
9], nutrition, and physical activity [
10].
The Lancet Commission on Adolescent Health and Wellbeing suggested that Digital Media offer “outstanding new possibilities for engagement” with youth populations [
11]. In dentistry, several studies investigated the contents of social media on oral health and treatment procedures [
12,
13,
14,
15,
16], but until now there has been little research on the effectiveness of social in relation to orthodontics. A good communication is an integral part of orthodontic treatments to obtain the patient’s compliance for the oral hygiene, considering that the insertion of fixed orthodontic appliances makes hygiene procedures more difficult, restricts salivary and mucosal self-cleaning capacity, altering the microbial environment and increasing plaque build-up [
17,
18,
19,
20]. As a result, gingivitis and enamel demineralization (including white spot lesions and dental caries) have been regarded as the most prevalent undesired effects that can lead to unsatisfactory results or premature termination of orthodontic therapy [
21]. Mehra et al. [
22] showed that 5% to 10% of orthodontic patients failed to complete their treatment just because of oral hygiene issues.
It is well known that patient’s compliance can be challenging during a long orthodontic therapy, especially in adolescents; therefore, both oral hygiene instruction (OHI) and patient motivation play a crucial role in maintaining an effective plaque control. To get better feedback, it would be appropriate to use communication tools that are familiar to youth population. As an innovative method, social media have the advantage of being constantly used, besides having interactive and engaging features such as animations [
23,
24]. The aim of this study is to investigate the effect of Instagram, the most used social media app among young adults [
25], in improving knowledge and compliance for oral hygiene among young patients with fixed orthodontic appliances.
The first null hypothesis of this study is that there is no significant difference in clinical parameters between young patients receiving conventional oral hygiene instructions with or without the additional use of a social media. Subsequently, the second null hypothesis is that no difference neither occurs when considering the increase of knowledge on oral health and oral practices as well as on dietary habits.
2. Materials and Methods
2.1. Trial Design
This study was designed as a prospective parallel-group, randomized, controlled, and single-center trial with a 1:1 allocation ratio. No changes to the methods occurred after the commencement of the study.
2.2. Participants, Eligibility Criteria, and Settings
This study obtained the approval of the Internal Review Board (2019–0717). Patients undergoing a fixed orthodontic treatment were recruited at the affiliation of the Authors of this article. The following criteria were applied to select participants of both sexes: presence of fixed orthodontic appliances on both arches during the following 6 months, age between 13 and 19 years old, no mental disabilities and no difficulties in reading or speaking the Italian language. Patients allocated in the intervention group had also to own a mobile phone with a valid account on Instagram. Signed consent was obtained from patients or parents (in case of underage patients) who were informed about the aim of the study before the recruitment as well as that the participation was voluntary with the possibility to withdraw at any time.
All the experimental phases took place at the affiliation of the Authors.
2.3. Interventions
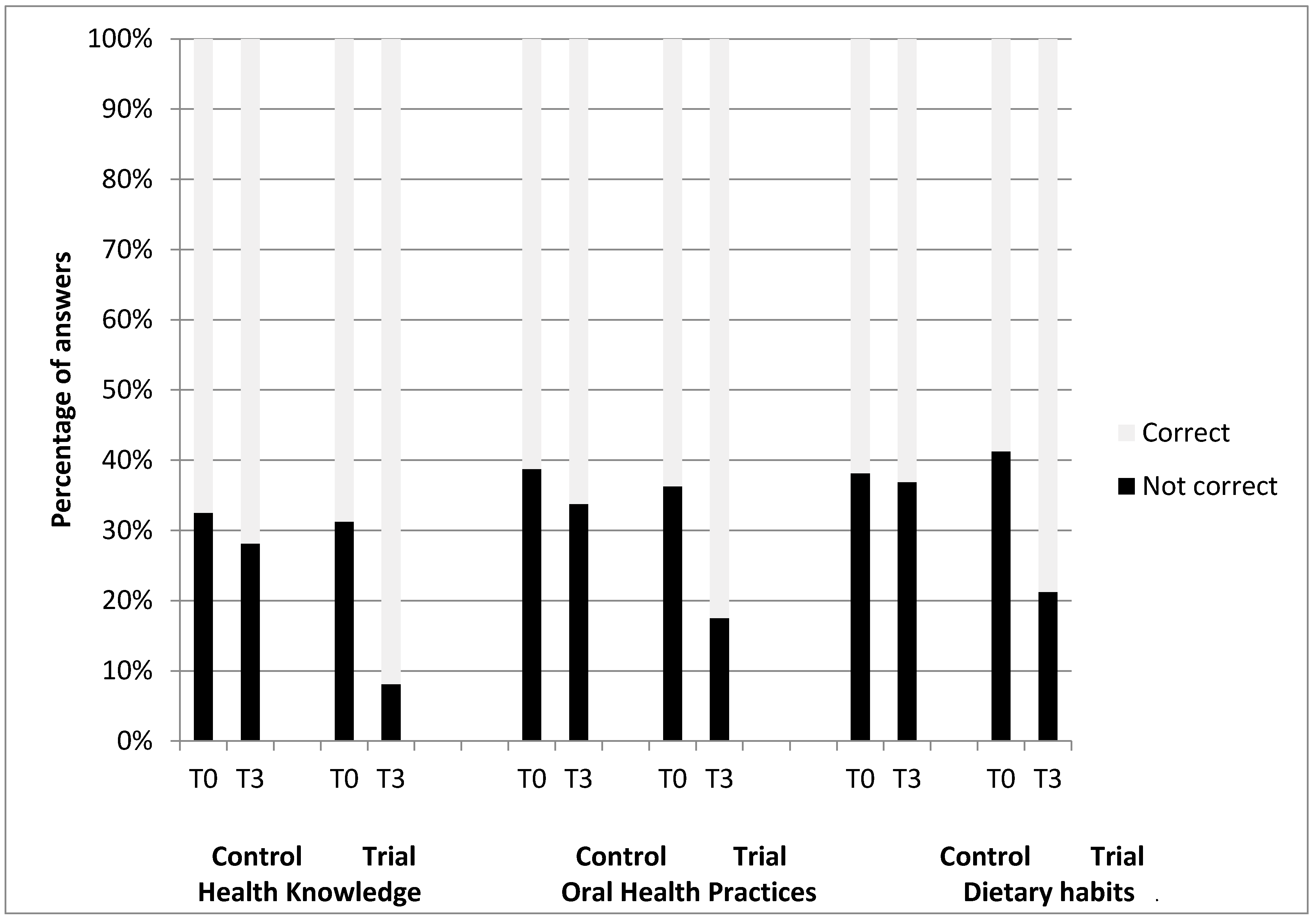
In order to investigate their knowledge on different topics related to oral health and hygiene, a multiple-choice questionnaire was given by a blind clinician to all participants at a first appointment (T0), before receiving oral instructions, and subsequently after six months, at the end of the study (T3). The questionnaire contained background information such as age, gender, parent’s education level, type of toothbrush, and 24 structured questions divided into three groups: oral health knowledge (see
Table S1), oral health practices (see
Table S2), and dietary habits (see
Table S3). Questions were adapted from various questionnaires [
26,
27,
28,
29,
30] and each question had 3 possible choices.
All patients received standardized oral hygiene instructions by the previous blind clinician who also used photos illustrating the most prevalent undesired effects of a bad plaque control. Motivation to oral hygiene was also performed during the succeeding appointments.
Participants selected according to the inclusion criteria were equally allocated to either the intervention or control group. In addition to the standard verbal information and motivation, patients allocated to the intervention group weekly received a post on Instagram for a period of 6 months by an unblind operator. The topics discussed on the social media were in form of photos and short videos and regarded 3 main themes, corresponding to the sections of the questionnaire: oral health knowledge, oral health practices, and dietary habits. Instagram posts were not sent to patients in the control group, however, during clinical appointments, they verbally received the same information.
2.4. Outcomes
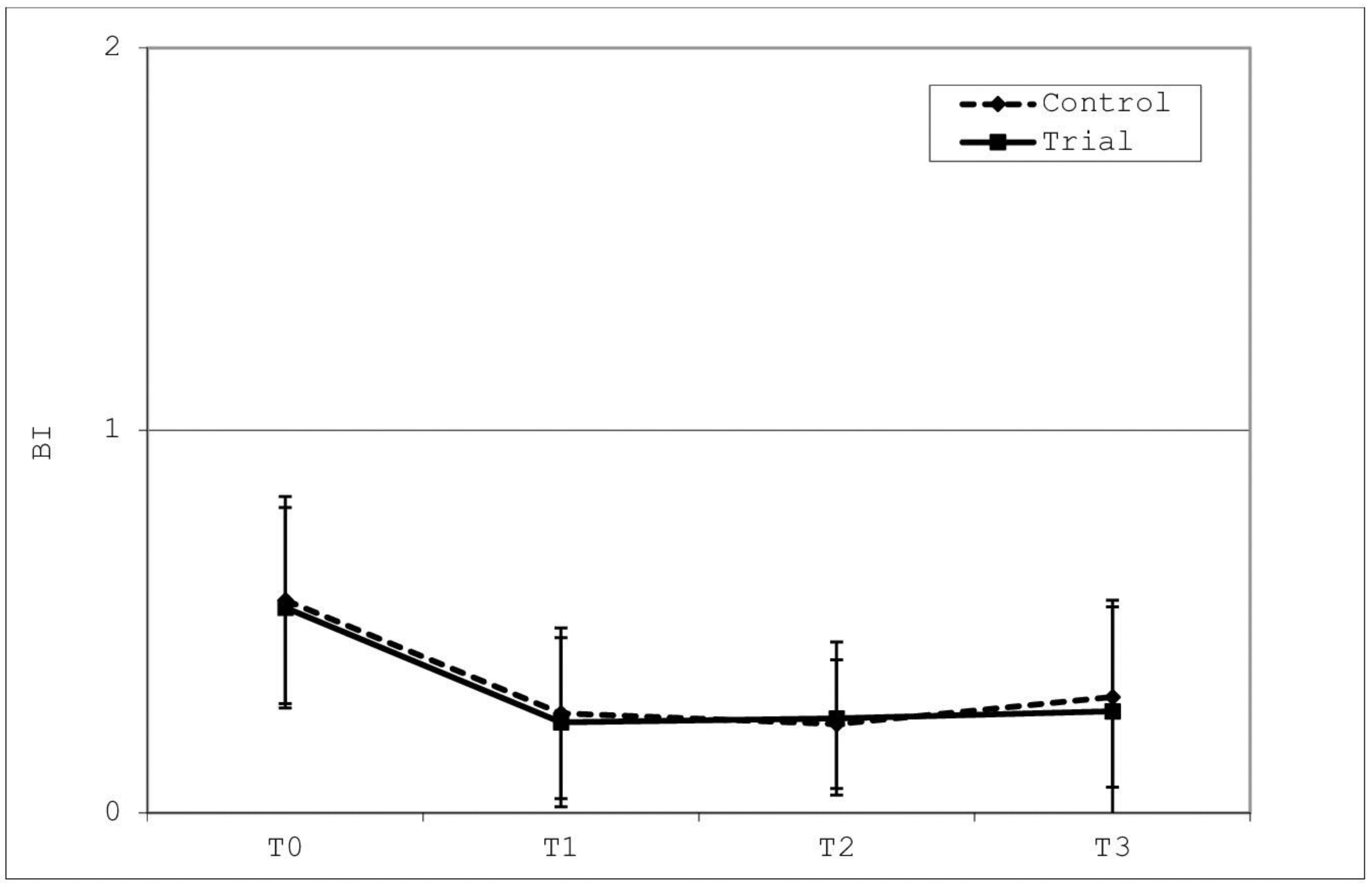
At every time point of the study (T0, T1, T2, and T3), clinical evaluations of the patient’s compliance for oral hygiene were performed assessing the bleeding index (BI), modified gingival index (MGI), and plaque index (PI) for all Ramfjord teeth (maxillary right first molar, maxillary left central incisor, maxillary left first premolar, mandibular left first molar, mandibular right first incisor, and mandibular right first premolar) [
31]. After probing three sites (mesio-buccal, buccal, and disto-buccal) of the gingival sulcus for each tooth examined (Probe UNC 15 R198; PDT, Missoula, MT, USA), the BI index was scored recording the absence of bleeding as 0, bleeding observed after 30 s as 1, and immediate bleeding as 2 [
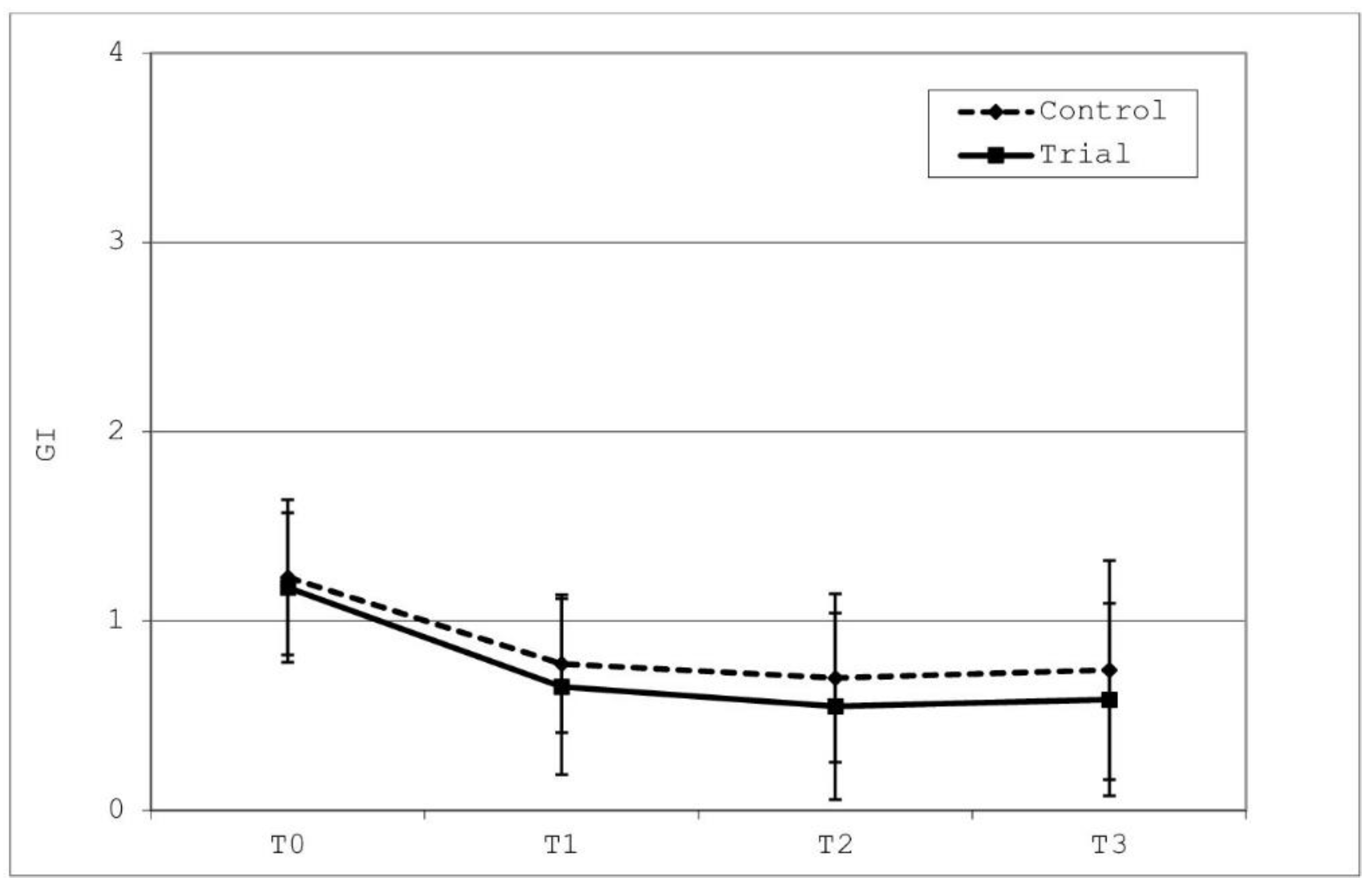
32]. On the same sites, the MGI was visually assessed assigning a grade from 0 to 3 denoting absent, mild, moderate, and severe inflammation of the buccal marginal gingiva, respectively [
33]. Finally, the PI was determined by making the patients chew a disclosing agent (Gum Red-Cote, Sunstar Italiana Srl, Saronno, Italy) according to the instructions of the manufacturer. The buccal surfaces of each tooth considered were divided into vertical and horizontal thirds with the bracket at the center [
34] and for both the two boxes alongside (mesial and distal) and for the three gingival (mesial-gingival, center-gingival, and disto-gingival) to the bracket, a score 0 (absence of plaque) or 1 (presence of plaque) was assigned by the operator [
35].
As regards the questionnaire submitted, the correct answers and those related to the optimal oral practice or dietary behaviour were scored. Percentages were calculated for the three different sections of the questionnaire.
Clinical assessments and questionnaires visualization were respectively performed by operators who were not involved in the previous phases and therefore did not know the participants’ allocation.
No changes to the outcomes occurred during the trial.
2.5. Sample Size Calculation
Sample size calculation (Alpha = 0.05; Power = 90%) for two independent study groups and a continuous primary outcome (oral health parameters) required 40 total participants (20 cases and 20 controls). Concerning the variable bleeding index (primary outcome) an expected mean of 0.89 was hypothesized, with a standard deviation of 0.087 [
31]. The expected difference between the means was supposed to be 0.09, therefore 20 patients were requested for each group. Loss to follow-up and incomplete compliance with therapy were excluded.
The answers to the questionnaire were considered as the secondary outcome. Interim analysis and stopping guidelines were not applicable.
2.6. Sequence Generation
Randomized sequence was generated with a computer software (R version 3.1.3, R Development Core Team, R Foundation for Statistical Computing, Wien, Austria) using a block randomization table and considering a permuted block randomization with twenty participants for each of the two fixed blocks.
2.7. Allocation Concealment
The operator who enrolled participants also achieved the allocation concealment using sequentially numbered and sealed envelopes containing the allocation cards previously prepared. The randomization list generated was held securely in remote location.
2.8. Implementation
The random allocation sequence list was generated by the operator who subsequently performed data analyses. Participants were enrolled by another operator who also assigned them to the respective treatment.
2.9. Blinding
Both the clinician giving verbal instructions to the patients, the two outcomes assessors and the data analyst were blinded during the study. The former operators were not aware of the allocation concealment, whereas the second did not took part to the clinical visits.
2.10. Statistical Methods
A computer software was used to calculate descriptive and inferential statistics (R version 3.1.3, R Development Core Team, R Foundation for Statistical Computing, Wien, Austria).
Descriptive statistics were used for the following clinical measurements: BI, MGI, and PI. Mean and standard deviation were calculated for each parameter at each time point. The normality of distributions was tested with Kolmogorov and Smirnov test. Inferential comparisons among groups were performed using ANOVA test with post hoc Tukey tests.
Chi squared test was used to analyze the frequency distributions of the answers in the three parts of the questionnaire.
The significant level was set at p < 0.05 for all the tests. No additional analyses were performed.
4. Discussion
The present report examined the effect of the social media Instagram in improving both the oral hygiene compliance as well as the knowledge on oral health and dietary habits in young orthodontic patients belonging to the so-called generations of “millennials” and “post-millennials”, which generally include youth generations respectively born at the end of the last century and at the beginning of the present one. Subjects of these categories are characterized by a widespread resort to social media as a form of communication. In particular, Instagram was chosen in this study because it is the most common platform nowadays [
9].
After the application of multibrackets appliances, a worsening of the oral hygienic conditions of the patient generally occurs [
36]. In addition to the verbal information and motivation, the strategy used to promote oral hygiene compliance in the intervention group of this study was that of sharing on Instagram multimedia contents consisting of pictures and short videos with written explanations, to analyze whether this latter action could be more effective than the traditional verbal communication. A variation of the compliance was clinically assessed through oral health indicators (BI, MGI, and PI) whereas a multiple-choice questionnaire investigated the improvements in patients’ knowledge.
The first null hypothesis of the present investigation was accepted. For both the trial and control group, and therefore independently of the system used by the clinician to give information, results demonstrated significantly lower BI, MGI, and PI scores at T1 (one month after baseline point) compared to those shown at T0, with no significant differences between the groups. Moreover, no significant differences were revealed between T1, T2 (three months after T0), and T3 (six months after T0), neither within each group nor between the two. These data suggest that oral hygiene instructions and motivation performed at the initial appointment, rather than afterwards, play the most important role in improving clinical indexes since after the initial step average values remained constant. No influence has been shown as regards the method used to communicate with the patient.
Many authors have tried to find the most appropriate ways for maintaining patients’ compliance, considering that an ineffective plaque control can lead to undesired effects such as gingival inflammation and dental caries. In order to prevent the most frequent consequences due to plaque build-up during a fixed orthodontic treatment, different studies have evaluated the efficacy of text message reminders demonstrating significant lower BI, MGI, and PI scores after different times [
31,
37,
38]. Leone et al., [
39] also showed the positive influence of these tools when used twice a week for a period of three months to stress the usage of intermaxillary elastics in the treatment of Class II malocclusions. However, text messages belong more to past years and generations, whereas in the present era social media are the dominating way of communicating and they could be more appropriate especially for millennials and post-millennials since they spent most hours of their day right on these online platforms.
Until now, there has been quite little research on the efficacy of social media in relation to orthodontics, but a recent systematic review stated that information about orthodontics and other psychosocial factors related to orthodontic patients are spread on social media [
40]. A study assessing their usage among patients and practitioners, as well as their potential benefit in marketing and communication strategies, has included Instagram [
41]. Moreover, El Tantawi et al., [
42] stated that social media, especially Instagram, were preferred by adolescents to receive oral health information. However, to date, we have found no study which ever tested this specific platform to improve the compliance and knowledge of the patients regarding dental hygiene during an orthodontic therapy and this makes our results not directly comparable to those of other analogue studies.
A randomized controlled trial considered an intervention with a messaging app (WeChat), consisting of regular reminders and educational messages which caused an improvement in the plaque index and in the gingival index but, as in the present study, the difference was not statistically significant with controls [
43]. Conversely, the intervention with the app was effective in decreasing the treatment duration and the bracket bond failure. It would be also interesting to evaluate the variation of these parameters after providing multimedia contents on Instagram.
Zotti et al. [
44] tested a WhatsApp chat room-based competition in a protocol for domestic oral hygiene maintenance where a group of young orthodontic patients enrolled as trials had to monthly share with the other participants self-photographs showing their oral hygiene status. The efficacy of new technologies in the oral health status was demonstrated. Although this result contrasts with that reported in our study, the methodology used is surely different. The active competition among participants, instead of a simple flow of information like in our research, has surely influenced the outcomes with a greater effect.
The reason why a major advantage was not assessed for the trial group might be related to a lack of accuracy in visualizing all multimedia contents and for their whole duration time, which represents a limitation of this report. In fact, other research considers information provided in a visual modality effective in improving the attitude of the youngest towards the dental care, however an excessive length of the video might cause a loss of interest and attention [
45]. Accordingly, this might justify why a significant improvement in oral hygiene indexes was found in some of the studies previously mentioned in which only text messages reminders were used [
31,
37,
38]. These latter are obviously shorter compared to multimedia contents and therefore they are likely to have been read entirely by all participants. Other limitations of our study could be related to the intrinsic limitations of the procedures used to evaluate the clinical indexes such as a different pressure when evaluating the BI, the subjectivity in assessing the MGI, and the rigidity of the PI only distinguishing the presence or absence of plaque with no intermediate distinctions. Moreover, the presence of the oral appliance in the mouth could have made the clinical measurements more difficult resulting in altered results. Finally, the present report tested over time the cooperation of patients after conventional professional oral hygiene (using ultrasonic instruments). Other oral hygiene procedures and protocols (involving ozone, laser, or probiotic treatment) have been reported to be effective [
46] so further studies on the topic are needed.
The second null hypothesis of this study was rejected: although weekly sharing of information on Instagram did not seem to be able to improve the oral hygiene compliance, it was effective in improving the patients’ knowledge on both oral health and correct oral practices as well as on dietary habits. Answers given to the same questionnaire at the beginning (T0) and at the end (T3) of the study were compared: for all the sections of the questionnaire, a significant increase in average scores of correct answers was shown in the intervention group. Instead, patients who obtained information only in a verbal form did not register statistically differences between the two timepoints considered. Despite a limitation of this questionnaire might regard a certain number of patients not always aware of the true answer but answering correctly by chance, these results are in line with the study of Al-Silwadi et al., [
17] that used YouTube as an information tool for orthodontic patients demonstrating an improvement in knowledge related to the care of the dentition compared to standard methods of providing information.
Overall, the results we have obtained show a contrasting effect of Instagram in orthodontic young patients. Despite this social media seems not to improve compliance assessed clinically through the most common oral hygiene indexes, a positive effect was evident for the acquisition of notions linked to oral health. The use of Instagram to transfer information to the patients cannot substitute the traditional face-to-face communication requiring a clinician who gives instructions of oral hygiene to the person under treatment. Since orthodontic therapies might be quite long with an eventual risk of psychological disturbances for the youngest patients [
47], it is fundamental for the operator to establish an alliance with the patient, firstly to obtain and subsequently to strength his/her compliance. Nevertheless, Instagram can be used as a support to make young patients aware of the oral health and of the best habits which favor this condition. In this sense, considering the amount of time spent on social media, weekly multimedia contents on Instagram might be effective to stress the importance of these topics on young orthodontic patients, more than what dentists could do since orthodontic visits generally occur over a long period of time with a low frequency.
It appears that presenting information to orthodontic young patients through the Instagram app guarantees improvements in knowledge, but social media alone without the instructions and motivation performed by the dentist and the dental hygienist is not enough to improve oral hygiene compliance. Further research would be necessary to understand how to completely take advantage of these potential resources.

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}